
Abstract
Background
This study aims to evaluate data quality, scaling properties, and reliability of the Swedish RAND-36 in a general population sample and to present reference data for the Swedish population.
Methods
Testing of data quality, scaling assumptions and reliability followed methods recommended for the International Quality of Life Assessment Project, previously used for psychometric testing of SF-36 and RAND-36. Data were collected via regular mail for a random stratified sample of the general population in a Swedish county. Weighted means for RAND-36 scores were used and differences by sex, age, education, and occupational groups were tested.
Results
The response rate was 42%, and the sample comprised 3432 persons (45% men, 55% women) with a median age of 56.9 years. The internal consistency reliability was satisfactory, with Cronbach’s alphas > 0.80 for all eight scales. The percentage of missing items was low, ranging between 1.3% and 3.2%. No floor effects (≥15%) were noted, while ceiling effects were observed for physical functioning, role-functioning/physical, pain, role-functioning/emotional, and social functioning. Item–scale correlations were satisfactory (r ≥ 0.40). Correlations among the physical health scales were strong (range 0.58–0.68) as were the correlations among the mental health scales (range 0.58–0.73). Men reported significantly better health-related quality of life (HRQoL) on all scales, although the gender differences were small. Comparisons among age groups showed approximately equal scores among those 20–29, 30–39, and 40–49 years, while significant decreases in physical health were observed in the older age groups. Substantially worse physical health scores were observed in the oldest age group (80+). Significant differences among age groups were noted also for the mental health scales; however, better energy/fatigue and emotional well-being scores were seen in the older age groups, except for the oldest (80+). Those with university education reported significantly better scores on all scales compared to those with mandatory education.
Conclusions
The study suggests that the Swedish version of RAND-36 is an acceptable and reliable instrument for measuring HRQoL in the general population. The study provides reference data that can be used for norm-based comparisons.
Similar content being viewed by others

Background
The Medical Outcome Study (MOS) Short Form-36 (SF-36) is the most commonly used generic instrument for measuring health-related quality of life (HRQoL). Two versions of the form with identical items and response options have been presented, the SF-36 version 1 (SF-36v1) [1] and the RAND-36 [2]. RAND-36 and its scoring instructions are publicly available on the RAND Corporation’s website and can be used free of charge, while a license and a license fee are required to use the revised SF-36 version 2 (SF-36v2) [3].
Scale scores for RAND-36 and SF-36v1 are identical for six of the eight scales, whereas scoring algorithms for the pain and general health scales are slightly different. However, Hays et al. demonstrated that the correlation between the scales using the two different scoring algorithms was 0.99 in the MOS study, indicating that the difference is negligible [2].
A Swedish version of SF-36v1 was presented in the early 1990s [4,5,6], while a Swedish translation of RAND-36 has been available since 2013 [7, 8]. The translation of the Swedish RAND-36 differs slightly from the translation of the Swedish SF-36v1, but the translations are assumed to be sufficiently equivalent to allow comparisons between the two versions [8, 9]. A difference between them, however, is that algorithms for calculation of the physical and mental summary scores (PCS and MCS) obtained for the Swedish SF-36v1 [6], are not available for the Swedish RAND-36 [8].
Reference data for the general population are essential to evaluate whether an individual or a group score is above or below the average and are frequently used for norm-based interpretation of HRQoL results in clinical studies [10,11,12]. Normative population data for SF-36v1 have been collected in a number of countries such as new Zeeland [13], Canada [14], Norway [15], Italy [16], Brazil [17], Tunisia [18], and Greece [19]. Population norms for the Swedish SF-36v1 were collected in 1991–92 [4, 5] and are presented in detail in the Swedish manual and interpretation guide [6]. However, the Swedish SF-36v1 norms have not been updated. Swedish norms for RAND-36 are currently not available.
The aim of the study was to evaluate data quality, scaling properties, and reliability of the Swedish RAND-36 in a general population sample. A second aim was to present RAND-36 norms for the general population in a central region of Sweden.
Methods
Design and setting
The Mid-Swed Health Survey [20] was conducted in Region Örebro County, a central region of Sweden with approximately 290,000 inhabitants. The region contains a larger city, several small towns, and rural areas, and about 250,000 people live in a city or small-town area and 40,000 in rural areas.
A random sample, stratified by sex and age, was selected from the general population. An equal part of men and women were randomly selected. From the age group 20–29 and 30–39 years, 800 persons were recruited to each group, as a lower response rate was expected in these age groups. From all other age groups, 340–480 persons were recruited.
