
Abstract
Background
The interactive effect of cumulative input and output on achieving optimal fluid balance has not been well elucidated in patients with acute kidney injury (AKI) requiring continuous renal replacement therapy (CRRT). This study evaluated the interrelation of fluid components with mortality in patients with AKI requiring CRRT.
Methods
This is a retrospective observational study conducted with a total of 258 patients who were treated with CRRT due to AKI between 2016 and 2018 in the intensive care unit of Ewha Womans University Mokdong Hospital. The amounts of fluid input and output were assessed at 24-h and 72-h from the initiation of CRRT. The study endpoints were 7- and 28-day all-cause mortality.
Results
The mean patient age was 64.7 ± 15.8 years, and 165 (64.0%) patients were male. During the follow-up, 7- and 28-day mortalities were observed in 120 (46.5%) and 157 (60.9%) cases. The patients were stratified into two groups (28-day survivors vs. non-survivors), and the cumulative fluid balances (CFBs) at 24 h and 72 h were significantly higher in the 28-day non-survivors compared with the survivors. The increase in 24-h and 72-h CFB was significantly associated with an increase in 7- and 28-day mortality risks. To examine the interactive effect of cumulative input or output on the impact of CFB on mortality, we also stratified patients into three groups based on the tertile of 24-h and 72-h cumulative input or output. The increases in 24-h and 72-h CFBs were still significantly related to the increases in 7-day and 28-day mortality, irrespective of the cumulative input. However, we did not find significant associations between increase in 24-h and 72-h CFB and increase in mortality risk in the groups according to cumulative output tertile.
Conclusions
The impact of cumulative fluid balance on mortality might be more dependent on cumulative output. The physicians need to decrease the cumulative fluid balance of CRRT patients as much as possible and consider increasing patient removal.
Similar content being viewed by others

Background
Fluid overload has been associated with aggravating renal dysfunction, an increase in length of intensive care unit (ICU) stay, and an elevation in mortality risk [1,2,3,4]. Hence, negative fluid balance is regarded as an essential strategy to improve survival rates in critically ill patients, and continuous renal replacement therapy (CRRT) has been widely used for fluid regulation in critically ill patients with acute kidney injury (AKI) [5,6,7]. However, there is no consensus on the optimal fluid management for such patients [8,9,10,11,12]. Several recent studies revealed that an increase of cumulative fluid balance (CFB) was significantly associated with an increase in mortality risk in critically ill patients [13,14,15,16,17], while Balakumar et al. showed that both positive and negative fluid balance were associated with higher mortality rates compared with even fluid balance [18]. Furthermore, Silversides et al. reported that active removal of fluid using RRT in critically ill patients was associated with less survival benefit compared with standard care [19,20,21].
Fluid resuscitation for critically ill patients with AKI has both advantages and disadvantages. Fluid resuscitation can help keep patients hemodynamically stable, maintain renal perfusion, and prevent further ischemic injury due to ongoing renal dysfunction. However, accumulating interstitial fluid hinders oxygen delivery to cells from blood vessels and can lead to renal ischemia and multi-organ failure [9, 12, 22]. Thus, optimal management of fluid balance in patients with AKI, especially those requiring CRRT, still needs to be investigated. In addition, most physicians have focused on CFB, even though CFB is determined by the amount of input and output. However, there is still no definite answer for which strategies better benefit survival: does higher output translate into better clinical outcomes, or does lower input translate into better clinical outcomes. Therefore, in this study, we investigated the association between CFB, cumulative input and output amounts at 24-h and 72-h after initiation of CRRT, and mortality risk among patients with AKI receiving CRRT.
Methods
Study population
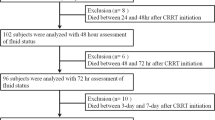
We conducted a retrospective review of patients aged 18 years or older who were treated with CRRT due to AKI between 2016 and 2018 in the ICU of Ewha Womans University Mokdong Hospital. A total 330 patients were initially screened. Exclusion criteria included patients with end-stage renal disease (ESRD) on chronic dialysis or those who underwent kidney transplantation, patients who died within 24-h immediately after CRRT initiation, and patients with missing fluid status data. Finally, a total of 258 patients with 24-h assessment of fluid status and 191 patients with 72-h assessment of fluid status were analyzed (Additional file 1: Figure S1). All the enrolled patients received CRRT management for longer than 24-h. This study was approved by the Institutional Review Board of Ewha Womans University, College of Medicine (IRB No. EUMC 2018-11-019). The need for informed consent from patients was waived because of the retrospective study design. All clinical investigations were conducted in accordance with 2013 Declaration of Helsinki guidelines.
