
Abstract
Background
A substantial degree of variability in practices exists amongst donor hospitals regarding the donor detection, determination of brain death, application of donor management techniques or achievement of donor management goals. A possible strategy to standardize the donation process and to optimize outcomes could lie in the implementation of a care pathway. The aim of the study was to identify and select a set of relevant key interventions and quality indicators in order to develop a specific care pathway for donation after brain death and to rigorously evaluate its impact.
Methods
A RAND modified three-round Delphi approach was used to build consensus within a single country about potential key interventions and quality indicators identified in existing guidelines, review articles, process flow diagrams and the results of the Organ Donation European Quality System (ODEQUS) project. Comments and additional key interventions and quality indicators, identified in the first round, were evaluated in the following rounds and a subsequent physical meeting. The study was conducted over a 4-month time period in 2016.
Results
A multidisciplinary panel of 18 Belgian experts with different relevant backgrounds completed the three Delphi rounds. Out of a total of 80 key interventions assessed throughout the Delphi process, 65 were considered to contribute to the quality of care for the management of a potential donor after brain death; 11 out of 12 quality indicators were validated for relevance and feasibility. Detection of all potential donors after brain death in the intensive care unit and documentation of cause of no donation were rated as the most important quality indicators.
Conclusions
Using a RAND modified Delphi approach, consensus was reached for a set of 65 key interventions and 11 quality indicators for the management of a potential donor after brain death. This set is considered to be applicable in quality improvement programs for the care of potential donors after brain death, while taking into account each country’s legislation and regulations regarding organ donation and transplantation.
Similar content being viewed by others


Background
Organ transplantation has proven to be lifesaving and to have improved the quality of life of numerous patients since the first successful kidney transplant in 1954. As the standard treatment for end-stage organ failure, organ transplantation is currently performed in 112 countries worldwide. In 2015, more than 143,000 patients across the 47 member states of the Council of Europe were on waiting lists for a heart, lung, kidney, liver, pancreas or intestinal transplant. Unfortunately, on average 18 of them died every day because of lack of timely organ availability [1]. The majority of transplant procedures rely on organs from donors after brain death (DBD). DBDs are more likely to donate multiple transplantable organs. The maintenance of perfusion and oxygenation in DBDs creates optimal conditions for successful organ transplantation.
In order to cope with these transplant needs, the field of organ donation and transplantation has been forced to evolve rapidly. Various health care services are required in this complex care process and therefore an effective organization and coordination of all involved health care professionals is essential. Nowadays, in many European Union member states, donor coordinators have been appointed in hospitals with an intensive care unit (ICU), where organ retrieval from deceased donors can be considered. Donor coordinators have clearly defined responsibilities in establishing, managing and reviewing the deceased donation processes in their hospital [2]. To support this, guidelines for the management of potential donors can provide donor coordinators with recommendations based on the best available evidence. However, in spite of efforts to develop standardized guidelines, there remains a large degree of variability in practices amongst hospitals regarding the determination of brain death, application of donor management techniques or achievement of donor management goals [3,4,5,6,7]. These may potentially contribute to under-recruitment of potential organ donors.
A possible strategy to standardize the donation process and to optimize outcomes could lie in the implementation of a validated care pathway. Care pathways are defined by the European Pathway Association as ‘a complex intervention for the mutual decision making and organization of care processes for a well-defined group of patients during a well-defined period’ [8]. They support the translation of clinical guidelines into local protocols and introduction into clinical practice [9]. Care pathways are used worldwide for a variety of patient groups to reduce undesired variability and standardize care based on the latest evidence [10]. They have also been developed for donation after brain death, such as the pathways of the United Network for Organ Sharing, National Institute for Health and Clinical Excellence or National Health Service Blood and Transplant [11,12,13]. However, a recent systematic review on the effects of existing care pathways for donation after brain death revealed that only one study effectively evaluated the impact of such a care pathway [14].
Typical active ingredients of a care pathway include the promotion of interdisciplinary teamwork, the integration of a set of evidence-based key interventions (KI), and the active follow-up of care processes by a set of quality indicators (QI) to verify compliance to KIs [15]. KIs are those which are required to guarantee high quality care, and hence in this setting will have a significant impact on patient, donor family, recipient or graft outcomes.
The present study therefore aims at selecting a set of KIs to be included in a care pathway for donation after brain death as well as a set of QIs that are relevant to assess the quality of care for potential DBDs and the impact of such a care pathway.
