
Abstract
Background
Achievement of normal volume status is crucial in hemodialysis (HD), since both volume expansion and volume contraction have been associated with adverse outcome and events.
Objectives
The objectives of this study are to assess the prevalence of fluid volume expansion and depletion and to identify the best clinical parameter or set of parameters that can predict fluid volume expansion in HD patients.
Design
This study is cross-sectional.
Setting
This study was conducted in three hemodialysis units.
Patients
In this study, there are 194 HD patients.
Methods
Volume status was assessed by multifrequency bio-impedance spectroscopy (The Body Composition Monitor, Fresenius) prior to the mid-week HD session.
Results
Of all patients, 48 % (n = 94) were volume-expanded and 9 % of patients were volume-depleted (n = 17). Interdialytic weight gain was not different between hypovolemic, normovolemic, and hypervolemic patients. Fifty percent of the volume-expanded patients were hypertensive. Paradoxical hypertension was very common (31 % of all patients); its incidence was not different between patient groups. Intradialytic hypotension was relatively common and was more frequent among hypovolemic patients. Multivariate regression analysis identified only four predictors for volume expansion (edema, lower BMI, higher SBP, and smoking). None of these parameters displayed both a good sensitivity and specificity.
Limitations
The volume assessment was performed once.
Conclusions
The study indicates that volume expansion is highly prevalent in HD population and could not be identified using clinical parameters alone. No clinical parameters were identified that could reliably predict volume status. This study shows that bio-impedance can assist to determine volume status. Volume status, in turn, is not related to intradialytic weight gain and is unable to explain the high incidence of paradoxical hypertension.
Abrégé
Mise en contexte
L’atteinte d’une volémie normale est primordiale dans le suivi des patients sous hémodialyse. Les états d’expansion et de contraction du volume hydrique sont associés aux complications majeures de l’insuffisance rénale et à une issue défavorable de la maladie.
Objectifs de l’étude
Cette étude visait à évaluer la prévalence de l’expansion et de la déplétion des fluides en situation d’hémodialyse. On a également voulu identifier les paramètres cliniques qui pourraient permettre de prévoir les épisodes d’expansion de volume hydrique chez les patients dialysés.
Cadre et type d’étude
Il s’agit d’une étude transversale qui s’est tenue dans trois unités d’hémodialyse, sur un total de 194 patients.
Methodes
La volémie des Par spectroscopie de bio-impédance à multifréquence (« Body composition Monitor » de Fresenius) tout juste avant la séance d’hémodialyse prévue en milieu de semaine.
Résultats
De tous les patients qui ont participé à l’étude, une proportion de 48 % (n = 94) était en situation d’expansion volumique alors que 9 % (n = 17) se trouvaient en état de déplétion. Toutefois, la prise de poids interdialytique était semblable pour tous les patients, qu’ils aient été hypovolémiques, normovolémiques ou hypervolémiques avant la séance d’hémodialyse. Il est à noter que la moitié des patients (50 %) en situation d’expansion volémique souffraient également d’hypertension artérielle. De fait, l’hypertension artérielle paradoxale s’est avérée répandue parmi les patients dialysés (31 %), mais aucune variation notable de son incidence n’a été observée dans les différents groupes. Les cas d’hypotension intradialytiques quant à eux, se sont avérés relativement courants, particulièrement chez les sujets hypovolémiques avant la séance d’hémodialyse. L’analyse par régression multivariée n’a révélé que quatre indicateurs susceptibles d’aider à prévoir les épisodes d’expansion de volume : la présence d’œdème, un indice de masse corporelle faible, une pression artérielle systolique élevée avant l’hémodialyse, ainsi que le fait de fumer. Cependant, aucun de ces paramètres n’a présenté une spécificité au plan diagnostique ni une sensibilité particulière pour prévoir les épisodes d’expansion de volume.
Limites de l’étude
La volémie des participants n’a été mesurée qu’une seule fois lors de cette étude.
Conclusion
L’étude a révélé une prévalence élevée de l’expansion du volume hydrique chez les patients sous hémodialyse, mais il a été impossible de la détecter à l’aide des paramètres cliniques utilisés. Qui plus est, aucun des paramètres mesurés n’a permis d’anticiper avec certitude des variations de la volémie. Concernant la bio-impédance, les résultats ont révélé qu’elle pourrait aider à évaluer l’expansion de volume chez les patients dialysés. En revanche, cette dernière ne peut être associée directement à la prise de poids intradialytique pas plus qu’elle ne peut à elle seule expliquer la forte incidence d’hypertension artérielle paradoxale.
