
Abstract
Background
The identification of factors associated with functional impairment, in particular those which are potentially modifiable, may help to delay the advanced stages of functional dependence in patients with neurocognitive disorders such as Alzheimer’s disease and related disorders.
The objectives of the MEMORA cohort are to investigate the factors associated, first with functional autonomy change over time, and secondarily with the cognitive performance and behavioral disorders changes over time.
Methods
The MEMORA study is a multicenter prospective cohort study carried out throughout the patient’s care pathway, in Memory centers of Lyon (France). The study will include 6780 patients at all stages of memory disorders in 6 years. The follow-up for each patient is planned for 3 years. The main outcome is the functional autonomy level change as assessed by the instrumental abilities of daily living (IADL) score. Patient characteristics include sociodemographic and clinical features, neuropsychological performance, pharmaceutical and non-pharmaceutical therapy.
Discussion
This study conducted in a context of routine care may help to identify the factors associated with functional impairment related to progressive neurocognitive disorders. Subsequently, interventions on potentially modifiable factors could be proposed to the patients to improve their management and delay functional dependence.
Trial registration
NCT02302482, registered 27 November 2014.
Similar content being viewed by others


Background
Alzheimer’s disease and related disorders (ADRD) result in cognitive loss that progress towards functional loss of autonomy, and behavioral disorders [1, 2]. The decline of functional abilities and cognitive performance, as well as a behavioral disturbance are among the main predictors of nursing home placement, and therefore represent an important burden for the family and the society, and a public health stake [3]. Previous studies have identified a number of potential risk factors for ADRD, major neurocognitive disorders (NCD), or cognitive decline i.e. high blood pressure, vascular risk factors, stroke, arterial fibrillation, diabetes mellitus, hypercholesterolemia, hyperhomocysteinemia, biological inflammation, genetic biomarkers, obesity, sedentary lifestyle, smoking habit, depression, educational level [1, 4,5,6]. Nevertheless, the role of some of these factors on the progression of the NCD remains unclear [7, 8]. In addition, there is little published data on to the risk factors for loss of functional autonomy in patients at all stages of NCD. Indeed, the previous published studies have considered either community-dwelling elderly subjects without NCD at inclusion, or patients with AD among whose functional autonomy was already altered [9,10,11,12].
As research for a curative treatment of ADRD continues, identifying and improving the understanding of the factors implicated in the progression of functional disability could allow to develop and propose interventions to target potentially modifiable factors with the perspective to prevent or slow the functional disability in patients with NCD [13, 14].
The MEMORA cohort, including patients followed in memory centers (MC), has been designed to study the determinants for functional decline of patients at all stage of memory troubles including subjective cognitive decline (SCD), and minor or major neurocognitive disorders (NCD) [15, 16].
In this manuscript, the MEMORA study protocol is presented.
Methods
Aims
Primary aim
The primary aim of the MEMORA cohort is to study the relationship between patient characteristics and functional autonomy change over time among patients attending a MC, including neuropsychological performance, pharmaceutical and non-pharmaceutical therapy, clinical and sociodemographic characteristics.
Secondary aims
The secondary aims are to investigate the factors associated with cognitive performance and its change over time, and those associated with behavioral disorders.
The MEMORA cohort design
The MEMORA cohort is a prospective, open study, started in November 2014 and conducted in a context of routine care (Table 1). The study includes patients over a period of 6 years, and each patient is followed for 3 years. The data collection is carried out throughout the care pathway. At the first visit, patients undergo a clinical examination with a medical specialist (neurologist, geriatrician, or psychiatrist). Evaluations are performed at baseline and include functional autonomy level, cognitive performance and presence and severity of behavioral disorders; depending on their cognitive status patients may be referred to a neuropsychological examination. Patients are then routinely followed-up and data are prospectively collected in an electronic Case Report Form (eCRF) using the Easily® software (University Hospital of Lyon, France); the interval between visits is 6 months to 1 year as planned in routine care by the physician in charge of the patient. The number of follow-up visits per patients has not been determined in advance and may vary from a patient to another.
Study sites and population
The MEMORA cohort includes patients attending the MC of the Charpennes Hospital, Villeurbanne, France since 2014, and has been extended since 2017 to the MC of the Dugougon Hospital, Lyon, France. The MC role is to offer evaluation and follow-up for patients with cognitive disorders, generally referred by a general practitioner or medical specialists.