Data collection
Baseline characteristics of the enrolled patients were collected at the time of CRRT initiation, including age, sex, body mass index (BMI), cause of AKI, systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), comorbidities (hypertension, diabetes mellitus, cardiovascular disease, malignancy), Charlson Comorbidity Index (CCI), Sequential Organ Failure Assessment (SOFA) score, Acute Physiology and Chronic Health Evaluation (APACHE) II score, and Glasgow Coma Score (GCS). In addition, the needs for mechanical ventilation and fraction of inspired oxygen (FiO2) were investigated, and the prescriptions for CRRT including target clearance, dialysate flow rate, replacement flow rate, and use of anticoagulation were also assessed. Laboratory data were collected at the initiation of CRRT, and estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease equation [23]. The definition of AKI, based on the Kidney Disease: Improving Global Outcomes clinical practice guidelines for AKI, was the presence of at least one of the following criteria: (1) an increase in serum creatinine level ≥ 0.3 mg/dL within 48-h, (2) an increase in serum creatinine level to ≥ 1.5 times the baseline level that was known or presumed to have occurred within the previous 7 days, or (3) urine volume < 0.5 mL/kg/h for 6-h [24].
CRRT protocol
The decision to initiate CRRT and the CRRT settings for target clearance; blood flow, dialysate, and replacement fluid rates; and anticoagulation administration were determined through discussion and consultation with nephrologists [25]. The criteria for CRRT initiation were medically intractable or persistent electrolyte imbalance and/or metabolic acidosis and decreased urine output with volume overload and/or progressive azotemia. Hemodynamic instability was also an important indication. Generally, vascular access for CRRT was via a femoral venous catheter, and the pre-dilution method of continuous venovenous hemodiafiltration was usually performed. After CRRT initiation, attending physicians and experienced nurses monitored body weight, urine output, laboratory results, actual delivered dose, and the hemodynamic status of the patients and discussed the results with nephrologists to maintain CRRT adequacy.
Fluid status assessment
The amounts of cumulative fluid input and output were assessed for 24-h and 72-h from the initiation of CRRT, and the CFB was calculated as cumulative input − cumulative output. We also investigated the type of infused fluid, including 0.9% sodium chloride, 0.45% sodium chloride, dextrose, plasma solution, lactate Ringer’s solution, 20% albumin, and enteral nutritional fluid, and compared the administered type between the 28-day survivors and non-survivors.
Statistical analysis
Patients were stratified into two groups: 28-day survivors vs. non-survivors. The baseline characteristics of the groups were compared using the independent t-test for continuous variables and the chi-squared test for categorical variables. Continuous variables are presented as the mean ± standard deviation, and categorical variables are presented as numbers and percentages. The non-normally distributed variables were expressed as medians (25th–75th percentiles) and were compared using the Mann-Whitney U or Kruskal-Wallis test. The study endpoints were all-cause mortality on the 7- and 28-day time points after commencing CRRT, and Cox proportional hazard analyses were performed to examine the effects of CFB on mortality. Significant covariates were identified by univariable analysis (P < 0.05), and the clinically important variables were selected for multivariable analysis. Age, sex, BMI, CCI, medical history, and eGFR at CRRT initiation were adjusted for multivariable Cox proportional regression analyses, as were the MAP, hemoglobin, SOFA score, use of vasopressor, and type of fluid administration at each time point (24-h and 72-h from CRRT start). Before investigating the interactive effect of cumulative input or output on the impact of CFB on mortality, multicollinearity between CFB and cumulative input or output was assessed based on the variance inflation factor (VIF). However, we found that the VIF was too large to adjust the cumulative input or output to show the effect of CFB on mortality risk, so we decided to analyze the effect of cumulative input and output on the impact of CFB on mortality after stratifying the patients. Thus, we stratified patients into three groups based on the tertile of 24-h and 72-h cumulative input or output and investigated the impact of CFB on the mortality in each group. All statistical tests were conducted using a two-tailed 95% confidence interval (CI), and a P value of less than 0.05 was considered statistically significant. All descriptive and survival analyses were performed using SPSS for Windows, version 23.0 (IBM, Armonk, NY, USA) and R software version 3.3.1 (R Development Core Team, Vienna, Austria).