Similar content being viewed by others

What was known before
Prevalence of extracellular fluid volume expansion has been previously reported to be high.
What this adds
The present study confirms the high prevalence of volume expansion and indicates that this cannot be estimated by clinical parameters. Moreover, the study adds that volume contraction is also relatively common. Last, volume status is not related to intradialytic weight gain and is unable to explain the high incidence of paradoxical hypertension.
Background
Accurate assessment of volume status (VS) remains one of the greatest challenges in the treatment of hemodialysis (HD) patients [1]. Chronic volume expansion contributes to hypertension, left ventricular hypertrophy, and heart failure in HD patients [2–6]. Conversely, volume contraction could predispose the HD patient to intradialytic hypotension, cramps, arrhythmias, cardiac stunning, and reduced well-being after treatment [2]. Therefore, adequate extracellular fluid volume (ECFV) control is crucial for blood pressure regulation and for prevention of cardiovascular complications in this population [7].
Clinical assessment of volume expansion by assessing blood pressure, edema, and central venous pressure has limitations [8–11]. Interdialytic weight gain (IDWG) is not sufficient to assess volume expansion since it does not necessarily correlate with ECFV expansion [12]. The inferior vena cava collapse index [2], ultrasound assisted assessment of pulmonary fluid content [13], and echocardiography [2] are helpful to assess volume status, but they do not provide an estimate of total ECFV expansion or depletion and are impractical for usage in clinical practice. Multifrequency bio-impedance spectroscopy is a convenient method to assess extracellular and intracellular fluid volume [14]. This method has been validated against gold standard dilution methods [14, 15] and is applicable in the setting of HD [16].
Given the mortality associated with ECFV expansion [6, 17] and the knowledge that adequate volume control provides better control of blood pressure [18], more accurate objective methods for volume assessment would be valuable. In the current study, we tested the hypothesis that volume expansion is highly prevalent in HD patients, likely due to the inability to judge volume status from clinical parameters. Bio-impedance spectroscopy was applied to assess volume status in an in-center HD population and compared with clinical volume assessment. Our aims were (1) to assess the prevalence of volume expansion and volume depletion in our HD population using bio-impedance spectroscopy measurements, (2) to investigate the association between clinical parameters and volume status as assessed by bio-impedance, and (3) to search for a set of clinical parameters that best predict volume status in HD patients.
Methods
Patients
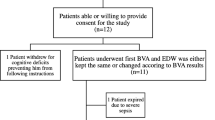
Two hundred HD sequential adult patients were included in the study. Inclusion criteria included all prevalent HD patients who agreed to participate in the study in three HD units of the Northern Alberta Renal Program. Patients were not included or excluded based on their blood pressure. Exclusion criteria were as follows: patients with a pacemaker or implanted defibrillator, amputation, and metallic prosthesis. Six patients were excluded from the analysis since they were new hemodialysis starts (<6 weeks) before the measurement. Ethics approval was obtained from the Human Research Ethics Board at the University of Alberta Hospital. All patients included in the study provided written informed consent.
Evaluation of volume status
The Body Composition Monitor (BCM, Fresenius Medical Care, Bad Homburg, Germany) is a multifrequency bio-impedance device that provides a convenient method to obtain extracellular fluid volume (ECFV) and has been validated previously [19]. The BCM uses the same technology as the HYDRA ECF/ICF 4200 platform (Xitron, San Diego, USA) used in this validation study. Overhydration is calculated by comparison of the measured ECFV with the predicted ECFV using a physiological model [20] with adjustments for subjects with high body mass index [21]. Measurements were performed at one occasion in triplicate with the device. Measurements were performed before the start of mid-week HD treatment with the patients in supine position for 10 min. Electrodes were applied on the ipsilateral arm and foot of the non-AV-fistula side. The BCM measures the impedance of different body compartments at 50 different frequencies between 5 and 1000 kHz. The BCM calculates volume status (VS) which is expressed as volume excess or depletion in liters compared to the estimated normal ECFV. The accuracy of bio-impedance in ECFV is estimated to be within −0.4 ± 1.4 L when compared to dilution methods [19]. To facilitate comparison between patients, the volume status was normalized to estimated extracellular fluid volume (VS/ECFV). The patient population was divided into hypovolemic, normovolemic, and hypervolemic groups. Volume contraction was considered more than 7 % below normal ECFV (equivalent to 1.1 L below normal ECFV) prior the mid-week HD session. Normovolemia was considered any measurement between −7 and +7 % relative to normal ECFV. Volume expansion was considered more than 7 % above normal ECFV (equivalent to 1.1 L above normal ECFV). The 7 % cutoff point was based on the thought that with a 75 mmol/d sodium intake, patients ideally swing from −1.1 below normal ECFV after their run to +1.1 L above normal ECFV before the next run.