Inclusion criteria are: attending a medical appointment in the MC, living at home or in retirement facility. The patients are informed of the study and its objectives and are given the opportunity to object to participation. Exclusion criteria are: hearing or visual impairment preventing cognitive assessment, institutionalization, being under legal protection.
Ethical and legal considerations
Information is individually provided to the patients and caregivers at inclusion. The MEMORA cohort protocol (clinicaltrial.gov number NCT02302482) has been approved by the regional ethics committee (Comité de protection des personnes Sud Est III) on July 29, 2014. Data processing has been approved by the national data protection commission.
Primary outcome
The primary outcome of the MEMORA cohort is the change in the level of functional autonomy that is assessed using the 8-item version of the Lawton Instrumental Activities of Daily Living (IADL) score, and the 6-item version of the Disability Assessment for Dementia scale (DAD-6) [17, 18]. In the MEMORA study, the functional scales are collected during an interview of the primary caregiver or the patient with a physician, a nurse, or a psychologist. The change in functional autonomy will be measured using successive scores measured during patient follow-up visits at the MC.
Secondary outcomes
The secondary outcomes include global cognitive function measured using the Mini-Mental State examination (MMSE) [19], and behavioral disorders measured using the Neuropsychiatric Inventory (NPI) [20]. The MMSE score ranges from 0 to 30 (optimal cognitive performance) and is collected during an interview with the patient by a physician, a nurse, or a psychologist. The NPI score ranges from 0 to 144 (a higher score indicating a greater number/severity of disorders) and is collected during an interview with the primary caregivers by a physician, a nurse, or a psychologist.
Patient characteristics and evaluations
The patient characteristics and evaluations collected in the MEMORA study are listed in Table 1. Diagnosis stage and etiologies are determined by the medical specialist in charge of the patient (neurologist, geriatrician, or psychiatrist). Patients with a subjective cognitive complaint and absence of objective evidence (i.e. normal neuropsychological performance), are considered having SCD [16]. Mild and major neurocognitive disorders (NCD) are identified using the Diagnosis and Statistical Manual of mental disorders (DSM-V) nomenclature [15]. Previous medical history, family history of dementia, and comorbidities are also collected. The neuropsychological tests are chosen in a set of 142 tests allowing examining different cognitive functions (memory, executive functions, and instrumental abilities) by the psychologist, based on the patient’s cognitive status and the patient’s complaint or his entourage. The pharmacological drugs used by the patient are collected from the current general practitioner prescription and the specialist prescription at the MC. Home services, such as nurse care, day care admission, speech therapy, physical therapy, psychological support, cognitive rehabilitation or other non-pharmacological treatments are also collected. The caregiver burden is evaluated for the main caregiver who accompanies the patient at the MC using the mini-Zarit questionnaire [21].
Sample size
This study is designed to be descriptive rather than analytical. Based on the number of patients attending a memory consultation in the MCs and meeting the inclusion criteria, the number of patients that can be included in the study has been estimated at 1130 per year. As the means available allow to plan an inclusion for 6 years, the sample size is estimated at 6780 patients. With an expected loss of follow-up of 20% in the context of patients with cognitive disorders, the corrected sample size reaches 5650 patients. In case an association between one factor of 2 categories and the outcome change over time is to be assessed, this sample size would allow to detect an effect size of 0.1 between the 2 patients categories, at a risk alpha of 0.05, with a power of 96%. In case of factor with more than 2 categories, the power would reach 99%. This number of subjects seems sufficient to allow to assess the associations between various factors and the outcomes of the primary and secondary objectives.
Data management and statistical analyses
Data are monitored by a clinical research associate (CRA). Inconsistencies will be reported to the study investigators in order to decide whether the data should be corrected or considered as missing data. Any changes in the data will be reported.
Descriptive analyses
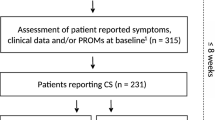
A flow-chart will present the number of patients included at baseline, and the number of patients with follow-up visits. Characteristics of the study population and proportions of missing values will be reported. Patient characteristics will be described using mean and standard deviation or median and interquartile range for quantitative variables, and frequencies and distribution for categorical variables. Comparison of baseline characteristics between patients with complete follow-up and those with attrition will be performed. In addition, methods for handling missing data will be used such as multiple imputation, by using mixed model or auxiliary variable when appropriate [22, 23].