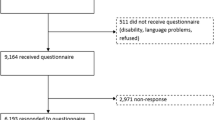
The sample size was calculated setting a power at 80% (α = 0.05) to detect a between-group difference of 10 scale points, which can be considered as a medium difference for scale scores ranging between 0 and 100 [12, 21, 22]. The estimation of sample size was based on the RAND-36 subscale (role-functioning/physical) that requires the largest sample to detect a 10-point difference between two groups. In September 2015, 4040 persons received an invitation to participate along with an information letter via regular mail. The survey comprised a 9-page questionnaire including the Swedish RAND-36 and questions about gender, year of birth, occupation, and level of education [20]. The questionnaire was distributed along with a prepaid return envelope via regular mail. After 2 weeks, a thank-you/reminder card was delivered. If the questionnaire was not returned after 5 weeks, a reminding letter and a new questionnaire was sent via regular mail. Because of a low response rate, an additional sample of 4100 persons were invited in March 2016, according to the same stratification principles.
Classification of subgroups
Age was grouped into 10-year intervals (20–29, 30–39, etc.) with people 80 years and older in one group.
Education was classified into three categories: mandatory (grade 0–9), high school (grade 10–12), and university education (> 12).
The occupation variable included 11 categories: employed, own company, parental leave, student, in labour market program, job seeker, old age pension, activity or sickness compensation, long term sickness, and other. The following subgroups were created from the occupation variable: 1. Employed and self-employed (including employed, own company and parental leave); 2. Unemployed (participants in labour market programs and job seeker) 3. On sick leave (including activity or sickness compensation, and long term sickness). Persons with old age pension and students were not included in the analysis of occupation.
Rand-36
The RAND-36 consists of 36 items grouped into eight multi-item scales: physical functioning (PF), role-functioning/physical (RP), pain (P), general health (GH), energy/fatigue (EF), social functioning (SF), role-functioning/emotional (RE), and emotional well-being (EW). An additional item asks about health change (HC) in the past year. Scale scores are summed and transformed into scales ranging from 0 (worst possible health state) to 100 (best possible state). A scale score was calculated if at least half of the items in a scale were answered by the respondent (half-scale method) and missing-item values were imputed using a person-specific mean value based on the non-missing items [1]. The half-scale rule is used in scoring of SF-36; however, this criterion is not used in the standard scoring algorithm for RAND-36.
Psychometric methods
Testing of data quality, scaling assumptions, and reliability followed methods recommended for the International Quality of Life Assessment (IQOLA) Project [23], previously used for psychometric testing of SF-36 and RAND-36 [24]. Psychometric tests were performed in the total sample and in subgroups by gender, age, education, and occupation.
Data quality
Completeness of data was evaluated by calculating the percentage of missing data for each of the 36 items. At the scale level, the percentage of computable scale scores was calculated using the half-scale method.
Floor and ceiling effects
Floor and ceiling effects were analyzed by calculating the proportion of participants scoring at the lowest and highest possible levels. At the item level, a floor or ceiling effect was considered if at least 50% of the respondents scored at the minimum or maximum level [25]. At the scale level, an effect was indicated if at least 15% of the respondents scored at the lowest or highest level [26].
Reliability
Cronbach’s alpha coefficients were computed to estimate the internal consistency reliability of scale scores. A coefficient of at least 0.70 is considered appropriate for group data, although 0.80 is desirable. A coefficient of 0.90 or better is recommended for individual assessment [27].
Test of scaling assumptions
Item–scale correlations, that is, the correlation between each item and its own subscale (corrected for overlap), were calculated. A correlation of 0.40 or greater is considered satisfactory [26]. The correlation between items and other subscales was assessed and considered adequate if the correlations were better with the own scale than with other scales. The significance of a difference between two item-scale correlations was determined using the standard error of the correlation matrix (1/√n). The recommended significance criterion of two standard errors was used [26]. Pearson correlation analysis was performed to assess the correlation between item and scales scores.
Inter-scale correlations
The correlations (Pearson correlation) among subscales were tested and interpreted as low (< 0.30), medium (0.30–0.49), or strong (0.50) [22] Hypotheses about the magnitude of inter-scale correlations were based on results of the validation of the Swedish SF-36v1 [6]. The strongest correlation was expected between energy/fatigue and emotional well-being, and the weakest between physical functioning and emotional well-being. According to factor analysis, physical functioning, role-functioning/physical, pain, and general health, are strongly related to physical health, while energy/fatigue, social functioning, role-functioning/emotional, and emotional well-being, are strongly associated to mental health. It was hypothesized that the correlations between the four scales that primarily measure physical health would be strong, as well as between the four scales that primarily measure mental health.
