
Abstract
Background
Oxidative stress is responsible for some alterations in the chemical structure and, consequently, in the function of proteins, lipids, and DNA. Recent studies have linked oxidative stress to cancers, particularly thyroid cancer, but the mechanisms remain unclear. Here, we further characterize the role of oxidative stress in thyroid cancer by analyzing the expression of two selenium antioxidant molecules, glutathione peroxidase (GPx1) and thioredoxin reductase (TrxR1) in thyroid cancer cells.
Methods
Samples of both healthy thyroid tissue and thyroid tumor were taken for analysis after total thyroidectomy. The expression of GPx1 and TrxR1 was revealed by Western blot analysis and quantified by densitometric analyses, while the evaluation of free radicals was performed by Electron Paramagnetic Resonance (EPR)-spin trapping technique.
Results
Our results show a decrease in the expression of GPx1 and TrxR1 (− 45.7 and − 43.2% respectively, p < 0.01) in the thyroid cancer cells compared to the healthy cells. In addition, the EPR technique shows an increase of free radicals in tumor tissue, significantly higher than that found in healthy thyroid tissue (+ 116.3%, p < 0.01).
Conclusions
Our findings underscore the relationship between thyroid cancer and oxidative stress, showing the imbalance of the oxidant/antioxidant system in thyroid cancer tissue. These results suggest that either the inability to produce adequate antioxidant defense or an increased consumption of antioxidants, due to the hyper-production of free radicals, may play a crucial role in thyroid cancer.
Similar content being viewed by others


Background
The overproduction of free radicals and the consequent increase in oxidative stress lead to irreversible cellular damage, frequently associated with diseases such as atherosclerosis, hypertension, diabetic nephropathy, pulmonary fibrosis, Alzheimer’s disease, and in particular, cancer [1,2,3,4,5,6,7,8,9,10]. In thyroid cancer specifically, chemical modifications of DNA structure that are typically induced by oxidative stress, such as the presence of 8-oxo-2′-deoxyguanosine, have been found by microarray and immunohistochemistry analyses [11]. Moreover, high concentrations of glutathione peroxidase (an antioxidant enzyme) and malondialdehyde (a product of lipid peroxidation) were found in the blood of patients affected by thyroid cancer [12]. We recently described an increase of oxidative stress in the blood of patients affected by thyroid cancer, detected by electronic proton resonance measurements, a refined technique to study qualitatively and quantitatively the oxidizing species in human blood. In addition, another interesting finding of our study was the meaningful decrease of oxidative stress observed in all subjects after thyroidectomy [13].
Our previous studies suggest the involvement of oxidative stress in the pathogenesis of thyroid cancer, but the mechanisms remain unclear. Cells regulate the redox state by balancing the generation of free radicals with their elimination by antioxidant systems [14]. A wide array of vitamins, minerals, and other minor compounds are involved these antioxidant systems [15]. In this study, we focused our attention on selenoproteins, a class of proteins containing selenium that seems to play a critical role in the balance of the oxidant/antioxidant systems. In fact, some of them, e.g. glutathione peroxidases (GPxs) [16] and thioredoxin reductases (TrxRs) [17] play a large role in antioxidant defense and in the maintenance of the intercellular reducing conditions. Since increased oxidative stress has been implicated in thyroid cancer, we hypothesized that the impairment of the expression of selenoproteins may be a key factor towards clarifying the relationship between thyroid cancer and oxidative stress. This study elucidates the mechanism involved in the antioxidant/oxidant system in thyroid cancer, focusing the attention on the role played by selenoproteins GPx1 and TrxR1.
