
Abstract
Background
The serum immunoglobulin A (IgA)/C3 ratio is considered to be an effective predictor of IgA nephropathy (IgAN). This study sought to explore the diagnostic value of the IgA/C3 ratio in IgAN among primary glomerular nephropathy patients in China.
Methods
We recruited 1095 biopsy-diagnosed primary glomerular nephropathy patients, including 757 IgAN patients and 338 non-IgAN patients. Patient demographics, serum immunological indices, and other clinical examinations were measured. IgAN cases were propensity score matched (PSM) to non-IgAN cases on the logit of the propensity score using nearest neighbor matching in a 1:1 fashion, with a caliper of 0.02 with no replacements, according to age, gender, BMI, proteinuria level, and estimated glomerular filtration rate (eGFR).
Results
We found that in both the full cohort and PSM cohort, the IgA/C3 ratio in the IgAN group was significantly higher than that of the non-IgAN group. The same results were also obtained with stratification by different levels of proteinuria and renal function. In the PSM cohort, there was no difference in IgA/C3 ratio in patients with IgAN between different proteinuria groups and different chronic kidney disease (CKD) groups. The area under the ROC curve (AUROC) of the IgA/C3 ratio in distinguishing IgAN among primary glomerular disease was 0.767 in the full cohort, and 0.734 in the PSM cohort. The highest AUROC of the IgA/C3 ratio was in the ≤1 g/d proteinuria group (0.801 in the full cohort, and 0.803 in the PSM cohort); however, there was no difference between all CKD groups. Meanwhile, the diagnostic accordance rate for the diagnosis of IgAN among all patients with an IgA/C3 ratio > 3.5304 was as high as 92.02% in the full cohort. IgAN was independently correlated with IgA/C3 ratio in the full cohort by multivariate logistic regression analysis.
Conclusions
The present study provides clear evidence that the IgA/C3 ratio is an effective predictor of IgA diagnosis, especially in patients with proteinuria ≤1 g/d. In order to study the effectiveness of this biomarker, and to determine a standardized cut-off value, additional multicenter large-scale studies are needed.
Similar content being viewed by others


Background
Immunoglobulin A nephropathy (IgAN), which was initially described by Berger and Hinglais in 1968 [1], is the most common type of primary glomerulonephritis worldwide [2,3,4], especially in the Asia-Pacific region [2, 5, 6]. IgAN accounts for more than 20% of glomerular diseases [5, 6]. An epidemiological survey showed that approximately 45% of the cases of primary glomerulonephritis in China were IgAN [6]. IgAN is diagnosed by renal biopsy with immunofluorescence staining or immunohistochemistry, and is histologically characterized by the presence of polymeric IgA deposits in glomerular mesangial areas [1, 7]. The clinical presentation of IgAN is highly variable between individuals, and ranges from a subclinical disease with isolated microscopic hematuria to severe end-stage renal disease (ESRD). The stereotypical IgAN patient is a young adult with asymptomatic microscopic hematuria or episodic macroscopic hematuria occurring during an upper respiratory tract infection. IgAN was previously considered to be a benign condition, but recent studies have demonstrated that up to 25–40% of patients progress to uremia within 10–20 years after the diagnostic biopsy [6, 8,9,10].
Until present, the diagnosis of IgAN relies on revealing IgA as the dominant or codominant immunoglobulin in the glomerular mesangium by kidney biopsy [1]. However, the pathogenesis of IgAN remains unclear. According to recent studies, IgAN is thought to be autoimmune in nature. Suzuki et al. put forward a four-hit hypothesis, in which the galactose-deficient IgA1 (GdIgA1) molecule plays a key pathogenic role [11, 12]. Although renal biopsy remains the gold standard for IgAN diagnosis, recent efforts have sought to find new biomarkers that can predict IgAN without the need for biopsy [13,14,15]. Previous studies have shown that IgA deposition in the mesangial area is necessary for IgAN progression and accompanying C3 deposition. However, the correlation between the changes in serum complement levels and diagnosis remains unclear [12, 16]. Some researchers have reported that IgAN patients usually have higher serum IgA and GdIgA1 levels [17, 18], alongside normal-to-low serum C3 levels, compared to those of patients with other types of primary glomerulonephritis [19, 20]. In 2000, Yasuhiko T et al. reported that patients with higher serum IgA/C3 ratios were more likely to be diagnosed with IgAN [13]. Since then, several studies have sought to evaluate whether the IgA/C3 ratio can serve as a useful clinical indicator to predict the diagnosis and prognosis of IgAN [13,14,15, 20,21,22]. However, most of these studies focused on a Japanese patient population and had small sample sizes. Thus, these findings require replication in other patient populations and larger sample sizes to confirm the validity of the association, and to account for potential ethnic differences. Moreover, previous studies have not reported whether the IgA/C3 ratio is of similar value when diagnosing IgAN by proteinuria levels or renal function.
