
Abstract
Background
In comparison to static spacers, articulating spacers have been shown to result in a similar infection eradication rate in two-stage revision of periprosthetic knee infections. However, the optimal construct for articulating spacers has not been identified yet. The aim of this study was to present a preliminary result of treatment for periprosthetic knee infection using a novel computer-aided design (CAD)-articulating spacer.
Methods
We retrospectively reviewed 32 consecutive cases of chronic periprosthetic knee infection occurring from January 2015 to December 2015. In these cases, we used an antibiotic-loaded, optimized CAD-articulating spacer based on the retrieved knee prosthesis. Evaluation included infection eradication rate, the Hospital of Special Surgery (HSS) knee score, range of motion (ROM), and spacer-related mechanical complications. All cases were regularly followed-up for 2 years minimum.
Results
Twenty-eight of 32 patients (87.5%) had infection eradication; 18 patients (56.3%) received reimplantation successfully. The mean interval between spacer insertion and reimplantation was 8.8 months (range 4.0–12.5 months). The mean HSS knee score and ROM significantly increased during each interval (p < 0.0001 for both). The mean HSS knee scores were 31.2 (range 20–48) at initial visit, 65.4 (range 60–78.8) at 1 month after spacer insertion, and 84.2 (range 78–90) at 3 months after reimplantation (p < 0.0001). The mean ROM were 72.0° (range 15–100°), 85.6° (range 35–110°), and 102.0° (range 80–122°), respectively (p = 0.002). Two (6.3%) spacer-related mechanical complications occurred.
Conclusions
The CAD-articulating spacer in two-staged revision of periprosthetic knee infection significantly controlled infection, improved clinical outcomes, increased ROM, and decreased mechanical complications in the preliminary study. Further larger clinical studies are needed to confirm the findings presented here.
Similar content being viewed by others


Background
Chronic periprosthetic infection is a devastating complication following total knee arthroplasty (TKA), and two-stage revision with an antibiotic-loaded spacer is the gold standard for treatment due to high infection eradication rates (as high as 80–90%) [1,2,3,4]. In comparison to static spacers, articulating spacers have been shown to result in a similar infection eradication rate. However, articulating spacers may provide better ROM and mobility, improved functional outcome, some weight-bearing, and easier subsequent reimplantation [4]. Although there are several types of articulating spacers, such as cement-on-cement handmade (COCH), cement-on-cement prefabricated (COCP), cement-on-cement molded (COCM), and metal-on-polyethylene (MOP), the optimal articulating spacer construct has not yet been identified [5]. Moreover, several articulating spacer-related mechanical complications have occurred, such as extensor apparatus problems, spacer loosening or fracture, and joint subluxation or dislocation; as many as 57% of cases have reported these complications [5, 6]. These problems might lead to further surgery, poor functional outcomes, prolonged treatment courses during interim stage, and difficulty in reimplantation [7, 8].
In the last decade three-dimensional (3D) printing technology has been applied more frequently in orthopedic surgical techniques [9], such as reverse engineering [10], computer-aided design (CAD) [11], computer-aided manufacture (CAM) [12], and rapid prototyping [13]. It was speculated that the CAD technique may help optimize articulating spacers [5].
Therefore, COCM articulating spacers were designed and fabricated using the CAD technique and were based on the retrieved knee prosthesis. This preliminary study was conducted to evaluate these CAD-articulating spacers and their efficacy in treating periprosthetic infection following TKA two-stage revision. It was hypothesized that these optimized spacers could (1) eradicate periprosthetic knee infection, (2) improve clinical outcomes, (3) increase ROM, and (4) decrease mechanical complications.
Methods
Design of CAD-articulating spacers
First, 3D computer models with reverse engineering were obtained. The smallest size of the right side retrieved knee prosthesis (U2 PSA Revision Knee; United Orthopedic Corporation, New Taipei City, Taiwan) was chosen as a prototype. The femoral and tibial insert components were scanned by the SmartSCAN-HE 3D scanner (Accurex, Braunschweig, Germany). The data were imported into Geomagic Design X (3D Systems Corporation, South Carolina, USA) to create 3D virtual models. Six sizes of the 3D femoral and tibial insert models were available after proportional amplification of the prototype (amplification was done without changing the curvature and geometry of the articular surface in Geomagic Design X).
Next, the articulating spacer was optimized with the CAD technique. In each femoral model, the trochlea groove was drawn centrally (Fig. 1a). The femoral cam and sagittal box were preserved, but the femoral stem and axial box were removed. All the depressions, gaps, or defected areas of the femoral models were drawn, filled, and aligned with the edge of the plane to smoothen the contour. Moreover, multiple concave semicircles that were 2.0 mm in diameter were created over the bony surface of femoral models in a checkerboard pattern, with 4.0 mm separating each semicircle (Fig. 1b).

