
Abstract
Background
Diet is a key risk factor for chronic disease, and an increasing concern among older adults. We aim to examine the changes in dietary patterns using principal component analysis and a diet quality index among older adults and examine the predictors of dietary change over a 4 year period.
Methods
Data was obtained via a postal survey in a prospective cohort, the Wellbeing Eating and Exercise for a Long Life (WELL) study. Australian adults aged 55 years and over (n = 1005 men and n = 1106 women) completed a food frequency at three time points and provided self-reported personal characteristics. Principal component analysis was used to assess dietary patterns and diet quality was assessed using the 2013 Revised Dietary Guideline Index. The relationships between predictors and change in dietary patterns were assessed by multiple linear regression.
Results
Two dietary patterns were consistently identified in men and women at three time points over 4 years. One was characterised by vegetables, fruit and white meat, and the other was characterised by red and processed meat and processed foods. Reduced consumption of key food groups within the principal component analysis-determined dietary patterns was observed. An increase in diet quality over 4 years was observed in men only. Reported higher education levels and favourable lifestyle characteristics, including not smoking and physical activity, at baseline predicted an increase in healthier dietary patterns over 4 years.
Conclusions
There was stability in the main dietary patterns identified over time, however participants reported an overall decrease in the frequency of consumption of key food groups. Compliance with the Australian Dietary Guidelines remained poor and therefore targeting this population in nutritional initiatives is important. Design of nutrition promotion for older adults need to consider those with lower socioeconomic status, as having a lower level of education was a predictor of poorer dietary patterns. It is important to consider how nutrition behaviours can be targeted alongside other lifestyle behaviours, such as smoking and inadequate physical activity to improve health.
Similar content being viewed by others

Background
Diet is an important risk factor for chronic diseases such as cardiovascular disease and type 2 diabetes [1]. Chronic disease is a major health concern among older adults [2] and of particular concern are those within the peri-retirement age group where these conditions begin to manifest. This is also a period of major life transition, with experiences such as changed work-loads, marital transitions, and children leaving home occurring. Transitional life stages may impact health behaviours including diet [3,4,5], and may provide a window of opportunity to promote dietary change [6]. Improving diet within this age group will help to reduce the burden of disease and improve quality of life in older adults [7].
The importance of foods and overall dietary patterns, rather than single nutrients, has emerged in the last few decades of nutrition research [8]. Exploration of dietary patterns allows the complex nature of diet to be acknowledges by considering the synergistic effects of foods and nutrients within the body as well as considering the way we consume food [9]. There are multiple methods for assessing dietary patterns, namely empirical methods that use statistical techniques to explore the dietary intake data, such as principal component analysis, and theoretically-based dietary patterns based on predefined patterns constructed from hypotheses and scientific evidence regarding nutritional health, such as dietary guidelines and recommendations [10]. Applying multiple methods within the same data set may increase our understanding of the use of these methods and the implication of using different methodologies [11].
Epidemiological studies often assess dietary patterns at just one-time point to represent typical or long-term dietary patterns, however, dietary patterns may change over time particularly during transitional life stages such as retirement. There is little research available that describes the dietary patterns of those within a peri-retirement life stage [12, 13], as many studies of older adults focus on a broader age range or more specifically on the elderly [14, 15]. For example, those with higher occupation and education levels are more likely to be associated with improved diet in adults aged 25–75 years [16] and 50–69 years old [17]. The number of longitudinal studies of dietary patterns in peri-retirement age are limited [17, 18] with only two studies in an Australian population [16, 19]. Furthermore, few existing studies have examined predictors of change in dietary patterns among peri-retirement [17, 18, 20]. Those studies found that a higher level of education and social class predicted individuals continuing with a healthier dietary pattern or improving their dietary pattern over time. In the broader adult population, older age, being female and being of higher socioeconomic position have consistently been shown to be predictors of improved dietary patterns [16, 21,22,23,24,25]. Understanding what predicts change in dietary patterns will inform future research and nutrition promotion interventions. The purpose of this study was to examine the dietary patterns among peri-retirement aged older adults over 4 years using principal component analysis (PCA) and the 2013 Revised Dietary Guideline Index (DGI-2013), and to examine predictors of change in dietary patterns.
Methods
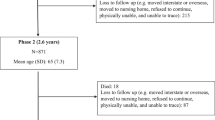
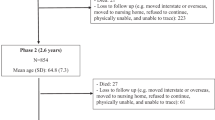
This study used data collected in the WELL study. The methods of the WELL study have been described in detail elsewhere [26]. In brief, a stratified random sample was selected from the Australian Electoral Commission’s electoral roll, a compulsory register for Australians. The sample was stratified by gender and three levels of Socioeconomic Position (SEP) according to the Index of Relative Socio-economic Disadvantage, a Socioeconomic Index for Areas (SEIFA) score, assigned by the Australian Bureau of Statistics [27]. Fourteen postcodes from three SEIFA categories (low, medium and high SEIFA) and in both rural and urban areas were randomly selected. From these, 134 participants (equal men and women) were randomly selected for the study, resulting in the final sampling pool of 11,256 Australian adults (55–65 years). Those who agreed to participate completed a postal questionnaire in 2010. In 2012 and 2014, participants who had not withdrawn were re-contacted via the post and invited to complete a follow-up survey. (WELL study participant recruitment flow diagram provided in additional file 1). The studies methods were approved by the Deakin University Human Research Ethics Committee (2009–105).