Test of group differences
Known-groups analysis was performed to test the sensitivity of the scales and ability to capture expected differences between subgroups based on gender, age, education, and occupation [12]. Based on the results of the validation of the Swedish SF-36v1 [5, 6], we assumed: a) that men report better health than women on all eight scales; b) that the four physical health scales gradually deteriorate with age; c) that the differences based on age are smaller for the four mental health scales; d) that those with a low level of education, the unemployed, or those on sick leave, report poorer health.
Weighted mean RAND-36 0–100 scale scores were calculated for the total sample and for subgroups based on gender, age, education, and occupation. Weighted mean T-scores were also calculated to improve comparability across subgroups. T-scores have a mean value of 50 and standard deviation of 10 in the total sample and a T-score above 50 indicates better HRQoL compared to the total norm population. A sampling weight was derived to reflect the demographic distribution of age and gender of the Swedish population in 2015, and non-response. Differences in weighted means between two groups were tested using the nonparametric Somers’ D-test [28], and three or more groups were tested using F-test, with taking account for the sampling design. P-values for post hoc pairwise comparisons of the weighted means were adjusted for multiple comparisons using Šidák’s method [29], and adjusted p-value 5% or lower was considered to be statistically significant. Linear regression was used to examine whether there was linear or quadratic trend by increasing age. To test a linear trend, the seven-level age variable was used as a continuous variable, and to test quadratic trend, the square of the age variable was added to the model. Survey design and the sampling weight were accounted in linear regression models. SAS 9.4 (SAS Institute, Cary, NC, USA), IBM’s Statistics for Windows Version 22 (IBM, Armonk, NY, USA) and Stata SE Version 15 (StataCorp, College Station, Texas, USA) were used for statistical analysis.
Results
Sample characteristics
The overall response rate was 42% and the final sample comprised 3422 participants [20]. The response rate varied according to age and was 61% in participants older than 60 years, 42% in participants 40–59 years, and 28% in the youngest participants (20–39 years old). The sample had a lower proportion of people aged 20–59 and a greater representation of people aged 60 years and older compared with the general Swedish population (Table 1). The weighted sample had the same gender and age distribution as the Swedish population. The age and sex distributions of participants and non-respondents did not differ markedly.
A total of 3422 people, 55% women and 45% men, participated in the study. Mean (SD) age was 56.9 (20.1) years (range 20–100 years). Half of the participants were 60 years or older.
Most participants (89%) were born in Sweden. One-third (33%) had university education, 43% had high school education, and 24% had mandatory education (Table 1). Approximately half (46%) of the participants were employed/self-employed, 39% were retirees, 4% were students, 3% on sick leave, and 3% were unemployed.
Measurement properties
Completeness of data
The percentage of missing items was generally low, ranging from 1.3% to 3.2%, averaging 2.2%. The proportion of participants for whom scale scores were computable was consistently high and ranged from 97.1% for role-functioning/emotional to 99% for social functioning (SF) (Table 2). Most subgroups had less than 2% missing scale scores, except for the unemployed with 5.8% missing, the oldest age group (80+) with 4.6% missing, and those with mandatory education with 3.0% missing scores (not presented in a table).
Floor and ceiling effects
On the item level, the proportion of subjects who chose the lowest response option (floor effect) varied between 0.8% for emotional well-being item 2 (EW2) and 33.0% for role-functioning/physical item 2 (RP2) (items are presented in Appendix 1). The proportion who chose the highest response option (ceiling effect) varied between 7.5% (EF2) and 70% (EW2). No floor effects (more than 50% at the lowest level) were noted, but ceiling effects (more than 50% at the highest level) were observed for all role-functioning/physical, pain, role-functioning/emotional, and social functioning items, all physical functioning items except PF1, one general health item (GH2), and two emotional well-being items (EW1, EW2).
On the scale level, the proportion who scored at the lowest level varied from 0.1% for emotional well-being and general health to 18.7% for role-functioning/physical (Table 2). The proportion who scored at the highest level varied from 3.5% for energy/fatigue to 64.2% for role-functioning/emotional. Floor effects (more than 15% at the lowest level) were found for role-functioning/physical, while ceiling effects (more than 15% at the highest level) were noted for role-functioning/emotional, role-functioning/physical, social functioning, and pain.