Results
Baseline characteristics and clinical parameters at the time of CRRT initiation
The baseline characteristics and clinical and laboratory parameters at baseline are shown in Tables 1 and 2. The mean patient age was 64.7 ± 15.8 years, and 165 patients (64.0%) were male. The primary cause of AKI was sepsis (n = 157, 60.9%) followed by ischemic injuries (n = 52, 20.2%). Among the total 258 patients, 157 patients (61%) died within 28 days after CRRT initiation. The patients were stratified into two groups, the 28-day survivors and the non-survivors. The SOFA, APACHE II score, and the need for mechanical ventilation were significantly higher in the 28-day non-survivors than in the survivors. Moreover, there was significantly more malignancy in the non-survivors compared with the survivors, while the survivors had significantly more hypertension compared with non-survivors (Table 1). Furthermore, the mean SBP and MAP were significantly higher in the survivors compared with the non-survivors. The mean platelet counts were significantly increased in the survivors compared with the non-survivors, whereas the mean total bilirubin level was significantly decreased in the survivors. There were no significant differences in the type of fluid administration or replacement of 20% albumin between the two groups, but the survivors received more enteral nutritional fluid than the non-survivors. The prescriptions for CRRT did not differ between two groups except for CRRT duration, which was longer in the survivors (Table 2). We further compared clinical parameters between the two groups at 24-h and 72-h after CRRT initiation, respectively (Additional file 1: Table S1 and S2). The SOFA and APACHE II scores, and need for mechanical ventilation were significantly higher in the non-survivors than the survivors at both 24-h and 72-h assessment after CRRT initiation. Furthermore, the mean MAP and platelet counts were lower, whereas white blood cell counts and total bilirubin levels were higher in the non-survivors compared to the survivors at both 24-h and 72-h assessment after CRRT initiation.
Change of CFB and cumulative input and output in survivors and non-survivors
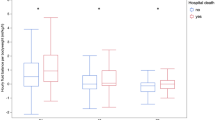
We assessed the CFB and total cumulative input and output at 24-h and 72-h after initiation of CRRT, and Fig. 1 shows the change in each status. In the non-survivors, the CFBs at each time point were significantly higher than that in the survivors. In contrast, the total cumulative inputs at each time point were also higher in the non-survivors compared with that in the survivors, but a statistically significant difference was seen only at 48-h after CRRT start, while the total cumulative outputs at each time point were significantly lower in the non-survivors than those in the survivors.

Comparison of fluid balance (a), total intake (b), and total output (c) between 28-day survivor vs. non-survivor. Each group was compared by two-way ANOVA, *P < 0.001, #P = 0.03. CRRT, continuous renal replacement therapy
The effect of CFB on mortality risk
We next investigated the impact of 24- and 72-h CFB on 7- and 28-day mortality risk. Univariable Cox proportional hazard analysis showed that increased CFB at 24- and 72-h was significantly associated with an increase in 7-day mortality risk [increase of 1 L per 24-h CFB; hazard ratio (HR) = 1.15, 95% confidence interval (CI) = 1.09–1.22, and an increase of 1 L per 72-h CFB; HR = 1.12, 95% CI = 1.07–1.16] and 28-day mortality risk [increase of 1 L per 24-h CFB; HR = 1.14, 95% CI = 1.08–1.20 and increase of 1 L per 72-h CFB; HR = 1.10, 95% CI = 1.06–1.14]. Moreover, the increase of CFB at each time point was still significantly related to the elevation of 7-day mortality rate [increase of 1 L per 24-h CFB; HR = 1.14, 95% CI = 1.06–1.22 and increase of 1 L per 72-h CFB; HR = 1.10, 95% CI = 1.05–1.15] and 28-day mortality rate [increase of 1 L per 24-h CFB; HR = 1.11, 95% CI = 1.04–1.18 and increase of 1 L per 72-h CFB; HR = 1.07, 95% CI = 1.03–1.12], even after adjusting for confounding factors (Table 3 and Fig. 2).