Dietary intake
Dietary intake at each time point was assessed using a 111-item Food Frequency Questionnaire (FFQ) adapted from the 1995 Australian National Nutrition Survey [28, 29]. The FFQ assessed participant’s dietary intake over the previous 6 months, with nine response categories for each item, ranging from ‘never or less than once a month’ to ‘6+ times per day’. No information was gathered on portion sizes. Data from participants with > 10% of the FFQ data missing were considered invalid [30] and not included in this study while all other missing FFQ responses were considered not consumed [30]. Additional food-behaviour questions concerning daily fruit and vegetable consumption, salt use, trimming the fat from meat and type of bread and milk consumed were also included in the questionnaire. These questions have been evaluated and shown to be valid measures of food intake behaviours [30,31,32,33,34,35].
Dietary patterns assessed using principal component analysis (PCA)
Dietary patterns were determined using PCA which has been described in detail elsewhere [11] and the results across all time points have been included in additional file 2. The FFQ items were converted to daily equivalents and categorised into 52 food groups according to nutritional content, culinary usage and food groups in the 2013 Australian Dietary Guidelines (ADG) [36] (Additional file 3). FFQ items consumed (≥ 1 time per week) by less than 10% of the population were combined with other food items where possible or omitted. Only soy beverages were omitted since a large proportion of the sample (91%) indicated they never consumed this item. The daily intake frequencies were used to determine dietary patterns by PCA. Servings per day (frequency), is routinely used to determine empirical dietary patterns [37].
Initially, PCA was conducted separately for each time point to assess whether similar patterns were present over time. The factor loadings for the dietary patterns identified at each time were examined qualitatively and quantitatively using Tucker’s coefficient of congruence [38] to determine the similarity of dietary patterns between time points. Only the patterns that were present at all three time points were included in the analysis. Factor scores for the retained patterns were calculated using the 2010 factor loadings for key foods (factor loadings of | ≥ 0.20|) as the sum of key food group frequencies multiplied by factor loading at each time point. Factor loadings from 2010 were used to calculate factor scores at all three time points for a consistent dietary pattern measure with changes due to frequency of consumption.
Dietary patterns assessed using diet quality
A diet quality index, the revised Dietary Guideline Index (DGI-2013) [13] was used to assess diet quality, according to the ADG [36] using data from the FFQ and additional food-behaviour questions. A detailed description of the DGI-2013 has been provided elsewhere [13]. The DGI-2013 includes 13 components, each scored out of ten. The total diet quality score range is 0 to 130. There are two categories of components, firstly those that reflect adequate intake of nutritious foods. This includes diet variety, vegetables, fruit, cereal, protein, dairy and water. Secondly those that reflect moderation or limited intake of foods and drinks high in saturated fat and/or added sugar, salt or alcohol and low in fiber. This includes discretionary food, saturated fat, salt, sugar and alcohol consumption. A higher DGI-2013 score indicates greater adherence to the ADG and therefore greater diet quality.
The original DGI has been associated with independently measured daily nutrient intakes, including an inverse relationship with fat and energy consumption and a positive relationship with dietary fibre and several important micronutrients such as β-carotene, vitamin C, folate, calcium, and iron [39]. A higher DGI score has been associated with a higher level of SEP and reduced cardiometabolic risk including Type 2 diabetes, hypertension, obesity and demonstrated reduced weight gain [40,41,42,43]. Since being updated, the DGI-2013 has shown similar qualities, with a higher score associated with higher education, being a non-smoker, higher physical activity and lower BMI [13] as well as better health-related quality of life [7].
Predictors
Potential predictors of dietary change were self-reported in the questionnaires, including socio-demographic characteristics (sex, education, retirement status and relationship status) and health-related behaviours and characteristics (anthropometry, weight loss intentions, smoking status, physical activity and diagnosed cardiometabolic disease-related conditions). Education was collapsed into three categories (no formal qualifications and up to year 10; year 12, trade, apprenticeship, certificate or diploma; and a university degree or higher). Retirement status at baseline was dichotomously coded as yes or no. Relationship status was collapsed from five categories into three (living as married-registered or de facto; separated or divorced; and never married). Baseline (2010) Body Mass Index (BMI) was calculated from self-reported height and weight and categorised according to the following criteria: underweight: BMI < 18.5; healthy: BMI ≥ 18.5 to < 25 kg/m2; overweight: BMI ≥ 25 to < 30 kg/m2; obese: BMI ≥ 30 kg/m2. Few participants were diagnosed with any cardiometabolic disease-related conditions after 2010, therefore the data from the three time points were converted into dichotomous variables; indicating whether they had ever been diagnosed with a cardiovascular (CVD)-related condition (stroke, blood clot, high blood pressure or heart disease) and whether they had ever been diagnosed with a diabetes-related condition (diabetes or impaired glucose tolerance). Weight loss intentions at baseline were categorised into three categories (trying to avoid gaining weight, trying to lose weight and not trying anything or trying to gain weight, since few (< 1%) participants reported trying to gain weight). A collapsed baseline smoking status variable was used (current smoker-occasionally or regularly; former smoker; and never smoked). Self-reported physical activity in the 7 days prior to the questionnaire was assessed using the long version of the International Physical Activity Questionnaire (IPAQ) [44]. IPAQ records the frequency, intensity, and duration of physical activity during the previous week. Only time spent in leisure time physical activity (walking, moderate and vigorous) was considered as research has shown leisure time physical activity is a better predictor of good self-rated health in comparison to work related physical activity [45, 46]. This is also a behaviour that lifestyle interventions may be more successful in addressing. Minutes of leisure time activity per week were calculated by summing the number minutes of moderate intensity leisure time physical activity per week and twice the number of minutes per week spent participating in leisure time vigorous intensity physical activity per week [44]. Participants were classified as to whether they did or did not meet the physical activity recommendations of at least 150 min of activity per week [47]. Age has previously been shown to predict diet [48] and change in diet [16], however, given the narrow age range in the WELL study, it was not explored as a predictor but included as a covariate. Given the known associations with diet; BMI smoking and physical activity [16, 21,22,23,24,25] were also adjusted for in the analysis of predictors were appropriate.
