
Abstract
Background
Patients with significant comorbidities often are denied laparoscopic colorectal resections, because they are thought to be too “high-risk.” This study was designed to examine the feasibility and safety of laparoscopic colorectal resections in high-risk colorectal cancer patients and to compare them with a similar cohort of patients undergoing open resections in the same time period.
Methods
This was a single-center, prospective, cohort study conducted at a high-volume, nonuniversity, tertiary care hospital. From a database of 616 patients submitted to elective colorectal surgery for cancer within a fast-track protocol (January 2005 to November 2011), 188 patients who met at least one minor (age >80 years and body mass index (BMI) >30 m/kg2) and one major (cardiac, pulmonary, renal or liver disease, diabetes mellitus) criterion were classified as high-risk. Differences in baseline characteristics, intraoperative outcomes, and short-term (30-day) postoperative outcomes, as well as the pathology findings and the readmission and reoperation rates, were compared between the open and laparoscopic cohorts in both high- and low-risk groups and between high- and low-risk groups.
Results
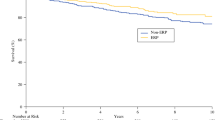
During the study period, 68 high-risk patients underwent laparoscopic resections and 120 had open surgeries. A shorter length of postoperative stay (6 vs. 9 days, p < 0.0001) and fewer postoperative nonsurgical complications (4 % vs. 19 %, p = 0.003) were observed among the laparoscopic group. Postoperative major (p = 0.774) and minor complications (p = 0.3) and reoperations (p = 0.196) were similar between the two groups, and a significantly lower rate of mortality (1.5 vs. 7.5 %, p = 0.038) was observed in the laparoscopic group than in the open group.
Conclusions
Laparoscopic colorectal resection can be safely performed on “high-risk” surgical patients with better results than a similar group of high-risk patients undergoing open colon resections.
Similar content being viewed by others


References
Schlinkert RT (1991) Laparoscopic-assisted right hemicolectomy. Dis Colon Rectum 34:1030–1031
Tinmouth J, Tomlinson G (2004) Laparoscopically assisted versus open colectomy for colon cancer. N Engl J Med 351(9):933–934
Guillou P, Quirke P, Thorpe H, Walker J, Jaine DG, Smith AM (2005) Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre randomized controlled trial. Lancet 365:1718–1726
Lacy AM, Garcia-Valdecasas JC, Pique JM, Delgado S, Campo E, Bordas JM (1995) Short-term outcome analysis of a randomized study comparing laparoscopic vs open colectomy for colon cancer. Surg Endosc 9:1101–1105
The COLOR Study Group (2000) COLOR: a randomized clinical trial comparing laparoscopic and open resection for colon cancer. Dig Surg 17:617–622
Rea JD, Cone MM, Diggs BS, Deveney KE, Lu KC, Herzig DO (2011) Utilization of laparoscopic colectomy in the United States before and after the clinical outcomes of surgical therapy study group trial. Ann Surg 254(2):281–288
Bilimoria KY, Bentrem DJ, Nelson H et al (2008) Use and outcomes of laparoscopic-assisted colectomy for cancer in the United States. Arch Surg 143(9):832–839
Marks JH, Kawun UB, Hamdan W, Marks G (2008) Redefining contraindications to laparoscopic colorectal resection for high-risk patients. Surg Endosc 22(8):1899–1904
Plocek MD, Geisler DP, Glennon EJ, Kondylis P, Reilly JC (2005) Laparoscopic colorectal surgery in the complicated patient. Am J Surg 190(6):882–885
Hemandas AK, Abdelrahman T, Flashman KG et al (2010) Laparoscopic colorectal surgery produces better outcomes for high risk cancer patients compared to open surgery. Ann Surg 252(1):84–89
McCloskey CA, Wilson MA, Hughes SJ, Eid GM (2007) Laparoscopic colorectal surgery is safe in the high-risk patient: a NSQIP risk-adjusted analysis. Surgery 142(4):594–597
Poon JT, Law WL, Chow LC, Fan JK, Lo SH (2011) Outcome of laparoscopic resection for colorectal cancer in patients with high operative risk. Ann Surg Oncol 18(7):1884–1890
