
Abstract
Background
Gene fusion events resulting from chromosomal rearrangements play an important role in initiation of lung adenocarcinoma. The recent association of four oncogenic driver genes, ALK, ROS1, RET, and NTRK1, as lung tumor predictive biomarkers has increased the need for development of up-to-date technologies for detection of these biomarkers in limited amounts of material.
Methods
We describe here a multi-institutional study using the Ion AmpliSeq™ RNA Fusion Lung Cancer Research Panel to interrogate previously characterized lung tumor samples.
Results
Reproducibility between laboratories using diluted fusion-positive cell lines was 100%. A cohort of lung clinical research samples from different origins (tissue biopsies, tissue resections, lymph nodes and pleural fluid samples) were used to evaluate the panel. We observed 97% concordance for ALK (28/30 positive; 71/70 negative samples), 95% for ROS1 (3/4 positive; 19/18 negative samples), and 93% for RET (2/1 positive; 13/14 negative samples) between the AmpliSeq assay and other methodologies.
Conclusion
This methodology enables simultaneous detection of multiple ALK, ROS1, RET, and NTRK1 gene fusion transcripts in a single panel, enhanced by an integrated analysis solution. The assay performs well on limited amounts of input RNA (10 ng) and offers an integrated single assay solution for detection of actionable fusions in lung adenocarcinoma, with potential savings in both cost and turn-around-time compared to the combination of all four assays by other methods.
Similar content being viewed by others


Background
Non-small cell lung carcinoma (NSCLC) has been categorized into several distinct entities by molecular characterization of genetic alterations occurring during epithelial cell transformation. These alterations lead mainly to the activation of oncogenes such as EGFR, KRAS, NRAS, BRAF or ERBB2, [1,2,3] which occur through point mutations, small deletions or insertions and, more rarely, amplifications. Several other key drivers have been implicated in lung cancer carcinogenesis through other mechanisms. Indeed, chromosomal rearrangements involving the tyrosine kinase receptor genes ALK, [4] ROS1, [5] RET, [6,7,8] and NTRK1, [9] have been more recently described, extending the repertoire of molecular alterations found in NSCLC. These fusion events, involving a variety of partner genes, result in the formation of chimeric fusion kinases capable of oncogenic transformation and induction of oncogene dependency within the neoplastic cells. The prevalence of each of these chromosomal rearrangements individually is 1–7% in NSCLC [4, 6, 10, 11], and altogether can be identified in approximately 5–9% of NSCLC [7, 12, 13].
The development of drugs that specifically target fusion proteins encoded by these rearrangements [9, 11, 14] has driven the need for systematic sensitive assays to detect them. Lung cancer fusions have traditionally been detected using FISH, IHC, or RT-PCR. While FISH is considered the gold standard, especially for ALK testing due to the availability of an FDA-approved ALK FISH assay, FISH analysis for multiple targets per sample can be costly. The massively parallel nature of next generation sequencing (NGS) allows a rapid characterization of point mutations, small insertions and deletions. Additionally, NGS can be used for the detection of chromosome rearrangements in a large set of genes by targeted sequencing of the fusion junctions or by paired-end mapping methods. In this study we validated a new library kit, the Ion AmpliSeq™ RNA Fusion Lung Cancer Research Panel, for characterization of the most frequent chromosome rearrangements in lung adenocarcinoma by NGS. This library kit is based on the high-multiplexing capabilities of PCR and focuses on the identification of 72 different transcripts. We report the sensitivity and specificity of this assay for the detection of gene fusions implicated in NSCLC.
Methods
Samples
A total of 138 clinical research samples previously tested for ALK, ROS1, and/or RET rearrangements were collected from 10 participating laboratories. All clinical research samples were studied in the laboratory of origin. All samples were from resections or biopsies that had been formalin-fixed and paraffin-embedded (FFPE), with the exception of three fresh frozen samples (one resection and two pleural effusions). These included 128 samples previously tested for ALK rearrangements by fluorescence in situ hybridization (FISH). Sixty-five of these samples had also been tested for ALK rearrangements by another method: immunohistochemistry (IHC), reverse transcription (RT)-PCR, and/or mass spectrometry (performed on the MassARRAY System from Agena Bioscience, San Diego, CA). Categorization of the ALK-tested samples as positive, negative or inconclusive was determined by the FISH results, as this methodology is considered the gold standard for ALK testing. For those samples previously tested by multiple methods, any discrepancies in results between the methodologies were noted. Thirteen of the ALK samples had also been tested for ROS1 and/or RET rearrangements. An additional 10 clinical research samples previously tested for ROS1 and/or RET, but for which ALK testing results were unavailable, were also included in this study. Categorization of the ROS1 and RET samples was based on the results from any available method, including FISH, IHC, RT-PCR and/or mass spectrometry, since there is not an established gold-standard for detection of these rearrangements.
