
Abstract
Introduction
In some randomised trials, the primary interest is in the mechanisms by which an intervention exerts its effects on health outcomes. That is, clinicians and policy-makers may be interested in how the intervention works (or why it does not work) through hypothesised causal mechanisms. In this article, we highlight the value of understanding causal mechanisms in randomised trials by applying causal mediation analysis to two randomised trials of complex interventions.
Main body
In the first example, we examine a potential mechanism by which an exercise programme for rheumatoid arthritis of the hand could improve hand function. In the second example, we explore why a rehabilitation programme for ankle fractures failed to improve lower-limb function through hypothesised mechanisms. We outline critical assumptions that are required for making valid causal inferences from these analyses, and provide results of sensitivity analyses that are used to assess the degree to which the estimated causal mediation effects could have been biased by residual confounding.
Conclusion
This paper demonstrates how the application of causal mediation analyses to randomised trials can identify the mechanisms by which complex interventions exert their effects. We discuss methodological issues and assumptions that should be considered when mediation analyses of randomised trials are used to inform clinical practice and policy decisions.
Similar content being viewed by others


Introduction
The utility of randomised controlled trials (RCTs) can be extended beyond the estimation of the effects of interventions on health outcomes. In some trials, the interest is in the mechanisms through which the intervention exerts its effects on health outcomes [1]. That is, clinicians and policy-makers may be interested in how the intervention works (or fails to work) through hypothesised causal mechanisms. By identifying the mechanisms of health interventions, researchers and clinicians can refine and adapt interventions to improve the effectiveness of health interventions and guide implementation. This is particularly useful for complex interventions where several mechanisms can be hypothesised to improve health outcomes. The UK Medical Research Council advocates the inclusion of mechanistic analyses in process evaluations of complex interventions [2].
Methods for identifying mediators have been available for decades [3] but recently more rigorous methods for causal mediation analysis have been developed that are based on clearly defined assumptions [4]. To the extent that these assumptions can be met, causal mediation analysis can provide consistent estimates of the extent to which interventions work through particular mechanisms.
In this article, we highlight the value of understanding causal mechanisms in RCTs. We illustrate key concepts by applying causal mediation analyses to two RCTs in physical rehabilitation. In the first example, we examine a potential mechanism by which an exercise programme for rheumatoid arthritis of the hand improves hand function. In the second example, we explore why a rehabilitation programme for ankle fractures failed to improve lower-limb function. We highlight key assumptions and discuss how these analyses may provide clinical and policy implications that extend beyond those provided by standard analyses of RCTs.
Example of estimating mechanistic effects of an effective intervention (how did the intervention work?)
In the Strengthening And stretching for Rheumatoid Arthritis of the Hand Trial (SARAH) trial (n = 490), Lamb et al. [5] showed that an exercise programme for people with rheumatoid arthritis improved hand function more than usual care (total effect = 4.4 [95% confidence interval (CI), 1.5–7.2] points on the 100-point Michigan Hand Outcome Questionnaire at 12 months). After the trial was completed, causal mediation analysis was used to determine how much of the intervention effect was mediated by increases in grip strength. A causal mediation analysis of complete cases (n = 387) indicated that 25% of the intervention effect on hand function at 12 months was mediated by increases in grip strength at 4 months (indirect effect = 1.1 [0.3–2.1]). This indicates that exercise improves hand function partly by increasing hand strength. The analysis also suggests that a substantial proportion of the total intervention effect is mediated through other pathways (represented by the direct effect of 3.3 [0.5–6.3]). Future research might seek to identify these alterative mechanisms with the aim of further refining the intervention.
Example of estimating mechanistic effects of an ineffective intervention (why didn't the intervention have a meaningful effect on the primary outcome?)
In the EXercise or Advice after ankle fracture trial (EXACT) trial (n = 214), Moseley et al. [6] tested whether a rehabilitation programme with advice was more effective at improving lower-limb function than advice alone for patients with ankle fracture. A hypothesised mechanism was that rehabilitation would increase physical activity levels, which in turn would improve lower-limb function. In contrast to the SARAH trial, the primary analysis of the EXACT trial did not find evidence of an intervention effect on the primary outcome (total effect = − 0.5 [− 5.0–3.8] on the 80-point Lower Extremity Functional Scale at 3 months). Here the question of interest is why the intervention did not have a meaningful effect on the primary outcome. A causal mediation analysis of complete cases (n = 156) found no evidence that physical activity at 1 month influenced function at 3 months (indirect effect = − 0.4 [− 2.1–1.0]). The analysis suggested that, while a change from low to high physical activity would improve lower-limb function by 8.7 points [2.2–15.3], the rehabilitation programme failed to increase physical activity (ratio of odds of being classified as low physical activity = 0.9 [0.6–1.2]). This indicates that although the EXACT investigators identified an important intervention target (physical activity), the rehabilitation programme failed to cause a sufficient change in this target mechanism. This implies that it might be possible to produce functional gains if physical activity levels could be increased using other interventions. These findings could guide the development of new interventions in this population.