Methods
Patient recruitment
The study population was recruited in 2014 at the Department of Surgical Sciences of the Umberto I Hospital of Rome. Patients were between 24 and 68 years of age, with thyroid nodules classified as indeterminate (TIR3B), suspicious for malignant (TIR4) or malignant (TIR5) after cytologic examination, according to the “Italian Consensus for the classification and reporting of thyroid cytology, 2014” [18]. The Fine Needle Aspiration (FNA) to obtain samples for the cytological evaluation was performed only on thyroid nodules ≥ 1 cm with suspicious ultrasound (US) features, according to “Sonographic and Clinical Features of Thyroid Nodules and Recommendations for FNA” of the American Thyroid Association (ATA) [19]. Considering the cytological results (Table 1), all patients were candidates for thyroid surgery, according to the ATA 2009, the only one known at the time of the recruitment.
Surgical treatment
Surgical treatment was planned taking into account the cytological diagnosis, lymph node involvement and the size of the suspicious nodule (both evaluated through US of the neck), age of patients, and a history of prior head and neck irradiation. In cases with a cytologic diagnosis of malignancy (TIR4, TIR5), the patients underwent total thyroidectomy, according to ATA 2009 (recommendation 26). Thyroid lobectomy alone may be sufficient treatment for small (< 1 cm), low-risk, unifocal, intrathyroidal papillary carcinomas in the absence of prior head and neck irradiation or radiologically or clinically involved cervical nodal metastases, as suggested by ATA 2009. However, none of our TIR4/TIR5 patients were candidates for lobectomy. In fact, as previously described, only patients with suspicious nodules ≥ 1 cm underwent FNA and were included in the study. Table 1 reports the histological size of the tumor, measured “ex vivo” after thyroidectomy, which is often different from the pre-operative US measurements. Patients with clinically involved central compartment (level VI) lymph nodes underwent therapeutic central neck dissection along with total thyroidectomy (Table 1, cases 2, 4, 5, 8, 9, 10, 11, 12, 13, 14, 15, 17, 18, 19, 20). Patients with suspicion for lateral lymph node disease (compartments II–IV) on preoperative US or intraoperative exam also underwent lateral neck dissection (Table 1, cases: 15, 17, 19, 20; ATA 2009, recommendation 27). Patients 3, 6, 7 and 16, with indeterminate nodules (TIR3B), preferred to undergo total thyroidectomy, to avoid the possibility of requiring a future surgery on the contralateral lobe as provided by ATA 2009 (recommendation 25b). Informed consent was obtained from all participants. The criteria of exclusion from the study were the presence of debilitating diseases (i.e. advanced stage diabetes, immunological diseases or hematologic disorders), lack of informed consent, and/or lack of authorization form for the processing of personal data. All subjects recruited for the study underwent the following: electrocardiogram, chest X-ray, indirect laryngoscopy, and whole blood sampling. The following blood tests were obtained for each patient: hemochromocytometric analysis, routine chemistry tests, TSH, FT3, FT4, calcitonin, thyroglobulin, anti-thyroperoxidase antibody (TPOAb), and anti-thyroglobulin antibody (TgAb). In order to obtain a comparison between healthy thyroid tissue and cancer tissue in each individual patient, we selected only those patients (candidates for total thyroidectomy) with unilateral suspicious cytological nodules.
Chemicals and instruments
Antibodies were obtained from the following sources: polyclonal anti-glutathione peroxidase (GPx1) and polyclonal anti-thioredoxin reductase 1 (TrxR1) and RIPA buffer from Sigma–Aldrich (St Louis, MO, USA), monoclonal anti-actin from Santa Cruz Biotechnology (Santa Cruz, CA, USA), peroxidase-conjugated goat anti-mouse and peroxidase-conjugated rabbit anti-goat from Amersham (Arlington Heights, IL, USA). Nitrocellulose paper was obtained from Shleicher & Schuell Bioscience Inc. (Dassel, Germany). Enhanced chemiluminescent kit (ECL kit) and BCA Protein Assay Kit were purchased from Pierce (Rockford, IL, USA). The densitometric analyses of selenium protein were performed using the GS-900 densitometer (Bio-Rad) and the “Image J” Software. Spin trap 1-hydroxy-3-carboxy-pyrrolidine (CPH), 3-carboxy-proxyl radical (CP·) was purchased from ENZO Biochem (Laufelfingen, Switzerland).