In the femoral model, a the view from articular surface showed the centrally drawn trochlea groove; b the view from the bony surface showed multiple 2.0 mm in diameter with 4.0 mm separating the concave semicircles in a checkerboard pattern; in the tibial insert model, c the view from the articular surface showed 30.0-mm thickness, with 2.0-mm mark intervals on bilateral surfaces as a scale; d the view from the bony surface showed multiple convex semicircles with the same pattern as in the femoral models; e the tibial molder based on the tibial insert model with a handle; f, g, and h fabrication of the CAD-femoral and CAD-tibial trials and tibial molder; i and j each corresponding silicone mold for fabricating the femoral and tibial cement spacers
In each tibial insert model, the post was preserved. The thickness of the insert was enlarged to 30.0 mm, with 2.0-mm intervals marked on the medial and lateral surfaces of the model to be used as a scale (Fig. 1c). The same procedure was done in femoral models to fill all defect areas. Conversely, multiple convex semicircles, with a 2.0-mm diameter, were created over the bony surface of tibial insert models with the same spread pattern as in femoral models (Fig. 1d). Each “tibial molder” was designed based on the tibial insert model, with removal of the post and attachment of a “handle” (Fig. 1e).
The last step (CAM) was to fabricate the femoral and tibial insert models as CAD-femoral and CAD-tibial trials using the Objet500 Connex3 3D printer (Stratasys, USA) using biocompatible resin MED610 (EN-International Standards Organization [ISO] 10993-5:2009, 10993-10:2013, 10993-3:2014, 10993-18:2009, USP Plastic Class VI USP 34 <88>) (Fig. 1f, g). Each tibial molder was manufactured with the same method (Fig. 1h). The corresponding molds for each CAD-femoral and CAD-tibial trials were manufactured with medical grade silicone rubber TSE3488T (Momentive, Gunma, Japan) (Fig. 1i, j). The silicone molds were made of a thermosetting polymer, and could be resterilized by hydrogen peroxide plasma for repetitive use without shape deformation.
Patient selection
This study was approved by the Institutional Review Board (CMUH107-REC3-130) and was designed as a series of retrospective consecutive cases. Adult patients with chronic periprosthetic knee infections after primary TKA were enrolled between January 2015 and December 2015. They underwent two-stage revision with the insertion of the CAD-articulating spacer and were followed up for a minimum of 2 years. All cases met the Musculoskeletal Infection Society (MSIS) criteria [14], and all exhibited chronic infection with a clinical duration lasting longer than 1 month [2]. Loosening of components was diagnosed by plain radiography. All surgeries were performed by a single fellowship-trained arthroplasty surgeon (TLL).
Surgical technique
Patients were given spinal anesthesia and placed in the supine position. The medial parapatellar approach was performed for all knees, with the use of a tourniquet. During the debridement, multiple soft tissues and fluid specimens were obtained, removed, and sent for culture. All the components, cement, synovium, and necrotic tissue were removed thoroughly, and care was taken to avoid fracture.
After component removals, molding of the CAD-femoral and CAD-tibial spacers were performed by another surgeon. Each of these two steps took approximately 30 min. The debridement was performed by one team of surgeons at the same time and took about 60 min. The CAD-femoral and CAD-tibial trials were sized against the ones retrieved. Then, the corresponding silicone molds were chosen for fabricating the cement spacer (Fig. 2a). The femoral spacer was prepared first. Antibiotics with 4.0 g vancomycin and 4.0 g ceftazidime were mixed into one package of CMW3 bone cement (DePuy Synthes, Warsaw, IN, USA) [15, 16]. The use of lubricant was not necessary because the cement did not adhere to the interface of the silicone mold. After the cement cured, the femoral spacer was easily separated from the mold (Fig. 2b). An additional package of antibiotic-loaded cement (comprised of the same formula) was used to implant the spacer in the distal femur. Gelfoam was packed in the metadiaphyseal junction to avoid infiltration of cement, but to fill the metaphyseal defect with stem-like cement. The cement technique was applied early to the spacer and late to the open bone ends, to allow molding to the bony defect surface without adherence and interdigitation [3].