Primary analysis
Univariate and multivariate analyses will be conducted to assess the relationship between the patient characteristics and the change in functional autonomy. Linear regression and ANOVA will be performed to assess the cross-sectional relationship between patient characteristics and functional autonomy scores. The successive assessments of the functional autonomy scores, considered as the dependent variables, will be modelled in a generalized linear mixed model to assess the longitudinal relationship between patient characteristics and change in functional autonomy [24,25,26]. The analyses will be adjusted for potential confounding factors when appropriate. An alpha level of 0.05 will be used for statistical significance, and tests will be bilateral.
Secondary analyses
Similar statistical methodologies will be applied to answer the secondary objectives. The successive measures of the MMSE and the NPI scores will be considered as the dependent variables of the models.
Data monitoring
The successful completion of the study is ensured by the CRA. The CRA also ensures compliance with the study protocol.
End of protocol
Patients are excluded from study follow-up if they no longer wish to participate at any time during the conduct of the study. However, as indicated in the information letter to the patients/caregivers, the data collected before exclusion may be used as part of the study.
Confidentiality
The nominative patient information the enabling follow-up to be conducted is kept in a separate file th at does not contain clinical data. The access to the nominative information is protected by a password and confidentiality is guaranteed by the study.
Protocol amendments
Any important modifications requiring a new ethics committee approval will be communicated in future publications. The potential impact of protocol modifications on the results will be discussed as appropriate.
Dissemination policy
The results of the primary and secondary objectives will be published in peer-reviewed journals. All authors of future publications will have to meet the criteria for authorship stated in the Uniform Requirements for Manuscripts Submitted to Biomedical Journals by the International Committee of Medical Journal Editors.
Discussion
The MEMORA cohort is conducted to investigate factors associated with progression of functional autonomy over time among patients with SCD or NCD in a real-life context. The data sources of the MEMORA cohort come from medical records and study-specific assessments. The real-life context of the study allows the inclusion of a large sample of patients at various stages of cognitive disorders and different management which can potentially influence the change over time of disorders related to NCD. This study can therefore been seen as a complementary approach to randomized controlled trials, which provide a higher level of evidence when well conducted but still represent high costs [27]. The results of this study should be beneficial to patients through the identification of profiles of at-risk patients and, later, targeted interventions could be assessed and proposed [28, 29]. Furthermore, the functional autonomy impairment that occurs during the course of NCD appears as a main factor associated with caregiver burden and rising societal costs, and therefore limiting its progression is likely to improve caregiver quality of life and better resource management [30,31,32]. The MEMORA study represents also an essential approach to assist the policymaker and healthcare decision-makers by providing results from a real-life context [33].
In terms of generalization of future results to other populations, the specificity of the study setting has be taken into account as the MCs are specialized in the ADRD diagnosis and management, providing early diagnosis and in-depth investigation. More generally, the limits associated with ADRD studies such as potential biases have been described [34], and will be taken into account when the results will be interpreted. Measurement and classification bias, referring to error in evaluation or classification of patients, could also occur and lead to reduce the reliability of the results. To limit these biases, training and information are regularly provided to the medical staff.
Conclusion
The MEMORA-cohort conducted in a context of routine care may help to identify the factors associated with functional impairment related to progressive neurocognitive disorders, and improve the understanding of functional and cognitive impairment as well as behavioral disorders over time. This may eventually lead to propose interventions on potentially modifiable factors to improve management and delay functional dependence of ADRD patients.
Availability of data and materials
The final dataset of the MEMORA study will not be publicly available due to regulations and agreements obtained to perform the study, but will be available on reasonable request after publication of the primary objective. Data requests can be submitted to the researchers at the Memory Research Centre of Lyon (CMRR of Lyon, Charpennes Hospital, University Hospital of Lyon, Villeurbanne, France).
Abbreviations
- AD:
-
Alzheimer’s disease
- ADRD:
-
Alzheimer’s disease and related disorders
- CRA:
-
Clinical research associate
- IADL:
-
Instrumental abilities of daily living
- MC:
-
Memory centers
- MMSE:
-
Mini-Mental State examination
- NCD:
-
Neurocognitive disorders
- NPI:
-
Neuropsychiatric inventory
- SCD:
-
Subjective cognitive decline
References
Ballard C, Gauthier S, Corbett A, Brayne C, Aarsland D, Jones E. Alzheimer’s disease. Lancet. 2011;377:1019–31.
