
Abstract
Background
Serum haptoglobin (Hp) has been closely associated with cardio-cerebrovascular diseases. We investigated a metabolic profile associated with circulating Hp and carotid arterial functions via a targeted metabolomics approach to provide insight into potential mechanisms.
Methods
A total of 240 participants, including 120 patients with type 2 diabetes mellitus (T2DM) and 120 non-diabetes mellitus (non-DM) subjects were recruited in this study. Targeted metabolic profiles of serum metabolites were determined using an AbsoluteIDQ™ p180 Kit (BIOCRATES Life Sciences AG, Innsbruck, Austria). Ultrasound of the bilateral common carotid artery was used to measure intima-media thickness and inter-adventitial diameter. Serum Hp levels were tested by enzyme-linked immunosorbent assay.
Results
Serum Hp levels in T2DM patients and non-DM subjects were 103.40 (72.46, 131.99) mg/dL and 100.20 (53.99, 140.66) mg/dL, respectively. Significant differences of 19 metabolites and 17 metabolites were found among serum Hp tertiles in T2DM patients and non-DM subjects, respectively (P < 0.05). Of these, phosphatidylcholine acyl-alkyl C32:2 (PC ae C32:2) was the common metabolite observed in two populations, which was associated with the serum Hp groups and lipid traits (P < 0.05). Furthermore, the metabolite ratios of two acidic amino acids, including aspartate to PC ae C32:2 (Asp/PC ae C32:2) and glutamate to PC ae C32:2 (Glu/PC ae C32:2) were correlated with serum Hp, carotid arterial functions and other biochemical index in both populations significantly (P < 0.05).
Conclusions
Targeted metabolomics analyses might provide a new insight into the potential mechanisms underlying the association between serum Hp and carotid arterial functions.
Similar content being viewed by others


Background
Type 2 diabetes mellitus (T2DM) represents a heterogeneous group of chronic metabolic disorders, and its increasing prevalence has led to an explosion of the global disease burden with increased mortality and morbidity [1, 2]. Systemic metabolic dysfunctions, such as hyperglycaemia, insulin resistance and dyslipidaemia, give rise to an elevated risk of cardio-cerebrovascular diseases, including cerebral infarction, stroke, and heart attacks [3, 4]. The pathogenesis underlying macroangiopathy is complicated and yet not well clarified [5,6,7,8]. A group of studies was previously launched to explore the causality underlying the relationship of several novel biomarkers with macroangiopathy risk [9,10,11], and a causal relationship between serum haptoglobin (Hp) levels and macroangiopathy was observed in Chinese T2DM patients via Mendelian randomization analysis [12].
As a kind of acute-phase response protein, serum Hp is mainly synthesized by hepatocytes and is widely distributed in the circulation in humans [13]. The main physiological function of serum Hp is binding free haemoglobin released from red blood cell lysis and protecting tissues and vessels from oxidative damage [14]. Several studies have reported that increases in circulating Hp levels were observed in T2DM patients and general population with cardio-cerebrovascular diseases [15,16,17]. Furthermore, it has been proposed that the influence of Hp on the cholesterol level might be related to the ability of Hp to bind apolipoprotein E, which is closely related to lipid metabolism and carotid atherosclerosis [18]. Thus, understanding the mechanisms underlying the interactions involving serum Hp, lipid metabolism and carotid arterial functions might provide a novel clue for the prevention and treatment of cardio-cerebrovascular diseases in T2DM patients and general population.
Recently, metabolomics has been used as a more expeditious and sensitive approach to explore changes in metabolic profiles of chronic metabolic diseases [19, 20]. Metabolites indicate intermediates and end products of metabolic pathways, including carbohydrates, fatty acids, amino acids, pigments, nucleotides, organic acids, vitamins and many other classes of compounds [21]. Changes in metabolites in organisms, tissues or cells are direct indicators of variation in the physiology and pathology of diseases [22]. In current metabolomics research, the three different approaches adopted in the measurement of metabolites are metabolic fingerprinting, metabolite profiling and targeted metabolomics [23].
In the current study, we aimed to investigate whether a targeted metabolomics approach involving a broader spectrum of metabolites may help to identify metabolites associated with the serum Hp levels in Chinese T2DM patients and non-diabetes mellitus (non-DM) subjects. Furthermore, analyses of the altered metabolites and metabolite ratios with the traits of carotid arterial functions, including intima-media thickness (IMT) and inter-adventitial diameter (IAD) of the bilateral common carotid arteries, were performed to provide further insight into the potential mechanisms involved.
Methods
Subjects
A total of 240 participants were enrolled in this study, including 120 T2DM patients from the Shanghai Diabetes Institute Inpatient Database and 120 non-DM subjects from the Shanghai Nicheng Cohort Study [24]. T2DM and non-DM were diagnosed by the 1999 WHO criteria following a 75 g oral glucose tolerance test. Written informed consent was obtained from all patients. This current study complied with the Declaration of Helsinki and was approved by the Institutional Review Board of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai, China. Exclusion criteria were subjects with cancer, severe disability, psychiatric disturbances, type 1 diabetes, pregnancy, haemolytic disease, cardiac failure, severe infection, and drug or alcohol addiction. Fasting venous blood samples of all patients were collected and centrifuged, and the separated serum samples were transferred and stored at − 80 °C until assayed.