Cubic spline plots for the 7- or 28-day mortality risks according to 24-h (a, b) and 72-h (c, d) cumulative fluid balance. Black lines = hazard ratios, dotted lines = 95% confidence intervals
The interactive effect of cumulative input and output on the impact of CFB on mortality
We stratified the patients into three groups based on the tertile of 24-h and 72-h cumulative input or output. The baseline characteristics of each group are shown in Additional file 1: Table S3. The patients in the higher input tertile were younger and showed higher baseline eGFR levels and SOFA scores than those in the lowest tertile at both 24-h and 72-h assessment after CRRT initiation. However, output tertile groups showed no significant differences in clinical characteristics, including blood pressure, comorbidity status, and SOFA scores at either 24-h or 72-h assessment after CRRT initiation. We then investigated the impact of CFB on the mortality in each group. Increases in 24-h CFB were significantly associated with the increase in 7- and 28-day mortality risks irrespective of the cumulative input, even after adjusting for age, sex, BMI, MAP, CCI, history of diabetes and hypertension, hemoglobin, eGFR, SOFA score, use of vasopressors, and type of fluid administration (Table 4 and Fig. 3). Moreover, the increases in 72-h CFB were also significantly related to the increase in 7- and 28-day mortality risk regardless of cumulative input, except for the T2 group for 7-day mortality. However, we did not find significant associations between the increase in 24- and 72-h CFB and 7- and 28-day mortality risk in the groups stratified according to cumulative output tertile. Instead, CFB was significantly related to an increase in 7- and 28-day mortality risk only in the T2 group of the 24-h cumulative output, and the T1 group of the 72-h cumulative output. Taken together, we surmise that the impact of CFB on mortality might be dependent on cumulative output (Table 4).

Comparison of adjusted hazard ratios for 7-day or 28-day mortality according to 24-h (a, b) or 72-h (c, d) cumulative fluid balance stratified with tertiles of total input and output. T1–3 represents tertile groups of total input and output. The exact values of T1–3 are presented in Table 4. Models were adjusted for age, sex, body mass index, mean arterial pressure, Charlson comorbidity index, history of diabetes and hypertension, hemoglobin, baseline estimated glomerular filtration rate, Sequential Organ Failure Assessment score, use of vasopressor, and type of fluid administration. Mean arterial pressure, hemoglobin, Sequential Organ Failure Assessment score, use of vasopressor use, and type of fluid administration at each of baseline and 72-h after CRRT initiation were used for adjustment in 24-h and 72 h-cumulative fluid balance models, respectively. *P < 0.05, **P < 0.01, ***P < 0.001. CRRT, continuous renal replacement therapy
Discussion
This study shows the effects of cumulative input and output on the impact of short-term (24-h) and relatively long-term (72-h) CFB on 7- and 28-day mortality risk among AKI patients undergoing CRRT. We found that both increases in short-term and longer-term CFB were significantly associated with increases in 7- and 28-day mortality risk, and the effect of CFB on mortality might be dependent on cumulative output.
The main concern in AKI patients undergoing CRRT is how to control their volume status [26, 27]. Several studies have examined this issue, and almost all suggested that fluid overload was significantly associated with increased mortality risk as well as aggravation of kidney function [2, 16, 28]. Although most studies have focused on a negative fluid balance in AKI patients with CRRT, physicians need to consider volume resuscitation, since it is crucial to restore and maintain hemodynamic stability in critically ill patients [29,30,31,32]. To reduce CFB, physicians need to choose low fluid resuscitation and high removal of resuscitation as much as possible. We stratified the patients in this study into three groups based on 24-h and 72-h cumulative input or output tertiles to reveal the interactive effect of cumulative input or output on the impact of CFB on mortality. We found a big VIF between CFB and cumulative input/output, respectively, and it was difficult to adjust cumulative input and output to show the impact of CFB on mortality risk, independently. We also found that the increase in CFB was still significantly associated with an increase in mortality risk irrespective of the stratification of cumulative input, which suggests that removal of more fluid output may reduce the mortality risk. In contrast, when we performed Cox analysis for mortality after patients were stratified based on cumulative output, there was no significant association between CFB increase and mortality risk, which means that reduction of cumulative input might not decrease mortality risk.
Moreover, we also investigated the characteristics of the three patient groups stratified by their cumulative input and output at 24-h and 72-h after CRRT initiation (Additional file 1: Table S3). Especially, there were no significant differences in MAP, CCI, and SOFA scores among the three groups stratified by output amount, suggesting that fluid removal might be done irrespective of illness severity. Therefore, we do not think a higher rate of fluid removal is simply a marker of lower illness severity. Instead, more fluid removal could provide an indirect benefit against the oxygen-mismatched diffusion and distorted tissue architecture that originate from fluid overload and tissue edema. Taken together, we suggest that physicians need to pay closer attention to decreasing CFB, especially by increasing fluid removal, to improve the clinical outcomes of their AKI patients receiving CRRT.