a The corresponding silicone molds were chosen after sizing against the retrieved prosthesis; b antibiotic-loaded cement CAD-femoral spacer; c the adequate thickness of the tibial spacer was determined with the silicone mold and tibial molder; d antibiotic-loaded cement CAD-tibial spacer; e and f intraoperative photograph of the assessment of stability and tracking of the knee joint after insertion of CAD-articulating spacers
After the cement had cured, adequate gap tension was measured under traction of the leg at full extension and the flexion of the knee joint was 90°; this was determined by using the depth scale on the CAD-tibial trial. The thickness of the tibial spacer was determined and prepared with the aid of the internal depth gage of the tibial mold and molder (Fig. 2c). Then the tibial spacer was easily separated from the mold after curing of cement (Fig. 2d). The same cement techniques were used for implanting the tibial spacer in the proximal tibia. The limb was taken to full extension in correct alignment and tension, allowing the tibial spacer to seek its appropriate level (Fig. 2e).
An assessment for stability and tracking was performed (Fig. 2f). Lateral release was performed if necessary. Then the wound was closed in layers with monofilament sutures and closed suction drains that were left in situ following surgery. Any sinus tract over the skin was excised and closed.
The mean surgical time took 103.3 min (range 86–124 min). The overall surgical time was not extended because molding of the CAD-articulating spacers and debridement were performed simultaneously.
Postoperative care
Use of continuous passive motion device started two days following the operation; toe-touch weight-bearing (with crutch) was allowed on the third day following surgery. Full weight-bearing was not allowed during the entire interim period. A knee brace was not used. The drains were removed when the volume of fluid drainage from the surgery site was at a minimum at 1 or 2 weeks after surgery. Intravenous (IV) antibiotics were administered according to the susceptibilities of each microorganism, while intravenous vancomycin with ceftazidime was administered under culture-negative conditions [15, 16]. IV antibiotics were administered for at least 4 weeks, until a progressive decline was seen in C-reactive protein (CRP) levels and erythrocyte sedimentation rate (ESR) and the wound was healed. After discharge, oral antibiotics were continued for at least 4 weeks for suppression until CRP levels and ESR returned to normal. Radiographic evaluations were conducted immediately after the operation, 1 month postoperatively, and every subsequent month in the outpatient clinic (Fig. 3). Criteria for reimplantation included negative clinical signs of infection, CRP and ESR values within normal limits, and negative-culture of arthrocentesis after holding oral antibiotics for 2 weeks [17].

Knee anteroposterior, lateral, and skyline Merchant radiographs were taken with the CAD-articulating spacer in situ
Evaluations
As the clinical outcome evaluation, the Hospital of Special Surgery (HSS) knee score [18] and ROM were documented at the initial visit, 1 month after spacer insertion and 3 months after reimplantation. Infection eradication was defined using the Delphi criteria [17]. Radiographic evaluations on following plain films were performed in the INFINITT’s Picture Archiving and Communications System. The following codes were for recording spacer-related mechanical complications: (1) optimal size and position of the spacer, (2) spacer loosening, tilting or migration, (3) spacer crack or fracture, (4) joint subluxation (including mediolateral or anterolateral translation in relation to the spacer component), (5) joint dislocation, and (6) extensor apparatus problems (patellar maltracking or fracture) [5, 6]. One musculoskeletal radiologist (HYC) and two arthroplasty surgeons (YCF and HCH) assessed and recorded all radiographic data independently.
Statistical analyses
Statistical analyses were performed using SPSS for Windows, version 24 (SPSS Inc, Armonk, NY). The Friedman two-way analysis of variance (ANOVA) by ranks test was used as a non-parametric test. For comparison, between each time interval, Wilcoxon signed-rank test was used. The reliability of spacer-related radiographic coding was examined by the intra-class correlation coefficient (ICC). Statistical significance was set at p < 0.05.
Results
Thirty-two adult patients were enrolled. There were 14 males and 18 females, with a mean age of 73.3 years old (range 58–93 years). Twenty-one patients (65.6%) underwent debridement procedures in other institutions before visiting our clinic. All patients exhibited primary TKA, including 10 (31.3%) of cruciate retaining (CR) type and 22 (68.7%) of cruciate substituting (CS) type. The average hospital stay was 5.4 weeks (range 4–8 weeks), whereas the average duration of follow-up was 36.9 months (range 30.1–45 months). The causative microorganisms were isolated in 27 knees, with polymicrobial infection occurring in three of 27 cases; the causative agent of infection was unknown in five knees. The clinical data are presented in Table 1.
The overall infection eradication rate was 87.5% (28/32). Reinfection occurred in four knees (12.5%), which satisfied either ≥ 1 major or ≥ 3 of 5 minor MSIS criteria [14]. Of the four knees, three received resection again with CAD-articulating spacer implantation and one received amputation above the knee. There was no soft tissue defect of the knee in this series; therefore, the flap reconstruction procedure was not used. The mean time interval between spacer insertion and reimplantation was 8.8 months (range 4.0–12.5 months). Eighteen knees (56.3%) received reimplantation with NexGen Legacy Constrained Condylar Knees (LCCK) (Zimmer, Warsaw, IN, USA). At the latest follow-up, none of them had evidence of infection nor required chronic antibiotic therapy.