Clinical examination
Anthropometric characteristics of all 240 participants, such as age, sex, height, weight, and duration of diabetes (years), were recorded. Body mass index (BMI) was defined as weight (kg)/height2 (m2). Blood pressure was measured using a mercury sphygmomanometer by an experienced physician, and the mean values of three repeated measurements were recorded. A vascular ultrasound was used to examine the bilateral common carotid arteries. Information on the IMT and IAD was recorded in T2DM patients and IMT was used in non-DM subjects. The mean values of IMT and IAD of the bilateral common carotid arteries were calculated for further analysis. Haemoglobin A1c (HbA1c) levels were measured by a Bio-Rad Variant II haemoglobin testing system (Bio-Rad Laboratories, Hercules, USA). Blood lipid profiles, which included levels of total cholesterol, triglycerides, high-density lipoprotein-cholesterol (HDL-C), and low-density lipoprotein-cholesterol (LDL-C), were tested by a Hitachi 7600-020 Automated Analyzer (Hitachi, Tokyo, Japan).
Metabolite measurements
The metabolite measurements were conducted via a targeted metabolomics approach by using an AbsoluteIDQ™ p180 Kit (BIOCRATES Life Sciences AG, Innsbruck, Austria) combined with flow injection analysis and liquid chromatography–tandem mass spectrometry. A total of 184 metabolites were detected by this kit, including 40 acylcarnitines (C x:y), 87 glycerophospholipids [14 lyso-phosphatidylcholines (lyso-PCs) (lyso-PC x:y) and 73 phosphatidylcholines (PCs) (35 PC aa x:y and 38 PC ae x:y)], 14 sphingolipids (SM x:y or SM (OH) x:y), 21 amino acids, 21 biogenic amines and 1 hexose. Glycerophospholipids were differentiated according to the presence of ester and ether bonds in the glycerol moiety. Double letters of “aa” or “ae” indicate that two glycerol positions are bound to a fatty acid residue via an ester bond or ether bond, whereas a single letter of “a” or “e” represents only one fatty acid residue bound to the glycerol backbone. The abbreviation “C x:y” is used to indicate the composition of a lipid fatty side chain, where “x” represents the number of carbon atoms and “y” indicates the number of double bonds in the side chain. The assay procedures for measurements and quality control followed the kit manufacturer’s instructions [25]. The samples were analysed using a Waters XEVO™ TQ mass spectrometer (Waters, Manchester, UK) coupled with a Waters ACQUITY(®) ultra performance liquid chromatography (UPLC). Biocrates MetIQ™ software (BIOCRATES Life Sciences AG, Innsbruck, Austria) was used to quantify metabolite concentrations and assess the quality of metabolites automatically. Identification and calculations of the metabolite concentration were achieved using internal standards. Metabolite concentrations were reported in the unit of μmol/L (μM), and an Excel file was exported for further statistical analyses. Metabolites below the limit of detection were excluded from further analysis.
Circulating Hp detection
An enzyme-linked immunosorbent assay (ELISA) was used to measure Hp concentrations by using a Human Haptoglobin Quantikine ELISA kit (R&D Systems, Inc., Minneapolis, USA) following the kit manufacturer’s instructions as described previously [12].
Statistical analyses
Statistical analyses of the quantitative characteristics were carried out using SAS for Windows (version 9.2; SAS Institute, Cary, NC, USA). Variables were subjected to normality tests, and any skewed quantitative trait data were logarithmically transformed before analysis. Statistical significance of clinical traits and metabolites among three groups of serum Hp levels tertiles (low Hp, middle Hp and high Hp) was determined by one-way analysis of variance (ANOVA) followed by Dunnett’s test to identify group differences at P < 0.05. Pearson correlation analysis was performed to evaluate correlations between two variables. Multiple linear regression analysis was used to test the association of metabolites and metabolite ratios with lipid traits after adjusting for confounding factors. All data are shown as n, the mean ± standard deviation or median (interquartile range). A two-tailed P value < 0.05 was considered nominally significant. A total of 184 metabolites were measured, and seven were excluded because of low detection quality. Bonferroni correction was applied to adjust for multiple testing (i.e., 177 tests for the analysis of metabolites association). Thus, associations of P < adjust P (0.05/177) = 2.8 × 10−4 for metabolites and serum Hp were considered significant. Comprehensive meta-analysis (version 2.2.057; Biostat, Englewood, New Jersey) was conducted to evaluate combined effects from two populations using a fixed or random effect model after testing for heterogeneity. The Cochran Q statistic and the I2 statistic were applied to assess the extent of heterogeneity.
Results
Basic clinical features
The median (interquartile range) values of serum Hp levels in T2DM patients and non-DM subjects were 103.40 (72.46, 131.99) mg/dL and 100.20 (53.99, 140.66) mg/dL, respectively. No significant difference was found in serum Hp levels between these two populations (P = 0.7315). Anthropometric and clinical characteristics of all the 240 participants grouped by serum Hp level tertiles are described in Table 1.
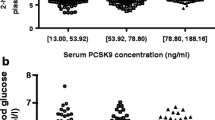
In T2DM patients, the median (interquartile range) values of serum Hp concentrations in low Hp, middle Hp and high Hp groups were 54.82 (3.60, 71.58) mg/dL, 103.20 (95.30, 107.27) mg/dL and 151.64 (131.12, 175.55) mg/dL, respectively. After comparison among groups, significant differences were found in sex (P = 0.0410), carotid IAD (P = 0.0088) and serum Hp levels (P < 0.0001) (Fig. 1). Furthermore, after adjusting for age, sex, BMI, blood pressure, duration of diabetes and HbA1c levels, the carotid IAD parameter was shown to have a significant relationship with serum Hp tertiles (P = 0.0042) (see Additional file 1: Table S1).