Arteaga González I, López-Tomassetti Fernández EM, Hernández Piñero Y et al (2008) Effectiveness of colorectal laparoscopic surgery on patients at high anesthetic risk: an intervention cohort study. Int J Colorectal Dis 23(1):101–106
Salihoglu Z, Baca B, Koksal S et al (2009) Analysis of laparoscopic colorectal surgery in high-risk patients. Surg Laparosc Endosc Percutan Tech 19(5):397–400
Feroci F, Kröning KC, Lenzi E, Moraldi L, Cantafio S, Scatizzi M (2011) Laparoscopy within a fast-track program enhances the short-term results after elective surgery for resectable colorectal cancer. Surg Endosc 25(9):2919–2925
Scatizzi M, Kröning KC, Boddi V, De Prizio M, Feroci F (2010) Fast-track surgery after laparoscopic colorectal surgery: is it feasible in a general surgery unit? Surgery 147(2):219–226
Gerges FJ, Kanazi GE, Jabbour-Khoury SI (2006) Anesthesia for laparoscopy: a review. J Clin Anesth 18:67–78
Bufalari A, Ferri M, Cao P et al (1996) Surgical care in octogenarians. Br J Surg 83:1783–1787
Reiss R, Deutsch A, Nudelman J (1992) Surgical problems in octogenarians: epidemiologic analysis of 1083 consecutive admissions. World J Surg 16:1017–1021
Isbister WH (1997) Colorectal surgery in the elderly: an audit of surgery in octogenarians. Aust N Z J Surg 67:557–561
Israelsson LA, Jonsson (1997) Overweight and healing of midline incisions: the importance of suture technique. Eur J Surg 163:175–180
Pikarsky AJ, Saida Y, Yamagucki T et al (2002) Is obesity a high-risk factor for laparoscopic colorectal surgery? Surg Endosc 16:855–858
Roberts JV, Bates T (1992) The use of body mass index in studies of abdominal wound infection. J Hosp Infect 20:217–220
Rullier E, Laurent C, Garrelon JL, Michel P, Saric J, Parneix M (1998) Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg 85:355–358
Frasson M, Braga M, Vignali A, Zuliani W, Di Carlo V (2008) Benefits of laparoscopic colorectal resection are more pronounced in elderly patients. Dis Colon Rectum 51(3):296–300
Law WL, Chu KW, Tung PH (2002) Laparoscopic colorectal resection: a safe option for elderly patients. J Am Coll Surg 195(6):768–773
Miller RD (ed) (2005) Miller’s anesthesia. Elsevier Churchill Livingstone, Philadelphia
Davenport DL, Bowe EA, Henderson WG, Khuri SF, Mentzer RM Jr (2006) National Surgical Quality Improvement Program (NSQIP) risk factors can be used to validate American Society of Anesthesiologists Physical Status Classification (ASA PS) levels. Ann Surg 243(5):636–641
Mak PH, Campbell RC, Irwin MG (2002) The ASA Physical Status Classification: inter-observer consistency. Anaesth Intensive Care 30:633–640
Haynes SR, Lawler PGP (1995) An assessment of the consistency of ASA Physical Status Classification allocation. Anaesthesia 50:195
Owens WD, Felts JA, Spitznagel EL Jr (1978) ASA Physical Status Classifications: a study of consistency of ratings. Anesthesiology 49:239–243
Bennett CL, Stryker SJ, Ferreira MR, Adams J, Beart RW Jr (1997) The learning curve for laparoscopic colorectal surgery: preliminary results from a prospective analysis of 1,194 laparoscopic-assisted colectomies. Arch Surg 132:41–44
Marusch F, Gastinger I, Schneider C et al (2001) Laparoscopic Colorectal Surgery Study Group (LCSSG). Experience as a factor influencing the indications for laparoscopic colorectal surgery and results. Surg Endosc 15:116–120
Schlacta CM, Mamazza J, Seshadri PA, Cadeddu M, Gregoire R, Poulin EC (2001) Defining a learning curve for laparoscopic colorectal resections. Dis Colon Rectum 44:217–222
Disclosures
Francesco Feroci, Maddalena Baraghini, Elisa Lenzi, Alessia Garzi, Andrea Vannucchi, Stefano Cantafio, and Marco Scatizzi have no conflict of interest or financial ties to disclose.
Funding
There was no financial support for this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Feroci, F., Baraghini, M., Lenzi, E. et al. Laparoscopic surgery improves postoperative outcomes in high-risk patients with colorectal cancer. Surg Endosc 27, 1130–1137 (2013). https://doi.org/10.1007/s00464-012-2559-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-012-2559-y