RNA was extracted from each of the clinical research samples by the participating laboratories using their respective standard extraction procedures. Six of the ten laboratories used the RecoverAll Total Nucleic Acid Isolation Kit for FFPE (Thermo Fisher Scientific, Waltham, MA); remaining labs used the Qiagen RNeasy FFPE Kit (Qiagen, Hilden, Germany), the Qiagen AllPrep DNA/RNA FFPE Kit, or the Maxwell LEV RNA FFPE Purification Kit (Promega, Madison, WI). RNA was quantified using the Qubit RNA assay kits (Thermo Fisher) at eight of the laboratories; Quant-iT RiboGreen RNA Assay Kit (Thermo Fisher) and the Nanodrop 2000 instrument (Thermo Scientific) were also used for quantification.
In addition to the clinical research samples, a cocktail of RNA isolated from the ALK fusion-positive H2228 (ATCC CRL-5935), ROS1 fusion-positive HCC-78 (DSMZ ACC 563), and RET fusion-positive LC-2/ad (ECACC LC-2/ad) cell lines was prepared by Thermo Fisher Scientific and supplied to each of the participating laboratories. Select laboratories also prepared and tested RNA isolated from FFPE versions of these cell lines and RNA isolated from the ALK fusion-positive cell line H3122 (ECACC NCI-H322) and the NTRK1 fusion-positive cell line KM-12.
Ion AmpliSeq RNA fusion lung Cancer research panel design
Primers spanning 72 fusions (37 ALK, 9 RET, 15 ROS1, and 11 NTRK1) were designed by a research team at Thermo Fisher. These primers were designed to span all previously described fusions, at the time of development, for ALK, ROS1, RET, and NTRK1 in lung cancers. Sources used for the curation of known fusions included the COSMIC and NCBI databases, and review of current medical literature. Targeted fusion genes are shown in Table 1. The multiplex primer mix also included primers for the amplification of five housekeeping genes: HMBS, ITGB7, LMNA, MYC, and TBP.
Additionally, primers designed to amplify 5′ and 3′ regions of ALK, ROS1, RET, and NTRK1 were included in the primer mix. Amplification of these regions for each gene of interest allowed for the comparison of expression levels between the 3′ end of the gene, which is part of the resulting fusion, and the non-involved 5′end of the gene. A list of all targets in the multiplex PCR – including targeted fusions (genes and exons), expression control genes, and 3′and 5′regions – is available in Additional file 1: Table S1.
Detection of fusions
A minimum of 10 ng of total RNA was reverse transcribed using the SuperScript VILO cDNA Synthesis Kit followed by library generation using the Ion AmpliSeq Library Kit 2.0 and the Ion AmpliSeq RNA Fusion Lung Cancer Research Panel (hereafter, AmpliSeq Fusion Lung Panel). Barcodes were utilized during library generation using the Ion Xpress Barcode Adapters. Libraries were quantified using the Qubit DNA assay, the 2100 BioAnalyzer (Agilent Technologies, Santa Clara, CA) or the Ion Library Quantitation Kit, then pooled in equimolar concentrations for sequencing. Eight to sixteen libraries were multiplexed and templated using the Ion OneTouch2 System with the Ion PGM Template OT2 200 Kit. Libraries were sequenced using the Ion PGM Sequencing 200 v2 kit on an Ion 316 v2 or 318 v2 chip on the Ion PGM instrument. (All reagents and instrumentation above are from Thermo Fisher Scientific, with the exception of the BioAnalyzer.) Typically, eight samples were sequenced per 316 chip and sixteen samples per 318 chip.