Adequate fluid resuscitation is essential to restore tissue perfusion in critically ill patients with AKI [27, 33, 34], and fluid administration contributes to improve glomerular filtration [9]. Moreover, fluid administration is aimed to restore systemic blood pressure, a major determinant of renal perfusion pressure and cardiac output [35,36,37]. In particular, patients with severe sepsis need adequate fluid resuscitation within 1 to 3 h of disease onset to overcome their hemodynamically unstable state [38, 39]. Thus, clinicians may try to administer more fluid to restore tissue perfusion and to improve disease course. However, fluid overload and tissue edema physiologically result in impaired diffusion of oxygen and metabolites, distorted tissue architecture, obstruction of capillary blood flow or lymphatic drainage, and disturbed cell-cell interactions. These processes subsequently contribute to progressive organ dysfunction. The patients in the current study were more likely to be overhydrated at CRRT start, and their severity scores (SOFA and APACHE II score) were higher than those in other studies [25, 40]. Thus, more removal of patient output seems to be more effective for a decrease in mortality compared with lower cumulative input, and interpretation of the current study should be made with caution. Generally, most AKI patients who require CRRT are critically ill and in an overhydrated condition [27, 41]. Moreover, effective circulating volume appears to be low in these patients [8]. Thus, we surmise that it might be more helpful to increase fluid removal than to decrease input. Furthermore, Murugan et al. [42] recently showed that higher ultrafiltration intensity (> 25 mL/kg/day) was associated with lower risk for mortality compared with lower ultrafiltration intensity (≤ 20 mL/kg/day) among critically ill patients with fluid overload who were undergoing CRRT. The authors suggested several reasons for the benefit of intensive removal. First, increase in cumulative output may reduce the risk of subsequent edema-related organ dysfunction [43]. Second, the increase in cumulative output by intensive net ultrafiltration may lead to better clearance of unknown molecules and contribute to better survival independently of fluid balance [44].
There are several limitations in the current study. First, this study was a retrospective study conducted in a single center with a relatively small sample size. Thus, selection bias was not completely avoidable, and these results may not be applicable to other ethnicities. Nevertheless, we assessed the power of our study sample size, and it was more than 80%, showing the robustness of our study sample size (Additional file 1: Table S4). In addition, previous studies with AKI patients undergoing CRRT were performed with sample sizes similar to ours [3, 45]. Moreover, this is the first study, to the best our knowledge, to reveal the interactive effect of fluid input and output in managing fluid balance for CRRT-treated AKI patients, so it can serve as precedent research for future prospective interventional studies with more patients that are needed to verify our study results. Second, we could not measure the effects of diet or drugs used or insensible water loss. However, most of these patients could not eat and nutritional support was provided via an infused solution for 72-h from CRRT start [only 28 (10.9%) patients were supplied with enteral nutritional fluid]. Third, physicians wanted to increase mechanical fluid removal when their patients could endure the increase in fluid removal, suggesting that patients whose removal was increased would experience better clinical outcomes. Several studies investigating the effect of fluid overload on mortality in critically ill patients have been performed, and most of these studies showed that a high CFB was significantly associated with increased mortality risk. However, it seems to be a case of the chicken and the egg. It can be difficult to increase fluid removal when patients are hemodynamically unstable, which suggests that greater illness severity, rather than increased CFB might be leading to worse clinical outcomes. In this study, however, we tried to adjust the severity indices, such as MAP, CCI, and SOFA score, to exclude the effect of those factors on mortality and we found that high CFB was still significantly related to an increase in 7- and 28-day mortality independently of the severity indices. Taken together, we surmise that fluid removal itself might provide an indirect benefit for clinical outcomes by improving tissue oxygenation, not just that a higher rate of fluid removal is a marker of lower severity of illness. Fourth, we arbitrarily stratified these patients into three groups based on cumulative input and/or output to examine the interaction of input and/or output on CFB impact on mortality. However, we investigated the interaction between CFB and cumulative input and output and found that VIF was too large to be adjusted with CFB. Thus, we decided to analyze the effect of cumulative input and output on the impact of CFB on mortality after stratifying the patients. Finally, we used eGFR as a marker of the patients’ renal function status, even though it is not a valid reflection of renal function in an acute setting. In this study, we could not have evaluated baseline kidney function with gold standard methods for GFR measurement such as inulin clearance, so we only used calculated eGFR values with MDRD equation. Further study is needed to accurately compare baseline kidney function measured by gold standard methods. Despite these limitations, this study reports robust clinical findings for the effect of an increase in short-term and longer-term CFB on mortality risk and the dependence of CFB on cumulative output.