In non-randomized studies, good study methodology not only effectively evaluates the clinical program, but also minimizes confounding variables. In statistical analyses, propensity score matching (PSM) between treatment groups is a practical method to reduce confounding bias, particularly in evaluating comparative effectiveness of two or more variables [23, 24]. Unlike stratification or regression, the new PSM cohort is in equilibrium with the measured covariates during the PSM process, and is also in “clinical equipoise”. In other words, in this selected cohort, every patient should be a reasonable candidate for every treatment being studied [24,25,26]. Increasing attention is being paid to the use of PSM as a statistical method in clinical studies.
The purpose of this study was to evaluate whether a high serum IgA/C3 ratio, the suggested novel biomarker, could be used as a diagnostic criterion for IgAN in a large Chinese patient population, using PSM methods.
Methods
Study population
Between January 2001 and December 2017, 813 IgAN patients, confirmed by renal biopsy at the third affiliated hospital of Sun Yat-Sen University, were recruited as the cohort for this cross-sectional study. Additionally, 264 patients with other forms of primary glomerular nephropathy (non-IgAN group) were recruited between January 2012 and December 2017. Also included were 137 IgAN patients and 146 non-IgAN patients from the First Affiliated Hospital of Jinan University between January 2012 and December 2017. All renal biopsy diagnoses were performed by professional pathologists. The exclusion criteria were as follows: 1) undergoing treatment with corticosteroids, immunosuppressants, or bacteriotoxic drugs; 2) secondary causes of renal diseases such as systemic lupus erythematosus (SLE), Henoch–Schonlein purpura, malignant tumors, hepatic diseases, lymphoma, or other systemic diseases; 3) acute interstitial nephritis; 4) acute changes in the estimated glomerular filtration rate (eGFR) > 30% in the previous 3 months; 5) patients aged < 18 years; 6) pregnancy; 7) acquired immunodeficiency syndrome or other autoimmune diseases; 8) inability to communicate and comply with all of the study requirements; 9) a deficiency of clinical data; and 10) patients undergoing maintenance dialysis.
Among IgAN patients, a total of 193 patients were excluded for the following reasons: 92 patients had undergone treatment with corticosteroids, immunosuppressants, or bacteriotoxic drugs; 46 patients had a secondary cause of IgAN; and 55 patients had a deficiency of clinical data. Among non-IgAN patients, 72 patients were excluded for the following reasons: 31 patients had undergone treatment with corticosteroids, immunosuppressants, or bacteriotoxic drugs; 15 patients had a secondary cause of renal disease; and 26 patients had a deficiency of clinical data (Fig. 1).

Study selection flow chart
In total, 757 IgAN patients and 338 non-IgAN patients were enrolled in the study. In terms of causes of the non-IgAN primary renal diseases, 110 patients had minimal change disease (MCD), 21 patients had Focal Segmental Glomerular Sclerosis (FSGS), 201 patients had membranous nephropathy (MN), and 6 patients had mesangial proliferative glomerular nephritis (MpGN; Fig. 1).
One thousand ninety-five patients with primary glomerular nephropathy were assigned a 1:1 PSM using the PSM extension program in the SPSS software package. The PSM cohort included 204 IgAN patients and 204 non-IgAN patients. The composition of the non-IgAN group included 55 cases of MCD, 13 cases of FSGS, 20 cases of MN, and 6 cases of MpGN (Fig. 1).
Measurements
Clinical data collection
We recorded demographic data including age, gender, course of disease, blood pressure (BP) and body mass index (BMI). Immunological parameters (serum IgG, IgM, IgA, C3, and C4 levels) were measured by turbidimetric immunoassays, and the reagents were adjusted according to the IFCC/CRM 470 certified reference material published by the International Federation of Clinical Chemistry. Proteinuria was tested by immunoturbidimetry, and urine samples were collected between 7 a.m. and 7 a.m. the following day to measure albuminuria levels over a 24 h period. Laboratory data [including cholesterol, triglyceride (TGs), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), hemoglobin, albumin, globulin, fasting glucose, uric acid, serum cystatin C, blood urea nitrogen (BUN), and serum creatinine (Scr)] were collected immediately upon patient admission. All the experimental indices were measured on a 7180 Biochemical Automatic Analyzer (Hitachi, Tokyo, Japan).
Renal assessment
According to data on Chinese chronic kidney disease (CKD) patients, the eGFR was calculated using a modified equation for Modification of Diet in Renal Disease (MDRD) [27]:
Definitions
According to eGFR, CKD can be classified into 3 stages: 1) CKD1 stage (eGFR ≥90 mL/min per 1.73 m2), 2) CKD2 stage (eGFR 60–90 mL/min per 1.73 m2), and 3) CKD3–5stage (eGFR < 60 mL/min per 1.73 m2) [28]. In addition, patients were categorized into three groups according to proteinuria: ≤1 g/d, 1–3.5 g/d, and > 3.5 g/d [29]. According to the reagents tested in our hospital, serum IgA > 4.0 g/L was considered to be increased IgA and serum C3 < 0.8 g/L was considered to be decreased C3.
Statistical analyses
In order to reduce the heterogeneity of data, IgAN cases were matched via PSM to non-IgAN cases on the logit of the propensity score with nearest neighbor matching in a 1:1 manner, with a caliper of 0.02 with no replacements, according to age, gender, BMI, proteinuria, and eGFR.