Serum haptoglobin levels and common carotid inter-adventitial diameter in T2DM patients. T2DM type 2 diabetes mellitus, Hp haptoglobin. Dot plot a shows a comparison of serum Hp levels among Hp tertiles, P < 0.0001. Dot plot b shows a comparison of common carotid artery inter-adventitial diameter levels among Hp tertiles, P = 0.0090. P values were determined by one-way analysis of variance. The Hp and carotid artery inter-adventitial diameter levels are shown in dot plots; the mean is indicated by the middle black solid line. The 95% confidence intervals are shown by the bottom and top black solid lines, respectively
In non-DM subjects, the median (interquartile range) values of serum Hp concentrations in low Hp, middle Hp and high Hp groups were 39.48 (17.23, 51.45) mg/dL, 99.41 (92.96, 113.38) mg/dL and 167.67 (140.35, 209.73) mg/dL, respectively, with a significant difference of serum Hp levels among three groups (P < 0.0001) (see Additional file 1: Figure S1). After adjusting for age, sex, BMI, blood pressure and HbA1c levels, no parameters was shown to have a significant relationship with serum Hp tertiles (P > 0.05) (see Additional file 1: Table S2).
Association between blood metabolites and serum Hp levels
A total of 184 metabolites were measured, and seven were excluded because of low detection quality. As a result, significant differences of 19 metabolites (2 acylcarnitines, 1 lyso-PCs, 12 PCs, and 4 amino acids) and 17 metabolites (5 acylcarnitines, 2 lyso-PCs, 7 PCs, and 3 amino acids) were found among the Hp level groups from the remaining 177 metabolites in T2DM patients and non-DM subjects, respectively (P < 0.05) (Table 2). After further linear regression analysis, 41 metabolites (1 acylcarnitine, 3 lyso-PCs, 33 PCs and 4 amino acids) and 17 metabolites (3 acylcarnitine, 1 lyso-PCs, 10 PCs and 3 amino acids) were found to be associated with serum Hp levels (P < 0.05) in T2DM patients and non-DM subjects, respectively (see Additional file 1: Table S3).
Selected metabolites associated with blood lipid traits
Multiple linear regression analysis was conducted to investigate the association of the altered metabolites with traits of blood lipids and carotid arterial functions (carotid IMT and carotid IAD). After adjusting for age, sex and BMI, 10 metabolites (1 lyso-PC, 7 PCs and 2 amino acids) and 10 metabolites (4 lyso-PC, 5 PCs and 1 amino acids) were found to be associated with the serum Hp groups and lipid traits in T2DM patients (Table 3) and non-DM subjects (Table 4), respectively. Among them, phosphatidylcholine acyl-alkyl C32:2 (PC ae C32:2) was the common metabolite associated with the serum Hp groups and lipid traits in both two populations. In T2DM patients, PC ae C32:2 was significantly correlated with total cholesterol (P = 0.0390), the serum Hp groups (P = 0.0005) and carotid IAD (P = 0.0182). In non-DM subjects, PC ae C32:2 was associated with HDL-C levels (P = 0.0133) and the serum Hp groups (P = 0.0390) significantly. The combined analysis of two populations by a meta-analysis revealed that PC ae C32:2 was correlated with the serum Hp groups (β ± SE = − 0.028 ± 0.007, P = 3.01 × 10−5). The Cochran Q test showed no heterogeneity in the relationships between PC ae C32:2 and serum Hp from T2DM patients and non-DM subjects (I2 = 0, P = 0.874). The levels of PC ae C32:2 in T2DM patients and non-DM subjects grouped by serum Hp levels are shown in Fig. 2.

Blood levels of metabolite PC ae C32:2 in subjects grouped by serum Hp levels. Hp haptoglobin, T2DM type 2 diabetes mellitus, Non-DM non-diabetes mellitus. Dot plot a shows the association of blood metabolite PC ae C32:2 with serum Hp tertiles in T2DM patients, P = 0.0005, β ± SE = − 0.028 ± 0.008. Dot plot b shows the association of blood metabolite PC ae C32:2 with serum Hp tertiles in non-DM patients, P = 0.0390, β ± SE = − 0.026 ± 0.012. P values and beta values were determined by multiple linear regression adjusting for age, sex, body mass index, total cholesterol, triglycerides, high-density lipoprotein-cholesterol, low-density lipoprotein-cholesterol, inter-adventitial diameter and/or carotid intima-media thickness. The PC ae C32:2 levels are shown in dot plots; the median is indicated by the middle black solid line. The lower and upper quartiles are shown by the bottom and top black solid lines, respectively
Metabolite ratios associated with clinical traits
In addition, changes in metabolite ratios might reflect biological situations such as changes in enzyme activities or imbalances in metabolic pathways [26]. The metabolite ratio of valine to PC ae C32:2 (Val/PC ae C32:2) was previously reported to be associated with an increased risk of type 2 diabetes and measures of insulin secretion and resistance [27]. In the current study, the ratios of 21 amino acids to PC ae C32:2 were compared to evaluate the association between serum Hp levels and clinical traits.
We found the metabolite ratios of 5 aliphatic amino acids (asparagine, aspartate, glutamate, isoleucine and valine) to PC ae C32:2 were associated with blood lipids, the serum Hp groups, and carotid IMT and/or IAD after adjusting for age, sex and BMI in T2DM patients (P < 0.05) (Table 5 and Additional file 1: Table S4). In non-DM subjects, the metabolite ratios of three amino acids (aspartate, glutamate, and phenylalanine) to PC ae C32:2 were associated with blood lipids, the serum Hp groups and carotid IMT after adjusting for age, sex and BMI (P < 0.05) (Table 6 and Additional file 1: Table S5).