Clinical and biochemical parameters
Clinical parameters collected include pre- and post-dialysis blood pressure for the same session and five previous sessions. BP was measured in the sitting position. Hypertension was considered if the average pre-dialysis BP exceeded 140/90 mmHg for the current and the four previous sessions or if the patient had a history of hypertension as defined by being prescribed antihypertensive medication. The prevalence of hypertension was calculated from this composite data. Intradialytic hypotension was defined as post-dialysis SBP falling below 100 mmHg and the difference between pre-dialysis SBP and post-dialysis SBP >20 mmHg with accompanying clinical symptoms during dialysis that required an intervention or cessation of ultrafiltration [22]. As there is no widely accepted definition of paradoxical hypertension [23], we considered it as a rise of SBP of >20 mmHg during or after dialysis with post-dialysis BP exceeding 140/90 mmHg. Patients were considered to have diabetes if it was mentioned in their charts or if the patient was on anti-diabetic medications. Pedal edema was assessed as present or absent. Dry weight (DW) was obtained from the patient charts. IDWG for the previous five sessions was recorded. IDWG was calculated by subtracting the post-dialysis weight of previous HD session from the pre-dialysis weight of the index HD session. To determine the correlation between IDWG and volume expansion, IDWG more than 7 % of ideal ECFV was considered elevated. All biochemical parameters (plasma Na, K, serum albumin, WBCs, urea reduction ratio, and cholesterol level) were obtained from the most recent monthly blood work of the patient. Clinical volume assessment was performed weekly by rounding physicians. Dialysate sodium composition was 137 mmol/L for all patients regardless of their plasma sodium concentration.
Statistical analysis
Continuous data are expressed as mean ± standard deviation. Categorical variables are expressed as percentage of total. One way ANOVA was used for univariate comparisons. Bonferroni multiple comparison test was used to detect between group differences when ANOVA showed a statistically significant result. Pearson’s test was used for univariate correlations. Multiple linear regression was performed with VS/ECFV% (volume status/extracellular fluid volume) as the target variable, to find predictors for volume expansion. Variables selected for the multivariate model based on a significant univariate analysis with a P value <0.10. Sensitivity and specificity were calculated using standard formulae. All data analysis was done with Graph prism (Graphpad 5, San Diego, CA, USA) and SPSS version 21 (SPSS Inc., Chicago, IL, USA). A P value <0.05 was considered statistically significant.
Results
General characteristics of the study population
Forty-five percent of the 194 participants were hypertensive as classified by the average pre-dialysis blood pressure for five HD sessions. On average patients displayed volume expansion with an average volume status of +7.8 % (volume expansion related to ECFV). Antihypertensive medication was prescribed in 48 % of patients. Most commonly prescribed were beta-blockers (26 %), calcium channel blockers (21 %), and angiotensin-converting enzyme inhibitors (12 %) Angiotensin receptor blockers and loop diuretics were prescribed in 3 and 14 % of patients, respectively. Characteristics of the patients are displayed in Table 1.
Prevalence of volume abnormalities
VS of all patients is shown in Fig. 1. In 43 % of the patients VS was normal (between −7 % and +7 % of the ideal ECFV); 48 % percent of all patients displayed >7 % ECFV expansion. Of these, 47 % (23 % of all patients) exhibited volume expansion >15 % of ECFV. Volume contraction of >7 % was observed in 9 % of the patients. Interestingly, clinically assessed fluid overload (in percentage of normal ECFV) in the hypervolemic group was significantly higher than the normovolemic group but not different from the hypovolemic group. Clinically assessed volume status and volume status assessed by the BCM were correlated, yet the slope was 0.265 and patients were estimated to be 11 % fluid overload clinically at the point where the BCM did not detect any fluid overload.