Sampling the thyroid tissue for selenoprotein analysis
A complete histological exam of the thyroid gland was performed after thyroidectomy to characterize the lesions and to obtain the definitive histological classification (Table 1). All patients in which the definitive histological exam revealed, in the uninvolved lobe, an incidental cancer lesion or signs of inflammation or other types of disease were excluded from this study. A sample of tissue containing the thyroid cancer and a sample of the contralateral lobe were taken from the gland at the time of surgery and conserved at − 80 °C for future analysis and measurement of selenoproteins, GPx1 and TrxR.
Preparation of thyroid gland proteins extract
To obtain a protein lysate on which to detect GPx1 and TrxR1 proteins, each thyroid sample was suspended in 200 µL of phosphate buffer saline and solubilized by incubation for 10 min at 0 °C with an equal volume of 100 mM Tris–HCl (pH 7.5), 0.6 M NaCl, 4% (w/v) Triton X-100, 4% (v/v) sodium deoxycholate, 0.4 mM PMSF, 1 µg/mL leupeptin and 1 µg/mL aprotinin (4× RIPA buffer). The solution was then diluted once with Phosphate Buffer Saline and adjusted to a final volume of 1 mL with 1× RIPA buffer. After centrifugation at 16,000g for 30 min at 4 °C, the supernatant, constituted by the thyroid tissue lysate, was collected for the western blot or EPR analyses. The protein content in thyroid tissue lysate was detected using the Pierce BCA Protein Assay Kit, to obtain an equal amount of protein in each sample.
Western blot analysis
Samples prepared for Western Blot analysis were solubilized in 4× loading buffer, boiled for 5 min, and resolved by Sodium Dodecyl Sulphate–PolyAcrylamide Gel Electrophoresis (SDS–PAGE). Proteins were transferred to nitrocellulose paper at 35 V overnight. Blots were washed with TBS containing 0.05% Tween 20 (TTBS) and blocked with 3% bovine serum albumin in TTBS for 2 h. Washed nitrocellulose filters were incubated overnight at 4 °C with the anti-GPX1 or anti-TrxR1 antibody. After extensive washes in TTBS, the immunoreactive bands were detected by chemiluminescence coupled to peroxidase activity, according to the manufacturer’s specifications (ECL kit; Pierce).
Densitometric analysis of the selenoproteins GPx1 and TrxR1
In order to measure GPx1 and TrxR1 expression levels, the intensities of specific bands, corresponding to the selenoproteins of interest, were measured. The densitometric analysis of the blots was done using the Image J Software [20]. In brief, the blot images were imported into the software and the contrast was adjusted such that the bands were clearly visible on the blot image. The area around each band was selected and the background intensity was subtracted from the blot image. The intensities of the selected bands were then expressed as a numeric value (arbitrary unit, a.u.) that could be used for carrying out further statistical analyses.
Electron paramagnetic resonance (EPR)-spin probing analysis of thyroid tissue
Free radicals are highly reactive species with half-lives usually less than 1 ms and are hardly detectable by direct EPR technique alone. This limitation is overcome by combining the EPR technique with spin probing. In brief, an organic compound (in our case 1-hydroxy-3-carboxy-pyrrolidine (CPH), capable of reacting with the radical species present, is added into the study system. The reaction product is a nitroxide radical (CP·), which is much more stable and therefore easily detectable by EPR technique [21]. Spectra were measured on a Bruker ECS 106 spectrometer equipped with a variable-temperature unit (ER4111VT). Samples were drawn up into a gas-permeable Teflon tube with 0.81-mm internal diameter and 0.05-mm wall thickness (Zeuss Industrial Products, Raritan, NJ, USA). The Teflon tube was folded four times, inserted into an open (air) quartz tube, and fixed to the EPR cavity (4108 TMH). The temperature was 37 °C. All ESR spectra were corrected for baseline drift by a linear function and double integrated and simulated using the software supplied by Bruker (ESP 1600 data system). Spectrometer conditions common to all spectra were modulation frequency, 100 kHz; microwave frequency, 9.4 GHz; microwave power, 20 mW.