Methods
Study design
To develop a set of relevant KIs and QIs, a RAND modified Delphi technique [16] was used with a predefined number of rounds to stop the Delphi process and a threshold value for consensus [17]. After selection of an extensive set of KIs and QIs from the literature and composition of a multidisciplinary expert panel, three anonymous questionnaire rounds and one physical meeting were performed to achieve panel consensus about the relevance of the proposed KIs and relevance and feasibility of the proposed QIs. Questionnaires were conducted through LimeSurvey®, an open-source software tool to conduct online surveys [18]. E-mail reminders were sent at 2 weeks following the initial email of each round. The consensus procedure took place between March and June 2016.
Composition of expert panel
The objective was to generate a multidisciplinary Delphi panel of physicians and nurses involved in the donation process after brain death in Belgium in order to guarantee relevance for clinical practice and generalizability of results [17, 19]. The main eligibility criteria consisted of a longstanding experience in the field of organ donation, preferably for a minimum of 10 years, and a minimum of 3 organ donors throughout 2015 in the donor hospital, in which the expert was professionally active.
All Belgian donor coordinators (n = 196), the board members of the Belgian Society of Intensive Care Medicine (n = 8), and the members of the Transplant Coordinators Section (n = 28) and the Belgian Organ Procurement Committee (n = 19) of the Belgian Transplantation Society were invited to join this study by an information letter (Additional file 1) sent by e-mail by the first author (PH), describing the criteria required to be involved in this Delphi panel.
Selection of key interventions and quality indicators
The selection of KIs and QIs consisted of 8 steps: (1) Delphi questionnaire preparation with extraction of KIs and QIs, (2) first Delphi round, (3) data analysis of the first round, (4) second Delphi round, (5) data analysis of the second round, (6) third Delphi round, (7) data analysis of the third round, and (8) physical consensus meeting.
Step 1: Delphi questionnaire preparation with extraction of key interventions and quality indicators
To develop a Delphi questionnaire including all possible relevant and feasible KIs and QIs, an extensive literature review was conducted by the first author (PH). For the review of guidelines on the management of a potential DBD, the following resources were explored: (I) Websites of national European transplantation organizations or societies: Agence de la biomédecine, British Transplantation Society, Deutsche Stiftung Organtransplantation, Nederlandse Transplantatie Stichting, NHS Blood and Transplant, and Organización Nacional de Trasplantes; (II) Websites of European transplantation or intensive care medicine organizations or societies: European Directorate for the Quality of Medicines and HealthCare, European Society of Intensive Care Medicine, European Society of Organ Transplantation, Eurotransplant, and Scandiatransplant; (III) Websites of international transplantation societies: International Liver Transplantation Society, International Transplant Nurses Society, The International Society for Heart & Lung Transplantation, and The Transplantation Society; (IV) Public resources for evidence-based clinical practice guidelines: Guidelines International Network, National Guideline Clearinghouse, National Institute for Health and Clinical Excellence, and Scottish Intercollegiate Guidelines Network; (V) Process flow diagrams based on evidence-based medicine: Map of Medicine and National Institute for Health and Clinical Excellence; and (VI) Electronic databases: MEDLINE, CINAHL and EMBASE.
For the first 5 resources, the following search terms were used: ‘organ donation’ and ‘brain death’. For the electronic database MEDLINE, the Medical Subject Headings (MeSH) terms ‘brain death’, ‘donor selection’, ‘tissue and organ harvesting’, ‘tissue and organ procurement’ or ‘tissue donors’ were used in combination with ‘guideline’ or ‘practice guideline’, both as publication type. The strategy was translated for the other databases. Search limit parameters included: (I) published between 2009 and 2015, and (II) written in English, Dutch or French.
Only few of these guidelines included KIs for donor management [20,21,22]. Therefore, an additional search was performed in the electronic databases, MEDLINE, CINAHL, EMBASE and The Cochrane Library, to include recent review articles, using the search term ‘donor management’. In addition to the QIs listed in the guidelines and review articles, the QIs identified in the organ donation process of the Organ Donation European Quality System (ODEQUS) project were also analyzed. These were developed by a consortium involving associated and collaborating partners from 16 European countries [23].