Of these, the metabolite ratios of two acidic amino acids, including aspartate to PC ae C32:2 (Asp/PC ae C32:2) and glutamate to PC ae C32:2 (Glu/PC ae C32:2) were the common significant ratios observed in both populations. The combined analysis of two populations by a meta-analysis revealed that Asp/PC ae C32:2 and Glu/PC ae C32:2 were correlated with the serum Hp groups (β ± SE = 0.045 ± 0.010, P = 1.45 × 10−5; β ± SE = 0.041 ± 0.011, P = 2.38 × 10−4), respectively. The Cochran Q test showed no heterogeneity in the relationships of Asp/PC ae C32:2 and Glu/PC ae C32:2 with serum Hp from T2DM patients and non-DM subjects (I2 = 0, P = 0.740; I2 = 0, P = 0.860), respectively. The ratios of Asp/PC ae C32:2 and Glu/PC ae C32:2 in T2DM patients and non-DM subjects grouped by serum Hp levels are shown in Figs. 3, 4, respectively.

Metabolite ratios of two acidic amino acids to PC ae C32:2 in T2DM patients. T2DM type 2 diabetes mellitus, Hp haptoglobin, Asp aspartate, Glu glutamate. Dot plot a shows the association of blood metabolite ratio Asp to PC ae C32:2 (Log transformed) with serum Hp tertiles, P = 0.0059, β ± SE = 0.041 ± 0.015. Dot plot b shows the association of blood metabolite ratio Glu to PC ae C32:2 (Log transformed) with serum Hp tertiles, P = 0.0160, β ± SE = 0.039 ± 0.016. P values and beta values were determined by multiple linear regression adjusting for age, sex, body mass index, total cholesterol, triglycerides, high-density lipoprotein-cholesterol, low-density lipoprotein-cholesterol, carotid intima-media thickness and inter-adventitial diameter. Metabolite ratios (Log transformed) are shown in dot plots; the median is indicated by the middle black solid line. The lower and upper quartiles are shown by the bottom and top black solid lines, respectively

Metabolite ratios of two acidic amino acids to PC ae C32:2 in non-DM subjects. Non-DM non-diabetes mellitus, Hp haptoglobin, Asp aspartate, Glu glutamate. Dot plot a shows the association of blood metabolite ratio Asp to PC ae C32:2 (Log transformed) with serum Hp tertiles, P = 0.0012, β ± SE = 0.048 ± 0.015. Dot plot b shows the association of blood metabolite ratio Glu to PC ae C32:2 (Log transformed) with serum Hp tertiles, P = 0.0071, β ± SE = 0.043 ± 0.016. P values and beta values were determined by multiple linear regression adjusting for age, sex, body mass index, total cholesterol, triglycerides, high-density lipoprotein-cholesterol, low-density lipoprotein-cholesterol and carotid intima-media thickness. Metabolite ratios (Log transformed) are shown in dot plots; the median is indicated by the middle black solid line. The lower and upper quartiles are shown by the bottom and top black solid lines, respectively
Discussion
In the current study, serum Hp levels in T2DM patients and non-DM subjects were 103.40 (72.46, 131.99) mg/dL and 100.20 (53.99, 140.66) mg/dL, respectively. Significant differences of 19 metabolites and 17 metabolites were found among serum Hp tertiles in T2DM patients and non-DM subjects, respectively. Among them, the phosphatidylcholine PC ae C32:2 was shown to be notably correlated with the serum Hp groups and lipid traits in both two populations. Furthermore, the metabolite ratios of two acidic amino acids, including aspartate to PC ae C32:2 (Asp/PC ae C32:2) and glutamate to PC ae C32:2 (Glu/PC ae C32:2) were associated with serum Hp, carotid arterial functions and other biochemical index significantly. These findings might provide a new insight into the potential mechanisms underlying the association between serum Hp and carotid arterial functions.
An acute-phase glycoprotein, Hp was identified in 1938 for the first time. This protein is produced mostly by hepatocytes and is widely distributed in the circulation in humans. The main physiological function of Hp is binding free haemoglobin with high affinity to form a stable haemoglobin–haptoglobin (Hb–Hp) complex, thereby protecting tissues and vessels from oxidative damage. In the range of 50–300 mg/dL, the circulating level of Hp ranks only behind the predominant plasma proteins albumin and immunoglobulins [13]. Several studies reported that circulating Hp levels were correlated with the progression of cardio-cerebrovascular diseases in T2DM patients and general population [16, 17]. Furthermore, a causal relationship between serum Hp levels and macroangiopathy was previously observed in Chinese T2DM patients via Mendelian randomization analysis [12]. Therefore, it is important to study the mechanisms underlying the interactions involving serum Hp and carotid arterial functions to provide a novel insight into the prevention and treatment for cardio-cerebrovascular diseases.
The advent of metabonomics, a new rapidly developing technology, offers a more powerful and sensitive means to explain the aetiology of complex chronic diseases [19, 22]. Glycerophospholipids including PCs and lyso-PCs have recently gained attention as potential biomarkers of cardiovascular disease [28, 29]. PCs not only play a key role as a component of cellular membranes but also act as a reservoir for fatty acids [30]. Lyso-PCs mostly come from the partial hydrolysis of PCs catalysed mainly by phospholipase A1 (PLA1) and phospholipase A2 (PLA2), lecithin–cholesterol acyltransferase (LCAT) activity or hepatic secretion [31]. Due to the diverse composition of fatty acid residues binding to the glycerol backbone, individual PCs and lyso-PCs have different functional properties and reactions to oxidative stress [32,33,34,35]. A reduction in the levels of several individual PC and lyso-PC species has previously been reported in patients with atherosclerosis in comparison to those of healthy subjects via a targeted metabolomics approach [36], indicating that abnormal glycerophospholipid metabolism might be correlated with the aberrant activity of several enzymes, such as PLA1, PLA2 and LCAT, crucial components of oxidized LDL (Ox-LDL), which contributes to atherogenesis [37, 38].