Statistical analysis
All data were expressed as the mean (± standard deviation) of at least three measurements and analyzed with the Student’s t test or Two-Way ANOVA with Bonferroni post-test using the statistical software Graph Pad Prism 4.0 (GraphPad Software, Inc., CA, USA).
Results
Surgical treatment and outcome
All patients underwent total thyroidectomy. Therapeutic lymph node dissection was performed when cervical lymph node metastases were suspected or shown preoperatively or intraoperatively by the clinical or radiological examination. For all patients, the recovery was uneventful, and discharge was on the third postoperative day. No significant decrease was detected in blood calcium levels after surgery.
Thyroid histological analysis and staging
Histology of the thyroid tissue demonstrated papillary thyroid cancer in all patients: 16 patients with classical variant (4 with multifocal cancer), and 4 patients with follicular variant. Cervical neck dissection was performed on 15 patients with clinically involved lymph nodes, and lymph node metastases were found in 10 patients. Table 1 summarizes the preoperative cytological diagnosis, the post-operative histological classification, the surgical approach, and the staging.
Evaluation of GPx1 and TrxR1 expression in thyroid tissue
The overall protein composition of each patient’s thyroid tissue was determined by SDS-PAGE, and the protein content was verified by a specific protein staining (data not shown). The expression of GPx1 and TrxR1 was detected by the appropriate antibodies, able to identify only these two proteins in the thyroid protein lysate. Figures 1 and 2 show the Western blotting results referred to GPx1 and TrxR1, respectively. For each patient, two samples were tested for the presence of GPx1 and TrxR1: one sample from the healthy thyroid tissue and one sample from the cancer tissue. As demonstrated in Fig. 1, the intensity of the band detected by the anti-GPx1 antibody in thyroid cancer tissue was lower for all patients than those detected in healthy tissue. Similar results were obtained using the anti-TrxR1 antibody. In fact, all patients showed a decrease of the TrxR1 expression in cancer tissue compared to the healthy tissue. These findings support the hypothesis that an impairment in the ability of the antioxidant system to counteract oxidative stress may be implicated in thyroid cancer.

a Densitometric analysis of Western blotting reveals a meaningful decrease of the GPx expression (− 44.4 ± 2.8%, p < 0.01) in cancer (red line) with respect to the healthy thyroid tissue (black line). No differences were found between cancer and healthy tissue for the actin expression (data not shown). b Western blotting analysis of GPx1 and actin expression in cancer (C) and healthy (H) thyroid tissue. The numbers below identify the patient (see Table 1). NS not significant, *p < 0.01)

a Densitometric analysis of Western blotting shows also in this case a significant decrease of TrxR1 expression (− 49 ± 1.2%, p < 0.01) in cancer (red line) with respect to the healthy thyroid tissue (black line). b Western blotting analysis of TrxR1 and actin in cancer (C) and healthy (H) thyroid tissue shows a general reduction of TrxR1 in cancer (C). The numbers below identify the patient (see Table 1). NS not significant, *p < 0.01
Densitometric analyses of antioxidant enzyme expression
Western blot analyses showed a decrease in GPx1 and TrxR1 expression in thyroid cancer, without a real quantification of the difference. In order to better quantify our results, we performed a densitometric analyses of the bands representing GPx1 and TrxR1 in the western blot. To be sure that these results were not due to a different protein content between the two types of tissue, we decided to normalize our results with respect to actin, a ubiquitous protein present in all eukaryotic cells. Taking all patients together, the densitometric analysis of the GPx1 expression showed a significant lower mean concentration in cancer tissue, compared to healthy tissue. GPx1 expression in cancer tissue (red line, Fig. 1a) was 44.4 ± 2.8% less than the average values detected in healthy tissue (black line, Fig. 1a) (p < 0.001, range + 27 to − 74%). Furthermore, the difference of the GPx1 expression between healthy and cancer tissue, measured for each patient, was statistically significant for 16 of the 20 patients studied (Fig. 1b). The average TrxR1 expression was also decreased in tumor tissue when compared to healthy tissue, a difference of 49 ± 1.2% (p < 0.001, range − 3 to − 63%). Moreover, the mean values of the peaks obtained by the densitometric analysis of TrxR1 expression in thyroid cancer tissue (red line, Fig. 2a) were significantly lower than those measured in healthy tissue (black line, Fig. 2a), 98,965 ± 103,326 vs. 1,963,000 ± 91,242 a.u., p < 0.0001, respectively. Comparing individual patients’ tumor tissue to their own healthy tissue, the difference of TrxR1 expression was statistically significant for everyone (Fig. 2b).