Continuous variables are presented as the mean ± standard deviation (SD), while non-parametric variables are presented as the median and interquartile ranges. Categorical variables are expressed as the frequency and percentage. The logarithmic transformation of proteinuria in regression analysis was performed because of the skewed distribution.
Student’s t-test, analysis of variance (ANOVA), or non-parametric test was used to compare continuous variables between groups, where appropriate. Differences between categorical variables were analyzed using a chi-square test or double-tailed Fisher’s exact test, depending on applicability.
In view of the absence of standardized cut-off points for serum IgG, IgA, IgM, C3, and C4 levels, as well as a cut-off for the IgA/C3 ratio, the diagnostic performance of IgAN was assessed using a receiver operating characteristic (ROC) curve, and the area under the ROC (AUROC) curve analysis, in order to choose the best cut-off point after maximizing for total sensitivity and specificity (maximum Youden index). A ROC curve was also drawn to examine the performance of the IgA/C3 ratio in predicting IgAN in every proteinuria classification, and in different CKD stages. Comparisons of the AUROC between groups were evaluated using a Z-test.
Multivariate logistic regression models were employed to study the association of indices of IgAN with age, gender, IgA/C3 ratio and other variables, with significant associations (P < 0.05) explored in a univariate logistic regression analysis.
All values are two-tailed, and P < 0.05 was considered statistically significant. Data were analyzed using IBM SPSS Statistics version 25.0 for Windows (IBM, Armonk, NY, USA) and Medcalc (Version 11.2, MedCalc Software, BE).
Results
Demographic and clinical characteristics of the study population
The mean age of the full patient cohort was 34.76 years, and 49.41% of the patient cohort was male. The median course of disease was 6 months, and the mean BP of patients was 142/90 mmHg. In the non-IgAN group, 48.82% of patients were classified as in CKD 1 stage, 34.02% as CKD2 stage, and 17.16% as CKD3–5stage. The prevalence of CKD in the IgAN group was 41.08% CKD1 stage, 30.78% CKD2 stage, and 28.14% CKD3–5stage (Table 1).
The median proteinuria in the IgAN group was 0.88 g/d, which was much lower than that of the non-IgAN group (4.00 g/d). 53.10% of IgAN patients had proteinuria ≤1 g/d, 33.55% had proteinuria between 1 and 3.5 g/d, and only 13.34% had proteinuria > 3.5 g/d. Among non-IgAN patients, the percentage of patients within the three proteinuria classifications were 13.91, 29.29, and 56.80% for proteinuria ≤1 g/d, proteinuria 1–3.5 g/d, and proteinuria > 3.5 g/d, respectively (Table 1).
Among the full cohort, compared to non-IgAN patients, patients with IgAN had a younger mean age, and were more likely to be female. They also had a longer disease course, a higher prevalence of hematuria and lower prevalence of proteinuria, and higher BP, serum albumin, serum globulin, serum cystatin C, BUN and Scr. IgAN patients also had lower BMIs, and lower levels of hemoglobin, cholesterol, triglycerides, HDL-C, LDL-C and eGFR (P < 0.05). IgAN patients had higher levels of IgG, IgA, IgM, IgA/C3 ratio and a higher prevalence of increased IgA, decreased C3 and IgA/C3 ratio > 3.53, as well as lower levels of C3 and C4 than non-IgAN patients (P < 0.05; Table 1).
After PSM, we pair-matched 204 IgAN patients with 204 non-IgAN patients, and found no differences in demographic and clinical characteristics, including gender, disease course, BMI, and proteinuria classification. There were also no differences in the levels of hemoglobin, serum fasting glucose, triglycerides, uric acid, serum cystatin C, BUN, Scr, eGFR and C4. In the PSM cohort, IgAN patients still had higher levels of IgG, IgA, IgM, IgA/C3 ratio and a higher prevalence of increased IgA and IgA/C3 ratio > 3.53, and lower C3 levels than non-IgAN patients (P < 0.05; Table 1).
Comparison of the IgA/C3 ratio between IgAN and non-IgAN patients
In the full cohort and the PSM cohort, the mean serum IgA/C3 ratios of the IgAN groups were 2.98 ± 1.27 mmol/L and 2.87 ± 1.31 mmol/L, respectively, which were significantly higher than those of the non-IgAN groups (1.94 ± 0.92 mmol/L and 1.96 ± 0.91 mmol/L, respectively, both P < 0.001).
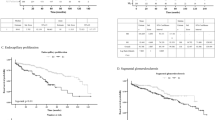
According to proteinuria levels, IgAN or non-IgAN patients were classified into three groups: ≤1 g/d, 1–3.5 g/d or > 3.5 g/d. IgAN patients in each cohort and in each of the three proteinuria groups had a higher IgA/C3 ratio than that of non-IgAN patients (all P < 0.001). Among the full cohort, only IgAN patients in the proteinuria> 3.5 g/d group had an IgA/C3 ratio lower than that of proteinuria≤1 g/d (P = 0.026), and non-IgAN patients in the proteinuria1–3.5 g/d group had an IgA/C3 ratio higher than that of proteinuria> 3.5 g/d in the PSM cohort (P = 0.026; Fig. 2).