In our study, the levels of 13 glycerophospholipids (1 lyso-PC and 12 PCs) and 9 glycerophospholipids (2 lyso-PC and 7 PCs) were observed to be significantly lower in the upper serum Hp tertile group than in the lower tertile group in T2DM patients and non-DM subjects, respectively. As reported previously, it was speculated that the influence of Hp on the cholesterol level might be related to the ability of Hp to bind apolipoprotein E, which results in the displacement and inhibition of the LCAT cholesterol esterification rate [18]. The decrease in levels of PC and lyso-PC species in patients with higher serum Hp concentrations, which might be caused by aberrant enzyme activity, provide a likely explanation for the potential mechanism underlying the interaction of serum Hp and lipid metabolism.
One highlight of the glycerophospholipids associated with serum Hp is PC ae C32:2, which was shown to be significantly correlated with carotid IAD in T2DM patients. Carotid IAD and IMT measured by ultrasound serve as a non-invasive surrogate for assessing the atherosclerotic process [39, 40]. Although carotid IMT is recommended for early detection and cardiovascular risk evaluation, the role of carotid IAD in cardiovascular outcomes prediction has gradually been recognized [41, 42]. Several studies observed that common carotid IAD and not carotid IMT was correlated with the prevalence of cardiovascular events and might have predictive value for cardiovascular outcomes [43, 44]. In our research, metabolite PC ae C32:2 was correlated with serum Hp and common carotid IAD in T2DM patients with a median diabetes duration of 10 years. We speculated that the lack of associations between metabolites and carotid IMT might due to several factors. One factor to take into consideration is vascular remodelling. With the deposition and development of atherosclerotic plaques, vascular remodelling occurs and results in increased carotid diameter, called the Glagov phenomenon [45]. As a sum of the lumen diameter and of IMT, carotid IAD is associated with carotid IMT, left ventricular mass and cardiovascular risk factors, which is more obvious to reflect the change of carotid arterial functions [46]. The other is the possibility that carotid IMT is more sensitive to metabolites in those patients with mild impaired glucose regulation or lower burdens of subclinical cardiovascular diseases than those with larger burden T2DM patients. Further studies should be carried out to cast insights into the mechanism behind the association of serum Hp and carotid arterial functions.
Interestingly, changes in the ratios between two single metabolites might reflect biological situations such as alterations in enzyme activities or imbalances in metabolic pathways relevant for a certain phenotype [47,48,49]. A study reported recently that the metabolite ratio of Val/PC ae C32:2 was not only associated with measures of oral glucose tolerance test -derived β cell function and insulin resistance but also correlated with an increased risk of T2DM [27]. The observed effects, independent of currently known risk factors, were stronger than those of the individual metabolites, indicating that the application of ratios might improve prediction above that of single metabolites.
Based on this background, the metabolite ratios of 21 amino acids to PC ae C32:2 were compared in this study to evaluate the association with serum Hp levels and clinical traits. As a result, we identified that the metabolite ratios of two acidic amino acids, including Asp/PC ae C32:2 and Glu/PC ae C32:2 were significantly correlated with serum Hp levels, carotid IMT or IAD, and other lipid metabolic parameters after adjusting for confounding factors. As reported previously, acidic amino acids, including aspartate and glutamate were identified to have an intrinsic peroxidase-like activity, which plays a key role in lipid oxidation [50]. It was speculated that metabolites found in our study might mediate the aberrant activity of several enzymes caused by the action of Hp binding to apolipoprotein E and apolipoprotein A-I, which disturbs cholesterol esterification and lipid oxidation, contributing to blood vessel endothelial dysfunction and atherogenesis [37, 38]. Changes in those metabolite ratios might reflect the alterations in enzyme activities relevant to the rate-limiting step in glycolipid catabolism [51, 52]. In view of this, we speculated that it might be useful for early identification of subjects with an increased risk of cardio-cerebrovascular diseases or helpful to identify potential drug targets for new therapies if verified by further prospective studies [53,54,55].
To the best of our knowledge, this is the first study to use a targeted metabolomics approach to analyse blood metabolites in relation to serum Hp levels and carotid arterial functions. However, there are several limitations in this research. First, the sample we recruited to perform metabolite measurements was relatively small, and large-scale studies are needed to confirm our results. Second, part of the explanation for our results is limited by the targeted metabolomics kit we used, as it does not provide a detailed analysis of the lipid composition of metabolites, such as PC ae C32:2. Its exact role in the physiology and molecular aetiology awaits examination in further functional studies. Third, as carotid IMT is recommended for early detection and cardiovascular risk evaluation in general population, carotid IAD was not recorded in non-DM subjects in this study. The association between serum Hp levels and carotid arterial functions should be evaluated in other complex diseases. Finally, a direct causal relationship cannot be established in view of the cross-sectional design of this study. Therefore, the findings identified in our study should be further validated in a prospective study.
Conclusions
To summarize, we show that a number of blood metabolites, especially PCs and lyso-PCs, were associated with serum Hp levels and blood lipid metabolism by using a targeted metabolomics approach in Chinese T2DM patients and non-DM subjects. This finding provides a new insight into potential mechanisms behind the interaction between serum Hp and carotid arterial functions. Furthermore, the metabolite ratios of two acidic amino acids, including Asp/PC ae C32:2 and Glu/PC ae C32:2 may be used to predict early risk of cardio-cerebrovascular diseases if validated in further studies.