Statistical analysis
All analyses were stratified by sex since dietary patterns and diet quality differ between men and women [37, 49]. Mixed-effect multi-linear regression with random intercepts for individuals and robust standard errors for the sampling locations (postcodes) was used to assess change in dietary scores across 2010, 2012 and 2014, where the linear effect of time was the predictor. This method recognises the relationship between successive observations while accounting for the individuals’ random effects [50]. Multiple linear regression with robust standard errors for the sampling location (postcodes) was used to assess the relationships between predictors and the change in dietary pattern scores from 2010 to 2014. The outcome (difference between 2010 and 2014) was achieved by using the 2014 score as the outcome adjusting for the baseline (2010) score. This is the recommended method in behavioural science to overcome measurement errors in studies of change [51]. Analysis of the base model was conducted followed by a model adjusting for baseline age, BMI, smoking and physical activity given their association with diet. In the models where these confounders were used as the predictor they themselves were not included in the model as a cofounder. Assumptions for linear regression were tested and adequately met for the models tested.
Results
Participant characteristics
In 2010, 4082 questionnaires were returned, 2757 were returned in 2012 and 2542 questionnaires were returned in 2014. Participants were excluded from the analysis if they did not provide their date of birth or sufficient dietary intake data (missing > 10% of FFQ or who were missing additional diet behaviour questions) resulting in the following sample sizes used to determine dietary patterns; 2010: n = 1888 men and 2071 women; 2012: n = 1269 men and 1428 women and 2014: n = 1183 men and 1309 women. For analysis of predictors, only those with complete data at baseline and the final time point were included (n = 1005 men and n = 1106 women). Participant characteristics are summarised in Table 1.
Dietary patterns
PCA-derived dietary patterns
In men, four dietary patterns were identified in 2010 [11], four in 2012, and two patterns were identified in 2014. Only two dietary patterns remained consistent across all time points and were therefore retained for further analysis (Table 2). Factor 1 was characterised by vegetable dishes, fruit, fish and poultry and factor 2 was characterised by red or processed meat, white bread, fried fish and hot chips. Tucker’s coefficient of congruence indicated that these two dietary patterns had fair to good similarity between 2010 and 2012 (coefficient of congruence 0.96 and 0.93). While the two factors identified in 2014 were qualitatively similar to the 2010 factors, quantitatively, they were different with low coefficient of congruence i.e. the factor loadings were different between the time points, (coefficient of congruence 0.66 and 0.72). For women, PCA identified two dietary patterns at each time point. Factor 1 was characterised by vegetables, fruit and fish and factor 2 was characterised by cakes, processed meat, hot chips and confectionary (Table 2). Fair to good similarity between dietary patterns was determined by the coefficient of congruence (coefficient of congruence range 0.90 to 0.97). The factor scores of all the PCA-derived dietary patterns significantly decreased over 4 years in both men and women (Table 3). Given the equation to calculate the factor scores (the sum of the 2010 factor loadings multiplied food frequency of key food groups), this suggests that the food frequency of the food groups decreased.
Diet quality
Over 4 years, the total DGI-2013 score increased in men (β = 0.42, 95%CI 0.16, 0.69, P = 0.002) while for women it did not significantly change (β = 0.07, 95%CI -0.19, 0.33, P = 0.584) (Table 3). Examining individual components of the DGI (Additional file 4) demonstrated that compliance to the diet variety and water intake recommendations decreased in men and women. Compliance with recommendations for vegetables, salt, sugar and alcohol intake increased in men over the 4 years. For women, compliance with fruit, cereal and saturated fat recommendations decreased, while compliance to discretionary food and sugar intake recommendations increased.