Methodological considerations
As with any causal modelling, the estimates derived from a causal mediation analysis may not be interpretable as causal effects if the underlying assumptions are not met. In the following sections we outline some important assumptions and discuss them within the contexts of the SARAH and EXACT trials.
Exchangeability
A critical requirement for robust inference of indirect and direct effects is to satisfy the exchangeability (no-confounding) assumption for the intervention-mediator, intervention-outcome and mediator-outcome effects [4, 7]. In an RCT, the intervention-mediator and intervention-outcome effects can be assumed to be unconfounded because trial participants are randomised to intervention or control conditions. However, the mediator-outcome effect can be confounded because the mediator is not randomised.
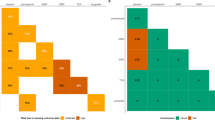
After adjusting for measured confounders, sensitivity analyses can be used to assess the degree to which the estimated effects could have been biased by residual confounding. For the SARAH trial, sensitivity plots (Fig. 1) show that a moderate level of residual confounding of the mediator-outcome effect would invalidate the indirect effect. This is apparent because the average indirect effect (on the vertical axis) diminishes to 0 when the sensitivity parameter (on the horizontal axis) shifts from 0 (no residual confounding) to 0.30 (moderate residual confounding). In contrast, the sensitivity analysis plots of the EXACT trial shows that the indirect effect would be stable even if there were moderate levels of residual confounding. These sensitivity analyses suggest that the findings of the causal mediation analysis were robust for the EXACT trial but not for the SARAH trial. Researchers conducting causal mediation analyses should always make the no-confounding assumption explicit and report sensitivity analyses. Readers of reports of causal mediation analyses should be aware of the potential impact of residual confounding when interpreting mediation analyses of RCTs.

Causal models of intervention mechanisms, effect decomposition, and sensitivity plots of the SARAH and EXACT trials. The causal models panel shows the hypothesised mechanisms of each intervention. The blue lines represent the effect of the intervention on the outcome through the mediator of interest (indirect effect); the green line represents the effect of the intervention on the outcome that is not exerted through the mediator (direct effect) which includes all other possible mechanisms; and the black lines represent possible confounding effects that were adjusted for in the analysis. Each model assumes that the intervention does not modify the mediator-outcome effect. The effect decomposition panel shows how the average total effect of the intervention on the outcome is decomposed into the indirect effect (blue lines in the causal models), and the direct effect (green lines). These effects are presented as unstandardised effects with their 95% confidence intervals. The sensitivity plots show how much the estimated indirect effect would change if there was residual confounding of the mediator-outcome effect. The sensitivity parameter (horizontal axis) represents hypothesised levels of residual confounding: 0 indicates no residual confounding, and − 1.0 and 1.0 are the maximum levels of residual confounding. The dashed horizontal line represents the estimated indirect effect when there is no residual confounding (sensitivity parameter = 0). The curved solid line represents the estimated indirect effect at varied levels of residual confounding. In the SARAH trial, the indirect effect estimate would become 0 if there was moderate residual confounding (sensitivity parameter = 0.30), whereas in the EXACT trial, the indirect effect is stable across levels of residual confounding. The grey zones represent 95% confidence intervals
In some situations, it might also be important to consider interactions between the intervention and confounder(s), and between the mediator(s) and confounder(s), to strongly control for confounding. However, unless there is substantial prior knowledge to believe that exposure-confounder or mediator-confounder interactions will confound the mediator-outcome effect, it may be sufficient to control only for the main effects of the confounders [4]. In SARAH and EXACT, we assumed that there would not be large interaction effects between the interventions and confounders, and between the mediators and confounders. So we only controlled for the main effects of the confounders.
The intervention should not have a causal effect on confounders of the mediator-outcome effect
It is important that the intervention is not a cause of confounders of the mediator-outcome effect. In SARAH and EXACT, the confounders were measured before the intervention was delivered, and, therefore, the confounders cannot be caused by the intervention. However, it is possible that there are other unmeasured variables caused by the intervention that could confound the mediator-outcome effect. These variables were not specified in our causal models and therefore did not inform our analysis.
Effect modification
In RCTs, it is possible that the effect of a mediator on an outcome could depend on treatment allocation. In other words, allocation may modify the effect of the mediator on the outcome. In the SARAH trial, the effect of grip strength on functional outcomes could depend on whether allocation was to the exercise programme or usual care. Likewise, in the EXACT trial, the effect of physical activity on lower-limb function could depend on whether allocation was to rehabilitation or advice only. When effect modifications are plausible, it is important to account for an intervention-mediator interaction term when specifying the causal model [4]. In practice, including the interaction term will produce indirect and direct effects that are conditional on intervention status. These conditional effects may differ from the average (marginal) effects in the entire population if there is effect modification. In both SARAH and EXACT, the estimated conditional effects were not substantially different from the marginal indirect and direct effects (Additional file 1).