a Frequency distribution of volume status corrected for extracellular fluid volume (VS/ECFV) for the whole study population. b Frequency distribution of interdialytic weight gain (IDWG) for the whole study population corrected for ECFV. VS/ECFV volume status/extracellular fluid volume, IDWG/ECFV interdialytic weight gain/extracellular fluid volume
Comparison of characteristics of hypovolemic, normovolemic, and hypervolemic patients
Hypertension, diabetes, smoking, and edema were more common and intradialytic hypotension less common in hypervolemic patients. Pulse pressure was higher in hypervolemic patients. When patients with mild volume expansion (+7 % < VS/ECFV < +15 %) were compared to patients with severe volume expansion (VS/ECFV > +15 %), incidence of edema and plasma potassium was higher in patients with severe volume expansion. No other clinical parameters were different between these patients. IDWG/ECFV displayed wide variation yet IDWG/ECFV and VS/ECFV were not correlated (Fig. 2; r 2 = 0.009945, P = 0.19).

a No significant correlation between volume status and IDWG (both corrected for ECFV) could be demonstrated, P = 0.985. b Correlation between clinically assessed volume status (VSclin/ECFV) and volume status assessed with the BCM (VS/ECFV). IDWG/ECFV interdialytic weight gain/extracellular fluid volume, VS/ECFV volume status/extracellular fluid volume as assessed by the BCM, VS clin /ECFV volume status as clinically assessed/extracellular fluid volume
Relation between blood pressure and volume status as assessed by bio-impedance
Twenty eight percent of the patients had hypertension and ECFV expansion. Of all patients, 23.5 % were normotensive and normovolemic and 19.5 % had normal blood pressure despite volume expansion. The majority of volume-expanded patients had normal blood pressure. Pre-dialysis BP was not significantly different between groups. Only Pre-dialysis PP was significantly higher in normovolemic patients compared to hypovolemic patients. Only pre-dialysis SBP showed a weak correlation to VS corrected for ECFV.
Incidence of intradialytic hypotension and paradoxical hypertension
Intradialytic hypotension was found in 17 % of patients. Intradialytic hypotension was significantly more common in hypovolemic patients (P = 0.007). The incidence of paradoxical hypertension was high (31 %), yet prevalence was not different between groups. The distribution of severity of paradoxical hypertension is shown in Fig. 3.

Frequency distribution of severity of paradoxical hypertension, illustrated as rise in SBP in mmHg (post-dialysis SBP—pre-dialysis SBP), average rise of SBP from pre- to post-dialysis was 38 mmHg. SBP systolic blood pressure
Clinical parameters and volume expansion
After univariate analysis, nine variables were included in the multiple regression model (DM, HTN, edema, BMI, smoking, pre-HD-PP, pre-HD-SBP, sodium, and albumin). Edema, lower BMI, SBP, and smoking were significant predictors for volume expansion (Table 2). Relative risk was most pronounced for edema (Table 3). Sensitivity, specificity, and positive and negative predictive values for the four individual parameters are shown in Table 3 and precluded the development of a robust volume expansion score. The cutoff points for calculating sensitivity and specificity for continuous variables were 140 mmHg for SBP and 25 for BMI, respectively.
Discussion
In the current study, ECFV expansion as assessed by bio-impedance in in-center HD patients was highly prevalent. ECFV contraction was also observed and was more frequently associated with intradialytic hypotension. Paradoxical hypertension was highly prevalent and not associated with volume status. Several clinical parameters were more prevalent in HD patients with ECFV expansion, however, were not sufficiently sensitive and specific to be applied to robustly assess volume status.
Fluid volume expansion in HD patients is a well-recognized problem [12, 24] associated with hypertension [2, 3], left ventricular hypertrophy, dilated cardiomyopathy [4], heart failure, and eventually with high mortality [5, 6]. Strikingly, about 50 % of our patients displayed mild to severe ECFV expansion of >7 % of ECFV. Moderate to severe ECFV expansion of >15 % of ECFV was observed in 23 % of the patients, despite frequent routine clinical volume assessment. Previous studies using bio-impedance for quantification of volume status reported slightly lower [25] or similarly high prevalence of ECFV expansion [4, 5]. Of note, volume status and interdialytic weight gain were not correlated in the current study. This implies that strategies to improve volume status need to separately address dry weight and dietary salt intake to achieve good volume regulation. Underscoring the relevance of IDWG, one study reported that reducing the interdialytic weight gain without changing the dry weight reduced ventricular hypertrophy [26]. Therefore, although the debate as to whether chronic ECFV expansion or IDWG is the most important factor determining cardiovascular outcome is not settled, controlling fluid overload can reduce hypertension and LVH and improve outcome [27]; controlling the latter could decrease cardiac stunning [28, 29].