Ten patients (31.2%) underwent spacer retention in situ because they were medically unfit for further surgery. However, until the last follow-up for 2 years minimum, there was no recurrent infection in patients who underwent spacer retention.
The mean HSS knee scores were 31.2 (range 20–48) at initial visit, 65.4 (range 60–78.8) at 1 month after spacer insertion, and 84.2 (range 78–90) at 3 months after reimplantation (p < 0.0001). The mean HSS knee score significantly increased during each interval (p < 0.0001 between the initial visit and the first month after spacer insertion and p < 0.0001 between the spacer and 3 months following reimplantation). The mean ROM values were 72.0° (range 15–100°) at initial visit, 85.6° (range 35–110°) at 1 month after spacer insertion, and 102.0° (range 80–122°) at 3 months after reimplantation (p = 0.002). The mean ROM value significantly increased during each time interval (p < 0.0001 and p < 0.0001, respectively).
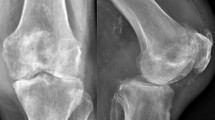
There were two spacer-related mechanical complications, with an overall complication rate of 6.3% (2 out of 32 cases). The ICC of spacer-related radiographic coding was 0.995 (range 0.991–0.997, p < 0.0001) (Table 2). The first complication, in case 2, was a medial plateau fracture with tibial spacer tilting after 3 months of spacer insertion (Fig. 4a). Fortunately, the patient received fair reimplantation. The second complication, in case 13, was patellar maltracking disorder, and it occurred during the first month after spacer insertion (Fig. 4b). The patient complained of lateral knee bulging with deep flexing, but flexing did not affect ROM of the knee joint (5–108°), and the HSS knee score was 70.2. The patient received reimplantation after 5.5 months, without further complications.

a Knee anteroposterior and lateral radiographs showing the medial plateau fracture with tibial spacer tilting 3 months after spacer insertion; b knee skyline Merchant radiograph showing patellar maltracking disorder 1 month after spacer insertion
Discussion
This was the first preliminary study to fabricate optimized articulating spacers based on retrieved knee prosthesis with reverse engineering, using CAD and CAM techniques. Particularly, it was the first study of its type to investigate the role of CAD-articulating spacers in the treatment of periprosthetic knee infection. The preliminary result demonstrated that CAD-articulating spacers in two-staged revision of periprosthetic knee infection could eradicate infection, improve clinical outcomes, increase ROM, and decrease mechanical complications.
After reverse engineering, the retrieved femur and tibial insert components, the real-sized prosthesis-like 3D models with corresponding geometry and high joint congruence prototype could be obtained. The prototype then was amplified proportionally without changing the curvature and geometry of the articular surface to obtain six different sizes of femoral and tibial insert models, respectively. With six sizes of CAD-femoral and CAD-tibial trials available, the surgeon could compare the retrieved components to select the adequate silicon mold quickly, reducing the disadvantage of the limited options regarding spacer sizes [5, 19,20,21,22]. In the present study, the size of each retrieved component was roughly compatible with CAD-trials regardless of different prosthesis brands.
Comparing using commercial prostheses as models in fabricating silicone molds, the reverse engineering and CAD techniques used in CAD-articulating spacer demonstrated the following advantages: (1) In CAD-femoral models, centralization of the trochlea area could reduce the number of instruments required for molding (for both knees) [7, 20, 23, 24]. Patellar tracking could be adjusted intraoperatively by lateral releasing; (2) the CAD-tibial trials with 2.0-mm gap and a total of 15 interval marks facilitated simple measurement of the flexion-extension gaps. The customized thickness of the CAD-tibial spacer could be molded by the internal depth gauze of the tibial mold, which was similar with StageOne knee spacers (Biomet, Warsaw, IN, USA) [6, 20, 25]; (3) the design of the novel CAD-tibial molder allowed surgeons to push the cement to make a flat plane and multiple small pits of bony surface on the tibial spacers. With the same pits of bony surface on the femoral spacers, increasing cement anchoring and decreasing loosening could be achieved; (4) filling all the depressions, defects, or gaps in the femoral and tibial insert models could allow smooth contours and decrease mechanical weakness in the cement spacer, avoiding cement crack or fracture.