Consistency
To make valid causal inferences from mediation analyses, the intervention and mediator must be well-defined [8]. This means that there cannot be multiple versions of the intervention and mediator implemented in the study [9]. In the technical literature, this requirement is often called the consistency assumption [10]. When the consistency assumption is violated and there are multiple versions of the intervention or mediator, interpretation of mediation effects becomes challenging [9].
In the EXACT trial, the challenge is to specifically define what is meant by the proposed mediator, physical activity level; and to articulate the level at which this mediator is fixed when we define our effects of interest. In EXACT, physical activity was classified as ‘low’ or ‘high’ based on metabolic equivalent minutes per week (precise definitions outlined in Additional file 1). In our definition of the indirect effect, we set physical activity to the level taken when individuals are allocated to receive rehabilitation, and the level taken when allocated to advice alone. In our definition of the direct effect, we fixed physical activity to the level taken when allocated to receive rehabilitation. We must assume that all possible versions of the intervention that could set physical activity to a given level will have the same effect on the outcome, lower-limb function. This assumption is at best only approximately satisfied in the EXACT trial.
In the SARAH trial, the consistency assumption concerns the grip-strength mediator. We must assume that, to the extent that there are multiple ways of bringing about change in grip strength, they all have the same effects on lower-limb function. Vanderweele (2012) explains that when consistency is violated and there are multiple versions of the mediator, the indirect effect is likely to be underestimated and the direct effect is likely to be overestimated [9].
Conclusion
Causal mediation analyses can identify the mechanisms by which health interventions exert their effects. This information can be used to emphasise and refine components of the intervention that operate through effective mechanisms and discard components of the intervention that target ineffective mechanisms. Clinicians and policy-makers could use the findings from causal mediation analyses of RCTs to prioritise critical aspects of multi-component interventions during implementation. Finally, causal mediation analyses can identify which mechanisms failed when promising interventions are found to be ineffective.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- EXACT:
-
EXercise or Advice after ankle fracture trial
- RCT:
-
Randomised controlled trial
- SARAH:
-
Strengthening And stretching for Rheumatoid Arthritis of the Hand Trial
References
Emsley R, Dunn G, White IR. Mediation and moderation of treatment effects in randomised controlled trials of complex interventions. Stat Methods Med Res. 2010;19(3):237–70.
Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ. 2015;350:h1258.
Judd CM, Kenny DA. Process analysis: estimating mediation in treatment evaluations. Eval Rev. 1981;5(5):602–19.
VanderWeele TJ. Explanation in causal inference: methods for mediation and interaction. Oxford: Oxford University Press; 2015.
Lamb SE, Williamson EM, Heine PJ, Adams J, Dosanjh S, Dritsaki M, et al. Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. Lancet. 2015;385(9966):421–9.
Moseley AM, Beckenkamp PR, Haas M, Herbert RD, C-WC L. Rehabilitation after immobilization for ankle fracture. JAMA. 2015;314(13):1376.
Keele L. Causal mediation analysis: Warning! Assumptions ahead. Am J Eval. 2015;36(4):500–13.
Hernán MA, Taubman SL. Does obesity shorten life? The importance of well-defined interventions to answer causal questions. Int J Obes. 2008;32:S8–14.
Vanderweele TJ. Mediation analysis with multiple versions of the mediator. Epidemiology. 2012;23(3):454–63.
VanderWeele TJ, Hernan MA. Causal inference under multiple versions of treatment. J Causal Inference. 2013;1(1):1–20.
Acknowledgements
We are thankful to the SARAH and EXACT trial team members for sharing data. HL had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. We are thankful to Dr. Alix Hall for verifying the analysis code.
Funding
HL and RH’s research fellowships are funded by the Australian National Health and Medical Research Council. HL and SL are supported by funding from the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care Oxford at Oxford Health NHS Foundation Trust. SL is supported by funding from the National Institute for Health Research Biomedical Research Centre at the Oxford Universities Hospital NHS Trust.
Author information
Authors and Affiliations
Contributions
All authors were involved in the concept and design of the study. HL wrote the first draft of the manuscript, and all authors contributed to subsequent revisions of the manuscript and approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
EXACT trial – the trial was approved by the Hawkesbury Human Research Ethics Committee of Northern Sydney Central Coast Health (1006234 M); SARAH trial – the trial was approved by the Oxford C Multicentre Research Ethics Committee (REC 08/H0606/47).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Indirect and direct effects that are conditional on intervention status. Physical activity level cutpoints. Annotated bibliography. (DOCX 338 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lee, H., Herbert, R.D., Lamb, S.E. et al. Investigating causal mechanisms in randomised controlled trials. Trials 20, 524 (2019). https://doi.org/10.1186/s13063-019-3593-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-019-3593-z