Conclusions
In conclusion, an increase in CFB was significantly associated with an increase in mortality risk in AKI patients undergoing CRRT, irrespective of cumulative period. Moreover, the impact of CFB on mortality might be dependent on cumulative output. Although a prospective interventional study with a larger number of patients will be needed, this study revealed that physicians need to decrease the CFB of CRRT patients as much as possible and to consider increasing the amount of fluid removal.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- AKI:
-
Acute kidney injury
- APACHE:
-
Acute Physiology and Chronic Health Evaluation
- BMI:
-
Body mass index
- CCI:
-
Charlson Comorbidity index
- CFB:
-
Cumulative fluid balance
- CRRT:
-
Continuous renal replacement therapy
- DBP:
-
Diastolic blood pressure
- eGFR:
-
Estimated glomerular filtration rate
- ESRD:
-
End-stage renal disease
- FiO2 :
-
Fraction of inspired oxygen
- GCS:
-
Glasgow Coma Score
- ICU:
-
Intensive care unit
- IRB:
-
Institutional Review Board
- MAP:
-
Mean arterial pressure
- SBP:
-
Systolic blood pressure
- SOFA:
-
Sequential Organ Failure Assessment
- VIF:
-
Variance inflation factor
References
Payen D, de Pont AC, Sakr Y, Spies C, Reinhart K, Vincent JL. A positive fluid balance is associated with a worse outcome in patients with acute renal failure. Crit Care. 2008;12(3):R74.
Bouchard J, Soroko SB, Chertow GM, Himmelfarb J, Ikizler TA, Paganini EP, Mehta RL. Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney Int. 2009;76(4):422–7.
Kim IY, Kim JH, Lee DW, Lee SB, Rhee H, Seong EY, Kwak IS, Song SH. Fluid overload and survival in critically ill patients with acute kidney injury receiving continuous renal replacement therapy. PLoS One. 2017;12(2):e0172137.
Moore PK, Hsu RK, Liu KD. Management of acute kidney injury: core curriculum 2018. Am J kidney Dis. 2018;72(1):136–48.
Ricci Z, Ronco C, D'Amico G, De Felice R, Rossi S, Bolgan I, Bonello M, Zamperetti N, Petras D, Salvatori G, et al. Practice patterns in the management of acute renal failure in the critically ill patient: an international survey. Nephrol Dial Transplant. 2006;21(3):690–6.
Wald R, McArthur E, Adhikari NK, Bagshaw SM, Burns KE, Garg AX, Harel Z, Kitchlu A, Mazer CD, Nash DM, et al. Changing incidence and outcomes following dialysis-requiring acute kidney injury among critically ill adults: a population-based cohort study. Am J Kidney Dis. 2015;65(6):870–7.
Park S, Lee S, Jo HA, Han K, Kim Y, An JN, Joo KW, Lim CS, Kim YS, Kim H, et al. Epidemiology of continuous renal replacement therapy in Korea: results from the National Health Insurance Service claims database from 2005 to 2016. Kidney Res Clin Pract. 2018;37(2):119–29.
Perner A, Prowle J, Joannidis M, Young P, Hjortrup PB, Pettila V. Fluid management in acute kidney injury. Intensive Care Med. 2017;43(6):807–15.
Prowle JR, Echeverri JE, Ligabo EV, Ronco C, Bellomo R. Fluid balance and acute kidney injury. Nat Rev Nephrol. 2010;6(2):107–15.
Bart BA, Goldsmith SR, Lee KL, Givertz MM, O'Connor CM, Bull DA, Redfield MM, Deswal A, Rouleau JL, LeWinter MM, et al. Ultrafiltration in decompensated heart failure with cardiorenal syndrome. N Engl J Med. 2012;367(24):2296–304.