A two-phase screening evaluation of publications from these resources was applied. In the first phase, publications were appraised for relevance based on appropriateness of the title and abstract. If relevance was unclear, or if the abstract was unavailable, the full text of these publications was assessed. In the second phase, the full text of the selected guidelines or process flow diagrams were reviewed. Following inclusion criteria were applied: (I) descriptions of KIs or QIs regarding an adult patient with a devastating brain injury or lesion with evolution to imminent brain death until post procurement, and (II) underpinning by in-text references of evidence to support their practice. The guidelines selected after full text review were appraised using the validated AGREE II-Global Rating Scale (AGREE II-GRS) quality assurance tool for clinical practice guidelines. This instrument consists of 4 items assessing the quality of guideline reporting. Each item is scored on a seven-point scale [24]. Guideline quality was independently rated by three reviewers (PH, KV and PF). A consensus meeting was held between these reviewers to determine the mean score of the overall guideline quality. Disagreements between reviewers during quality rating were resolved through discussion until consensus was reached. Only clinical practice guidelines with a mean score of 5–7 points on the overall guideline quality were included.
After the extensive literature review, potential KIs and QIs were selected by PH, EH and PF. These KIs and QIs were integrated in an internet-based Delphi questionnaire, consisting of three main parts: demographic questions (name and type of hospital or organization, number of intensive care beds, number of organ donors, professional group, function, years of experience in organ donation, age and gender), KIs and QIs. The demographic questions are included in the Additional file 1. The provisional Delphi questionnaire was pretested by three intensivists, who were not eligible to participate in the expert panel.
Step 2: Delphi round 1
During the first round, the participants received an e-mail with a link to the internet-based Delphi questionnaire. In addition to the demographic information, experts were asked to provide comments on the listed KIs and QIs or add new ones.
Step 3: Data analysis of Delphi round 1
Based on the comments in Delphi round 1, adjustments with regard to the description of the KIs and QIs were made and KIs or QIs were deleted. Newly identified KIs or QIs suggested by the expert panel were included in the questionnaire.
Step 4: Delphi round 2
In preparation for the second round, the participants received feedback of all the first-round panel members’ comments, deleted KIs and QIs, and the additionally proposed KIs and QIs. In the first part of the second Delphi round, experts were asked to rate on a 9-point Likert rating scale (score 1 indicating “strongly disagree”; score 9 “strongly agree”), to what extent each KI would contribute to the quality of care for the management of a potential donor (or the donor family, recipient or graft) and similarly to which extent each QI could be considered relevant and/or feasible to be implemented. The KIs & QIs of the Delphi round 2 are presented in the Additional file 1.
Step 5: Data analysis of Delphi round 2
The results of the second round were analyzed using predefined consensus criteria based on a systematic review about the use and reporting of the Delphi method for selecting health care QIs [17]. A KI was considered valid if it had a median score of 7 or more with 75% or more of the ratings in the highest tertile (Likert score: 7–9). A QI was accepted with agreement if the attribute relevance had a median score of 7 or more with 75% or more of the ratings in the highest tertile (Likert score: 7–9) and the attribute feasibility had a median score of 7 or more.
Step 6: Delphi round 3
In round 3, feedback on the quantitative panel results was provided to all members of the panel, presented by the following summary statistics: central tendencies (median, minimum, maximum, and mode), frequency of ratings in each tertile Likert category (1–3, 4–6, and 7–9), rating of contribution (ratio of “sum of ratings on the intervention given by participants” to “sum of ratings on the intervention if all respondents rated the interventions as ‘strongly agree’”), and the respondent’s own responses. Using this information, respondents were asked to re-rate the KIs and QIs in case they would like to change their previous answers.
Step 7: Data analysis of Delphi round 3
The same predefined consensus criteria as in step 5 were applied to the analysis of the results of the third Delphi round. If participants of round 2 did not respond in round 3, their answers of round 2 were considered as final.
Step 8: Physical consensus meeting
A face-to-face consensus meeting (June 2016) was organized to discuss and re-rate the KIs and QIs without consensus after the third round [17]. The nominal group technique was used as consensus method [25]. One author (DV) moderated this meeting in order to contain the influence of dominant personalities. Another author (PH) presented the available literature concerning the ‘no consensus’ KIs and QIs. Subsequently, the experts had the possibility to discuss the literature, followed by the opportunity for re-rating previous individual scores using the same Likert rating scale.
Results
Delphi panel participants’ characteristics
A total number of 20 eligible experts agreed to participate in this study. The expert panel had an average of 18-year experience in the field of organ donation (Table 1 for more detailed characteristics of the expert panel). In round 1, 18 of 20 invited experts completed the questionnaire. All 18 participants completed the three Delphi rounds. The physical meeting was attended by 9 experts.