The use of lubricant was necessary when fabricating COCM spacers with metallic mold [26], cement mold [7, 27], and polypropylene mold [24]. This led to multiple pitting or a rough joint surface, possibly increasing friction when gliding. Moreover, the cement mold had to be removed before the spacer cement cured; the articular surface of the spacer tends to be deformed, requiring reshaping. The cured CAD-articulating spacers were easily separated from the elastic silicon molds without changing the shape. Medical-grade silicone rubber TSE3488T (Momentive, Gunma, Japan) has low viscosity with excellent releasability, which meant that the lubricant was not necessary because the cement does not adhere to the interface of the silicone mold [28]. Moreover, the high tear and tensile strength of TSE3488T easily separated the cement spacer from the mold after the cement cured. This made a CAD-articulating spacer with perfect contour and ultra-high joint congruence. Moreover, these durable CAD trials and silicone molds are a highly cost-effective method for spacer fabrication because they can be easily cleaned, sterilized, and reused.
Struelens et al. [6] reported high mechanical complications (57%) with StageOne spacers, with more incidence of spacer tilting (24%) and mediolateral translation (21%). The cause might be related to poor fixation and poor constraint design of the spacers. However, Van Thiel et al. [25] recorded a complication of only 1.7% with the same spacers, which might be due to the postoperative restricted protocol of hinged knee brace or knee immobilizer for protection. Poor mechanical circumstances, such as bony loss, cruciate or collateral ligament defects following infection and resection arthroplasty, and poor constraining spacer design, made the infected knee joint inherently unstable and similar with the environment of revision TKA [23, 29]. This poor design of spacers resulted in more spacer-related mechanical complications, such as joint subluxation or dislocation [6]. Shen et al. [7] highlight that the tibial post can only maintain mediolateral stability, but the femoral cam is a key construct for anteroposterior stability and rollback mechanism. Most COCM spacers had no post-cam design [1, 19, 20] or had only a tibial post design [23, 24]. A post-cam design has been only seen in MOP spacers [5, 30, 31], Shen et al.’s spacers [7], and the CAD-articulating spacers in the present study. In comparison to primary TKA CS design, CAD-articulating spacers based on revision knee prosthesis had a larger box, cam, and post, which resulted in more constraint to counter the instability of the anteroposterior and mediolateral directions after infection. This could explain why knee braces were not necessary in our series.
The COCM spacers fabricated by Hsu et al. [24], Su et al. [23], and Shen et al. [7], and the COCH spacers produced by Villanueva-Martínez et al. [29], had acceptable complication rates ranging from 4.8% to 13.3%. The lower CAD-articulating spacer-related mechanical complication rate (6.3%) was similar to or lower than the rates found in previous studies. However, it was the first study to investigate spacer-related mechanical complications and to strictly define the sizing, position, and integrity of spacers and the relationship of bone and spacer of the femoral-tibial and patellar-femoral joints. Moreover, all the radiographs were reviewed independently by one musculoskeletal radiologist and two arthroplasty surgeons, which minimized the underestimation of the complication rate.
Ocguder et al. [22] used COCP spacer, which has International Organization for Standardization (ISO)-tested and ISO-approved mechanical properties and facilitates partial load-bearing. However, spacer cracks were detected in as high as 35.3%. The inclusion of high-dose antibiotics increases bactericidal capacity locally but also substantially weakens cement, especially hand-blended ones [32]. This might be the reason why antibiotic-loaded cement spacer cracks after even partial weight-bearing. Only toe weight-bearing was allowed in our series during the entire interim period; thus, no spacer crack or fracture occurred.
Haddad et al. [33] presented more complications with the earlier version of the PROSTALAC spacer (DePuy Synthes) due to minimal constraint design (non-posterior stabilized), but the complication rate deceased after those knees were managed with the current version of PROSTALAC spacer (posterior-stabilized). In their study, the total spacer-related mechanical complication rate (sum of two versions of PROSTALAC) based on our radiographic definition was 24.4%. In contrast with the results of Haddad et al., Meek et al. [31], and Gooding et al. [34] reported lower complication rates (2.1% and 6.1%, respectively) for the current PROSTALAC. With resterilized constrained MOP spacers, Hofmann et al. [30] and Pietsch et al. [35] reported lower mechanical complication rates (4.0% and 6.1%, respectively). There was 20.8% loosening of MOP spacers and 50.0% migration of COCH spacers in the series of Jämsen et al. [36], which might be related to the cement technique used, i.e., loose fixation of the spacer with cement. However, there was no spacer loosening or migration in our series, except in one medial plateau fracture with tibial spacer tilting, which was due to the patient’s dementia and full weight-bearing without protection. The multiple small pits over the bony surface of the CAD-articulating spacers could increase the roughness and allow better cement fixation. The metaphyseal stem-like cement could share the load of CAD-articulating spacers due to relatively poor bone stock after infection. The advantages of both mechanics could allow the spacer to be stably implanted in the bone, potentially minimizing the risk of spacer loosening or migration. Moreover, with the cementing technique we used [3], the spacers did not tightly interdigitate the bony surface, and the removal of spacers was simple with minimal bone loss. All the spacer-related mechanical complications of two-stage revision of periprosthetic knee infection that had been mentioned in the literature are summarized in Table 3.