Tschanz JT, Corcoran C, Schwartz S, et al. Progression of cognitive, functional and neuropsychiatric symptom domains in a population cohort with Alzheimer’s dementia the Cache County dementia progression study. Am J Geriatr Psychiatry. 2011;19:532–42.
Toot S, Swinson T, Devine M, Challis D, Orrel M. Causes of nursing home placement for older people with dementia: a systematic review and meta-analysis. Int Psychogeriatr. 2017;29:195–208.
Lipnicki DM, Crawford J, Kochan NA, et al. Risk factors for mild cognitive impairment, dementia and mortality: the Sydney memory and ageing study. J Am Med Dir Assoc. 2017;18:388–95.
Abellan van Kan G, Rolland Y, Nourhashémi F, Coley N, Andrieu S, Vellas B. Cardiovascular disease risk factors and progression of Alzheimer’s disease. Dement Geriatr Cogn Disord. 2009;27:240–6.
Musicco M, Palmer K, Salamone G, et al. Predictors of progression of cognitive decline in Alzheimer’s disease: the role of vascular and sociodemographic factors. J Neurol. 2009;256:1288–95.
Sims-Robinson C, Kim B, Rosko A, Feldman EL. How does diabetes accelerate Alzheimer disease pathology? Nat Rev Neurol. 2010;6:551–9.
Barocco F, Spallazzi M, Concari L, Gardini S, Pelosi A, Caffarra P. The progression of Alzheimer’s disease: are fast decliners really fast? A four-year follow-up. J Alzheimers Dis. 2017;57:775–86.
Pérès K, Verret C, Alium A, Barberger-Gateau P. The disablement process: factors associated with progression to disability and recovery in French elderly people. Disabil Rehabil. 2005;27:263–76.
Dharmasaroja PA, Lolekha P, Kulkantrakorn K, Charernboon T, Watcharakorn A, Piyabhan P. Natural course and predictors of severe disability and death in Thai patients with dementia. J Clin Neurosci. 2017;46:37–40.
Lechowski L, De Stampa M, Tortrat D, et al. Predictive factors of rate of loss of autonomy in Alzheimer’s disease patients. A prospective study of the REAL.FR cohort. J Nutr Health Aging. 2005;9:100–4.
Palmer K, Lupo F, Perri R, et al. Predicting disease progression in Alzheimer's disease: the role of neuropsychiatric syndromes on functional and cognitive decline. J Alzheimers Dis. 2011;24:35–45.
McLaren AN, Lamantia MA, Callahan CM. Systematic review of non-pharmacologic interventions to delay functional decline in community-dwelling patients with dementia. Aging Ment Health. 2013;17(6):655–66.
Rosenberg PB, Mielke MM, Tschanz J, et al. Effects of cardiovascular medications on rate of funtional decline in Alzheimer disease. Am J Geriatr Psychiatry. 2008;16:883–92.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC; 2013. https://guides.library.ualberta.ca/apa-citation-style/dsm-v.
Jessen F, Amariglio RE, van Boxtel M, et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer's disease. Alzheimers Dement. 2014;10:844–52.
Lawton M, Brody E. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179–86.
de Rotrou J, Wu YH, Hugonot-Diener L, et al. DAD-6: a 6-item version of the disability assessment for dementia scale which may differenciate Alzheimer's disease and mild cognitive impairment from controls. Dement Geriatr Cogn Disord. 2012;33:210–8.
Folstein M, Folstein S. Mini-mental state: a practical method for grading the cognitive Stade of patients for the clinician. J Psychiatr Res. 1975;12:189–98.
Mckeith I, Cummings J. Behavioural changes and psychological symptoms in dementia disorders. Lancet Neurol. 2005;4:735–42.
Revel V, Haritchabalet I, Kervinio C, et al. Construction d'une échelle simplifiée pour la détection en médecine générale du fardeau de l'aidant d'une personne âgée dépendante. L'année gérontologique. 2002;16:131–7.
Ferro MA. Missing data in longitudinal studies: cross-sectional multiple imputation provides similar estimates to full-information maximum likelihood. Ann Epidemiol. 2014;24:75–7.
Twisk J, de Boer M, de Vente W, Heymans M. Multiple imputation of missing values was not necessary before performing a longitudinal mixed-model analysis. J Clin Epidemiol. 2013;66:1022–8.
Locascio JJ, Atri A. An overview of longitudinal data analysis methods for neurological research. Dement Geriatr Cogn Disord. 2011;1:330–57.