Comparison of the IgA/C3 ratio in different proteinuria levels. (* indicated comparison with Non-IgAN group, p < 0.05; # indicated comparison with proteinuria≤1 g/d group in the full cohort and comparison with proteinuria 1–3.5 g/d group in the PSM cohort, p < 0.05)
We divided IgAN and non-IgAN patients into 3 CKD stages: CKD1, CKD2, and CKD3–5. In both the full cohort and the PSM cohort, the IgA/C3 ratio in patients with IgAN was significantly higher than that of non-IgAN patients, in all different groups (all P < 0.001). In the full cohort, non-IgAN patients in CKD3–5 stage had a higher IgA/C3 ratio than that of CKD1 and CKD2 stage patients (P = 0.005 and 0.021, respectively). IgAN patients in CKD3–5 stage had a higher IgA/C3 ratio than that of CKD1 stage patients (P = 0.023). There was no difference in the IgA/C3 ratio among non-IgAN and IgAN patients between different CKD groups in the PSM cohort (P = 0.116 and 0.578, respectively; Fig. 3).

Comparison of the IgA/C3 ratio in different CKD stages. (* indicated comparison with Non-IgAN group, p < 0.05; # indicated comparison with CKD 1 stage, p < 0.05; $ indicated comparison with CKD 2 stage, p < 0.05)
Predictors of IgAN
In order to distinguish between IgAN and non-IgAN, the ROC curve was used to assess the value of serum IgG, IgA, IgM, C3, and C4 levels, as well as the IgA/C3 ratio, in predicting IgAN. In both the full cohort and the PSM cohort, the AUROCs of the IgA/C3 ratio were as high as 0.767 (sensitivity 75.03%, specificity 67.46%, P < 0.001) and 0.734 (sensitivity 58.82%, specificity 77.45%, P < 0.001; Table 2 and Additional file 1: Figure S1).
In the different proteinuria groups, the highest AUROC of the IgA/C3 ratio in predicting IgAN was in the proteinuria≤1 g/d group (full cohort: AUROC 0.801, sensitivity 70.75%, specificity 80.85%; PSM cohort: AUROC 0.803, sensitivity 66.67%, specificity 82.98%; all P < 0.001), which was respectively significantly higher than that in the proteinuria> 3.5 g/d group (full cohort: AUROC 0.688, sensitivity 74.25%, specificity 59.16%; PSM cohort: AUROC 0.704, sensitivity 65.22%, specificity 70.00%; all P < 0.001) (full cohort: P = 0.011; PSM cohort: P = 0.021). There was no difference in the AUROC of the IgA/C3 ratio in predicting IgAN between all other groups (all P > 0.05; Table 3 and Additional file 2: Figure S2).
There was no difference in the AUROC of the IgA/C3 ratio in predicting IgAN between all the CKD groups (all P > 0.05; Table 4 and Additional file 3: Figure S3).
Prediction efficiency of specific cut-off points of the IgA/C3 ratio
In the PSM cohort, the 95% cut-off point for the IgA/C3 ratio in the non-IgAN group was 3.5304, and the 5% cut-off point for the IgA/C3 ratio in the IgAN group was 1.0546. This cut-off assumes that patients with an IgA/C3 ratio > 3.5304 are predicted to be IgAN, and patients with an IgA/C3 ratio < 1.0546 are non-IgAN. In the full cohort, the diagnostic accordance rate of an IgAN diagnosis among all patients with an IgA/C3 ratio > 3.5304 was as high as 92.02%, but the diagnostic accordance rate of a diagnosis of non-IgAN among all patients with an IgA/C3 ratio < 1.0546 was only 63.34% (Fig. 4).

Prediction efficiency of specific cut-off points of the IgA/C3 ratio
Factors associated with IgAN
In the full cohort, a multivariate logistic regression analysis was performed to clarify which factors were independently associated with IgAN. The analysis showed that the IgA/C3 ratio was independently correlated with IgAN, in multivariate adjusted models (all P < 0.001; Table 5).
Discussion
In the present study, we assessed 1095 primary glomerular nephropathy patients, including 757 IgAN patients and 338 Non-IgAN patients, to investigate whether a high IgA/C3 ratio could be used as a diagnostic criterion for IgAN, using a PSM method. Our study revealed that both in the full cohort and PSM cohort, the serum IgA/C3 ratio of the IgAN was significantly higher than that of the non-IgAN. The same results were also obtained when comparisons were stratified by level of proteinuria or level of renal function. In the PSM cohort, there was no difference in the IgA/C3 ratio of IgAN patients between different proteinuria groups and different CKD stages. The AUROC for the IgA/C3 ratio was 0.767 in the full cohort, and 0.734 in the PSM cohort in distinguishing IgAN among primary glomerular disease. The highest AUROC of the IgA/C3 ratio for an IgAN diagnosis was in the proteinuria≤1 g/d group (0.801 in the full cohort, and 0.803 in the PSM cohort); however, there was no difference in the AUROC of the IgA/C3 ratio between all CKD groups. Meanwhile, the diagnostic accordance rate for a diagnosis of IgAN among all patients with an IgA/C3 ratio > 3.5304 was as high as 92.02% in the full cohort. A multivariate logistic regression analysis showed that IgAN was independently correlated with IgA/C3 ratio.