Abbreviations
- T2DM:
-
type 2 diabetes mellitus
- Non-DM:
-
non-diabetes mellitus
- Hp:
-
haptoglobin
- IMT:
-
intima-media thickness
- IAD:
-
inter-adventitial diameter
- BMI:
-
body mass index
- HbA1c:
-
haemoglobin A1c
- HDL-C:
-
high-density lipoprotein-cholesterol
- LDL-C:
-
low-density lipoprotein-cholesterol
- lyso-PCs:
-
lyso-phosphatidylcholines
- PCs:
-
phosphatidylcholines
- UPLC:
-
ultra performance liquid chromatography
- μM:
-
μmol/L
- ELISA:
-
enzyme-linked immunosorbent assay
- ANOVA:
-
analysis of variance
- Hb–Hp:
-
haemoglobin–haptoglobin
- PLA1:
-
phospholipase A1
- PLA2:
-
phospholipase A2
- LCAT:
-
lecithin–cholesterol acyltransferase
- Ox-LDL:
-
oxidized LDL
References
Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–223.
Gu K, Cowie CC, Harris MI. Mortality in adults with and without diabetes in a national cohort of the U.S. population, 1971–1993. Diabetes Care. 1998;21(7):1138–45.
Newman JD, Schwartzbard AZ, Weintraub HS, Goldberg IJ, Berger JS. Primary prevention of cardiovascular disease in diabetes mellitus. J Am Coll Cardiol. 2017;70(7):883–93.
Mellbin LG, Anselmino M, Ryden L. Diabetes, prediabetes and cardiovascular risk. Eur J Cardiovasc Prev Rehabil. 2010;17(Suppl 1):S9–14.
Bao X, Borne Y, Johnson L, Muhammad IF, Persson M, Niu K, Engstrom G. Comparing the inflammatory profiles for incidence of diabetes mellitus and cardiovascular diseases: a prospective study exploring the ‘common soil’ hypothesis. Cardiovasc Diabetol. 2018;17(1):87.
Ijas P, Saksi J, Soinne L, Tuimala J, Jauhiainen M, Jula A, Kahonen M, Kesaniemi YA, Kovanen PT, Kaste M, et al. Haptoglobin 2 allele associates with unstable carotid plaque and major cardiovascular events. Atherosclerosis. 2013;230(2):228–34.
Dalan R, Liew H, Goh LL, Gao X, Chew DE, Boehm BO, Leow MK. The haptoglobin 2-2 genotype is associated with inflammation and carotid artery intima-media thickness. Diabetes Vasc Dis Res. 2016;13(5):373–6.
Orchard TJ, Backlund JC, Costacou T, Cleary P, Lopes-Virella M, Levy AP, Lachin JM, Group DER. Haptoglobin 2-2 genotype and the risk of coronary artery disease in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study (DCCT/EDIC). J Diabetes Complications. 2016;30(8):1577–84.
Jansen H, Samani NJ, Schunkert H. Mendelian randomization studies in coronary artery disease. Eur Heart J. 2014;35(29):1917–24.
Jimenez-Rosales A, Amaya-Chavez A, Dominguez Garcia MV, Camarillo-Romero E, Huitron Bravo GG, Cruz AM. Association of inflammatory and oxidative stress biomarkers in subjects with cardiovascular risk. Am J Ther. 2013;20(4):422–31.
Xuan Y, Gao X, Holleczek B, Brenner H, Schottker B. Prediction of myocardial infarction, stroke and cardiovascular mortality with urinary biomarkers of oxidative stress: results from a large cohort study. Int J Cardiol. 2018;273:223–9. https://doi.org/10.1016/j.ijcard.2018.08.002
Wang S, Wang J, Zhang R, Wang T, Yan D, He Z, Jiang F, Hu C, Jia W. Mendelian randomization analysis to assess a causal effect of haptoglobin on macroangiopathy in Chinese type 2 diabetes patients. Cardiovasc Diabetol. 2018;17(1):14.
Andersen CBF, Stodkilde K, Saederup KL, Kuhlee A, Raunser S, Graversen JH, Moestrup SK. Haptoglobin. Antioxid Redox Signal. 2017;26(14):814–31.
Alayash AI, Andersen CB, Moestrup SK, Bulow L. Haptoglobin: the hemoglobin detoxifier in plasma. Trends Biotechnol. 2013;31(1):2–3.
Can U, Buyukinan M, Guzelant A, Ugur A, Karaibrahimoglu A, Yabanciun S. Investigation of the inflammatory biomarkers of metabolic syndrome in adolescents. J Pediatr Endocrinol Metab. 2016;29(11):1277–83.
Awadallah S, Madkour M, Hamidi RA, Alwafa EA, Hattab M, Zakkour B, Al-Matroushi A, Ahmed E, Al-Kitbi M. Plasma levels of apolipoprotein A1 and lecithin: cholesterol acyltransferase in type 2 diabetes mellitus: correlations with haptoglobin phenotypes. Diabetes Metab Syndr. 2017;11(Suppl 2):S543–6.
Melander O, Modrego J, Zamorano-Leon JJ, Santos-Sancho JM, Lahera V, Lopez-Farre AJ. New circulating biomarkers for predicting cardiovascular death in healthy population. J Cell Mol Med. 2015;19(10):2489–99.
Cigliano L, Pugliese CR, Spagnuolo MS, Palumbo R, Abrescia P. Haptoglobin binds the antiatherogenic protein apolipoprotein E—impairment of apolipoprotein E stimulation of both lecithin:cholesterol acyltransferase activity and cholesterol uptake by hepatocytes. FEBS J. 2009;276(21):6158–71.
Sas KM, Karnovsky A, Michailidis G, Pennathur S. Metabolomics and diabetes: analytical and computational approaches. Diabetes. 2015;64(3):718–32.
Newgard CB. Metabolomics and metabolic diseases: where do we stand? Cell Metab. 2017;25(1):43–56.
Johnson CH, Ivanisevic J, Siuzdak G. Metabolomics: beyond biomarkers and towards mechanisms. Nat Rev Mol Cell Biol. 2016;17(7):451–9.