Development of Delphi questionnaire
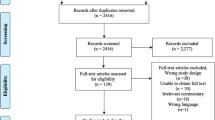
The literature research initially revealed 12 guidelines, 9 process flow diagrams, and 1719 digital records from the electronic medical databases. After screening and assessment for eligibility and quality appraisal of full-texts, 10 guidelines [20,21,22, 26,27,28,29,30,31,32] and 9 process flow diagrams [33,34,35,36,37,38,39,40,41] were included (Fig. 1). In addition, several review articles [42,43,44,45,46,47,48,49] and the results of the ODEQUS project [23] were also included.

Selection of guidelines and process flow diagrams
Based on the review of the literature, 77 potential KIs and 12 QIs were selected by PH, EH and PF. The KIs were distributed into 10 domains: (I) detection outside the ICU and communication to the ICU (n = 1); (II) detection inside the ICU and notification to a transplant center (n = 12); (III) donor evaluation and characterization (n = 15); donor management: (IV) general care (n = 7), (V) monitoring (n = 20), (VI) cardiovascular management (n = 5), (VII) respiratory management (n = 6), (VIII) renal and electrolyte management (n = 5), (IX) hormone substitution (n = 3); and (X) post procurement care (n = 3). The QIs were distributed into 3 domains: (I) structure (n = 5), (II) process (n = 5), and (III) outcome indicators (n = 2) respectively.
Results of the key interventions
Based on the comments in Delphi round 1, some adjustments with regard to the description of some of the 77 KIs were made and 2 KIs were deleted: ‘request to a transplant center to perform a liver biopsy in case of hepatic steatosis and ship it to a transplant center for evaluation by a pathologist’ (donor evaluation and characterization) and ‘central venous pressure monitoring, which is used as a dynamic measure to assess volume status or fluid responsiveness’ (donor management: monitoring). There were 5 newly identified KIs suggested by the expert panel, presented in Table 2 and Additional file 2. These additional interventions were situated within the topics: ‘donor evaluation and characterization’, ‘donor management: cardiovascular management and hormone substitution’, and ‘post procurement’.
In the second and third round, the experts could rate the now 80 KIs. The full Delphi panel of 18 experts reached consensus for 65 of the 80 KIs after the third round (data given in Table 2 with their respective Likert ratings). These interventions were considered to contribute to the quality of care for the management of a potential donor (or the donor family, recipient or graft). Because not all the experts could attend the physical meeting after round 3, the results about these 65 KIs with Likert weighted consensus were considered as the final results of this Delphi survey.
The 15 KIs without consensus after the third round are displayed in the Additional file 2. In the physical meeting, after discussion of the literature, 9 experts reached consensus about 4 out of the remaining 15 KIs without consensus after the third round: (I) Continue an appropriate prescription of deep venous thrombosis prophylaxis: low molecular weight heparin (donor management: general care); (II) Periodically re-assess cuff pressure to check if there is no cuff leak and if cuff pressure is between 20 and 30 cm H2O to avoid aspiration; (III) Ensuring coagulation screening or thromboelastography to target therapy if there is a clinically relevant bleeding; and (IV) Monitoring of glycemic status to target blood glucose ≤ 180 mg/dL (donor management: monitoring). The main reasons for not selecting certain KIs after the third round and physical meeting, as described by the experts, were low level of evidence, the prior inclusion in standard ICU care, conflicting evidence, or rather qualification as an additional intervention rather than a KI.
Results of the quality indicators
The expert panel did not suggest new QIs or adjustments to the 12 QIs in the first Delphi round. The full Delphi panel of 18 experts reached consensus for 11 of 12 QIs (4 structure, 5 process and 2 outcome indicators) after the third round. In parallel with the KIs, the results about these 11 QIs with Likert weighted consensus were considered as the final results of the Delphi survey (Table 3).
The QI without consensus after the third round is included in Additional file 2 and was not withheld in the physical meeting.
Discussion
To our knowledge, this is the first report on the selection of a set of KIs that can be used for the clinical content of a care pathway for donation after brain death. A set of 65 KIs was developed as relevant to quality of care. These interventions cover the complete organ donation pathway, including donor detection, brain death determination, family approach, donor evaluation and characterization, donor management, and the post procurement phase. Furthermore, to assess the quality of care for potential DBDs and the impact of this care pathway, a set of 11 QIs was validated for the attributes relevance and feasibility. To include recent data of studies, a continuous monitoring and updating process of this set of KIs and QIs and the resulting donor pathway is obviously needed.