Free radical production in thyroid cancer detected by EPR-spin probing
As previously described [20] EPR-spin technique has proved very useful in being able to detect free radicals within some human tissues. Using this technique, we detected a significant increase in the production of free radicals in all of the thyroid tumor tissue samples, compared to the healthy tissue of the same patient. In particular, the mean value detected in the cancer tissues was 12.07 ± 0.97 a.u., while that detected in healthy tissues was 5.58 ± 0.89 a.u. p < 0.01). These data indicate, unequivocally, that the process of carcinogenesis is closely related to the physiological mechanisms responsible for the balance between oxidants and antioxidants species (Fig. 3).

EPR measurement of reactive oxygen species in thyroid tissue. The red line shows the concentration of CP· in cancer tissue (C), while the black line shows the concentration of CP· detected in healthy thyroid tissue (H). The statistical analysis was significant for all patients
Discussion
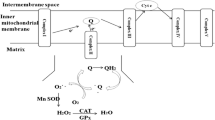
It has been suggested that up to 100 selenoproteins may exist in mammalian systems [22], of which up to 30 have been identified by 75Se labeling in vivo [23]. GPx enzymes, known as classical GPx1 (the first selenoprotein identified), gastrointestinal GPx2, plasma GPx3 and phospholipid hydroperoxide GPx4, represent the major classes of functionally important selenoproteins. GPx1 is ubiquitously expressed in many tissues and is present in the cell cytosol and in the mitochondria, where it functions as an antioxidant by directly reducing H2O2 to water and lipid hydroperoxides to their corresponding alcohol [24]. It may also act as a storage vehicle for selenium, containing 4 selenocysteine residues in a tetrameric structure [25, 26].
Another interesting selenoprotein is TrxR, an enzyme that catalyzes the NADPH-dependent reduction of thioredoxin and therefore plays a regulatory role in its metabolic activity. In fact, thioredoxins are proteins characterized at the level of their amino acid sequence by the presence of two cysteines that act as antioxidants by facilitating the reduction of other oxidized proteins by cysteine thiol-disulfide exchange [27]. TrxR is the only enzyme known to catalyze the reduction of thioredoxin. In brief, the electrons are taken from NADPH via TrxR and transferred to the active site of thioredoxin, which goes on to reduce protein disulfides or other substrates.
Moreover, thioredoxin stimulates proliferation of normal and tumor cells, and is present in high concentrations in tumor cells [28], so an impairment of the TrxR activity may be involved in some forms of cancer. In fact, the expression levels of the cytosolic isoform Trx1 and TrxR1 are linked to tumor aggressiveness, chemo-resistance and to resistance to apoptosis [29,30,31]. As previously described, numerous types of cancer cells have high levels of free radicals [32,33,34]. Cancer cells with elevated free radicals production frequently present a compromised antioxidant defense system, which will give rise to an overproduction of free radicals and the consequent increase in oxidative stress, resulting in the impairment of some physiological activities such as cellular metabolism, cellular growth and mitosis [35].