Pre-dialysis volume depletion of >7 % of ECFV (comparable to 1.1 L for average ECFV) was demonstrated in 9 % of patients, compared to >1.1 L in 5 % of patients in a previous report [25]. Volume-depleted patients only differed from normo- or hypervolemic patients regarding more frequent intradialytic hypotension. Intradialytic hypotension occurred in 17 % of all patients. Previous studies reported the incidence of intradialytic hypotension to be between 15 and 25 % of HD sessions [30, 31]. Since volume status was assessed pre-dialysis and several hypovolemic patients had substantial interdialytic weight gains of >25 % of ECFV, these patients would be severely hypovolemic post-dialysis. Although several patients with volume depletion had very substantial interdialytic weight gain, no correlation could be established between interdialytic weight gain and volume contraction. Fluid overload has previously been inversely associated with IDWG, in about 15000 patients from 60 dialysis centers [12]. Taken together, our study indicates that a relevant fraction of patients showed fluid depletion and a higher risk of intradialytic hypotension.
Hypertension was present in 54 % (27 % of total) of hypervolemic and in 36 % (19 % of total) of normovolemic patients. Fluid status and systolic blood pressure were correlated, in contrast to ECFV expansion and diastolic and pulse pressure. This shows that the relationship between blood pressure and volume status is complex. Wabel et al. analyzed the relation between blood pressure and volume expansion using comparable methodology in 500 HD patients [32]. Volume-dependent hypertension was found in 15 % of patients; the majority of patients (27 %) were normotensive and normovolemic. Only 10 % of patients had normal blood pressure despite volume expansion. This suggests that volume expansion is responsible for hypertension in HD patients; yet, the use of antihypertensives might obscure the importance of fluid overload for BP control.
Paradoxical hypertension in HD patients has been associated with increased risk of mortality [33]. Paradoxical hypertension was common in our study population (31 %) and was not significantly different among the three patient groups. Limited information is available about the prevalence of paradoxical hypertension and its relation to volume status in a large HD population. A previous study using similar definition of paradoxical hypertension reported prevalence in 21 % of patients [34]. UF rate was significantly lower in patients with paradoxical hypertension; however, no assessment of ECFV was performed [34]. Using several different definitions for paradoxical hypertension, other studies report incidence of 10–15 % [23]. A recent study reported a decline in the incidence of paradoxical hypertension with excessive ultrafiltration concluding that intradialytic hypertension may be a sign of volume expansion [35]; ECFV was not assessed in that study. Altogether, our data indicate a high frequency of paradoxical hypertension but no clear association with volume expansion. Moreover, it underscores the need to understand this important problem with consequences for outcome better [36].
In search for clinical and laboratory characteristics associated with volume status, multivariate regression analysis identified only four predictors for volume expansion (edema, lower BMI, higher SBP, and smoking). None of these parameters displayed both a good sensitivity and specificity. In our study, the presence of edema had a good positive predictive value. A previous study reported that pedal edema correlates well with cardiovascular risk factors and left ventricular mass, but it did not reflect volume in HD patients as assessed by cardiac biomarkers and echocardiography [37]. Using a similar methodology in PD patients, multiple regression analysis revealed that DM, higher SBP, older age, male gender, lower serum albumin, and lower BMI were significant predictors for volume expansion [38]. It seems therefore that a set of parameters that can assist to better assess fluid volume in HD patients on clinical grounds cannot be formulated. In addition to the evaluation of specific clinical indicators of fluid overload, we related the clinically assessed volume status to the estimated normal ECFV and compared this with the volume status measured by the BCM. This yields the interesting observation that although there is a positive correlation between clinically assessed and BCM assessed volume status, clinical assessment indicated fluid overload at normovolemia assessed by BCM. Moreover, the slope between clinically assessed and BCM assessed VS was far below unity. This indicates that a clinical assessment is not precise and that severe fluid overload is underestimated.