Ronco C, Bellomo R, Ricci Z. Hemodynamic response to fluid withdrawal in overhydrated patients treated with intermittent ultrafiltration and slow continuous ultrafiltration: role of blood volume monitoring. Cardiology. 2001;96(3–4):196–201.
Rosenberg AL, Dechert RE, Park PK, Bartlett RH. Review of a large clinical series: association of cumulative fluid balance on outcome in acute lung injury: a retrospective review of the ARDSnet tidal volume study cohort. J Intensive Care Med. 2009;24(1):35–46.
Dos Santos TOC, Oliveira MAS, Monte JCM, Batista MC, Pereira Junior VG, Dos Santos BFC, Santos OFP, Durao Junior MS. Outcomes from a cohort of patients with acute kidney injury subjected to continuous venovenous hemodiafiltration: the role of negative fluid balance. PLoS One. 2017;12(4):e0175897.
Sakr Y, Rubatto Birri PN, Kotfis K, Nanchal R, Shah B, Kluge S, Schroeder ME, Marshall JC, Vincent JL. Higher fluid balance increases the risk of death from sepsis: results from a large international audit. Crit Care Med. 2017;45(3):386–94.
Neyra JA, Li X, Canepa-Escaro F, Adams-Huet B, Toto RD, Yee J, Hedayati SS. Cumulative fluid balance and mortality in septic patients with or without acute kidney injury and chronic kidney disease. Crit Care Med. 2016;44(10):1891–900.
Wang N, Jiang L, Zhu B, Wen Y, Xi XM. Fluid balance and mortality in critically ill patients with acute kidney injury: a multicenter prospective epidemiological study. Crit Care. 2015;19:371.
Eun Jung K, Chul Ho C, Moo Yong P, Soo Jeong C, Jin Kuk K, Seung Duk H. Mortality predictors in patients treated with continuous renal replacement. Kidney Res Clin Pract. 2011;30(1):73–9.
Balakumar V, Murugan R, Sileanu FE, Palevsky P, Clermont G, Kellum JA. Both positive and negative fluid balance may be associated with reduced long-term survival in the critically ill. Crit Care Med. 2017;45(8):e749–57.
Silversides JA, Major E, Ferguson AJ, Mann EE, McAuley DF, Marshall JC, Blackwood B, Fan E. Conservative fluid management or deresuscitation for patients with sepsis or acute respiratory distress syndrome following the resuscitation phase of critical illness: a systematic review and meta-analysis. Intensive Care Med. 2017;43(2):155–70.
Murugan R, Hoste E, Mehta RL, Samoni S, Ding X, Rosner MH, Kellum JA, Ronco C. Precision fluid Management in Continuous Renal Replacement Therapy. Blood Purif. 2016;42(3):266–78.
Flythe JE, Kimmel SE, Brunelli SM. Rapid fluid removal during dialysis is associated with cardiovascular morbidity and mortality. Kidney Int. 2011;79(2):250–7.
Chen KP, Cavender S, Lee J, Feng M, Mark RG, Celi LA, Mukamal KJ, Danziger J. Peripheral edema, central venous pressure, and risk of AKI in critical illness. Clin J Am Soc Nephrol. 2016;11(4):602–8.
Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, Kusek JW, Van Lente F. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247–54.
Kellum JA, Lameire N. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care. 2013;17(1):204.
An JN, Hwang JH, Kim DK, Lee H, Ahn SY, Kim S, Park JT, Kang SW, Oh YK, Kim YS, et al. Chronic kidney disease after acute kidney injury requiring continuous renal replacement therapy and its impact on long-term outcomes: a multicenter retrospective cohort study in Korea. Crit Care Med. 2017;45(1):47–57.
Claure-Del Granado R, Mehta RL. Fluid overload in the ICU: evaluation and management. BMC Nephrol. 2016;17(1):109.
Bouchard J, Mehta RL. Volume management in continuous renal replacement therapy. Semin Dial. 2009;22(2):146–50.
Zhang L, Chen Z, Diao Y, Yang Y, Fu P. Associations of fluid overload with mortality and kidney recovery in patients with acute kidney injury: a systematic review and meta-analysis. J Crit Care. 2015;30(4):860 e867–813.
Prowle JR, Kirwan CJ, Bellomo R. Fluid management for the prevention and attenuation of acute kidney injury. Nat Rev Nephrol. 2014;10(1):37–47.
Srivastava A. Fluid resuscitation: principles of therapy and “kidney safe” considerations. Adv Chronic Kidney Dis. 2017;24(4):205–12.