Predictors of change in dietary patterns
PCA-derived dietary patterns
For men, having a higher level of education, trying to avoid gaining weight in 2010 and meeting physical activity recommendations in 2010 were predictors of an increase in factor 1 score (vegetable dishes, fruit, fish and poultry) by 2014 (β = 0.14: 95% CI: 0.06, 0.22: P = 0.001; β = 0.08: 0.01, 0.15: P = 0.023 and β = 0.09: 0.02, 0.16: P = 0.008, respectively) (Table 4). Men who reported trying to lose weight in 2010 experienced a decrease in factor 2 score (red or processed meat, white bread, fried fish and hot chips) over 4 years, compared to those not trying anything for their weight (β = − 0.07: − 0.13, − 0.01: P = 0.018). Men who reported being smokers in 2010 experienced an increase in factor 2 (red or processed meat, white bread, fried fish and hot chips) score over the 4 years compared to those who never smoked (β = 0.12: 0.04, 0.20: P = 0.004). Among women, while a number of variables were associated with changes in dietary patterns (trying to lose weight, meeting physical activity recommendations and education), there were no significant findings in women after adjusting for covariates (Table 5).
Diet quality
Compared to those that reported never smoking, being a smoker in 2010 was associated with a decrease in DGI-2013 (β = − 4.77: − 6.76, − 2.78: P < 0.001 and β = − 4.11: − 6.92, − 1.31: P = 0.005 for men and women, respectively) (Table 6). A diagnosis of a cardiometabolic-related condition prior to 2010 was associated with an increase in diet quality in men over 4 years compared to not having been diagnosed (β = 1.25: 0.09, 0.58: P = 0.035). There were no other significant associations identified for men or women.
Discussion
This longitudinal study adds to the limited research regarding dietary patterns over time and contributing to our understanding of the predictors of dietary patterns in adults of peri-retirement age. Qualitatively, there was stability in the main dietary patterns that were identified over time in the men and women, with a healthy and an unhealthy dietary pattern consistently identified. However, scores on these dietary patterns decreased over the 4 years in men and women, indicating that participants may have reported an overall decrease in the frequency of consumption of key food groups. Diet quality as assessed by the DGI-2013 increased from 2010 to 2014 in men, while no change was found in women, however compliance with the Australian Dietary Guidelines remained poor. Of the predictors examined, men with a higher level of education, not smoking and meeting the physical activity recommendations were predictors of a favorable change in dietary patterns .
The key dietary patterns identified remained consistent across time, however changes in consumption were observed. All the factor scores of the dietary patterns determined by PCA decreased over time suggesting that there may have been an overall decrease in the consumption of the key food items by this population. Diet quality, as assessed by the DGI-2013, increased from 2010 to 2014 in men, while no change was observed in women. Previous research has shown positive changes in diet quality scores over time [52,53,54]. Trends in the individual DGI-2013 components differed, with men making some favourable changes to their diet by increasing compliance with the vegetable intake guideline and decreasing their salt use, extra sugar use and alcohol consumption. However, diet variety, a favourable dietary behaviour, also decreased. Poorer dietary changes were identified in women, with a decrease in diet variety, fruit intake and water consumption and an increase in saturated fat observed, while favourable changes including reduced discretionary foods and extra sugar intake were also seen. Compliance to the overall Australian Dietary Guidelines remained low, with a mean (SD) DGI-2013 score of 83.1 (14.1) and 90.6 (13.1) for men and women, respectively in 2014, out of a total achievable score of 130.
It may be that the decrease in diet variety in men and women resulted from the overall decrease in food intake observed in the analysis of the PCA-derived dietary patterns (indicated by the negative change for all factor scores). There have been mixed results in previous studies with respect to diet variety and age. Some studies have reported increased diet variety with age [55,56,57], while others have shown a decrease [58]. Measurement of diet variety in the current study may be limited by the use of a FFQ to collect dietary intake information with a restricted number of food items included.
When examining predictors of dietary change, we found that higher education and other healthy lifestyle characteristics including not smoking, meeting physical activity recommendations and avoiding weight gain predicted favourable changes in dietary patterns. These results are in line with previous studies [16, 19, 59]. It is well understood that higher education is often associated with health-promoting dietary behaviours [48]. The relationship between diet and socioeconomic position is complex [60] and there is a need to consider those with low socioeconomic position when targeting nutritional messages. Smoking status and previous diagnosis of a cardiometabolic-related condition were the only factors that predicted change in diet quality. However, as there was very little change in the DGI-2013 score overall, power was limited in this analysis.
Smoking is often coupled with other negative health behaviours such as poor diet and physical inactivity and the combined effects of these risk factors lead to poor health outcomes [61]. This was supported in the current study, in that smoking predicted a decrease in diet quality over time and not meeting physical activity recommendations predicted a decrease in favourable dietary patterns. In line with this, the 1958 British Birth Cohort found those who increased their physical activity between the age of 33 and 42 years, also made improvements in diet [62].
Few studies have explored change in dietary patterns longitudinally, with most assessing diet at just one time point. Comparison of dietary patterns identified by the empirically-based techniques across different time points presents challenges. Since PCA identifies patterns within the available data, assessing the derived patterns at different time points may result in different patterns identified or factor loading of similar patterns will have unavoidably changed. For PCA, calculating PCA factor scores based on the baseline factor loadings rather than comparing the dietary patterns identified at each time point helps to overcome these concerns [18, 19]. However, this technique is limited if the overall dietary patterns are not similar across time or when comparing different population groups. In the current study, we found that the PCA-derived dietary patterns were comparable across time in terms of the type of food present. However, in men the coefficient of congruence indicated that the identified patterns were not quantitatively equal over time. This suggests that while similar food groups loaded highly on the dietary patterns identified at each time, their factor loadings were different. This is a limitation of using empirical dietary pattern methods in longitudinal studies and is why it is important to use consistent factor loadings over time.