In recent years, studies have confirmed that IgAN is a complex immune disease that involves deposits of the circulating immune complexes (CIC) IgA, C3, and IgG in the mesangial region of the glomeruli [11]. Although the pathophysiology of IgAN is still unclear, researchers currently favor a four-hit hypothesis, wherein GdIgA1 plays a key pathogenic role [11, 12]. Firstly, increased levels of circulating GdIgA1 with aberrant O-glycosylation of its hinge region result in exposed N-acetylgalactosamine. And then, N-acetylgalactosamine results in the production of unique antiglycan antibodies Gd-IgA1-binding proteins, which are thought to target the terminal N-acetylgalactosamine in the hinge region of Gd-IgA1. The third hit is the formation of pathogenic Gd-IgA1–containing CICs. Finally, these complexes are deposited in the mesangial region, leading to glomerular injury [11, 12, 30]. Studies have also revealed that mesangial IgA can activate C3, which speeds the production of terminal complex c5b-9, which in-turn activates macrophage to produce inflammatory mediators and matrix proteins. Thus, both IgA and C3 play an important role in the development and occurrence of IgAN. Due to glomerular deposition of IgA1 or IgA1-IgG immune complexes, serum C3 levels are lower in IgAN, and together with elevated serum IgA, this result in a higher IgA/C3 ratio, which can be used as a biomarker for IgAN [31]. In addition to measurements of pure serum IgA or C3 levels, previous studies have also found that the serum IgA/C3 ratio can clearly distinguish between severe IgA histological lesions and mild IgA histological lesions [13, 22, 32]. Our study is in line with these previous results, as in our PSM cohort, the AUROC of the IgA/C3 ratio for the diagnosis of IgAN reached 0.734, while the AUROC of IgA and C3 alone were only 0.696 and 0.621, respectively. However, additional data from larger samples are still needed, especially as previous studies have all examined relatively small patient populations.
In the present study, IgAN patients had a significantly higher IgA/C3 ratio than that of non-IgAN primary glomerular disease patients, in both the full cohort and the PSM cohort. Our results are consistent with previous studies [13, 14, 21, 22], and are also the first to demonstrate the predictive value of IgA/C3 ratio among primary glomerular nephropathy patients between different levels of proteinuria and different renal functions. The cut-off value of the serum IgA/C3 ratio was 2.102 in the full cohort, with an AUROC as high as 0.767 and 2.410, and an AUROC as high as 0.734 in the PSM cohort. These results are close to the cut-off value of 2.14 with an AUROC of 0.71, which was reported by Yasuhiko T et al. in a comparison of IgAN and non-IgAN patients [13]. The Yasuhiko T team also reported that the serum IgA/C3 ratio might be used to diagnose and predict prognostic grading in patients with IgAN [33], and combined with microscopic hematuria and/or persistent proteinuria, high serum IgA levels, and the serum IgA/C3 ratio could be used to distinguish IgAN from other primary renal diseases [34]. A study that collected data from 44 children with IgAN treated with multi-drug combination therapy showed that combined serum IgA/C3 ratio and glomerular C3 staining could predict the prognosis of IgA nephropathy [35]. However, a study involving 1564 IgAN patients indicated that a decrease in serum C3 levels in IgAN was not associated with renal progression [36].
Persistent proteinuria has proven to be an adverse prognostic factor for IgAN, as its progression varies with different levels of proteinuria. A follow-up study by Heather N. R et al. showed that when proteinuria level was < 1 g/d, the renal function of IgAN patients decreased at a 90% slower rate than average. The rate of renal function decrease was accelerated with increased proteinuria, and in IgAN patients with continuous proteinuria > 3 g/d, the decrease in renal function was 25 times faster than that of patients with proteinuria < 1 g/d [29]. Studies have also shown that compared to other types of progressive glomerulonephritis, IgAN appears to be associated with a poorer prognosis when presenting with nephrotic proteinuria between 3 and 3.5 g/d. Therefore, it has been suggested that IgAN with proteinuria < 1 g/d often indicates a favorable prognosis [29, 37,38,39,40]. Based on these observations, we divided proteinuria into three levels: ≤1 g/d, 1–3 g/d and > 3.5 g/d, and revealed that patients with proteinuria ≤1 g/d had the highest AUROC of the IgA/C3 ratio (which was higher than 0.80 in both the full cohort and the PSM cohort with cut-off points 2.229 and 2.352, respectively) in distinguishing IgAN among primary glomerular disease, while those in the proteinuria > 3.5 g/d group had the lowest. Meanwhile, renal function was also divided into three groups (eGFR ≥90, 90–60, and < 60 mL/min per 1.73 m2), but we found no difference in the AUROC of the IgA/C3 ratio for the diagnosis of IgAN between these groups.