Bednarczyk JM, Fridfinnson JA, Kumar A, Blanchard L, Rabbani R, Bell D, Funk D, Turgeon AF, Abou-Setta AM, Zarychanski R. Incorporating dynamic assessment of fluid responsiveness into goal-directed therapy: a systematic review and meta-analysis. Crit Care Med. 2017;45(9):1538–45.
Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med. 2013;369(13):1243–51.
Cecconi M, Hofer C, Teboul JL, Pettila V, Wilkman E, Molnar Z, Della Rocca G, Aldecoa C, Artigas A, Jog S, et al. Fluid challenges in intensive care: the FENICE study: a global inception cohort study. Intensive Care Med. 2015;41(9):1529–37.
Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med. 2013;369(25):2462–3.
Liu YL, Prowle J, Licari E, Uchino S, Bellomo R. Changes in blood pressure before the development of nosocomial acute kidney injury. Nephrol Dial Transplant. 2009;24(2):504–11.
Schrier RW. Body fluid volume regulation in health and disease: a unifying hypothesis. Ann Intern Med. 1990;113(2):155–9.
Cecconi M, De Backer D, Antonelli M, Beale R, Bakker J, Hofer C, Jaeschke R, Mebazaa A, Pinsky MR, Teboul JL, et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40(12):1795–815.
Levy MM, Evans LE, Rhodes A. The Surviving Sepsis Campaign Bundle: 2018 update. Crit Care Med. 2018;46(6):997–1000.
Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013;39(2):165–228.
Chen H, Wu B, Gong D, Liu Z. Fluid overload at start of continuous renal replacement therapy is associated with poorer clinical condition and outcome: a prospective observational study on the combined use of bioimpedance vector analysis and serum N-terminal pro-B-type natriuretic peptide measurement. Crit Care. 2015;19:135.
Kashani K, Mehta RL. We restrict CRRT to only the most hemodynamically unstable patients. Semin Dial. 2016;29(4):268–71.
Murugan R, Balakumar V, Kerti SJ, Priyanka P, Chang CH, Clermont G, Bellomo R, Palevsky PM, Kellum JA. Net ultrafiltration intensity and mortality in critically ill patients with fluid overload. Crit Care. 2018;22(1):223.
O'Connor ME, Prowle JR. Fluid Overload. Crit Care Clin. 2015;31(4):803–21.
Brunet S, Leblanc M, Geadah D, Parent D, Courteau S, Cardinal J. Diffusive and convective solute clearances during continuous renal replacement therapy at various dialysate and ultrafiltration flow rates. Am J Kidney Dis. 1999;34(3):486–92.
Vaara ST, Korhonen AM, Kaukonen KM, Nisula S, Inkinen O, Hoppu S, Laurila JJ, Mildh L, Reinikainen M, Lund V, et al. Fluid overload is associated with an increased risk for 90-day mortality in critically ill patients with renal replacement therapy: data from the prospective FINNAKI study. Crit Care. 2012;16(5):R197.
Funding
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI17C1827). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
JJH, SK, DDK, KBC, HJO, DRR, and HJO have made substantial contributions to the conception and design of this study. JJH, HAL, SK, YKK, JEK, SL, and HJO have made contributions to the acquisition and interpretation of the data. JJH and HJO drafted the article and revised it for important intellectual content. All the authors took part in the manuscript writing and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study protocol complied with the Declaration of Helsinki guidelines and received full approval from the Institutional Review Board at Ewha Womans University Mokdong Hospital. We obtained informed consent from the participants prior to enrollment in the present study.
Consent for publication
We obtained consent to publish from the participants for the reporting of individual patient data.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1:
Figure S1. Flow diagram for patient enrollment. Table S1. Clinical parameters at 24-hr after initiation of continuous renal replacement therapy. Table S2. Clinical parameters at 72-hr after initiation of continuous renal replacement therapy. Table S3. Comparison of patient’s characteristics according to amount of input or output at 24-hr and 72-hr assessment after CRRT initiation. Table S4. Power analysis to assess validity of the study sample size.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Jhee, J.H., Lee, H.A., Kim, S. et al. The interactive effects of input and output on managing fluid balance in patients with acute kidney injury requiring continuous renal replacement therapy. Crit Care 23, 329 (2019). https://doi.org/10.1186/s13054-019-2633-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13054-019-2633-0