Limited studies have explored empirically derived dietary patterns longitudinally [17, 18, 23, 53, 59, 63] and there is little consensus on the methodological approaches to use. Mishra et al. (2006) used exploratory factor analysis to determine dietary patterns at baseline, and similar to the present study, they used an equation defined at baseline to calculate the diet scores at the two follow-up times. Using this approach enables researchers to assess the changes in dietary pattern identified at baseline but does not allow for new dietary patterns that may have emerged over time [64].
Dietary patterns assessed using diet quality scores are simpler to compare over time since they are not data-driven and criteria for scoring can be applied consistently across time. However, as diet quality indices are based on prior knowledge or existing national guidelines they require significant efforts to design them and to ensure validity prior to use [65]. A potential limitation of interpreting the overall dietary patterns derived by either approach, is that they encompass multiple components of diet and it is possible that there are different predictors of change for the separate components of diet quality.
This study has a number of strengths and limitations. Strengths of this study include the population-based design of the WELL study, the focus on older adults and the comparison of different methods of assessing dietary patterns. Although the response rate was modest (38%), the sampling technique resulted in a sample with characteristics consistent with both state [66] and national data [67, 68] maximising the generalisability of the study results. Furthermore, the specific age range of 55–65 years captures an understudied population during a transitional life stage and the comparative nature of this study adds to the limited research in this area.
The use of FFQs are known to be susceptible to measurement error of dietary intake. The FFQ used in this study has previously been used to assess dietary patterns and behaviours, demonstrating that it is a valid predictor of health outcomes and suggesting it has predictive validity [7, 29, 39]. Portion sizes were not measured in this study and the FFQ assumes that each eating occasion was a standard serve of the food or food group. This is a limitation of the dietary pattern methodologies used. Further to this, energy intake could not be estimated and used to adjust for in the analyses of input variables for dietary pattern analysis and predictors of change nor could under-reporters be identified. However, research shown that frequency of intake is the major determinant of energy intake [69, 70] and non-energy adjusted frequency is more sensitive to the intake of important low-energy foods such as fruit and vegetables [71, 72].
This study relied on self-reported measures, which may result in measurement error, for example height, weight and BMI. However, self-reported height and weight has previously been shown to be a valid estimate of BMI in large epidemiological studies [73, 74]. The short follow-up period was a further limitation, which meant that few participants experienced change in predictor variables, therefore this could not be considered in the analyses.
Both empirical-based dietary pattern and theoretical techniques have inherent limitations and considerations for dietary pattern analysis. Several researcher-determined decisions are required such as determining the index components and scoring methods, the collapsing and format of input variable, the number of derived empirical patterns and assigning labels to patterns for example [37, 65, 75]. Steps were taken to reduce subjectivity. For example, the FFQ foods were grouped based on approaches used in previous literature and consistent with the Australian Dietary Guidelines [36]. Established criteria and best practice were used to determine the dietary patterns and objective criteria were used to compare the dietary patterns between men and women in PCA.
Conclusions
In this sample of peri-retirement aged adults the dietary patterns identified over 4 years remained stable in men and women. Changes observed within individuals included reduced consumption of key foods within the PCA-determined dietary patterns in both men and women. While there were improvements in diet quality in men, overall diet quality remains poor. Several predictors of changes in dietary patterns were identified, with higher education and favourable baseline lifestyle characteristics tending to predict an increase in healthier dietary patterns. Design of nutrition promotion initiatives for older adults need to consider those with lower socioeconomic status, as having a lower level of education was a predictor of poorer dietary patterns. It is also important to consider how nutrition behaviours can be targeted alongside other lifestyle behaviours, such as smoking and inadequate physical activity recommendations to improve health. This study adds to the limited literature of longitudinal dietary pattern and dietary patterns of peri-retirement aged adults.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- 95% CI:
-
95% confidence interval
- ADG:
-
Australian Dietary Guidelines
- BMI:
-
Body Mass Index
- CVD:
-
Cardiovascular disease
- DGI-2013:
-
2013 Revised Dietary Guideline Index
- FFQ:
-
Food Frequency Questionnaire
- PCA:
-
Principal component analysis
- SEIFA:
-
Index of Relative Socio-economic Disadvantage, a Socioeconomic Index for Areas score
- SEP:
-
Socioeconomic Position
- WELL:
-
Wellbeing Eating and Exercise for a Long Life study
References
Mozaffarian D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity: a comprehensive review. Circulation. 2016;133(2):187–225.
World Health Organization. World report on ageing and health. Geneva: WHO Press; 2015.
Lee S, Cho E, Grodstein F, Kawachi I, Hu FB, Colditz GA. Effects of marital transitions on changes in dietary and other health behaviours in US women. Int J Epidemiol. 2005;34(1):69–78.
Eng PM, Kawachi I, Fitzmaurice G, Rimm EB. Effects of marital transitions on changes in dietary and other health behaviours in US male health professionals. J Epidemiol Community Health. 2005;59(1):56–62.
Davies L. Retirement courses: should they include nutrition? J R Soc Health. 1990;110(1):20–2.