Our study has several limitations. First of all, bio-impedance spectroscopy-based extracellular fluid volume assessment has an error of −0.4 ± 1.4 L compared to gold standard dilution methods [19]. The study did not separately assess the validity on the 120 healthy subjects in the study and the 32 HD patients. However, a recent review reported that radioisotope methods, previously considered the gold standard, have similar accuracy compared to bio-impedance in dialysis patients [39]. Moreover, bio-impedance is highly reproducible with inter-observer and intra-observer errors of less than 2 % [39]. The measurement was performed once, prior to the second dialysis session of the week. Although this could introduce some noise, it is not likely that it would affect our interpretation of the data. Finally, we cannot assure that different devices to assess fluid status and different methodology to calculate the normal ECFV or an individual would not lead to slightly different numerical results. It is considered not likely that the overall interpretation of the study would have been different.
Conclusions
In summary, using bio-impedance spectroscopy, we found that volume expansion is highly prevalent in our HD patients and volume contraction was also not uncommon. Intradialytic hypotension was more common in hypovolemic patients. Fluid volume expansion or contraction could not be reliably identified by clinical parameters, except that edema predicted fluid volume expansion. This study shows that bio-impedance can assist to determine volume status. Volume status, in turn, is not related to intradialytic weight gain and is unable to explain the high incidence of paradoxical hypertension. Whether volume expansion or contraction determined using bio-impedance is associated with worse outcome still needs to be determined.
References
Wizemann V, Schilling M. Dilemma of assessing volume state—the use and the limitations of a clinical score. Nephrol Dial Transplant. 1995;10(11):2114–7.
Braam B, Jindal K, Mees EJD. Hypertension and cardiovascular aspects of dialysis treatment: clinical management of volume control. vol Book, Whole. Pabst Science Publishers; 2011.
Leypoldt JK, Cheung AK, Delmez JA, Gassman JJ, Levin NW, Lewis JAB, et al. Relationship between volume status and blood pressure during chronic hemodialysis. Kidney Int. 2002;61(1):266–75.
Machek P, Jirka T, Moissl U, Chamney P, Wabel P. Guided optimization of fluid status in haemodialysis patients. Nephrol Dial Transplant. 2010;25(2):538–44. doi:10.1093/ndt/gfp487.
Voroneanu L, Cusai C, Hogas S, Ardeleanu S, Onofriescu M, Nistor I, et al. The relationship between chronic volume overload and elevated blood pressure in hemodialysis patients: use of bioimpedance provides a different perspective from echocardiography and biomarker methodologies. Int Urol Nephrol. 2010;42(3):789–97.
Kalantar-Zadeh K, Regidor DL, Kovesdy CP, Van Wyck D, Bunnapradist S, Horwich TB, et al. Fluid retention is associated with cardiovascular mortality in patients undergoing long-term hemodialysis. Circulation. 2009;119(5):671–9. doi:10.1161/CIRCULATIONAHA.108.807362.
Ozkahya M, Ok E, Toz H, Asci G, Duman S, Basci A, et al. Long-term survival rates in haemodialysis patients treated with strict volume control. Nephrol Dial Transplant. 2006;21(12):3506–13. doi:10.1093/ndt/gfl487.
Dou Y, Zhu F, Kotanko P. Assessment of extracellular fluid volume and fluid status in hemodialysis patients: current status and technical advances. Seminars in Dialysis; 2012: Wiley Online Library.
Kooman JP, van der Sande FM, Leunissen KM. Sodium, blood pressure and cardiovascular pathology: is it all volaemia? Nephrol Dial Transplant. 2004;19(5):1046–9. doi:10.1093/ndt/gfh091.
Raimann J, Liu L, Tyagi S, Levin NW, Kotanko P. A fresh look at dry weight. Hemodial Int. 2008;12(4):395–405.
Sinha AD. Why assistive technology is needed for probing of dry weight. Blood Purif. 2011;31(1-3):197–202. doi:10.1159/000321840;10.1159/000321840.
Hecking M, Karaboyas A, Antlanger M, Saran R, Wizemann V, Chazot C et al. Significance of interdialytic weight gain versus chronic volume overload: consensus opinion. American Journal of Nephrology. 2013;38(1):78-90. doi:10.1159/000353104; 10.1159/000353104.
Vitturi N, Dugo M, Soattin M, Simoni F, Maresca L, Zagatti R, et al. Lung ultrasound during hemodialysis: the role in the assessment of volume status. Int Urol Nephrol. 2014;46(1):169–74.