After sequencing, unaligned BAM files were transferred to the Ion Reporter Software 4.2 and analyzed using the AmpliSeq Lung Fusion single sample workflow. This workflow utilizes a BED file comprised of chimeric sequences for targeted fusion transcripts along with sequences for the expression control genes and the 3′and 5′regions of ALK, ROS1, RET, and NTRK1. The alignment consists of three main steps. In the first step, the aligner requires that the reads align end to end (i.e, reads that are trimmed, or soft clipped, at the ends are not allowed). Each read is then aligned to the best primary alignment and filtering criteria are applied. Alignments to the fusion targets are counted only if the read overlaps at least 70% of the expected fusion insert with high local alignment score. Alignments to the imbalance and control targets are counted if the read overlaps at least 50%. In the second step, all unaligned reads, and reads that aligned but were filtered out, are split into two fragments. These fragmented reads are then re-aligned to the same reference file. Trimming of the reads is allowed in this step and all the alignments of every read (not just the primary alignments) are kept in the alignments files. This step helps recover more counts for the targets in the reference file and also finds any non-targeted fusion isoforms that are not present in the original list of targets. A novel fusion isoform involving existing primers is reported in the output if there is evidence from at least 100 different pairs of fragments. Lastly, counts from steps one and two are aggregated and all the fusion targets that have counts higher than the threshold are reported as “fusion present.” The algorithm generates a 3′/5′expression imbalance metric for each of the driver genes based on the individual counts of the 5′assay and 3′assay. It is calculated by subtracting the count of 5′reads from the count of 3′reads, and dividing the result by the sum of counts of all control targets. This metric can be used to confirm the detection of a known fusion or to predict a fusion in the sample that is not covered by the isoforms in the panel.
Results
Cell lines
Using the cocktail of RNA from the ALK, ROS1, and RET fusion-positive cell lines, each of the ten participating laboratories successfully detected all three rearrangements using the AmpliSeq Fusion Lung Panel assay (see Table 2). The fusions detected corresponded to the rearrangements previously described for these cell lines [11, 15,16,17,18] (see Table 3). The expected rearrangements were also detected from RNA isolated from the FFPE cell blocks of the same cell lines and from the ALK-positive H3122 cell line [11] (Tables 2 and 3). In the KM12 cell line [19], primers for the specific NTRK fusion were not included in the assay design, but the rearrangement was detected by a positive 3′/5′imbalance result of 0.076, above the cut-off of 0.025 (Table 2).
ALK clinical samples
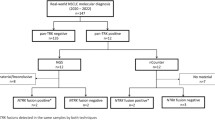
Of the 138 clinical research samples tested, 117 (84.5%) passed the QC requirement of a minimum of 20,000 total reads. One hundred of these samples had previously been tested for ALK rearrangements by FISH with conclusive results; AmpliSeq Fusion Lung Panel results were 97% concordant (97/100 samples) with FISH analysis (see Table 4). ALK rearrangements were detected in 28/30 ALK FISH-positive samples, with a sensitivity of 93.3%; exact fusions were identified in 24 of the samples and an additional 4 samples showed evidence of rearrangement using the 3′/5′imbalance calculation. In samples negative for ALK rearrangements by FISH, 69 of 70 samples were also negative by the AmpliSeq assay, thus resulting in a specificity of 98.6%. Details on all ALK clinical research samples are shown in Additional file 1: Table S2.
Closer analysis of the discordant results (see Table 5), revealed that two of the FISH-positive ALK samples without a detected fusion showed 10% rearranged cells (below the usual cut-off of 15%). One of these samples showed only weak staining by IHC, and subsequent re-testing by the AmpliSeq Fusion Lung Panel gave a positive result of a fusion of HIP1-ALK with 30 reads. Five of the remaining seven discordant ALK FISH-positive samples showed an atypical FISH result of one red signal, rather than the split red-green signal; of these, two were IHC negative for ALK and one was positive by IHC originally, but negative upon repeat testing. The remaining two FISH-positive, AmpliSeq fusion-negative samples showed typical FISH results with 19% and 20% rearranged cells, respectively, and both were positive for ALK IHC staining.
One discordant sample was negative by FISH and positive by AmpliSeq. This sample showed an EML4- ALK fusion with 6137 fusion reads, and the 3′/5′imbalance in this sample also showed a positive result. Additionally, this sample had previously tested positive for ALK protein expression by IHC.