Internal consistency reliability
In the total sample, internal consistency reliability coefficients (Cronbach’s alpha) were greater than 0.80 for all scales (Table 3). Alphas above the 0.90 level were noted for physical functioning and role-functioning/physical. In subgroups, the reliability coefficients varied between 0.73 and 0.94 and were above 0.80 in most analyses (93%).
Test of scaling assumptions
In the total sample, item–scale correlations were satisfactory (r ≥ 0.40) (Appendix 2, Table 3). Significantly higher correlations between items and other scales were supported for all items except two items (EW3, EW5) that correlated highly in both emotional well-being and energy/fatigue (items are presented in Appendix 1).
Inter-scale correlations
As expected, the weakest inter-scale correlation was noted between physical functioning and emotional well-being (r = 0.32), while the strongest correlation was seen for energy/fatigue and emotional well-being (r = 0.73) (Appendix 2). Correlations among the physical health scales (PF, RP, P, GH) were strong and ranged between 0.58 and 0.68. Also, correlations among the mental health scales (EF, SF, RE, EW) were strong and varied between 0.58 and 0.73. General health correlated strongly with other scales (range 0.50–0.66) and was most strongly associated with energy/fatigue (r = 0.66). Energy/fatigue showed a medium to strong correlation with other scales (range 0.43–0.73) and was most weakly associated with physical functioning (r = 0.43).
Swedish RAND-36 scores in the general population
Weighted mean RAND-36 scores were calculated for the total sample as well as for categories by gender, age, education, and occupation, and are presented in Tables 4 and 5. Weighted mean T-scores for the subgroups are presented in supplementary Tables 6 and 7.
Sex
Men had significantly better scores then women on all RAND-36 scales, although the differences were small (2.4–6.5 scale points) (Table 4).
Age groups
There was statistically significant differences in all RAND-36 scales by age group (Table 4). Post-hoc pairwise comparisons between the age groups 20–29, 30–39 and 40–49 showed that there was only one significant difference, i.e. pain was significantly worse at the ages of 40–49 years compared with those aged 20–29 years. As expected, decreases in physical health (PF, RP, P and GH) were observed with increasing age and substantially worse scores were seen in the oldest age groups (70–79 and 80+ years) compared to those aged 20–49 years. The decline by age was most prominent for physical functioning and role-functioning/physical.
Significant differences between age groups were noted also for the mental health scales (EF, SF, RE, and EW); however, better energy/fatigue and emotional well-being scores were seen in the older age groups, except for the oldest group (80+). People between 60 and 79 years reported significantly better energy/fatigue compared to all other age groups, including the younger adults (20–39 years). Energy/fatigue was also significantly better in the 50–59 age group compared to the oldest group (80+). Social functioning scores were roughly equal among those between 20 and 79 years, while significantly worse scores were observed in the oldest group (80+). No significant differences in role-functioning/emotional scores were observed among those aged 20–59 and 70–79 years, but significantly better scores were noted for those aged 20–79 years compared with the oldest (80+) and for those between 60 and 69 years compared with the group 30–39 years. Emotional well-being scores were significantly better in those 60–79 years compared to the younger and middle-aged (20–49 years) and the oldest (80+).
Education
Participants with mandatory education as their highest education were older than those with high school or university education, 73.4 (SD 13.7) vs. 48.6 (SD 18.3) and 49.6 (SD 17.8) years, respectively (p < 0.0001). Thus, tests of significant differences in HRQoL between education levels were adjusted for age. All age-adjusted RAND-36 scales differed significantly by level of education (Table 5). Pairwise comparisons showed that those with university and high school education reported significantly better scores on five of the RAND-36 scales (physical functioning, role-functioning/physical, general health, energy/fatigue, and social functioning) compared to those with mandatory education. Scores on five scales (general health, energy/fatigue, social functioning, role-functioning/emotional, and emotional well-being were roughly equal among those with high school and university education, whereas three scales (physical functioning, role-functioning/physical, and pain were significantly better in those with university education.
Occupation
Participants on sick leave were somewhat older than the employed and unemployed, 49.2 (SD 12.8) vs. 45.4 (SD 13.5) and 43.3 (SD 16.3) years, respectively (p = 0.008), and comparisons between groups were adjusted for age. All age-adjusted RAND-36 scales differed significantly by occupation group. Pairwise comparisons showed there were clear differences for all eight RAND-36 scales between employees/self-employed, unemployed, and those on sick leave (Table 5). Employees reported the best health status, while people on sick leave reported the worst health status.