Lara J, Hobbs N, Moynihan PJ, Meyer TD, Adamson AJ, Errington L, et al. Effectiveness of dietary interventions among adults of retirement age: a systematic review and meta-analysis of randomized controlled trials. BMC Med. 2014;12(1):1–12.
Milte CM, Thorpe MG, Crawford D, Ball K, McNaughton SA. Associations of diet quality with health-related quality of life in older Australian men and women. Exp Gerontol. 2015;64:8–16.
Mozaffarian D, Rosenberg I, Uauy R. History of modern nutrition science-implications for current research, dietary guidelines, and food policy. BMJ. 2018;361:k2392.
Reedy J, Krebs-Smith SM, Hammond RA, Hennessy E. Advancing the science of dietary patterns research to leverage a complex systems approach. J Acad Nutr Diet. 2017;117(7):1019–22.
Krebs-Smith SM, Subar AF, Reedy J. Examining dietary patterns in relation to chronic disease: matching measures and methods to questions of interest. Circulation. 2015;132(9):790–3.
Thorpe MG, Milte CM, Crawford D, McNaughton SA. A comparison of the dietary patterns derived by principal component analysis and cluster analysis in older Australians. Int J Behav Nutr Phys Act. 2016;13:30.
Markussen MS, Veierod MB, Kristiansen AL, Ursin G, Andersen LF. Dietary patterns of women aged 50-69 years and associations with nutrient intake, sociodemographic factors and key risk factors for non-communicable diseases. Public Health Nutr. 2016;19(11):2024–32.
Thorpe MG, Milte CM, Crawford D, McNaughton SA. A revised Australian dietary guideline index and its association with key Sociodemographic factors, health behaviors and body mass index in Peri-retirement aged adults. Nutrients. 2016;8(3):160.
Govindaraju T, Sahle BW, McCaffrey TA, McNeil JJ, Owen AJ. Dietary Patterns and Quality of Life in Older Adults: A Systematic Review. Nutrients. 2018;10(8):971.
Tourlouki E, Matalas AL, Panagiotakos DB. Dietary habits and cardiovascular disease risk in middle-aged and elderly populations: a review of evidence. Clin Interv Aging. 2009;4:319–30.
Arabshahi S, Lahmann PH, Williams GM, Marks GC, van der Pols JC. Longitudinal change in diet quality in Australian adults varies by demographic, socio-economic, and lifestyle characteristics. J Nutr. 2011;141(10):1871–9.
Harrington JM, Dahly DL, Fitzgerald AP, Gilthorpe MS, Perry IJ. Capturing changes in dietary patterns among older adults: a latent class analysis of an ageing Irish cohort. Public Health Nutr. 2014;17(12):2674–86.
Mishra GD, McNaughton SA, Bramwell GD, Wadsworth ME. Longitudinal changes in dietary patterns during adult life. Br J Nutr. 2006;96(4):735–44.
Nguyen HH, Wu F, Oddy WH, Wills K, Brennan-Olsen SL, Jones G, et al. Dietary patterns and their associations with socio-demographic and lifestyle factors in Tasmanian older adults: a longitudinal cohort study. Eur J Clin Nutr. 2019;73(5):714–23.
Tabung FK, Steck SE, Zhang J, Ma Y, Liese AD, Tylavsky FA, et al. Longitudinal changes in the dietary inflammatory index: an assessment of the inflammatory potential of diet over time in postmenopausal women. Eur J Clin Nutr. 2016;70(12):1374–80.
Kristal AR, Hedderson MM, Patterson RE, Neuhouser M. Predictors of self-initiated, healthful dietary change. J Am Diet Assoc. 2001;101(7):762–6.
Lake AA, Mathers JC, Rugg-Gunn AJ, Adamson AJ. Longitudinal change in food habits between adolescence (11-12 years) and adulthood (32-33 years): the ASH30 study. J Public Health. 2006;28(1):10–6.
Lee S, Harnack L, Jacobs DR Jr, Steffen LM, Luepker RV, Arnett DK. Trends in diet quality for coronary heart disease prevention between 1980-1982 and 2000-2002: the Minnesota heart survey. J Am Diet Assoc. 2007;107(2):213–22.
Shatenstein B, Gauvin L, Keller H, Richard L, Gaudreau P, Giroux F, et al. Individual and collective factors predicting change in diet quality over 3 years in a subset of older men and women from the NuAge cohort. Eur J Nutr. 2015;55(4):1671–81.
Mishra GD, Prynne CJ, Paul AA, Greenberg DC, Bolton-Smith C. The impact of inter-generational social and regional circumstances on dietary intake patterns of British adults: results from the 1946 British birth cohort. Public Health Nutr. 2004;7(6):737–44.
McNaughton SA, Crawford D, Ball K, Salmon J. Understanding determinants of nutrition, physical activity and quality of life among older adults: the wellbeing, eating and exercise for a long life (WELL) study. Health Qual Life Outcomes. 2012;10(1):109.
Australian Bureau of Statistics. Information Paper: An Introduction to Socio-Economic Indexes for Areas (SEIFA), 2006 (cat. no. 2039.0). Camberra: ABS; 2008.
Smith KJ, McNaughton SA, Gall SL, Blizzard L, Dwyer T, Venn AJ. Involvement of young Australian adults in meal preparation: cross-sectional associations with sociodemographic factors and diet quality. J Am Diet Assoc. 2010;110(9):1363–7.