ROS1 and RET clinical samples
Panel results for ROS1 and RET were concordant in 21/22 samples (95.5%) for ROS1 and 14/15 (93.3%) for RET as compared to previous testing using available methods, including FISH, IHC, RT-PCR, and mass spectrometry. The AmpliSeq assay detected the appropriate fusions in 3/4 ROS1-positive samples and in 1/1 RET-positive sample. Samples previously determined to be negative for ROS1 using other methodologies (18 samples) were all negative using the AmpliSeq Fusion Lung Panel. In samples previously determined to be negative for RET fusions, 13 of 14 were negative by the AmpliSeq panel, and one showed a positive imbalance result of 0.197, in the absence of a detected fusion isoform (Additional file 1: Table S3). This sample was subsequently tested using the RET FISH break-apart probe and also re-run using the AmpliSeq panel; both results were negative.
Detection and confirmation of additional fusions
Testing of the clinical research samples yielded the detection of ROS1 fusions in two samples which were ALK-negative by FISH (Samples 63 and 67, Additional file 1: Table S2). In both cases, the CD74-ROS1 fusion was detected and subsequent testing using a TaqMan assay with primers specific for the detected fusion confirmed the results. Prior to this study, neither of these samples had been tested for ROS1 rearrangements.
RET fusions were detected in three of the ALK-negative samples (Samples 48, 55, and 98, Additional file 1: Table S2). In Sample 98, the KIF5B-RET fusion was detected and subsequently confirmed by a TaqMan assay. Samples 48 and 55 showed positive RET 3′/5′imbalance results of 0.041 and 0.271, respectively. Subsequent FISH analysis of Sample 55 showed 10% split signals in the tissue area used for extraction of RNA for the AmpliSeq Fusion Lung Panel assay. Additional material for confirmatory testing was not available for Sample 48.
Lastly, a ROS1 fusion was detected with 83 fusion reads in one of the ALK FISH-positive samples (Sample 8, Additional file 1: Table S2). The presence of two fusion events is unlikely, and subsequent testing by RT-PCR did not confirm the presence of this fusion.
Samples with low Total reads
Upon initial evaluation of the 138 clinical research samples, samples below the QC cut-off of 20,000 were repeated with either 30 PCR cycles or simply re-pooling prior to bead templating. Five of ten samples successfully repeated, and those samples are included in the data above. In the other five samples and in samples for which repeat testing was not possible, reasons for failure included insufficient RNA quantity (< 10 ng), degraded RNA, and improper pooling of libraries.
Discussion
The advent of therapies targeting the fusion proteins arising from ALK, ROS1, and RET gene fusions makes the routine detection of these events important in patients with lung adenocarcinoma. We have described here an international, multi-institutional study using a multiplex RT-PCR next generation sequencing-based method that enables simultaneous detection of ALK, RET, ROS1, and NTRK1 gene fusion transcripts in a single assay. The simultaneous detection of these fusions has important implications for turn-around-time and cost. Further, it can be performed with very little input RNA. This is particularly attractive for an assay targeted at lung cancers, as these samples are often biopsies with limited available tissue. Lung cancer fusions have traditionally been detected using FISH, IHC, or RT-PCR. While FISH is considered the gold standard, especially for ALK testing due to the availability of an FDA-approved ALK FISH assay, FISH analysis for multiple targets per sample can be costly. Often these analyses are done in step-wise fashion, which can reduce the overall cost of performing multiple FISH assays, but potentially extend the time needed to rule out all relevant gene rearrangements. Immunohistochemistry staining offers a cheaper alternative; however, this methodology is subjective, sometimes making interpretation difficult. [20] RT-PCR, on the other hand, can offer precise detection of fusions, including identification of both partner genes and the exons involved. The main limitation of traditional RT-PCR is that it typically focuses on only the most common fusion events and is thus limited in detecting rare exon combinations. [21]
In contrast to FISH or IHC, the detection of ALK, ROS1, RET, and NTRK1 fusions are combined in a single assay with the AmpliSeq design. From the 70 clinical research samples that previously had been determined to be ALK-negative by FISH, we detected two ROS1 fusions and three RET fusions. Both of the ROS1 fusions and two of RET fusions were confirmed to be positive by orthogonal methods; tissue for additional testing was not available for the third RET-positive sample. Further, the detection of fusions by NGS offers a timely methodology that can also be designed to accommodate the simultaneous detection of point mutations and insertions and deletions in the DNA of relevant genes in a single assay. Analysis of these types of mutations, particularly in EGFR and KRAS, is typically part of the work-up of lung adenocarcinoma patients. Methods to detect both DNA mutations and fusion events in a timely manner are particularly important in these patients due to the aggressive nature of the disease. While combined analysis of DNA and RNA was not the focus of this study, it is currently being performed by many of the institutions that participated in this study.