Lu J, Xie G, Jia W, Jia W. Metabolomics in human type 2 diabetes research. Front Med. 2013;7(1):4–13.
Klupczynska A, Derezinski P, Kokot ZJ. Metabolomics in medical sciences-trends, challenges and perspectives. Acta Pol Pharm. 2015;72(4):629–41.
Chen P, Hou X, Hu G, Wei L, Jiao L, Wang H, Chen S, Wu J, Bao Y, Jia W. Abdominal subcutaneous adipose tissue: a favorable adipose depot for diabetes? Cardiovasc Diabetol. 2018;17(1):93.
Qiu Y, Zhou B, Su M, Baxter S, Zheng X, Zhao X, Yen Y, Jia W. Mass spectrometry-based quantitative metabolomics revealed a distinct lipid profile in breast cancer patients. Int J Mol Sci. 2013;14(4):8047–61.
Suhre K, Raffler J, Kastenmuller G. Biochemical insights from population studies with genetics and metabolomics. Arch Biochem Biophys. 2016;589:168–76.
Molnos S, Wahl S, Haid M, Eekhoff EMW, Pool R, Floegel A, Deelen J, Much D, Prehn C, Breier M, et al. Metabolite ratios as potential biomarkers for type 2 diabetes: a DIRECT study. Diabetologia. 2018;61(1):117–29.
Stegemann C, Pechlaner R, Willeit P, Langley SR, Mangino M, Mayr U, Menni C, Moayyeri A, Santer P, Rungger G, et al. Lipidomics profiling and risk of cardiovascular disease in the prospective population-based Bruneck study. Circulation. 2014;129(18):1821–31.
Wang Z, Klipfell E, Bennett BJ, Koeth R, Levison BS, Dugar B, Feldstein AE, Britt EB, Fu X, Chung YM, et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature. 2011;472(7341):57–63.
Glomset JA. The mechanism of the plasma cholesterol esterification reaction: plasma fatty acid transferase. Biochim Biophys Acta. 1962;65:128–35.
Chen L, Liang B, Froese DE, Liu S, Wong JT, Tran K, Hatch GM, Mymin D, Kroeger EA, Man RY, et al. Oxidative modification of low density lipoprotein in normal and hyperlipidemic patients: effect of lysophosphatidylcholine composition on vascular relaxation. J Lipid Res. 1997;38(3):546–53.
Oka H, Kugiyama K, Doi H, Matsumura T, Shibata H, Miles LA, Sugiyama S, Yasue H. Lysophosphatidylcholine induces urokinase-type plasminogen activator and its receptor in human macrophages partly through redox-sensitive pathway. Arterioscler Thromb Vasc Biol. 2000;20(1):244–50.
Kim M, Jung S, Kim SY, Lee SH, Lee JH. Prehypertension-associated elevation in circulating lysophosphatidlycholines, Lp-PLA2 activity, and oxidative stress. PLoS ONE. 2014;9(5):e96735.
Li X, Fang P, Li Y, Kuo YM, Andrews AJ, Nanayakkara G, Johnson C, Fu H, Shan H, Du F, et al. Mitochondrial reactive oxygen species mediate lysophosphatidylcholine-induced endothelial cell activation. Arterioscler Thromb Vasc Biol. 2016;36(6):1090–100.
Takahashi M, Okazaki H, Ogata Y, Takeuchi K, Ikeda U, Shimada K. Lysophosphatidylcholine induces apoptosis in human endothelial cells through a p38-mitogen-activated protein kinase-dependent mechanism. Atherosclerosis. 2002;161(2):387–94.
Paapstel K, Kals J, Eha J, Tootsi K, Ottas A, Piir A, Jakobson M, Lieberg J, Zilmer M. Inverse relations of serum phosphatidylcholines and lysophosphatidylcholines with vascular damage and heart rate in patients with atherosclerosis. Nutr Metab Cardiovasc Dis. 2018;28(1):44–52.
Mannheim D, Herrmann J, Versari D, Gossl M, Meyer FB, McConnell JP, Lerman LO, Lerman A. Enhanced expression of Lp-PLA2 and lysophosphatidylcholine in symptomatic carotid atherosclerotic plaques. Stroke. 2008;39(5):1448–55.
Nakhjavani M, Asgharani F, Khalilzadeh O, Esteghamati A, Ghaneei A, Morteza A, Anvari M. Oxidized low-density lipoprotein is negatively correlated with lecithin–cholesterol acyltransferase activity in type 2 diabetes mellitus. Am J Med Sci. 2011;341(2):92–5.
Eigenbrodt ML, Bursac Z, Rose KM, Couper DJ, Tracy RE, Evans GW, Brancati FL, Mehta JL. Common carotid arterial interadventitial distance (diameter) as an indicator of the damaging effects of age and atherosclerosis, a cross-sectional study of the Atherosclerosis Risk in Community Cohort Limited Access Data (ARICLAD), 1987-89. Cardiovasc Ultrasound. 2006;4:1.
Naqvi TZ, Lee MS. Carotid intima-media thickness and plaque in cardiovascular risk assessment. JACC Cardiovasc Imaging. 2014;7(10):1025–38.
Saba L, Araki T, Kumar PK, Rajan J, Lavra F, Ikeda N, Sharma AM, Shafique S, Nicolaides A, Laird JR, et al. Carotid inter-adventitial diameter is more strongly related to plaque score than lumen diameter: an automated tool for stroke analysis. J Clin Ultrasound. 2016;44(4):210–20.
Kozakova M, Morizzo C, La Carrubba S, Fabiani I, Della Latta D, Jamagidze J, Chiappino D, Di Bello V, Palombo C. Associations between common carotid artery diameter, Framingham risk score and cardiovascular events. Nutr Metab Cardiovasc Dis. 2017;27(4):329–34.