Smith KJ, Gall SL, McNaughton SA, Blizzard L, Dwyer T, Venn AJ. Skipping breakfast: longitudinal associations with cardiometabolic risk factors in the childhood determinants of adult health study. Am J Clin Nutr. 2010;92(6):1316–25.
McLennan W, Podger A. National nutrition survey users' guide, 1995 Australian Bureau of Statistics Catalogue no. 4801.0. Canberra: Australian Government Publishing Service; 1998.
Australian Institute of Health and Welfare. Towards national indicators for food and nutrition: an AIHW view: reporting against the Dietary Guidelines for Australian Adults (cat. no. PHE 70). Canberra: AIHW; 2006.
CATI Technical Reference Group. Population health monitoring and surveillance: question development background paper nutritional food behaviour in Australia. 2003. Available from: http://www.health.vic.gov.au/archive/archive2014/nphp/catitrg/nutritionbgpaper.pdf
Coyne T, Ibiebele TI, McNaughton S, Rutishauser IH, O'Dea K, Hodge AM, et al. Evaluation of brief dietary questions to estimate vegetable and fruit consumption - using serum carotenoids and red-cell folate. Public Health Nutr. 2005;8(3):298–308.
Hodge A, Patterson AJ, Brown WJ, Ireland P, Giles G. The anti Cancer Council of Victoria FFQ: relative validity of nutrient intakes compared with weighed food records in young to middle-aged women in a study of iron supplementation. Aust NZ J Public Health. 2000;24(6):576–83.
Rutishauser IHE, Webb K, Abraham B, Allsopp R. Evaluation of short dietary questions from the 1995 National Nutrition Survey. Commonwealth Department of Health and Aged Care: Canberra; 2001.
National Health and Medical Research Council. Eat for health: Australian Dietary Guidelines. Canberra: NHMRC; 2013.
Newby PK, Tucker KL. Empirically derived eating patterns using factor or cluster analysis: a review. Nutr Rev. 2004;62(5):177–203.
Lorenzo-Seva U, ten Berge JMF. Tucker's congruence coefficient as a meaningful index of factor similarity. Methodol Eur J Res Methods Behav Soc Sci. 2006;2(2):57–64.
McNaughton SA, Ball K, Crawford D, Mishra GD. An index of diet and eating patterns is a valid measure of diet quality in an Australian population. J Nutr. 2008;138(1):86–93.
McNaughton SA, Dunstan DW, Ball K, Shaw J, Crawford D. Dietary quality is associated with diabetes and cardio-metabolic risk factors. J Nutr. 2009;139(4):734–42.
Alhazmi A, Stojanovski E, McEvoy M, Brown W, Garg ML. Diet quality score is a predictor of type 2 diabetes risk in women: the Australian longitudinal study on Women's health. Br J Nutr. 2014;112(6):945–51.
Backholer K, Spencer E, Gearon E, Magliano DJ, McNaughton SA, Shaw JE, et al. The association between socio-economic position and diet quality in Australian adults. Public Health Nutr. 2016;19(3):477–85.
Arabshahi S, van der Pols JC, Williams GM, Marks GC, Lahmann PH. Diet quality and change in anthropometric measures: 15-year longitudinal study in Australian adults. Br J Nutr. 2012;107(9):1376–85.
Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–95.
Okano G, Miyake H, Mori M. Leisure time physical activity as a determinant of self-perceived health and fitness in middle-aged male employees. J Occup Health. 2003;45(5):286–92.
Kaleta D, Makowiec-Dabrowska T, Dziankowska-Zaborszczyk E, Jegier A. Physical activity and self-perceived health status. Int J Occup Med Environ Health. 2006;19(1):61–9.
Australian Institute of Health and Welfare. Australia’s health 2014. Canberra: AIHW; 2014.
Kant AK. Dietary patterns and health outcomes. J Am Diet Assoc. 2004;104(4):615–35.
Wirfalt E, Drake I, Wallstrom P. What do review papers conclude about food and dietary patterns? Food Nutr Res. 2013;57:10.
Fitzmaurice GM, Laird NM, Ware JH. Applied longitudinal analysis. 2nd ed. Hoboken: Wiley; 2011.
Cohen J, Cohen P. Applied multiple regression/correlation analysis for the behavioral sciences. 2nd ed: Hillsdale. NJ: Erlbaum; 1983.
Hu FB, Stampfer MJ, Manson JE, Grodstein F, Colditz GA, Speizer FE, et al. Trends in the incidence of coronary heart disease and changes in diet and lifestyle in women. N Engl J Med. 2000;343(8):530–7.
Fung TT, McCullough M, van Dam RM, Hu FB. A prospective study of overall diet quality and risk of type 2 diabetes in women. Diabetes Care. 2007;30(7):1753–7.
Mertens E, Deforche B, Mullie P, Lefevre J, Charlier R, Knaeps S, et al. Longitudinal study on the association between three dietary indices, anthropometric parameters and blood lipids. Nutr Metab. 2015;12:47.
Vadiveloo M, Dixon LB, Mijanovich T, Elbel B, Parekh N. Dietary variety is inversely associated with body adiposity among US adults using a novel food diversity index. J Nutr. 2015;145(3):555–63.