With multiple mechanical advantages, such as the corresponding geometry, matched sizing, balanced gap, ultra-high joint congruence, optimal post-cam constrain construction, and stable fixation, the optimized CAD-articulating spacer could significantly improve HSS knee score and ROM of the knee joint. With adequate debridement techniques and antibiotic-loaded spacers, our series shared a similar infection eradication rate (87.5%) with other studies [24, 27, 37, 38]. During reimplantation, there was no need for extensive release due to good soft tissue tension of the spacer. The ROM and HSS knee score after reimplantation significantly increased and improved, respectively. Increased ROM after reimplantation could be predicted from the good ROM at the interim stage [5, 39], as a theoretical functional outcome.
This study had some limitations. First, there were limited numbers of patients and the lack of a control group. Second, our case series only involved periprosthetic knee infection after primary TKA but did not include cases of post revision TKA. We did not have experience regarding whether CAD-articulating spacers could maintain stable joints if there were larger bony defects or more collateral ligament loss after TKA revision for infection. Third, nearly one third of the subjects underwent retention of the spacer because they were medically unfit. It was well reported that this situation was infrequent and had a high complication rate [40]. However, we did not record final functional score or ROM of these knees, but these spacers seemed to be positioned well and were stable, according to radiography at the outpatient clinic during the last follow-up. This might be ascribed to the novel congruent and more constrained design of CAD-articulating spacer. This study provides a platform for further evaluation of TKA two-step revision, similar to the study conducted by Choi et al. [41]. Lastly, we did not evaluate the biomechanical properties of CAD-articulating spacers like the experiment performed by Villa et al. [42]. However, if CAD-articulating spacers were tough enough to withstand failure on full weight-bearing, it would have been an added advantage. Elderly patients are likely to manage better with full weight-bearing while awaiting revision TKA. This provides another platform for further study.
Conclusions
This was the first preliminary study to design and fabricate optimized CAD-articulating spacers based on retrieved knee prosthesis by reverse engineering and CAD/CAM techniques that provided multiple benefits. In two-stage revision of periprosthetic knee infection, the CAD-articulating spacer significantly controlled infection, improved clinical outcome, increased ROM, and decreased mechanical complications. Further larger clinical studies are needed to confirm the findings presented here.
Abbreviations
- 3D:
-
Three-dimensional
- ANOVA:
-
Analysis of variance
- CAD:
-
Computer-aided design
- CAM:
-
Computer-aided manufacture
- COCH:
-
Cement-on-cement handmade
- COCM:
-
Cement-on-cement molded
- COCP:
-
Cement-on-cement prefabricated
- CR:
-
Cruciate retaining
- CRP:
-
C-reactive protein
- CS:
-
Cruciate substituting
- ESR:
-
Erythrocyte sedimentation rate
- HSS:
-
Hospital of Special Surgery
- ICC:
-
Intra-class correlation coefficient
- ISO:
-
International Organization for Standardization
- LCCK:
-
Legacy Constrained Condylar Knee
- MOP:
-
Metal-on-polyethylene
- MSIS:
-
Musculoskeletal Infection Society
- ROM:
-
Range of motion
- TKA:
-
Total knee arthroplasty
References
Durbhakula SM, Czajka J, Fuchs MD, Uhl RL. Antibiotic-loaded articulating cement spacer in the 2-stage exchange of infected total knee arthroplasty. J Arthroplasty. 2004;19(6):768.
Segawa H, Tsukayama DT, Kyle RF, Becker DA, Gustilo RB. Infection after total knee arthroplasty. A retrospective study of the treatment of eighty-one infections. J Bone Joint Surg Am. 1999;81(10):1434.
Cui Q, Mihalko WM, Shields JS, Ries M, Saleh KJ. Antibiotic-impregnated cement spacers for the treatment of infection associated with total hip or knee arthroplasty. J Bone Joint Surg Am. 2007;89(4):871.
Anderson JA, Sculco PK, Heitkemper S, Mayman DJ, Bostrom MP, Sculco TP. An articulating spacer to treat and mobilize patients with infected total knee arthroplasty. J Arthroplasty. 2009;24(4):631.
Spivey JC, Guild GN 3rd, Scuderi GR. Use of articulating spacer technique in revision total knee arthroplasty complicated by sepsis: a systematic meta-analysis. Orthopedics. 2017;40(4):212.