The methodology described in this paper relies on RT-PCR for the initial amplification of fusion events; however, the design of this assay circumvents a limitation of traditional RT-PCR. The AmpliSeq Fusion Lung Panel assay includes multiplexing of primers for 72 different fusion combinations and thus is not limited to only the most common fusions. A second limitation of traditional RT-PCR is that one must have previous knowledge of all possible relevant fusions. The AmpliSeq assay addresses this issue in two ways. First, during the analysis of the sequenced reads, all reads that are initially unaligned to the reference sequence are split in half and allowed to re-align. This step fosters the detection of novel fusions involving existing primers. Secondly, the assay includes a method for detection fusions involving unknown partners using the 3′/5′imbalance calculation. This step analyzes the expression levels of the 3′ and 5′ends of each driver gene. For genes involved in a fusion event, the 3′ end of the gene is now under different regulatory control and shows overexpression relative to the 5′end of the gene. Another recently described methodology using NanoString technology also exploits this phenomenon of 3′overexpression. [22] That study found that evaluation of the imbalance between 3′and 5′expression works relatively well for ALK and RET, which are normally not expressed in lung tissue, but that this calculation was more difficult for ROS1 as this gene is normally expressed at high levels. Given that a positive imbalance result is suggestive of a fusion event, but alone does not identify an exact fusion, our suggestion for the AmpliSeq assay is to use the imbalance calculation as a method for identifying possible fusions that should be followed up with orthogonal testing methods if desired.
Further analysis of discordant samples within our study found that some samples had either low levels of rearranged cells by FISH or discordant results between FISH and IHC. One of the samples for which FISH testing showed 10% rearranged cells, was positive for a HIP1-ALK fusion upon repeat testing with the AmpliSeq assay. The repeat result had fusion reads falling just above the cut-off, while the initial negative result did identify the same fusion but with a number of reads falling below the cut-off, indicating the sample was likely approaching the limit of detection for the assay. Discordance between ALK FISH and other methods has been noted previously [23,24,25] and brings up the question of a true “gold standard.” Three of the ALK FISH-positive samples for which the AmpliSeq assay was negative, were also negative by IHC. Additionally, we found that five of the discordant samples displayed single red signals by FISH. This phenomenon of a single red signal represents a likely deletion of the 5′end of ALK and is not unusual for this structural variant; however, previous studies have also shown a similar discordance between ALK FISH-positive results displaying a deletion of the 5′ALK probe and IHC [24] or PCR. [26] The exact nature of these fusion events may be of interest for future studies. We also observed discordant results for one of the ALK FISH-negative samples. In this case, the AmpliSeq assay identified an EML4-ALK fusion with a high number of reads and the sample was also positive by IHC. While this sample was officially classified as an AmpliSeq “false positive,” it likely represents a true positive in which FISH testing failed to detect the fusion.
A recent study using the AmpliSeq method for fusion detection reported 100% concordance between this and other methodologies. [27] It is unknown, but probable, that the testing for this study was performed at a single institution. The difference between a single or limited institution study and a larger study (in this case, ten institutions) may explain the difference in concordance results between the Pfarr study [27] and the study described here. The international, multi-institutional nature of this study presented many challenges. Scoring criteria between laboratories often varies even for well-established reference methods, e.g., some samples in this study were deemed FISH-positive, yet fell below the cut-off of 15% used by other institutions. A lack of concordance between multiple institutions for detection of ALK rearrangements has been previously observed, [20, 28] and this phenomenon may have contributed to the lower concordance of compared methods in this study. A further challenge of the multi-institutional study included a lack of material for follow up on discrepant samples, as the samples were not only from the participating institutions but in some cases were from additional laboratory partners. However, we believe that the advantages of this multi-institutional study far outweigh the disadvantages. Reproducibility across different laboratories using cell line mixtures was 100%, despite potential differences in laboratory practices and personnel. Additionally, an international, multi-institutional study such as this allows for the inclusion of more varied samples and more fully explores the performance of the assay.