Vadiveloo M, Dixon LB, Mijanovich T, Elbel B, Parekh N. Development and evaluation of the US healthy food diversity index. Br J Nutr. 2014;112(9):1562–74.
Drewnowski A, Henderson SA, Driscoll A, Rolls BJ. The dietary variety score: assessing diet quality in healthy young and older adults. J Am Diet Assoc. 1997;97(3):266–71.
Michels KB, Wolk A. A prospective study of variety of healthy foods and mortality in women. Int J Epidemiol. 2002;31(4):847–54.
Prevost AT, Whichelow MJ, Cox BD. Longitudinal dietary changes between 1984-5 and 1991-2 in British adults: association with socio-demographic, lifestyle and health factors. Br J Nutr. 1997;78(6):873–88.
Mishra G, Ball K, Arbuckle J, Crawford D. Dietary patterns of Australian adults and their association with socioeconomic status: results from the 1995 National Nutrition Survey. Eur J Clin Nutr. 2002;56(7):687–93.
Loef M, Walach H. The combined effects of healthy lifestyle behaviors on all cause mortality: a systematic review and meta-analysis. Prev Med. 2012;55(3):163–70.
Parsons TJ, Power C, Manor O. Longitudinal physical activity and diet patterns in the 1958 British birth cohort. Med Sci Sports Exerc. 2006;38(3):547–54.
Dekker LH, Boer JM, Stricker MD, Busschers WB, Snijder MB, Nicolaou M, et al. Dietary patterns within a population are more reproducible than those of individuals. J Nutr. 2013;143(11):1728–35.
Northstone K, Emmett PM. A comparison of methods to assess changes in dietary patterns from pregnancy to 4 years post-partum obtained using principal components analysis. Br J Nutr. 2008;99(5):1099–106.
Waijers PM, Feskens EJ, Ocke MC. A critical review of predefined diet quality scores. Br J Nutr. 2007;97(2):219–31.
Department of Health and Human Services. Victorian health monitor food and nutrition report. Melbourne: State Government of Victoria; 2012.
Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results - Foods and Nutrients, 2011–12 (cat. no. 4364.0.55.007). Canberra: ABS; 2014.
Australian Bureau of Statistics. Retirement and Retirement Intentions, Australia, July 2010 to June 2011 (cat. no. 6238.0). Canberra: ABS; 2011.
Leech RM, Worsley A, Timperio A, McNaughton SA. Understanding meal patterns: definitions, methodology and impact on nutrient intake and diet quality. Nutr Res Rev. 2015;28(1):1–21.
Nothlings U, Murphy SP, Sharma S, Hankin JH, Kolonel LN. A comparison of two methods of measuring food group intake: grams vs servings. J Am Diet Assoc. 2006;106(5):737–9.
Bailey RL, Gutschall MD, Mitchell DC, Miller CK, Lawrence FR, Smiciklas-Wright H. Comparative strategies for using cluster analysis to assess dietary patterns. J Am Diet Assoc. 2006;106(8):1194–200.
Ocke MC. Evaluation of methodologies for assessing the overall diet: dietary quality scores and dietary pattern analysis. Proc Nutr Soc. 2013;72(2):191–9.
McAdams MA, Van Dam RM, Hu FB. Comparison of self-reported and measured BMI as correlates of disease markers in US adults. Obesity. 2007;15(1):188–96.
Burton NW, Brown W, Dobson A. Accuracy of body mass index estimated from self-reported height and weight in mid-aged Australian women. Aust NZ J Public Health. 2010;34(6):620–3.
Devlin UM, McNulty BA, Nugent AP, Gibney MJ. The use of cluster analysis to derive dietary patterns: methodological considerations, reproducibility, validity and the effect of energy mis-reporting. Proc Nutr Soc. 2012;71(4):599–609.
Acknowledgements
Kylie Ball and Jo Salmon contributed to the study design and the development and implementation of the WELL study.
Funding
The WELL study was funded by the Diabetes Australia Research Trust and Australian Research Council (DP1095595, FT100100581). SAM is supported by an NHMRC Career Development Fellowship Level 2 (ID1104636) and was previously supported by an ARC Future Fellowship (2011–2015, FT100100581). Funder’s had no role in the design, analysis or writing of this article.
Author information
Authors and Affiliations
Contributions
SAM and DC (along with those acknowledged) designed the study and contributed to the development and implementation of the study. MGT conducted the analysis and interpretation of the data with the assistance of CMM, DC and SAM. MGT drafted the manuscript and all authors contributed to editing and reviewing of the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the Deakin University Human Research Ethics Committee (2009–105). Written informed consent was obtained from all subjects/patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
The Wellbeing Eating and Exercise for a Long Life study participant recruitment flow diagram
Additional file 2.
Factor loadings for dietary patterns derived by principal component analysis at three time points in men of the Wellbeing Eating and Exercise for a Long Life Study
Additional file 3.
A list of the 52 food groups derived from the 111 items in the food frequency questionnaire
Additional file 4.
Examining change in individual components of the DGI over three time points
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Thorpe, M.G., Milte, C.M., Crawford, D. et al. Education and lifestyle predict change in dietary patterns and diet quality of adults 55 years and over. Nutr J 18, 67 (2019). https://doi.org/10.1186/s12937-019-0495-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12937-019-0495-6