In China, there are many nephropathy patients without access to renal biopsy. This is for a variety of reasons – such as the uneven distribution of medical resources, the prevalence of rural hospitals without access to biopsy technology, incidences of renal function impaired to a level unable to tolerate renal biopsy, and a prevalence of patients with a low level of proteinuria (i.e. < 1 g/d) with no obvious clinical symptoms, who elect not to undergo this invasive procedure. However, the prevalence of IgAN is very high in China, and therefore there is a strong need for noninvasive, readily available clinical indicators that better predict IgAN. Our study has shown that the IgA/C3 ratio, a non-invasive index, is of high predictive value for IgAN, especially in patients with primary glomerulonephritis with proteinuria < 1 g/d. Moreover, the predictive value of the IgA/C3 ratio is not affected by kidney function.
In analyzing non-experimental data without a random distribution, differences between groups must be considered, and the PSM approach simplifies this problem by considering only one dimension: the propensity score dimension. Rather than matching all variables, you may compare individual subjects based only on their propensity score [23,24,25,26, 41]. As a novel and effective statistical tool that is increasingly being used in clinical studies, the PSM method is able to correct initial data mismatch between control groups. In the present study, there were significant differences between the two groups in baseline indicators such as age, gender, proteinuria, BMI, and eGFR prior to matching. In order to exclude the influence of confounders, we used the PSM method to balance these non-observational factors to reach more reliable conclusions. In the end, we achieved very similar results in both the full cohort and the PSM cohort, indicating that the clinical significance of these indicators is trustworthy. Using this improved statistical method, we calculated the 95% cut-off point for the IgA/C3 ratio in the non-IgAN population, which was 3.5304, and the diagnostic accordance rate of an IgAN diagnosis among all patients with an IgA/C3 ratio > 3.5304 was as high as 92.02% in the full cohort. Moreover, by multivariate logistic regression analysis of the full cohort, we demonstrated that IgAN was independently correlated with the IgA/C3 ratio. Together this analysis demonstrates that our measured indicators are consistent with observed clinical symptoms.
The present study has several advantages. Firstly, we used a large sample size to prove that the IgA/C3 ratio is of diagnostic value to IgAN. Secondly, a stratified analysis was carried out, controlling for different levels of renal function and levels of proteinuria. The results showed that the IgA/C3 ratio, as a non-invasive index, was of higher predictive value for IgAN in patients with primary glomerulonephritis, particularly those whose proteinuria was less than 1 g/d, and was not affected by renal function. Thirdly, we suggest that this index can be applicable to patients with glomerulonephropathy in remote areas without access to renal biopsy, and to patients with severe renal failure where there is an inability to perform renal biopsy. The limitations to our study include a relatively small number of non-IgAN patients, particular those with normal GFR and proteinuria≤1 g/d, the inclusion of only two units of data, lack of the correlation between of IgA/C3 ratio and histopatological MEST score and the lack of multicenter and follow-up data. Additionally, as a cross-sectional clinical study, we were unable to explain why the IgA/C3 ratio has higher diagnostic efficacy in patients with proteinuria < 1 g/d and the potential role of IgA/C3 ratio as prognostic marker of therapeutic response. Finally, as an observational study, we cannot firmly establish a cause and effect relationship between IgA/C3 ratio and IgAN, thus additional basic research is needed.
Conclusions
In conclusion, the results of the present study provide clear evidence that the IgA/C3 ratio is a valid predictor for diagnosis of IgAN, particularly in patients with proteinuria less than 1 g/d. Additional multicenter large-scale studies are necessary in order to investigate the validity of this biomarker, and determine a standardized cut-off value.
References
Berger J, Hinglais N. Intercapillary deposits of IgA-IgG. Journal d'urologie et de nephrologie. 1968;74(9):694.
D'Amico G. The commonest glomerulonephritis in the world: IgA nephropathy. Q J Med. 1987;64(245):709–27.
Pesce F, Schena FP. Worldwide distribution of glomerular diseases: the role of renal biopsy registries. Nephrol Dial Transpl. 2010;25(2):334–6.
McGrogan A, Franssen CFM, de Vries CS. The incidence of primary glomerulonephritis worldwide: a systematic review of the literature. Nephrol Dial Transpl. 2011;26(2):414–30.
Glassock RJ. The pathogenesis of IgA nephropathy. Curr Opin Nephrol Hypertens. 2011;20(2):153–60.
Li L, Liu Z. Epidemiologic data of renal diseases from a single unit in China: analysis based on 13,519 renal biopsies. Kidney Int. 2004;66(3):920–3.
Tomino Y, Sakai H, Miura M, Endoh M, Nomoto Y. Detection of polymeric IgA in glomeruli from patients with IgA nephropathy. Clin Exp Immunol. 1982;49(2):419–25.
Berthoux FC, Mohey H, Afiani A. Natural history of primary IgA nephropathy. Semin Nephrol. 2008;28(1):4–9.