While several guidelines, review articles, and process flow diagrams for the management of a potential donor have been published, there remains a lack of high quality evidence to guide clinical practice. The recommendations are largely based on physiological rationale on the one hand and, consensus statements that overwhelmingly comprised observational studies and retrospective case series on the other hand. This represents low-quality evidence, with a lack of randomized controlled trials [42, 46]. Remarkably however, only 15 of the 80 KIs after the third Delphi round were considered as not valid nor relevant by the expert panel, so consensus was reached for most interventions. This implies that the KIs selected out of the literature are reasonably well in agreement with the opinions of our expert panel, representing a “mainstream” of expert opinion.
The Delphi procedure is an accepted methodology for the selection of KIs and QIs in health care. This systematic approach is recommended in research areas hampered by limited evidence to guide clinical practice and disagreement between experts on its interpretation. This method combines evidence-based practice with expert opinion by using a multidisciplinary panel. A large group of experts across diverse locations and areas of expertise can be included anonymously, thus avoiding domination of the consensus process by one or a few experts. This group facilitation technique is designed to transform individual opinions of experts into group consensus. It includes a series of questionnaires or rounds to gather information and achieve consensus [17, 19, 25].
In this Delphi study, outcomes such as patient and graft survival, graft function, or acute rejection are not included [29]. These are valuable variables but are likely dependent on a number of factors that are not related to the donation procedure (e.g. recipient characteristics, organ procurement, and preservation), and thereby provide less information to guide quality improvements at a donor hospital. Beside QIs related to organ donation, a set of transplant QIs can also be identified. Accountability of the transplant centers on these transplant QIs, will not only stimulate the donor hospitals towards more active engagements in the field but also increase more transparency to the general public [50].
This study was restricted to the phase of KIs and QIs selection. In a next step, further research should explore which KIs (I) are effectively implemented in practice (adherence), and (II) could be improved. These interventions can then be used as a standard to evaluate the quality of existing DBD care and in quality improvement programs. Research should also determine the effect of these interventions on a set of QIs in order to substantiate progress. To this purpose, the three dimensions of structure, process and outcome indicators can be used to assess quality of care [25]. QIs rated as most important were (I) detection of all potential DBDs in the ICU and (II) documentation of cause of not proceeding to donation in potential donors. Reliability and feasibility in practice of this indicator set needs to be tested in both low- and high-volume donor hospitals. With these indicators, donor coordinators could evaluate the quality of the organ donation process at the hospital level.
Our study has several strengths. We used the systematic RAND modified Delphi method, a common and validated technique in which scientific evidence is combined with expert opinion. Our procedure is consistent with the guideline of Boulkedid et al. for using and reporting this consensus technique, in which the median number of panel members was 17 [17]. Our panel was multidisciplinary, with 18 experts covering 5 different functions: intensive care medicine, anesthesiology, intensive care nursing, donor coordination, and transplant coordination. All involved stakeholders were presented. All the experts completed the three Delphi rounds, which implies that we had a low non-response bias, increasing the validity of the results. These are highly relevant and applicable for clinical teams managing potential DBDs in different health systems, while taking into account each country’s legislation and regulations regarding organ donation and transplantation. For being universally accepted, these KIs and QIs need to be tested in an international setting.
However, this study has also some limitations. It is uncertain whether the experts who participated are a true representation of the potentially available experts with preferably a minimum of 10 years’ experience and a minimum of 3 organ donors in 2015. On average, only 32% (n = 31) of the Belgian acute care hospitals (n = 98) had more than 3 donors in 2012/2013, therefore the majority of the informed donor coordinators did not meet the criteria to participate in this study [50]. A second limitation of this study is the national setting in which these KIs and QIs were selected. However, international literature was reviewed and the QIs development of the ODEQUS project was performed by a multidisciplinary panel, in which several members have international experience and expertise on the topic. Another potential limitation is the attendance of the physical meeting by only 9 experts because of logistic reasons. However, in this meeting only the KIs and QIs without consensus after round 3 were re-rated by the experts present and the results of this meeting were not included in the final results of the Delphi survey. Finally, only literature published in English, Dutch or French was included in this study, which may include language bias for example to Spanish or German literature.
Conclusions
Using a RAND modified Delphi approach, consensus was reached for a set of 65 KIs for the management of potential DBDs. To assess quality of care for potential DBDs and the impact of this care pathway, 11 QIs were validated for the attributes relevance and feasibility. These KIs are to be considered as a first description of a standard bundle of care for potential DBDs, while the QIs identified can be incorporated into specific quality improvement programs.