The coupling of the EPR-spin trapping probing technique with CPH can be used to assess the redox pro-oxidant state of cells, both in physiological and pathological conditions. The EPR technique is able to detect the oxidizing species produced and is extremely sensitive to the changes in the redox state [36, 37]. A refined technique like EPR gave us the opportunity to detect the overproduction of free radicals in cancer cell lysate compared to those detected in healthy thyroid tissue.
In this preliminary study, we show that oxidative stress in thyroid cancer is increased compared to that detected in healthy tissues, as suggested by the statistically higher CP· concentration. Moreover, the decrease in antioxidant enzymes GPx1 and TrxR1 in cancer tissue indicates that the antioxidant system in cancer cells is unable to adequately counteract the effects of the free radicals. All patients affected by thyroid cancer showed a reduced expression of these two antioxidants enzymes in tumor tissue, compared to those detected in healthy tissue.
Several different mechanisms are involved in the overproduction of free radicals, resulting in the augmented oxidative stress that afflicts thyroid cancer. As a result, the oxidative stress can only be partially explained by taking into account the defective antioxidant system of seleno-enzymes GPx1 and TrxR1. There are many sophisticated changes in the biology of cancer cells, so to consider only these enzymes as responsible for thyroid cancer is reductive, although our study shows that a contribution of GPxr1 and TrxR1 is likely possible. There are numerous variabilities that we were unable to account for in this small pilot study, such as the size of tumor, lymph node involvement, the multifocality of cancer, or the histotype of cancer. Moreover, our small population of subjects limited our statistical power, though, by comparing healthy vs. tumor samples within the same patient, we attempted to control for many between-patient variables.
Conclusions
Our findings show, unequivocally, the involvement of oxidative stress in thyroid cancer by demonstrating the imbalance of the oxidant/antioxidant system directly in thyroid cancer tissue. Further studies on the distribution of antioxidant molecules in cancer cells and the characterization of free radical intracellular pathways will be the critical steps in defining the role of the oxidant/antioxidant system in the thyroid cancer. The data obtained in our pilot study push us to further explore the role of seleno-enzymes in cancer. Currently, we are increasing our sample size and performing metabolic studies, with the use of magnetic resonance, to detect changes in metabolites of thyroid cancer cells.
Abbreviations
- GPx1:
-
glutathione peroxidase
- TrxR1:
-
thioredoxin reductases
- TT:
-
total thyroidectomy
- EPR:
-
electron paramagnetic resonance
- TPOAb:
-
anti-thyroperoxidase antibodies
- TgAb:
-
anti-thyroglobulin antibodies
- CPH:
-
1-hydroxy-3-carboxy-pyrrolidine
- CP·:
-
3-carboxy-proxyl radical
- US:
-
ultrasound
References
Halliwell B. Lipid peroxidation, antioxidants and cardiovascular disease: how should we move forward? Cardiovasc Res. 2000;47:410–8.
Halliwell B. Reactive oxygen species and the central nervous system. J Neurochem. 1992;59:1609–23.
Halliwell B, Gutteridge JM, Cross CE. Free radicals, antioxidants, and human disease: where are we now? J Lab Clin Med. 1992;119:598–620.
Visioli F, Keaney JF, Halliwell B. Antioxidants and cardiovascular disease; panaceas or tonics for tired sheep? Cardiovasc Res. 2000;47:409.
Mallozzi C, Martire A, Domenici MR, Metere A, Popoli P, Di Stasi AMM. L-NAME reverses quinolinic acid-induced toxicity in rat corticostriatal slices: involvement of src family kinases. J Neurosci Res. 2007;85:2770–7.
Afanas’ev I. Signaling of reactive oxygen and nitrogen species in Diabetes mellitus. Oxid Med Cell Longev. 2010;3:361–73.
Obulesu M, Venu R, Somashekhar R. Lipid peroxidation in Alzheimer’s disease: emphasis on metal-mediated neurotoxicity. Acta Neurol Scand. 2011;124:295–301.