D'Amico G. Natural history of idiopathic IgA nephropathy and factors predictive of disease outcome. Semin Nephrol. 2004;24(3):179–96.
Barratt J, Feehally J. Treatment of IgA nephropathy. Kidney Int. 2006;69(11):1934–8.
Suzuki H, Kiryluk K, Novak J, Moldoveanu Z, Herr AB, Renfrow MB, Wyatt RJ, Scolari F, Mestecky J, Gharavi AG, et al. The pathophysiology of IgA nephropathy. Journal of the American Society of Nephrology : JASN. 2011;22(10):1795–803.
Maillard N, Wyatt RJ, Julian BA, Kiryluk K, Gharavi A, Fremeaux-Bacchi V, Novak J. Current understanding of the role of complement in IgA nephropathy. Journal of the American Society of Nephrology : JASN. 2015;26(7):1503–12.
Tomino Y, Suzuki S, Imai H, Saito T, Kawamura T, Yorioka N, Harada T, Yasumoto Y, Kida H, Kobayashi Y, et al. Measurement of serum IgA and C3 may predict the diagnosis of patients with IgA nephropathy prior to renal biopsy. J Clin Lab Anal. 2000;14(5):220–3.
Yanagawa H, Suzuki H, Suzuki Y, Kiryluk K, Gharavi AG, Matsuoka K, Makita Y, Julian BA, Novak J, Tomino Y. A panel of serum biomarkers differentiates IgA nephropathy from other renal diseases. PLoS One. 2014;9(5):e98081.
Zhang J, Wang C, Tang Y, Peng H, Ye ZC, Li CC, Lou TQ. Serum immunoglobulin a/C3 ratio predicts progression of immunoglobulin a nephropathy. Nephrology (Carlton). 2013;18(2):125–31.
Oortwijn BDP, Eijgenraam JM, Rastaldi MMP, Roos AP, Daha MRP, van Kooten CP. The role of secretory IgA and complement in IgA nephropathy. Semin Nephrol. 2008;28(1):58–65.
Trascasa ML, Egido J, Sancho J, Hernando L. IgA glomerulonephritis (Berger's disease): evidence of high serum levels of polymeric IgA. Clin Exp Immunol. 1980;42(2):247–54.
Moldoveanu Z, Wyatt RJ, Lee JY, Tomana M, Julian BA, Mestecky J, Huang WQ, Anreddy SR, Hall S, Hastings MC, et al. Patients with IgA nephropathy have increased serum galactose-deficient IgA1 levels. Kidney Int. 2007;71(11):1148–54.
Nakayama K, Ohsawa I, Maeda-Ohtani A, Murakoshi M, Horikoshi S, Tomino Y. Prediction of diagnosis of immunoglobulin a nephropathy prior to renal biopsy and correlation with urinary sediment findings and prognostic grading. J Clin Lab Anal. 2008;22(2):114–8.
Kim SJ, Koo HM, Lim BJ, Oh HJ, Yoo DE, Shin DH, Lee MJ, Doh FM, Park JT, Yoo TH, Kang SW, Choi KH, Jeong HJ, Han SH. Decreased circulating C3 levels and mesangial C3 deposition predict renal outcome in patients with IgA nephropathy. PLoS One. 2012;7(7):e40495. https://doi.org/10.1371/journal.pone.0040495. Epub 2012 Jul 6.
Komatsu H, Fujimoto S, Hara S, Sato Y, Yamada K, Eto T. Relationship between serum IgA/C3 ratio and progression of IgA nephropathy. Intern Med. 2004;43(11):1023–8.
Mizerska-Wasiak M, Małdyk J, Rybi-Szumińska A, Wasilewska A, Miklaszewska M, Pietrzyk J, Firszt-Adamczyk A, Stankiewicz R, Bieniaś B, Zajączkowska M. Relationship between serum IgA/C3 ratio and severity of histological lesions using the Oxford classification in children with IgA nephropathy. Pediatr Nephrol. 2015;30(7):1113.
Austin PC. A critical appraisal of propensity-score matching in the medical literature between 1996 and 2003. Stat Med. 2008;27(12):2037–49.
Rassen JA, Shelat AA, Franklin JM, Glynn RJ, Solomon DH, Schneeweiss S. Matching by propensity score in cohort studies with three treatment groups. Epidemiology (Cambridge, Mass). 2013;24(3):401–9.
Stürmer T, Joshi M, Glynn RJ, Avorn J, Rothman KJ, Rothman KJ, Schneeweiss S. A review of the application of propensity score methods yielded increasing use, advantages in specific settings, but not substantially different estimates compared with conventional multivariable methods. J Clin Epidemiol. 2006;59(5):431–7.
Brookhart MA, Sturmer T, Glynn RJ, Rassen J, Schneeweiss S. Confounding control in healthcare database research: challenges and potential approaches. Med Care. 2010;48(6 Suppl):S114–20.
Ying-Chun M, Li Z, Jiang-Hua C, Qiong L, Xue-Qing Y, Ying L, Jin-Sheng X, Song-Min H, Li-Ning W, Wen H. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006;17(10):2937.
Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, Hogg RJ, Perrone RD, Lau J, Eknoyan G, et al. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003;139(2):137.
Reich HN, Troyanov S, Scholey JW, Cattran DC, Toronto GR, For TTGR. Remission of proteinuria improves prognosis in IgA nephropathy. J Am Soc Nephrol. 2007;18(12):3177–83.
Suzuki H, Fan R, Zhang Z, Brown R, Hall S, Julian BA, Chatham WW, Suzuki Y, Wyatt RJ, Moldoveanu Z, et al. Aberrantly glycosylated IgA1 in IgA nephropathy patients is recognized by IgG antibodies with restricted heterogeneity. J Clin Invest. 2009;119(6):1668.
Satake K, Shimizu Y, Sasaki Y, Yanagawa H, Suzuki H, Suzuki Y, Horikoshi S, Honda S, Shibuya K, Shibuya A, et al. Serum under-O-glycosylated IgA1 level is not correlated with glomerular IgA deposition based upon heterogeneity in the composition of immune complexes in IgA nephropathy. BMC Nephrol. 2014;15(1):89.
Hiemstra PS, Biewenga J, Gorter A, Stuurman ME, Faber A, van Es LA, Daha MR. Activation of complement by human serum IgA, secretory IgA and IgA1 fragments. Mol Immunol. 1988;25(6):527.
Ishiguro C, Yaguchi Y, Funabiki K, Horikoshi S, Shirato I, Tomino Y. Serum IgA/C3 ratio may predict diagnosis and prognostic grading in patients with IgA nephropathy. NEPHRON. 2002;91(4):755–8.
Maeda A, Gohda T, Funabiki K, Horikoshi S, Shirato I, Tomino Y. Significance of serum IgA levels and serum IgA/C3 ratio in diagnostic analysis of patients with IgA nephropathy. J Clin Lab Anal. 2003;17(3):73–6.
Kawasaki Y, Maeda R, Ohara S, Suyama K, Hosoya M. Serum IgA/C3 and glomerular C3 staining predict severity of IgA nephropathy. Pediatr Int. 2018;60(2):162–7.
Yang X, Wei RB, Wang Y, Su TY, Li QP, Yang T, Huang MJ, Li KY, Chen XM. Decreased serum C3 levels in immunoglobulin a (IgA) nephropathy with chronic kidney disease: a propensity score matching study. Med Sci Monit. 2017;23:673–81.
Radford JMG, Donadio JJV, Bergstralh EJ, Grande JP. Predicting renal outcome in IgA nephropathy. J Am Soc Nephrol. 1997;8(2):199.
Szeto CC, Lai FM, To KF, Wong TY, Chow KM, Choi PC, Lui SF, Li PK. The natural history of immunoglobulin a nephropathy among patients with hematuria and minimal proteinuria. Am J Med. 2001;110(6):434–7.
Donadio JV, Bergstralh EJ, Grande JP, Rademcher DM. Proteinuria patterns and their association with subsequent end-stage renal disease in IgA nephropathy. Nephrol Dial Transplant. 2002;17(7):1197–203.
Eiro M, Katoh T, Kuriki M, Asano K, Watanabe K, Watanabe T. The product of duration and amount of proteinuria (proteinuria index) is a possible marker for glomerular and Tubulointerstitial damage in IgA nephropathy. NEPHRON. 2002;90(4):432–41.
Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar Behav Res. 2011;46(3):399–424.
Acknowledgements
The authors would like to acknowledge all patients and their families for participating in this study.
Funding
This work was financially supported by“the project of cultivating young teachers in Sun Yat-sen University” (No. 17kypy56). The funding body supported the team to design the study and collection, analysis, and interpretation of data and write the manuscript.
Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Contributions
WYG participated in the study design, performed literature review, and aided in manuscript preparation. ML performed the database setup and statistical analysis. DL, FNL, LHY and YQL performed the data collection and analysis and participated in manuscript writing. JZ and PH participated in the study design and coordination and helped to draft the manuscript. All of the authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was performed in adherence to the declaration of Helsinki and approved by the institutional ethics review boards (the third affiliated hospital of Sun Yat-Sen university and the first affiliated hospital of Jinan university), and was performed with an approved waiver of informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional files
Additional file 1:
Figure S1. ROC curve of serum IgG, IgA, IgM, C3, C4 and IgA/C3 ratio in predicting IgAN. (TIF 1613 kb)
Additional file 2:
Figure S2. ROC curve of IgA/C3 ratio in predicting IgAN in different proteinuria levels. (TIF 3214 kb)
Additional file 3:
Figure S3. ROC curve of IgA/C3 ratio in predicting IgAN in different CKD stages. (TIF 3265 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Gong, Wy., Liu, M., Luo, D. et al. High serum IgA/C3 ratio better predicts a diagnosis of IgA nephropathy among primary glomerular nephropathy patients with proteinuria ≤ 1 g/d: an observational cross-sectional study. BMC Nephrol 20, 150 (2019). https://doi.org/10.1186/s12882-019-1331-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12882-019-1331-0