Discussion
The purpose of the study was to evaluate the psychometric properties of the Swedish version of RAND-36 in the general population and to present Swedish reference values. The performance of the instrument was tested in the total sample as well as in subgroups by gender, age, education, and occupation. The completeness of data was satisfactory both at the item level and at the scale level, indicating that the questionnaire was well accepted by the respondents.
No floor effects (≥15%) for scale scores were observed in the total sample, while ceiling effects were noted, especially for role-functioning/physical, role-functioning/emotional, and social functioning (> 50%) but also for pain and physical functioning (28%–30%). Ceiling effects for these scales are expected in population studies [4, 23]. However, ceiling effects for role-functioning/physical and role-functioning/emotional can also be attributed to the use of dichotomous response options that limit the ability to discriminate between individuals. Also, the social functioning scale consists of only two items with similar wordings, which contributes to ceiling effects and weak discriminatory capacity. Ceiling effects in the total sample were lower for all scales compared to the validation of the Swedish SF-36v1 in the 1990s [4]. One likely explanation is that the response rate in the current study is lower, especially in the younger ages, which leads to a larger proportion of older people with worse scores on the physical health scales.
Satisfactory item–scale correlations (r ≥ 0.40) were confirmed for all eight scales and item–other scale correlations were in most cases acceptable. However, two emotional well-being items correlated equally strongly in the emotional well-being and energy/fatigue domains. Inter-scale correlations also showed that emotional well-being and energy/fatigue were strongly associated (r = 0.73). Cronbach’s alpha for the eight scales in the total sample ranged from 0.82 to 0.94, showing satisfactory internal consistency reliability for group comparisons. Alpha values were roughly at the same levels as in the validation of the Swedish SF-36v1 [4].
Men scored slightly better than women on all RAND-36 scales, in line the previous Swedish SF-36v1 validation study [4] and several other population studies in different countries [15, 17,18,19, 30]. In the present study, effect size estimates (Cohen’s d) indicated trivial gender differences for six scales (physical functioning, role-functioning/physical, pain, general health, social functioning, and role-functioning/emotional, while the differences for energy/fatigue and emotional well-being were in the small range.
As expected, comparisons among age groups showed worse physical health scores in the oldest age groups, especially for physical functioning and role-functioning/physical, which is consistent with results in other normative population studies [5, 13, 15, 17,18,19, 31]. Analyses of the mental health scales, however, showed better energy/fatigue and emotional well-being scores for those 60–79 years old compared to the youngest, middle-aged, and oldest (80+ years). The latter finding differs from the results in the validation of the Swedish SF-36v1 [5]. In the present study, mean scores on social functioning and role-functioning/emotional were roughly equal between age groups, except for the oldest who reported worse levels. The results regarding the mental health scales in different age groups differ between countries. Some studies have reported better mental health in older persons [15, 31], while the opposite trend has been observed in other countries [5, 18, 19]. Approximately equal mental health scores among age groups have also been reported [17].
As expected, those with university education reported better RAND-36 scores than those with mandatory education. Also, employed persons scored better than those who were on sick leave and the unemployed. These findings are in line with the previous Swedish SF-36v1 validation study [5] as well as most other normative population studies in other countries [15, 18, 19, 31] .
This study provides reference data for RAND-36 collected in 2015–16, based on a random sample of 3422 participants aged 20–100 years from the general population in a region in central Sweden. The demographic structure of the region is similar to many other regions in Sweden, and the data may be suitable as a reference for the general Swedish population. The Swedish SF-36v1 population norms, which were collected in the early 1990s, have frequently been used to compare and interpret the health profiles of patient populations. However, the demographic and socioeconomic changes as well as lifestyle changes in recent decades may well have affected the health status of the population, and it is unclear whether the SF-36v1 reference data are still valid for norm-based evaluations. Comparisons of SF-36 scores between population surveys in 1996, 2002, and 2015 in Norway indicated relatively stable scores over the 19-year period, but significant changes were observed in specific age groups [15].
Comparison of the RAND-36 and SF-36v1 health profiles in the total samples of the present and earlier Swedish validation study show generally worse scores in the current study on all scales except pain. Most scales (role-functioning/physical, general health, energy/fatigue, social functioning and role-functioning/emotional are clearly worse (5.8–9.0 points), while physical functioning and emotional well-being scores are slightly worse (4.4–4.8 points). These differences may to some extent be due to differences in the age distribution in the two studies. The unweighted mean age in the current study was 56.9 years, which is markedly higher than in the SF-36v1 validation study, where the mean age was 42.7 years [4]. However, in the present study a sampling weight was used to accurately reflect the demographic distribution of the Swedish population in 2015. The weighted mean age was 50 years, which is equal to the whole Swedish population but still significantly higher than in the previous validation study of SF-36v1.