Metere A, Mallozzi C, Minetti M, Domenici MR, Pèzzola A, Popoli P, Di Stasi AMM. Quinolinic acid modulates the activity of src family kinases in rat striatum: in vivo and in vitro studies. J Neurochem. 2006;97:1327–36.
Minetti M, Pietraforte D, Straface E, Metere A, Matarrese P, Malorni W. Red blood cells as a model to differentiate between direct and indirect oxidation pathways of peroxynitrite. Methods Enzymol. 2008;440:253–72.
Straface E, Marchesi A, Gambardella L, Metere A, de Jacobis IT, Viora M, Giordani L, Villani A, Del Principe D, Malorni W, et al. Does oxidative stress play a critical role in cardiovascular complications of Kawasaki disease? Antioxid Redox Signal. 2012;17(10):1441–6.
Young O, Crotty T, O’Connell R, O’Sullivan J, Curran AJ. Levels of oxidative damage and lipid peroxidation in thyroid neoplasia. Head Neck. 2010;32:750–6.
Akinci M, Kosova F, Cetin B, Sepici A, Altan N, Aslan S, Cetin A. Oxidant/antioxidant balance in patients with thyroid cancer. Acta Cir Bras. 2008;23:551–4.
Metere A, Chiesa C, Di Cosimo C, Fierro G, Giacomelli L, Pietraforte D. A novel approach to study oxidative stress in thyroid diseases: a preliminary study. Eur Rev Med Pharmacol Sci. 2012;16:646–52.
Lushchak VI. Free radicals, reactive oxygen species, oxidative stresses and their classifications. Ukr Biochem J. 2015;87:11–8.
Graffouillère L, Deschasaux M, Mariotti F, Neufcourt L, Shivappa N, Hébert JR, Wirth MD, Latino-Martel P, Hercberg S, Galan P, et al. Prospective association between the Dietary Inflammatory Index and mortality: modulation by antioxidant supplementation in the SU.VI.MAX randomized controlled trial. Am J Clin Nutr. 2016;103:878–85.
Lubos E, Loscalzo J, Handy DE. Glutathione peroxidase-1 in health and disease: from molecular mechanisms to therapeutic opportunities. Antioxid Redox Signal. 2011;15:1957–97.
Koháryová M, Kollárová M. Thioredoxin system—a novel therapeutic target. Gen Physiol Biophys. 2015;34:221–33.
Nardi F, Basolo F, Crescenzi A, Fadda G, Frasoldati A, Orlandi F, Palombini L, Papini E, Zini M, Pontecorvi A, et al. Italian consensus for the classification and reporting of thyroid cytology. J Endocrinol Invest. 2014;37:593–9.
Cooper DS, Doherty GM, Haugen BR, Hauger BR, Kloos RT, Lee SL, Mandel SJ, Mazzaferri EL, McIver B, Pacini F, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–214.
Schneider CA, Rasband WS, Eliceiri KW. NIH Image to Image J. 25 years of image analysis. Nat Methods. 2012;9:671–5.
Davies MJ. Detection and characterisation of radicals using electron paramagnetic resonance (EPR) spin trapping and related methods. Methods. 2016;109:21–30.
Burk RF, Hill KE. Regulation of selenoproteins. Annu Rev Nutr. 1993;13:65–81.
Evenson JK, Sunde RA. Selenium incorporation into selenoproteins in the Se-adequate and Se-deficient rat. Proc Soc Exp Biol Med. 1988;187:169–80.
Rotruck JT, Pope AL, Ganther HE, Swanson AB, Hafeman DG, Hoekstra WG. Selenium: biochemical role as a component of glutathione peroxidase. Science. 1973;179:588–90.
Burk RF. Molecular biology of selenium with implications for its metabolism. FASEB J. 1991;5:2274–9.