Struelens B, Claes S, Bellemans J. Spacer-related problems in two-stage revision knee arthroplasty. Acta Orthop Belg. 2013;79(4):422.
Shen H, Zhang X, Jiang Y, Wang Q, Chen Y, Wang Q, et al. Intraoperatively-made cement-on-cement antibiotic-loaded articulating spacer for infected total knee arthroplasty. Knee. 2010;17(6):407.
Lau AC, Howard JL, Macdonald SJ, Teeter MG, Lanting BA. The effect of subluxation of articulating antibiotic spacers on bone defects and degree of constraint in revision knee arthroplasty. J Arthroplasty. 2016;31(1):199.
Cai H. Application of 3D printing in orthopedics: status quo and opportunities in China. Ann Transl Med. 2015;3(Suppl 1):S12.
Chrzan R, Urbanik A, Karbowski K, Moskala M, Polak J, Pyrich M. Cranioplasty prosthesis manufacturing based on reverse engineering technology. Med Sci Monit : Int Med J Exp Clin Res. 2012;18(1):Mt1.
Dai KR, Yan MN, Zhu ZA, Sun YH. Computer-aided custom-made hemipelvic prosthesis used in extensive pelvic lesions. J Arthroplasty. 2007;22(7):981.
Yang J, Cai H, Lv J, Zhang K, Leng H, Sun C, et al. In vivo study of a self-stabilizing artificial vertebral body fabricated by electron beam melting. Spine. 2014;39(8):E486.
Li H, Wang L, Mao Y, Wang Y, Dai K, Zhu Z. Revision of complex acetabular defects using cages with the aid of rapid prototyping. J Arthroplasty. 2013;28(10):1770.
Parvizi J, Gehrke T. Definition of periprosthetic joint infection. J Arthroplasty. 2014;29(7):1331.
Hsu YH, Hu CC, Hsieh PH, Shih HN, Ueng SW, Chang Y. Vancomycin and ceftazidime in bone cement as a potentially effective treatment for knee periprosthetic joint infection. J Bone Joint Surg Am. 2017;99(3):223.
Carli AV, Sethuraman AS, Bhimani SJ, Ross FP, Bostrom MPG. Selected heat-sensitive antibiotics are not inactivated during polymethylmethacrylate curing and can be used in cement spacers for periprosthetic joint infection. J Arthroplasty. 2018;33(6):1930.
Diaz-Ledezma C, Higuera CA, Parvizi J. Success after treatment of periprosthetic joint infection: a Delphi-based international multidisciplinary consensus. Clin Orthop Relat Res. 2013;471(7):2374.
Slupik A, Bialoszewski D. A comparative analysis of the clinical utility of the Staffelstein-score and the hospital for special surgery knee score (HSS) in monitoring physiotherapy of total knee replacement patients--preliminary study. Ortop Traumatol, Rehabil. 2009;11(1):37.
Kohl S, Evangelopoulos DS, Kohlhof H, Krueger A, Hartel M, Roeder C, et al. An intraoperatively moulded PMMA prostheses like spacer for two-stage revision of infected total knee arthroplasty. Knee. 2011;18(6):464.
Park SJ, Song EK, Seon JK, Yoon TR, Park GH. Comparison of static and mobile antibiotic-impregnated cement spacers for the treatment of infected total knee arthroplasty. Int Orthop. 2010;34(8):1181.
Pitto RP, Spika IA. Antibiotic-loaded bone cement spacers in two-stage management of infected total knee arthroplasty. Int Orthop. 2004;28(3):129.
Ocguder A, Firat A, Tecimel O, Solak S, Bozkurt M. Two-stage total infected knee arthroplasty treatment with articulating cement spacer. Arch Orthop Trauma Surg. 2010;130(6):719.
Su YP, Lee OK, Chen WM, Chen TH. A facile technique to make articulating spacers for infected total knee arthroplasty. J Chin Med Assoc. 2009;72(3):138.
Hsu YC, Cheng HC, Ng TP, Chiu KY. Antibiotic-loaded cement articulating spacer for 2-stage reimplantation in infected total knee arthroplasty: a simple and economic method. J Arthroplasty. 2007;22(7):1060.
Van Thiel GS, Berend KR, Klein GR, Gordon AC, Lombardi AV, Della Valle CJ. Intraoperative molds to create an articulating spacer for the infected knee arthroplasty. Clin Orthop Relat Res. 2011;469(4):994.
Fehring TK, Odum S, Calton TF, Mason JB. Articulating versus static spacers in revision total knee arthroplasty for sepsis. The Ranawat Award. Clin Orthop Relat Res. 2000;380:9.
Ha CW. A technique for intraoperative construction of antibiotic spacers. Clin Orthop Relat Res. 2006;445:204.