The study presents no summary measures for physical and mental health, as there is no standard procedure available for the RAND-36. It should be noted that the SF-36 method for scoring the physical and mental component scores has been criticized, since the calculations in some cases tend to produce scores that deviate from the results obtained for the corresponding subscales [32, 33]. However, alternative scoring algorithms for the RAND-36 summary measures that differ from the SF-36 standard method have been proposed [33].
The large sample size (n = 3422) is a strength of the study that made it possible to repeat the psychometric analyses in several subgroups. According to recommendations in the IQOLA project, the sample size for norming of SF-36v1 in the general population should be approximately 2500 to 3000 participants [23]. The low response rate (42%) is a weakness that may affect the representativeness of the respondents and introduce bias in examined associations, even though this is not necessarily so [34]. The response rate was higher among those 60 years of age and older (61%), while only 28% in the youngest age groups (20–39 years) responded. The response rate in the present study is considerably lower than in the previous validation study of the SF-36v1 with a response rate of 68% [4]. The response rate has declined, especially in the younger ages, in several Swedish general population surveys during the last decades [35]. For example, the response rates in the Swedish national public health surveys have gradually decreased from 60% in 2004 to 47% in 2016. The current study was distributed by regular mail, but it may be advisable to include internet-based assessment to improve the response rate. To compensate for the expected low response rate in the younger age groups, the sample was stratified by age to obtain a sufficient number of respondents in all age groups. We also used a sampling weight to adjust the age and gender distribution to the general Swedish population, which means that the normative RAND-36 data presented in the study are estimated to be comparable to the Swedish population in 2015.
Conclusion
The study suggests that the Swedish version of RAND-36 is an acceptable and reliable instrument for measuring HRQoL in the general population. The study provides reference data that can be used for norm-based comparisons.
Availability of data and materials
The data that support the findings of this study are available from University Health Care Research Center, Faculty of Medicine and Health, Örebro University, Örebro, Sweden, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Abbreviations
- ANCOVA:
-
One-way analysis of covariance
- EF:
-
Energy/fatigue
- EW:
-
Emotional well-being
- GH:
-
General Health
- HRQoL:
-
Health-related quality of life
- IQOLA:
-
International Quality of Life Assessment
- P:
-
Pain
- PF:
-
Physical functioning
- RP:
-
Role-functioning/physical
- SF-36:
-
The Medical Outcome Study Short Form-36
- SF:
-
Social functioning
- RE:
-
Role-functioning/emotional
References
Ware Jr., J. E., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care, 30(6), 473–483.
Hays, R. D., Sherbourne, C. D., & Mazel, R. M. (1993). The RAND 36-item health survey 1.0. Health Economics, 2(3), 217–227. https://doi.org/10.1002/hec.4730020305.
Ware Jr., J. E. (2000). SF-36 health survey update. Spine (Phila Pa 1976), 25(24), 3130–3139. https://doi.org/10.1097/00007632-200012150-00008.
Sullivan, M., Karlsson, J., & Ware Jr., J. E. (1995). The Swedish SF-36 health survey--I. evaluation of data quality, scaling assumptions, reliability and construct validity across general populations in Sweden. Social Science & Medicine, 41(10), 1349–1358. https://doi.org/10.1016/0277-9536(95)00125-Q.
Sullivan, M., & Karlsson, J. (1998). The Swedish SF-36 health survey III. Evaluation of criterion-based validity: Results from normative population. Journal of Clinical Epidemiology, 51(11), 1105–1113. https://doi.org/10.1016/S0895-4356(98)00102-4.
Sullivan, M., Karlsson, J., & Ware Jr., J. E. (1994). SF-36 Hälsoenkät: svensk manual och tolkningsguide (Swedish manual and interpretation guide). Gothenburg: Sahlgrenska University Hospital.
Registercentrum (2021) Beställ RAND-36 kostnadsfritt. Sydöstra sjukvardsregionen. https://sydostrasjukvardsregionen.se/samverkansgrupper/kvalitetsregister/registercentrum-sydost/bestall-rand-36-kostnadsfritt/. Accessed 26-02-21 2021
Orwelius, L., Nilsson, M., Nilsson, E., Wenemark, M., Walfridsson, U., Lundstrom, M., … Kristenson, M. (2017). The Swedish RAND-36 health survey - reliability and responsiveness assessed in patient populations using Svensson's method for paired ordinal data. Journal of Patient Reported Outcomes, 2(1), 4. https://doi.org/10.1186/s41687-018-0030-0.