Abbreviations
- AGREE:
-
Appraisal of Guidelines for Research & Evaluation
- DBD:
-
Donor after Brain Death
- ICU:
-
Intensive Care Unit
- KI:
-
Key Intervention
- MeSH:
-
Medical Subject Headings
- ODEQUS:
-
Organ Donation European Quality System
- QI:
-
Quality Indicator
References
Council of Europe. Newsletter transplant: international figures on donation and transplantation 2016. 2017 https://www.edqm.eu/. Accessed 9 Oct 2017.
European Directorate for the Quality of Medicines and Healthcare. Guide to the quality and safety of organs for Transplantation 2016. https://www.edqm.eu/en/organ-tissues-cells-transplantation-guides-1607.html. Accessed 9 Oct 2017.
Greer DM, Wang HH, Robinson JD, Varelas PN, Henderson GV, Wijdicks EF. Variability of brain death policies in the United States. JAMA Neurol. 2016;73:213–8.
Franklin GA, Santos AP, Smith JW, Galbraith S, Harbrecht BG, Garrison RN. Optimization of donor management goals yields increased organ use. Am Surg. 2010;76:587–94.
Selck FW, Deb P, Grossman EB. Deceased organ donor characteristics and clinical interventions associated with organ yield. Am J Transplant. 2008;8:965–74.
Maciel CB, Greer DM. ICU management of the potential organ donor: state of the art. Curr Neurol Neurosci Rep. 2016;16:86.
Wahlster S, Wijdicks EF, Patel PV, Greer DM, Hemphill JC 3rd, Carone M, et al. Brain death declaration: practices and perceptions worldwide. Neurology. 2015;84:1870–9.
Vanhaecht K, De Witte K, Sermeus W. The impact of clinical pathways on the organisation of care processes. Leuven: ACCO; 2007.
Campbell H, Hotchkiss R, Bradshaw N, Porteous M. Integrated care pathways. BMJ. 1998;316:133–7.
Panella M, Marchisio S, Di Stanislao F. Reducing clinical variations with clinical pathways: do pathways work? Int J Qual Health Care. 2003;15:509–21.
UNOS. Critical pathway for Organ donor. 2002. https://www.unos.org/wp-content/uploads/unos/Critical_Pathway.pdf. Accessed 9 Oct 2017.
NHS Blood and Transplant. Organ donation, Retrieval and transplantation teams. 2017. https://www.odt.nhs.uk/odt-structures-and-standards/organ-donation-retrieval-and-transplantation-teams/. Accessed 9 Oct 2017.
National Institute for Health and Clinical Excellence. Organ donation for transplantation overview. 2016. http://pathways.nice.org.uk/pathways/organ-donation-for-transplantation/organ-donation-for-transplantation-overview.pdf. Accessed 9 Oct 2017.
Hoste P, Vanhaecht K, Ferdinande P, Rogiers X, Eeckloo K, Blot S, et al. Care pathways for organ donation after brain death: guidance from available literature? J Adv Nurs. 2016;72:2369–80.
Vanhaecht K, Sermeus W, Peers J, Lodewijckx C, Deneckere S, Leigheb F, et al. The impact of care pathways for patients with proximal femur fracture: rationale and design of a cluster-randomized controlled trial. BMC Health Serv Res. 2012;12:124.
Fitch K, Bernstein SJ, Aguilar MD, Burnand B, LaCalle JR, Lázaro P, et al. The RAND/UCLA appropriateness method user's manual. Santa Monica: RAND Corporation; 2001.
Boulkedid R, Abdoul H, Loustau M, Sibony O, Alberti C. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS One. 2011;6:e20476.
Lime Survey Project Team / Carsten Schmitz. LimeSurvey: an open source survey tool / LimeSurvey project. 2015. http://www.limesurvey.org. Accessed 9 Oct 2017.
Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32:1008–15.
European Directorate for the Quality of Medicines & Healthcare. Guide to the quality and safety of organs for Transplantation 2013. https://www.edqm.eu/en/organ-tissues-cells-transplantation-guides-1607.html. Accessed 9 Oct 2017.
Eurotransplant. Eurotransplant manual: the donor. 2015. http://www.eurotransplant.org/cms/mediaobject.php?file=H9+The+Donor_June+20151.pdf. Accessed 9 Oct 2017.