Conclusion
The RT-PCR NGS assay described here offers many advantages for laboratory testing in lung adenocarcinoma samples. This methodology allows detection of multiple fusions in a single assay and can easily also be multiplexed with detection of point mutations and small insertions and deletions in genes such as KRAS and EGFR that are also important in the work up of these patients. The single-assay format potentially allows for faster turn-around-time and lower cost than doing the assays separately. Further, the small amount of input RNA required is very advantageous for these samples. However, the AmpliSeq assay primarily targets known fusions. Inclusion of the 3′/5′imbalance calculation aims to address this limitation, but could likely benefit from further refinement of cut-offs values as more data is generated by this assay. Lastly, efforts to periodically update the primer pool as additional partner genes for ALK, ROS1, RET, and NTRK1 fusions are identified would aid in the continuing utility of this assay.
Abbreviations
- FFPE:
-
Formalin-fixed paraffin-embedded
- FISH:
-
Fluorescence in situ hybridization
- IHC:
-
Immunohistochemistry
- NGS:
-
Next generation sequencing
- NSCLC:
-
Non-small cell lung cancer
- RT-PCR:
-
Reverse transcriptase-polymerase chain reaction
References
Cancer Genome Atlas Research N. Comprehensive molecular profiling of lung adenocarcinoma. Nature. 2014;511(7511):543–50.
Ding L, Getz G, Wheeler DA, Mardis ER, McLellan MD, Cibulskis K, Sougnez C, Greulich H, Muzny DM, Morgan MB, et al. Somatic mutations affect key pathways in lung adenocarcinoma. Nature. 2008;455(7216):1069–75.
Sholl LM, Aisner DL, Varella-Garcia M, Berry LD, Dias-Santagata D, Wistuba II, Chen H, Fujimoto J, Kugler K, Franklin WA, et al. Multi-institutional oncogenic driver mutation analysis in lung adenocarcinoma: the lung Cancer mutation consortium experience. J Thorac Oncol. 2015;10(5):768–77.
Soda M, Choi YL, Enomoto M, Takada S, Yamashita Y, Ishikawa S, Fujiwara S, Watanabe H, Kurashina K, Hatanaka H, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007;448(7153):561–6.
Rikova K, Guo A, Zeng Q, Possemato A, Yu J, Haack H, Nardone J, Lee K, Reeves C, Li Y, et al. Global survey of phosphotyrosine signaling identifies oncogenic kinases in lung cancer. Cell. 2007;131(6):1190–203.
Kohno T, Ichikawa H, Totoki Y, Yasuda K, Hiramoto M, Nammo T, Sakamoto H, Tsuta K, Furuta K, Shimada Y, et al. KIF5B-RET fusions in lung adenocarcinoma. Nat Med. 2012;18(3):375–7.
Takeuchi K, Soda M, Togashi Y, Suzuki R, Sakata S, Hatano S, Asaka R, Hamanaka W, Ninomiya H, Uehara H, et al. RET, ROS1 and ALK fusions in lung cancer. Nat Med. 2012;18(3):378–81.
Li F, Feng Y, Fang R, Fang Z, Xia J, Han X, Liu XY, Chen H, Liu H, Ji H. Identification of RET gene fusion by exon array analyses in “pan-negative” lung cancer from never smokers. Cell Res. 2012;22(5):928–31.
Vaishnavi A, Capelletti M, Le AT, Kako S, Butaney M, Ercan D, Mahale S, Davies KD, Aisner DL, Pilling AB, et al. Oncogenic and drug-sensitive NTRK1 rearrangements in lung cancer. Nat Med. 2013;19(11):1469–72.
Uguen A, De Braekeleer M. ROS1 fusions in cancer: a review. Future Oncol. 2016;12(16):1911–28.
Koivunen JP, Mermel C, Zejnullahu K, Murphy C, Lifshits E, Holmes AJ, Choi HG, Kim J, Chiang D, Thomas R, et al. EML4-ALK fusion gene and efficacy of an ALK kinase inhibitor in lung cancer. Clin Cancer Res. 2008;14(13):4275–83.
Scarpino S, Rampioni Vinciguerra GL, Di Napoli A, Fochetti F, Uccini S, Iacono D, Marchetti P, Ruco L. High prevalence of ALK+/ROS1+ cases in pulmonary adenocarcinoma of adoloscents and young adults. Lung Cancer. 2016;97:95–8.
Pan Y, Zhang Y, Li Y, Hu H, Wang L, Li H, Wang R, Ye T, Luo X, Zhang Y, et al. ALK, ROS1 and RET fusions in 1139 lung adenocarcinomas: a comprehensive study of common and fusion pattern-specific clinicopathologic, histologic and cytologic features. Lung Cancer. 2014;84(2):121–6.