Wolkewitz M, Allignol A, Harbarth S, de Angelis G, Schumacher M, Beyersmann J. Time-dependent study entries and exposures in cohort studies can easily be sources of different and avoidable types of bias. J Clin Epidemiol. 2012;65:1171–80.
Liu S, Rovine MJ, Molenaar PC. Selecting a linear mixed model for longitudinal data: repeated measures analysis of variance, covariance pattern model, and growth curve approaches. Psychol Methods. 2012;17:15–30.
Maisonneuve H, Babany G. Données de vie réelle et recherche clinique: le complément des données des essais randomisés? Presse Med. 2015;44:586–9.
Callahan CM, Boustani MA, Schmid AA, et al. Targeting functional decline in Alzheimer disease. Ann Intern Med. 2017;166:164–71.
Vellas B, Andrieu S, Sampaio C, Caley N, Wilcock G. Endpoints for trials in Alzheimer’s disease: a European task force consensus. Lancet Neurol. 2008;7:436–50.
Gustavsson A, Brinck P, Bergvall N, et al. Predictors of costs of care in Alzheimer’s disease: a multinational sample of 1222 patients. Alzheimers Dement. 2011;7:318–27.
Hill J, Fillit H, Thomas S, Chang S. Functional impairment, healthcare costs and the prevalence of institutionalisation in patients with Alzheimer’s disease and other dementias. Pharmacoeconomics. 2006;24:265–80.
Joling KJ, Schöpe J, van Hout HP, van Marwijk HW, van der Horst HE, Bosmans JE. Predictors of societal costs in dementia patients and their informal caregivers: a two-year prospective cohort stud. Am J Geriatr Psychiatry. 2015;23:1193–203.
Garrison LJ, Neumann PJ, Erickson P, Marshall D, Mullins CD. Using real-world data for coverage and payment decisions: the ISPOR real-world data task force report. Value Health. 2007;10:326–35.
Weuve J, Proust-Lima C, Power MC, et al. Guidelines for reporting methodological challenges and evaluating potential bias in dementia research. Alzheimers Dement. 2015;11:1098–109.
Acknowledgements
The authors thank all the specialist physicians of the geriatric and memory centers who contribute to inclusion of patients in the study, Philippe Castets (DSII, Hospices Civils de Lyon), and the IT service for their support for the creation and maintenance of the MEMORA cohort database, the memory center of Charpenne Hospital and the Dugougon Hospital for their contribution to data collection, and the Dr. Philip Robinson (DRCI, Hospices Civils de Lyon) for help in manuscript preparation.
*The MEMORA group includes:
Pierre Krolak-Salmon, Virginie Dauphinot, Florian Delphin-Combe, Zaza Makaroff, Denis Federico, Marie-Hélène Coste, Isabelle Rouch, Jean-Michel Dorey, Alexis Lepetit, Keren Danaila, Julien Vernaudon, Anthony Bathsavanis, Alain Sarciron, Yves Guilhermet, Sylvain Gaujard, Pierre Gromaître, Claire Moutet, Mathieu Verdurand.
Funding
The MEMORA study is supported by a grant of the MSD Avenir fund. This funding body enabled the funding of a researcher and nurses to carry out the research and the questionnaires; it had no role in the design of the study, the collection, the analysis, the interpretation and the writing in the manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
All authors have read and approved the manuscript. VD participated to the conception and design of the study, will conduct data analysis, interpret results, and drafted this manuscript. CM, IR, FDC, MV, CM and SG are participating to the inclusion of patients and the data collection, will conduct data analysis and interpret results and critically revised this manuscript. PKS conceived the research idea, is responsible for the data, is participating to the inclusion of patients, will interpret results and critically revised this manuscript.
Authors’ information
Not applicable
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approvals were obtained with three committees as required in France: the Committee for the protection of persons concerned (CPP) on July 29, 2014, the Advisory Committee on Information Processing in Material Research in the Field of Health, and the National Commission for Data Protection and Liberties (CNIL). Witten information was provided to participants and oral consent had to be obtained to participate, as required by the French committee for this type of non-interventional study. The study enrolment began in November 2014. The study enrolment began in November 2014.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Dauphinot, V., Moutet, C., Rouch, I. et al. A multicenter cohort study to investigate the factors associated with functional autonomy change in patients with cognitive complaint or neurocognitive disorders: the MEMORA study protocol. BMC Geriatr 19, 191 (2019). https://doi.org/10.1186/s12877-019-1204-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12877-019-1204-1