Nilsson, E., Orwelius, L., & Kristenson, M. (2016). Patient-reported outcomes in the Swedish National Quality Registers. Journal of Internal Medicine, 279(2), 141–153. https://doi.org/10.1111/joim.12409.
Aspinen, S., Kärkkäinen, J., Harju, J., Juvonen, P., Kokki, H., & Eskelinen, M. (2017). Improvement in the quality of life following cholecystectomy: A randomized multicenter study of health status (RAND-36) in patients with laparoscopic cholecystectomy versus minilaparotomy cholecystectomy. Quality of Life Research, 26(3), 665–671. https://doi.org/10.1007/s11136-016-1485-1.
de Vries, G. E., Jorritsma, W., Dijkstra, P. U., Geertzen, J. H., & Reneman, M. F. (2015). The construct validity of the short Form-36 health survey for patients with nonspecific chronic neck pain. International Journal of Rehabilitation Research, 38(2), 137–143. https://doi.org/10.1097/mrr.0000000000000102.
Fayers, P. M., & Machin, D. (2016). Quality of life : The assessment, analysis, and reporting of patient-reported outcomes third edition edn. Chichester, West Sussex: Wiley.
Scott, K. M., Tobias, M. I., Sarfati, D., & Haslett, S. J. (1999). SF-36 health survey reliability, validity and norms for new Zealand. Australian and New Zealand Journal of Public Health, 23(4), 401–406. https://doi.org/10.1111/j.1467-842x.1999.tb01282.x.
Hopman, W. M., Berger, C., Joseph, L., Towheed, T., Prior, J. C., Anastassiades, T., … Tenenhouse, A. (2009). Health-related quality of life in Canadian adolescents and young adults: Normative data using the SF-36. Canadian Journal of Public Health, 100(6), 449–452. https://doi.org/10.1007/bf03404342.
Jacobsen, E. L., Bye, A., Aass, N., Fosså, S. D., Grotmol, K. S., Kaasa, S., … Hjermstad, M. J. (2018). Norwegian reference values for the short-form health survey 36: Development over time. Quality of Life Research, 27(5), 1201–1212. https://doi.org/10.1007/s11136-017-1684-4.
Apolone, G., & Mosconi, P. (1998). The Italian SF-36 health survey: Translation, validation and norming. Journal of Clinical Epidemiology, 51(11), 1025–1036. https://doi.org/10.1016/s0895-4356(98)00094-8.
Cruz, L. N., Fleck, M. P., Oliveira, M. R., Camey, S. A., Hoffmann, J. F., Bagattini, A. M., & Polanczyk, C. A. (2013). Health-related quality of life in Brazil: Normative data for the SF-36 in a general population sample in the south of the country. Ciencia & Saúde Coletiva, 18(7), 1911–1921. https://doi.org/10.1590/s1413-81232013000700006.
Salem, S., Malouche, D., & Ben Romdhane, H. (2019). Tunisian population quality of life: A general analysis using SF-36. Eastern Mediterranean Health Journal, 25(9), 613–621. https://doi.org/10.26719/emhj.18.030.
Pappa, E., Kontodimopoulos, N., & Niakas, D. (2005). Validating and norming of the Greek SF-36 health survey. Quality of Life Research, 14(5), 1433–1438. https://doi.org/10.1007/s11136-004-6014-y.
Ohlsson-Nevo, E., & Karlsson, J. (2019). Impact of health-related stigma on psychosocial functioning in the general population: Construct validity and Swedish reference data for the stigma-related social problems scale (SSP). Research in Nursing & Health, 42(1), 72–81. https://doi.org/10.1002/nur.21924.
Ware, J. E., Snow, K. K., Kosinski, M., & Gandek, B. (1993). SF-36 health survey. Boston: Manual and Interpretation Guide New England Medical Center.
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155–159. https://doi.org/10.1037//0033-2909.112.1.155.
Gandek, B., Ware Jr., J. E., Aaronson, N. K., Alonso, J., Apolone, G., Bjorner, J., … Sullivan, M. (1998). Tests of data quality, scaling assumptions, and reliability of the SF-36 in eleven countries: Results from the IQOLA project. International quality of life assessment. Journal of Clinical Epidemiology, 51(11), 1149–1158. https://doi.org/10.1016/S0895-4356(98)00106-1.