Gainor JF, Shaw AT. Novel targets in non-small cell lung cancer: ROS1 and RET fusions. Oncologist. 2013;18(7):865–75.
Phelps RM, Johnson BE, Ihde DC, Gazdar AF, Carbone DP, McClintock PR, Linnoila RI, Matthews MJ, Bunn PA Jr, Carney D, et al. NCI-navy medical oncology branch cell line data base. J Cell Biochem Suppl. 1996;24:32–91.
Virmani AK, Fong KM, Kodagoda D, McIntire D, Hung J, Tonk V, Minna JD, Gazdar AF. Allelotyping demonstrates common and distinct patterns of chromosomal loss in human lung cancer types. Genes chromosomes cancer. 1998;21(4):308–19.
Matsubara D, Kanai Y, Ishikawa S, Ohara S, Yoshimoto T, Sakatani T, Oguni S, Tamura T, Kataoka H, Endo S, et al. Identification of CCDC6-RET fusion in the human lung adenocarcinoma cell line, LC-2/ad. J Thorac Oncol. 2012;7(12):1872–6.
Davies KD, Le AT, Theodoro MF, Skokan MC, Aisner DL, Berge EM, Terracciano LM, Cappuzzo F, Incarbone M, Roncalli M, et al. Identifying and targeting ROS1 gene fusions in non-small cell lung cancer. Clin Cancer Res. 2012;18(17):4570–9.
Ardini E, Bosotti R, Borgia AL, De Ponti C, Somaschini A, Cammarota R, Amboldi N, Raddrizzani L, Milani A, Magnaghi P, et al. The TPM3-NTRK1 rearrangement is a recurring event in colorectal carcinoma and is associated with tumor sensitivity to TRKA kinase inhibition. Mol Oncol. 2014;8(8):1495–507.
Tembuyser L, Tack V, Zwaenepoel K, Pauwels P, Miller K, Bubendorf L, Kerr K, Schuuring E, Thunnissen E, Dequeker EM. The relevance of external quality assessment for molecular testing for ALK positive non-small cell lung cancer: results from two pilot rounds show room for optimization. PLoS One. 2014;9(11):e112159.
Wallander ML, Geiersbach KB, Tripp SR, Layfield LJ. Comparison of reverse transcription-polymerase chain reaction, immunohistochemistry, and fluorescence in situ hybridization methodologies for detection of echinoderm microtubule-associated proteinlike 4-anaplastic lymphoma kinase fusion-positive non-small cell lung carcinoma: implications for optimal clinical testing. Arch Pathol Lab Med. 2012;136(7):796–803.
Lira ME, Choi YL, Lim SM, Deng S, Huang D, Ozeck M, Han J, Jeong JY, Shim HS, Cho BC, et al. A single-tube multiplexed assay for detecting ALK, ROS1, and RET fusions in lung cancer. J Mol Diagn. 2014;16(2):229–43.
To KF, Tong JH, Yeung KS, Lung RW, Law PP, Chau SL, Kang W, Tong CY, Chow C, Chan AW, et al. Detection of ALK rearrangement by immunohistochemistry in lung adenocarcinoma and the identification of a novel EML4-ALK variant. J Thorac Oncol. 2013;8(7):883–91.
Gao X, Sholl LM, Nishino M, Heng JC, Janne PA, Oxnard GR. Clinical implications of variant ALK FISH rearrangement patterns. J Thorac Oncol. 2015;10(11):1648–52.
Ali SM, Hensing T, Schrock AB, Allen J, Sanford E, Gowen K, Kulkarni A, He J, Suh JH, Lipson D, et al. Comprehensive genomic profiling identifies a subset of Crizotinib-responsive ALK-rearranged non-small cell lung Cancer not detected by fluorescence in situ hybridization. Oncologist. 2016;21(6):762–70.
Dai Z, Kelly JC, Meloni-Ehrig A, Slovak ML, Boles D, Christacos NC, Bryke CR, Schonberg SA, Otani-Rosa J, Pan Q, et al. Incidence and patterns of ALK FISH abnormalities seen in a large unselected series of lung carcinomas. Mol Cytogenet. 2012;5(1):44.
Pfarr N, Stenzinger A, Penzel R, Warth A, Dienemann H, Schirmacher P, Weichert W, Endris V. High-throughput diagnostic profiling of clinically actionable gene fusions in lung cancer. Genes chromosomes cancer. 2016;55(1):30–44.