Momentive Performance Materials Japan LLC. https://www.techsil.co.uk/media/wysiwyg/Brochures/momentive-mould-making-brochure.pdf. Accessed 2014.
Villanueva-Martinez M, Rios-Luna A, Pereiro J, Fahandez-Saddi H, Villamor A. Hand-made articulating spacers in two-stage revision for infected total knee arthroplasty: good outcome in 30 patients. Acta Orthop. 2008;79(5):674.
Hofmann AA, Goldberg T, Tanner AM, Kurtin SM. Treatment of infected total knee arthroplasty using an articulating spacer: 2- to 12-year experience. Clin Orthop Relat Res. 2005;(430):125.
Meek RM, Masri BA, Dunlop D, Garbuz DS, Greidanus NV, McGraw R, et al. Patient satisfaction and functional status after treatment of infection at the site of a total knee arthroplasty with use of the PROSTALAC articulating spacer. J Bone Joint Surg Am. 2003;85-a(10):1888.
DeLuise M, Scott CP. Addition of hand-blended generic tobramycin in bone cement: effect on mechanical strength. Orthopedics. 2004;27(12):1289.
Haddad FS, Masri BA, Campbell D, McGraw RW, Beauchamp CP, Duncan CP. The PROSTALAC functional spacer in two-stage revision for infected knee replacements. Prosthesis of antibiotic-loaded acrylic cement. J Bone Joint Surg Br. 2000;82(6):807.
Gooding CR, Masri BA, Duncan CP, Greidanus NV, Garbuz DS. Durable infection control and function with the PROSTALAC spacer in two-stage revision for infected knee arthroplasty. Clin Orthop Relat Res. 2011;469(4):985.
Pietsch M, Hofmann S, Wenisch C. Treatment of deep infection of total knee arthroplasty using a two-stage procedure. Oper Orthop Traumatol. 2006;18(1):66.
Jämsen E, Sheng P, Halonen P, Lehto MU, Moilanen T, Pajamaki J, et al. Spacer prostheses in two-stage revision of infected knee arthroplasty. Int Orthop. 2006;30(4):257.
Carli AV, Bhimani S, Yang X, de Mesy Bentley KL, Ross FP, Bostrom MPG. Vancomycin-loaded polymethylmethacrylate spacers fail to eradicate periprosthetic joint infection in a clinically representative mouse model. J Bone Joint Surg Am. 2018;100(11):e76.
Evans RP. Successful treatment of total hip and knee infection with articulating antibiotic components: a modified treatment method. Clin Orthop Relat Res. 2004;427:37.
Ritter MA, Harty LD, Davis KE, Meding JB, Berend ME. Predicting range of motion after total knee arthroplasty. Clustering, log-linear regression, and regression tree analysis. J Bone Joint Surg Am. 2003;85-a(7):1278.
Petis SM, Perry KI, Pagnano MW, Berry DJ, Hanssen AD, Abdel MP. Retained antibiotic spacers after total hip and knee arthroplasty resections: high complication rates. J Arthroplasty. 2017;32(11):3510.
Choi HR, Freiberg AA, Malchau H, Rubash HE, Kwon YM. The fate of unplanned retention of prosthetic articulating spacers for infected total hip and total knee arthroplasty. J Arthroplasty. 2014;29(4):690.
Villa T, Carnelli D. Experimental evaluation of the biomechanical performances of a PMMA-based knee spacer. Knee. 2007;14(2):145.
Acknowledgements
We thank the 3D Printing Medical Research Center, Department of Orthopedic Surgery, Department of Radiology, and Division of Infection Disease, Department of Internal Medicine, China Medical University Hospital, Taichung, Taiwan, for providing facility support services for the study.
Funding
The authors received no specific funding for this work.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Author information
Authors and Affiliations
Contributions
CHT and HCH designed the study. HYC, YWC, YCF, MWH, and CHC collected subjects’ data. MYS performed statistical analysis. An initial draft of the manuscript was written by TLL, and CHT re-drafted parts of the manuscript and provided helpful advice on the final revision. All authors edited and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research did not increase the risk and economic burden of patients, the patients’ rights were fully protected, and the project design was conducted in line with scientific and ethical principles. This study was approved by the Institutional Review Board (CMUH107-REC3-130). All participants in this study have provided informed written consent prior to enrollment.
Consent for publication
All participants in this study have provided informed written consent prior to enrollment.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Tsai, CH., Hsu, HC., Chen, HY. et al. A preliminary study of the novel antibiotic-loaded cement computer-aided design-articulating spacer for the treatment of periprosthetic knee infection. J Orthop Surg Res 14, 136 (2019). https://doi.org/10.1186/s13018-019-1175-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13018-019-1175-0