Westphal GA, Caldeira Filho M, Fiorelli A, Vieira KD, Zaclikevis V, Bartz M, et al. Guidelines for maintenance of adult patients with brain death and potential for multiple organ donations. Transplant Proc. 2012;44:2260–7.
Manyalich M, Guasch X, Gomez MP, Páez G, Teixeira L. Organ donation European quality system: ODEQUS project methodology. Transplant Proc. 2013;45:3462–5.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, et al. The global rating scale complements the AGREE II in advancing the quality of practice guidelines. J Clin Epidemiol. 2012;65:526–34.
Campbell SM, Braspenning J, Hutchinson A, Marshall MN. Research methods used in developing and applying quality indicators in primary care. BMJ. 2003;326:816–9.
Karam G, Kälble T, Alcaraz A, Aki FT, Budde K, Humke U, et al. Guidelines on renal Transplantation 2014. http://uroweb.org/guideline/renal-transplantation/#. Accessed 9 Oct 2017.
National Institute for Health and Clinical Excellence. Organ donation for transplantation: improving donor identification and consent rates for deceased organ donation. 2011. http://guidance.nice.org.uk/CG135. Accessed 9 Oct 2017.
National Institute for Health and Clinical Excellence. Organ donawtion for transplantation: evidence update January 2014 http://www.nice.org.uk/guidance/cg135/evidence/cg135-organ-donation-evidence-update2. Accessed 9 Oct 2017.
European Renal Best Practice Transplantation. Guideline Development Group ERBP guideline on the management and evaluation of the kidney donor and recipient. Nephrol Dial Transplant. 2013;28(Suppl 2):ii1–71.
Kotton CN, Kumar D, Caliendo AM, Asberg A, Chou S, Danziger-Isakov L, et al. Updated international consensus guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation. 2013;96:333–60.
Seem DL, Lee I, Umscheid CA, Kuehnert MJ. PHS guideline for reducing human immunodeficiency virus, hepatitis B virus, and hepatitis C virus transmission through organ transplantation. Public Health Rep. 2013;128:247–343.
Wijdicks EFM, Varelas PN, Gronseth GS, Greer DM. Evidence-based guideline update: determining brain death in adults. Neurology. 2010;74:1911–8.
Map of Medicine Consent / authorisation for donation after brain-stem death (adult). 2010. https://nhsbtmediaservices.blob.core.windows.net/organ-donation-assets/pdfs/Consent_and_Authorisation.pdf. Accessed 9 Oct 2017.
Map of Medicine Management of brain-stem dead donor (adult). 2010. http://nhsbtmediaservices.blob.core.windows.net/organ-donation-assets/pdfs/Management_of_brain_stem_dead_donor.pdf. Accessed 9 Oct 2017.
Map of Medicine Neurological determination of death - testing (adult). 2010. https://nhsbtmediaservices.blob.core.windows.net/organ-donation-assets/pdfs/Neurological_Determination_of_Death_Testing.pdf. Accessed 9 Oct 2017.
Map of Medicine Assessment for donation after brain-stem death (adult). 2012. https://nhsbtmediaservices.blob.core.windows.net/organ-donation-assets/pdfs/Assessment_Donation_After_Brainstem_Death.pdf. Accessed 9 Oct 2017.
Map of Medicine Donor identification in emergency medicine 2012. https://nhsbtmediaservices.blob.core.windows.net/organ-donation-assets/pdfs/Donor_Identification_Emergency_Medicine.pdf. Accessed 9 Oct 2017.
Map of Medicine Neurological determination of death - assessment and planning (adult). 2010. https://nhsbtmediaservices.blob.core.windows.net/organ-donation-assets/pdfs/Neurological_Determination_of_Death_Assessment.pdf. Accessed 9 Oct 2017.
National Institute for Health and Clinical Excellence. Organ donation for transplantation: discussions with those close to the patient. 2014 http://pathways.nice.org.uk/pathways/organ-donation-for-transplantation/organ-donation-for-transplantation-discussions-with-those-close-to-the-patient.pdf. Accessed 9 Oct 2017.
National Institute for Health and Clinical Excellence. Organ donation for transplantation: early identification of potential organ donors. 2014. http://pathways.nice.org.uk/pathways/organ-donation-for-transplantation/organ-donation-for-transplantation-early-identification-of-potential-organ-donors.pdf. Accessed 9 Oct 2017.
National Institute for Health and Clinical Excellence. Organ donation for transplantation: organisation and policy. 2014. http://pathways.nice.org.uk/pathways/organ-donation-for-transplantation/organ-donation-for-transplantation-organisation-and-policy.pdf. Accessed 9 Oct 2017.