Polak JF, Sacco RL, Post WS, Vaidya D, Arnan MK, O’Leary DH. Incident stroke is associated with common carotid artery diameter and not common carotid artery intima-media thickness. Stroke. 2014;45(5):1442–6.
Eigenbrodt ML, Sukhija R, Rose KM, Tracy RE, Couper DJ, Evans GW, Bursac Z, Mehta JL. Common carotid artery wall thickness and external diameter as predictors of prevalent and incident cardiac events in a large population study. Cardiovasc Ultrasound. 2007;5:11.
Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis GJ. Compensatory enlargement of human atherosclerotic coronary arteries. N Engl J Med. 1987;316(22):1371–5.
Polak JF, Wong Q, Johnson WC, Bluemke DA, Harrington A, O’Leary DH, Yanez ND. Associations of cardiovascular risk factors, carotid intima-media thickness and left ventricular mass with inter-adventitial diameters of the common carotid artery: the multi-ethnic study of atherosclerosis (MESA). Atherosclerosis. 2011;218(2):344–9.
Petersen AK, Krumsiek J, Wagele B, Theis FJ, Wichmann HE, Gieger C, Suhre K. On the hypothesis-free testing of metabolite ratios in genome-wide and metabolome-wide association studies. BMC Bioinform. 2012;13:120.
Zhai G, Wang-Sattler R, Hart DJ, Arden NK, Hakim AJ, Illig T, Spector TD. Serum branched-chain amino acid to histidine ratio: a novel metabolomic biomarker of knee osteoarthritis. Ann Rheum Dis. 2010;69(6):1227–31.
Illig T, Gieger C, Zhai G, Romisch-Margl W, Wang-Sattler R, Prehn C, Altmaier E, Kastenmuller G, Kato BS, Mewes HW, et al. A genome-wide perspective of genetic variation in human metabolism. Nat Genet. 2010;42(2):137–41.
Shi Y, Liu L, Yu Y, Long Y, Zheng H. Acidic amino acids: a new-type of enzyme mimics with application to biosensing and evaluating of antioxidant behaviour. Spectrochim Acta A Mol Biomol Spectrosc. 2018;201:367–75.
Aftring RP, Manos PN, Buse MG. Catabolism of branched-chain amino acids by diaphragm muscles of fasted and diabetic rats. Metabolism. 1985;34(8):702–11.
Adeva-Andany MM, Lopez-Maside L, Donapetry-Garcia C, Fernandez-Fernandez C, Sixto-Leal C. Enzymes involved in branched-chain amino acid metabolism in humans. Amino Acids. 2017;49(6):1005–28.
Katakami N, Mita T, Irie Y, Takahara M, Matsuoka TA, Gosho M, Watada H, Shimomura I, Sitagliptin Preventive study of Intima-media thickness Evaluation C. Effect of sitagliptin on tissue characteristics of the carotid wall in patients with type 2 diabetes: a post hoc sub-analysis of the sitagliptin preventive study of intima-media thickness evaluation (SPIKE). Cardiovasc Diabetol. 2018;17(1):24.
Bhanpuri NH, Hallberg SJ, Williams PT, McKenzie AL, Ballard KD, Campbell WW, McCarter JP, Phinney SD, Volek JS. Cardiovascular disease risk factor responses to a type 2 diabetes care model including nutritional ketosis induced by sustained carbohydrate restriction at 1 year: an open label, non-randomized, controlled study. Cardiovasc Diabetol. 2018;17(1):56.
Rizzo M, Rizvi AA, Patti AM, Nikolic D, Giglio RV, Castellino G, Li Volti G, Caprio M, Montalto G, Provenzano V, et al. Liraglutide improves metabolic parameters and carotid intima-media thickness in diabetic patients with the metabolic syndrome: an 18-month prospective study. Cardiovasc Diabetol. 2016;15(1):162.
Authors’ contributions
SW and JW contributed equally to this work. CH and WJ conceived of and designed the research. JW, WJ, FJ and DY contributed reagents/materials and tools. SW, JW, RZ, AZ and XZ performed the experiments and analysed the data. SW and JW drafted the manuscript. All authors contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Acknowledgements
We thank all the research subjects for their participation and acknowledge the supports of Biobank of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, the skilful work of the entire medical staff at the Shanghai Clinical Center for Diabetes, Center for Translational Medicine and Shanghai Key Laboratory of Diabetes Mellitus.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its additional files.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Ethical approval was granted by the Institutional Review Board of Shanghai Jiao Tong University Affiliated Sixth People’s Hospital according to Helsinki Declaration II. All subjects provided written informed consent to participate.
Funding
This work was financially supported by grants from the National Key Research and Development Project of China (2016YFC0903303); National Natural Science Foundation of China grants (81570713 and 91649112); Outstanding Academic Leaders of Shanghai Health System (2017BR008); the National Program for Support of Top-notch Young Professionals; and Yangtze River Scholar.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding authors
Additional file
Additional file 1: Table S1.
Correlation between clinical traits and serum Hp levels in T2DM patients. Table S2. Correlation between clinical traits and serum Hp levels in non-DM subjects. Table S3. Blood metabolites associated with serum Hp levels. Table S4. Metabolite ratios correlated with clinical traits in T2DM patients. Table S5. Metabolite ratios correlated with clinical traits in non-DM subjects. Figure S1. Serum Hp levels in non-diabetes mellitus subjects.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Wang, S., Wang, J., Zhang, R. et al. Association between serum haptoglobin and carotid arterial functions: usefulness of a targeted metabolomics approach. Cardiovasc Diabetol 18, 8 (2019). https://doi.org/10.1186/s12933-019-0808-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-019-0808-2