Ware Jr., J. E., & Gandek, B. (1998). Methods for testing data quality, scaling assumptions, and reliability: The IQOLA project approach. International quality of life assessment. Journal of Clinical Epidemiology, 51(11), 945–952. https://doi.org/10.1016/s0895-4356(98)00085-7.
Cappelleri, J. C., Bushmakin, A. G., Gerber, R. A., Leidy, N. K., Sexton, C. C., Lowe, M. R., & Karlsson, J. (2009). Psychometric analysis of the three-factor eating questionnaire-R21: Results from a large diverse sample of obese and non-obese participants. International Journal of Obesity (Lond), 33(6), 611–620. https://doi.org/10.1038/ijo.2009.74.
McHorney, C. A., Ware Jr., J. E., Lu, J. F., & Sherbourne, C. D. (1994). The MOS 36-item short-form health survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Medical Care, 32(1), 40–66. https://doi.org/10.1097/00005650-199401000-00004.
Nunnally, J. C., Bernstein, I. R., & Bernstein, I. R. (1994). Psychometric theory, (3rd ed., ). New York: McGraw-Hill.
Newson, R. (2006). Confidence intervals for rank statist. Stata Journal, 6(3), 309–334. https://doi.org/10.1177/1536867x0600600302.
StataCorp (2017). Stata Statistical Software: Release 15. College Station: StataCorp LLC.
Hopman, W. M., Towheed, T., Anastassiades, T., Tenenhouse, A., Poliquin, S., Berger, C., … Papadimitropoulos, E. (2000). Canadian normative data for the SF-36 health survey. Canadian multicentre osteoporosis study research group. CMAJ, 163(3), 265–271.
Roser, K., Mader, L., Baenziger, J., Sommer, G., Kuehni, C. E., & Michel, G. (2019). Health-related quality of life in Switzerland: Normative data for the SF-36v2 questionnaire. Quality of Life Research, 28(7), 1963–1977. https://doi.org/10.1007/s11136-019-02161-5.
Taft, C., Karlsson, J., & Sullivan, M. (2001). Do SF-36 summary component scores accurately summarize subscale scores? Quality of Life Research, 10(5), 395–404. https://doi.org/10.1023/A:1012552211996.
Laucis, N. C., Hays, R. D., & Bhattacharyya, T. (2015). Scoring the SF-36 in Orthopaedics: A brief guide. The Journal of Bone and Joint Surgery American Volume, 97(19), 1628–1634. https://doi.org/10.2106/jbjs.O.00030.
Stang, A., & Jockel, K. H. (2004). Studies with low response proportions may be less biased than studies with high response proportions. American Journal of Epidemiology, 159(2), 204–210. https://doi.org/10.1093/aje/kwh009.
Waller Lidstrom, M., Wennberg, P., Lundqvist, R., Forssen, A., & Waller, G. (2017). Time trends of comparative self-rated health in adults aged 25-34 in the northern Sweden MONICA study, 1990-2014. PLoS One, 12(11), e0187896. https://doi.org/10.1371/journal.pone.0187896.
Acknowledgements
The authors are thankful to Ulf Johansson at the University Health Care Research Center, Örebro, Sweden, for support with tables and analysis.
Funding
The Research Committee of Örebro County Council supported the study. Grant number OLL-506801.
Author information
Authors and Affiliations
Contributions
The authors’ contributions were as follows: concept and design (EON, JK, MM, PN); acquisition of data (EON, JK, PN); statistical analysis and interpretation of data (EON, JK YH); manuscript writing (EON, JK, MM, PN, AH); drafting revision of the manuscript for important intellectual, content (EON, JK, MM, AH). All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Regional Ethical Review Board of Uppsala (reference number 2015/071).
Consent for publication
No data of individual patients included in this study are contained in this manuscript; hence, no consent for publication was needed.
Competing interests
No potential competing interest was reported by the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 6.
Weighted mean (SD) T-scores for the RAND-36 scales by gender and age group.
Additional file 2: Table 7.
Weighted mean (SD) T-scores for the RAND-36 scales by educational level and occupational group.
Additional file 3: Appendix 1.
Item description.
Additional file 4: Appendix 2.
RAND-36 item descriptive statistics, inter-scale, item-total (corrected for overlap), and item-other scale correlations (n = 3422).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ohlsson-Nevo, E., Hiyoshi, A., Norén, P. et al. The Swedish RAND-36: psychometric characteristics and reference data from the Mid-Swed Health Survey. J Patient Rep Outcomes 5, 66 (2021). https://doi.org/10.1186/s41687-021-00331-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41687-021-00331-z