Kotloff RM, Blosser S, Fulda GJ, Malinoski D, Ahya VN, Angel L, et al. Management of the potential organ donor in the ICU: Society of Critical Care Medicine/American College of Chest Physicians/Association of Organ Procurement Organizations consensus statement. Crit Care Med. 2015;43:1291–325.
Van Raemdonck D, Neyrinck A, Verleden GM, Dupont L, Coosemans W, Decaluwe H, et al. Lung donor selection and management. Proc Am Thorac Soc. 2009;6:28–38.
McKeown DW, Ball J. Treating the donor. Curr Opin Organ Transplant. 2014;19:85–91.
Sally M, Malinoski D. Current research on organ donor management. Anesthesiol Clin. 2013;31:737–48.
Rech TH, Moraes RB, Crispim D, Czepielewski MA, Leitao CB. Management of the brain-dead organ donor: a systematic review and meta-analysis. Transplantation. 2013;95:966–74.
Dikdan GS, Mora-Esteves C, Koneru B. Review of randomized clinical trials of donor management and organ preservation in deceased donors: opportunities and issues. Transplantation. 2012;94:425–41.
Dare AJ, Bartlett AS, Fraser JF. Critical care of the potential organ donor. Curr Neurol Neurosci Rep. 2012;12:456–65.
Youn TS, Greer DM. Brain death and management of a potential organ donor in the intensive care unit. Crit Care Clin. 2014;30:813–31.
Hoste P, Ferdinande P, Hoste E, Vanhaecht K, Rogiers X, Eeckloo K, et al. Recommendations for further improvement of the deceased organ donation process in Belgium. Acta Clin Belg. 2016;71:303–12.
Acknowledgements
The intensivists within the Donation after Brain Death Study Group, responsible for the pretesting of the Delphi questionnaire, were Liesbet De Bus (Ghent University Hospital, Belgium), Dirk Rijckaert (General Hospital Sint-Lucas Ghent), and Joris Vermassen (Ghent University Hospital, Belgium).
Members of the Delphi panel within the Donation after Brain Death Study Group were Patrick Biston (CHU de Charleroi, Belgium), Charlotte Castelain (General Hospital Groeninge Kortrijk, Belgium), Els Colla (Jan Yperman Hospital, Belgium), Kirsten Colpaert (Ghent University Hospital, Belgium), Jacques Creteur (ULB Hôpital Erasme, Belgium), Johan De Blanger (Hospital Network Antwerp, Belgium), Annick De Weerdt (Antwerp University Hospital, Belgium), Bruno Desschans (University Hospitals Leuven, Belgium), Patrick Evrard (CHU Mont-Godinne, Université Catholique de Louvain, Belgium), Denis Glorieux (Grand Hopital de Charleroi, Belgium), Philippe Hantson (UCL - Saint-Luc, Belgium), Anne Joosten (CHU de Charleroi, Belgium), Josée Monard (CHU de Liège, Belgium), Baudewijn Oosterlynck (General Hospital Sint-Jan Brugge-Oostende AV, Belgium), Alain Roman (CHU Saint-Pierre, Belgium), Riet Minnekeer (Jessa Hospital Hasselt, Belgium), Gerda Van Beeumen (Antwerp University Hospital, Belgium), and Sophie Van Cromphaut (Antwerp University Hospital, Belgium).
Funding
This work was supported by a grant offered by the Belgian Federal Public Service Health, Food Chain Safety and Environment.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article and its additional files.
Author information
Authors and Affiliations
Consortia
Contributions
PH executed the research project, maintained all correspondence, collected the data, performed the analysis, participated in data interpretation, and drafted the manuscript. EH, PF, DV, AVH and the Donation after Brain Death Study Group participated in study design, data collection, data interpretation, and manuscript revision. KV, XR, KE, and KV participated in study design and manuscript revision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Informed consent and consent to participate was obtained from the expert panel prior to the start of the project. Because no patients were involved in this study, approval of an ethics committee was not required for this project.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Questionnaire. (DOC 677 kb)
Additional file 2:
Additional results of the third Delphi round and the physical meeting. (DOC 113 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hoste, P., Hoste, E., Ferdinande, P. et al. Development of key interventions and quality indicators for the management of an adult potential donor after brain death: a RAND modified Delphi approach. BMC Health Serv Res 18, 580 (2018). https://doi.org/10.1186/s12913-018-3386-1
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12913-018-3386-1