Marchetti A, Barberis M, Papotti M, Rossi G, Franco R, Malatesta S, Buttitta F, Ardizzoni A, Crino L, Gridelli C, et al. ALK rearrangement testing by FISH analysis in non-small-cell lung cancer patients: results of the first italian external quality assurance scheme. J Thorac Oncol. 2014;9(10):1470–6.
Acknowledgements
The authors wish to thank Xiao Zhang (Queen’s University, Kingston Ontario, Canada), Miguel Silva (Ipatimup, Porto, Portugal) and Ana Justino (Ipatimup, Porto, Portugal).
Funding
This work resulted from projects “Institute for Research and Innovation in Health Sciences” (POCI-01-0145-FEDER-007274), “GenomePT” (POCI-01-0145-FEDER-022184), “Advancing cancer research: from knowledge to application” (NORTE-01-0145-FEDER-000029) supported by COMPETE 2020 - Operational Programme for Competitiveness and Internationalisation (POCI), Norte Portugal Regional Programme (NORTE 2020), Lisboa Portugal Regional Operational Programme (Lisboa2020), Algarve Portugal Regional Operational Programme (CRESC Algarve2020), under the PORTUGAL 2020 Partnership Agreement, through the European Regional Development Fund (ERDF), and by FCT - Fundação para a Ciência e a Tecnologia (PTDC/DTP-PIC/2500/2014). This work was supported by a grant from the Associazione Italiana per la Ricerca sul Cancro (AIRC) to N. Normanno (Grant number: IG17135).
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on a reasonable request.
Author information
Authors and Affiliations
Contributions
Study concept and design: IC, PLP, NN, OS, RP, KB, JC, CV, AM. Data acquisition, analysis and interpretation: IC, AR, PLP, VB, RB, BT, NN, MJ, FM, HF, OS, KB, AS, JC, CV, MB, KN, KS, AM, AR, SC, DC, HK. Drafting of the manuscript or revising it critically for important intellectual content: IC, PLP, VB, NN, MJ, HF, AB, OS, AS, JC, CV, JM, AM, SC. All authors have given final approval of the version to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Samples were retrieved from the archives of the collaborating institutions and de-identified. For the following institutions, the study was interpreted as a service improvement not requiring specific research ethics committee approval as stated in the EU Clinical Trials Directive (2001/20/EC): Radboud university medical center, VIOLLIER (assay performed by Viollier, samples mainly from University Hospital Basel and Luzerner Kantonsspital, Switzerland), Applied Research on Cancer Centre (ARC-NET), University Hospitals Coventry and Warwickshire (UHCW), Institut National de la Sante et de la Recherche Medicale (INSERM), and Centro di Ricerche Oncologiche di Mercogliano (CROM). Samples from the following institutions were used under approved Institutional Review Board protocols: ARUP Laboratories (ARUP Laboratories Ethics Committee approval 24,487), Queen’s University (Health Sciences and Affiliated Teaching Hospitals Research Ethics Board approval 6,010,968), and Kinki University (Institutional Review Board of Kindai University Faculty of Medicine approval 22–106). Samples from Ipatimup were used in accordance with Article 19 (“DNA Banks and Other Biological Products”) of Portuguese Law No. 12/2005 of 26 January (“Personal genetic information and health information”).
Competing interests
Thermo Fisher Scientific provided reagents for this study to participating laboratories at a discount. Travel funds were partially reimbursed for consortium members to attend a group meeting. Authors R.P., V.B., and K.B. are employed by Thermo Fisher Scientific. NN is a member of the editorial board (Associate Editor) of this journal.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. RT-PCR Targets within the Ion AmpliSeq™ Lung Fusion Research Panel. A list of all targets in the multiplex PCR studied – including targeted fusions (genes and exons), expression control genes, and 3′and 5′regions. Table S2. ALK Clinical Samples. Table depicting details on all ALK clinical research samples analyzed in the study. Table S3. ROS1 and RET clinical samples. Table depicting details on all ROS1 and RET clinical research samples analyzed in the study. (DOCX 57 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Vaughn, C.P., Costa, J.L., Feilotter, H.E. et al. Simultaneous detection of lung fusions using a multiplex RT-PCR next generation sequencing-based approach: a multi-institutional research study. BMC Cancer 18, 828 (2018). https://doi.org/10.1186/s12885-018-4736-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12885-018-4736-4