Chu FF, Doroshow JH, Esworthy RS. Expression, characterization, and tissue distribution of a new cellular selenium-dependent glutathione peroxidase, GSHPx-GI. J Biol Chem. 1993;268:2571–6.
Sun QA, Wu Y, Zappacosta F, Jeang KT, Lee BJ, Hatfield DL, Gladyshev VN. Redox regulation of cell signaling by selenocysteine in mammalian thioredoxin reductases. J Biol Chem. 1999;274:24522–30.
Holmgren A, Björnstedt M. Thioredoxin and thioredoxin reductase. Methods Enzymol. 1995;252:199–208.
Eriksson SE, Prast-Nielsen S, Flaberg E, Szekely L, Arnér ESJ. High levels of thioredoxin reductase 1 modulate drug-specific cytotoxic efficacy. Free Radical Biol Med. 2009;47:1661–71.
Grogan TM, Fenoglio-Prieser C, Zeheb R, Bellamy W, Frutiger Y, Vela E, Stemmerman G, Macdonald J, Richter L, Gallegos A, et al. Thioredoxin, a putative oncogene product, is overexpressed in gastric carcinoma and associated with increased proliferation and increased cell survival. Hum Pathol. 2000;31:475–81.
Raffel J, Bhattacharyya AK, Gallegos A, Cui H, Einspahr JG, Alberts DS, Powis G. Increased expression of thioredoxin-1 in human colorectal cancer is associated with decreased patient survival. J Lab Clin Med. 2003;142:46–51.
Toyokuni S, Okamoto K, Yodoi J, Hiai H. Persistent oxidative stress in cancer. FEBS Lett. 1995;358:1–3.
Schumacker PT. Reactive oxygen species in cancer cells: live by the sword, die by the sword. Cancer Cell. 2006;10:175–6.
Trachootham D, Alexandre J, Huang P. Targeting cancer cells by ROS-mediated mechanisms: a radical therapeutic approach? Nat Rev Drug Discov. 2009;8:579–91.
Metere A, Iorio E, Pietraforte D, Podo F, Minetti M. Peroxynitrite signaling in human erythrocytes: synergistic role of hemoglobin oxidation and band 3 tyrosine phosphorylation. Arch Biochem Biophys. 2009;484(2):173–82.
Suzen S, Gurer-Orhan H, Saso L. Detection of reactive oxygen and nitrogen species by electron paramagnetic resonance (EPR) technique. Molecules. 2017;22:181.
Abbas K, Babić N, Peyrot F. Use of spin traps to detect superoxide production in living cells by electron paramagnetic resonance (EPR) spectroscopy. Methods. 2016;109:31–43.
Authors’ contributions
AM designed this study and carried out the study and drafted the manuscript. DP performed EPR analysis, FF, ADL and MV carried out the statistical and data analyses. CEG and LG assisted with the manuscript preparation. All authors read and approved the final manuscript.
Acknowledgements
This work represents a Ph.D. research project of the Doctorate “Biotechnology in Clinical Medicine” and the Doctorate “Advanced Surgical Technologies” of the “Sapienza”, University of Rome. We are grateful to Prof. S. Filetti, and his laboratory equipe, for the management of the thyroid samples, and to prof. M. Arca and P. Trapani for the helpful advice.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The data supporting the conclusions of this paper are included within the article.
Consent for publication
All authors are responsible for the submission of this article and accept the conditions of submission.
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards and with the ethical standards of the ethics committee of the Umberto I Hospital of Rome that approved the study (Id Number: 4240). All the patients provided written informed consent for the use of clinical specimens for medical research.
Funding
Not applicable.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Metere, A., Frezzotti, F., Graves, C.E. et al. A possible role for selenoprotein glutathione peroxidase (GPx1) and thioredoxin reductases (TrxR1) in thyroid cancer: our experience in thyroid surgery. Cancer Cell Int 18, 7 (2018). https://doi.org/10.1186/s12935-018-0504-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12935-018-0504-4