Basso F, Milan Manani S, Cruz DN, Teixeira C, Brendolan A, Nalesso F, et al. Comparison and reproducibility of techniques for fluid status assessment in chronic hemodialysis patients. Cardiorenal Med. 2013;3(2):104–12. doi:10.1159/000351008.
Piccoli A. Estimation of fluid volumes in hemodialysis patients: comparing bioimpedance with isotopic and dilution methods. Kidney Int. 2014;85(4):738–41.
Oei EL, Fan SL. Practical aspects of volume control in chronic kidney disease using whole body bioimpedance. Blood Purif. 2015;39(1-3):32–6. doi:10.1159/000368953.
Wizemann V, Wabel P, Chamney P, Zaluska W, Moissl U, Rode C, et al. The mortality risk of overhydration in haemodialysis patients. Nephrology, Dialysis, Transplantation. 2009;24(5):1574–9. doi:10.1093/ndt/gfn707.
Charra B, Bergstrom J, Scribner BH. Blood pressure control in dialysis patients: importance of the lag phenomenon. Am J Kidney Dis. 1998;32(5):720–4.
Moissl UM, Wabel P, Chamney PW, Bosaeus I, Levin NW, Bosy-Westphal A, et al. Body fluid volume determination via body composition spectroscopy in health and disease. Physiol Meas. 2006;27(9):921.
Wang Z, Deurenberg P, Wang W, Pietrobelli A, Baumgartner RN, Heymsfield SB. Hydration of fat-free body mass: new physiological modeling approach. Am J Physiol. 1999;276(6 Pt 1):E995–E1003.
Chamney PW, Wabel P, Moissl UM, Muller MJ, Bosy-Westphal A, Korth O, et al. A whole-body model to distinguish excess fluid from the hydration of major body tissues. Am J Clin Nutr. 2007;85(1):80–9.
Sulowicz W, Radziszewski A. Pathogenesis and treatment of dialysis hypotension. Kidney Int. 2006;70:S36–S9. doi:10.1038/sj.ki.5001975.
Inrig JK. Intradialytic hypertension: a less-recognized cardiovascular complication of hemodialysis. Am J Kidney Dis. 2010;55(3):580–9. doi:10.1053/j.ajkd.2009.08.013.
Charra B, Chazot C. Volume control, blood pressure and cardiovascular function. Lessons from hemodialysis treatment. Nephron Physiol. 2003;93(4):p94-101. doi:70242.
Passauer J, Petrov H, Schleser A, Leicht J, Pucalka K. Evaluation of clinical dry weight assessment in haemodialysis patients using bioimpedance spectroscopy: a cross-sectional study. Nephrology, Dialysis, Transplantation. 2010;25(2):545–51. doi:10.1093/ndt/gfp517.
Fagugli RM, Reboldi G, Quintaliani G, Pasini P, Ciao G, Cicconi B, et al. Short daily hemodialysis: blood pressure control and left ventricular mass reduction in hypertensive hemodialysis patients. Am J Kidney Dis. 2001;38(2):371–6. doi:10.1053/ajkd.2001.26103.
London GM, Pannier B, Guerin AP, Blacher J, Marchais SJ, Darne B, et al. Alterations of left ventricular hypertrophy in and survival of patients receiving hemodialysis: follow-up of an interventional study. J Am Soc Nephrol. 2001;12(12):2759–67.
Burton JO, Jefferies HJ, Selby NM, McIntyre CW. Hemodialysis-induced cardiac injury: determinants and associated outcomes. Clin J Am Soc Nephrol. 2009;4(5):914–20. doi:10.2215/CJN.03900808.
McIntyre CW. Haemodialysis-induced myocardial stunning in chronic kidney disease—a new aspect of cardiovascular disease. Blood Purif. 2010;29(2):105–10. doi:10.1159/000245634;10.1159/000245634.
Tomson CR. Advising dialysis patients to restrict fluid intake without restricting sodium intake is not based on evidence and is a waste of time. Nephrol Dial Transplant. 2001;16(8):1538–42.
van der Sande FM, Kooman JP, Leunissen KM. Intradialytic hypotension—new concepts on an old problem. Nephrol Dial Transplant. 2000;15(11):1746–8.
Wabel P, Moissl U, Chamney P, Jirka T, Machek P, Ponce P, et al. Towards improved cardiovascular management: the necessity of combining blood pressure and fluid overload. Nephrology, Dialysis, Transplantation. 2008;23(9):2965–71. doi:10.1093/ndt/gfn228.
Inrig JK, Patel UD, Toto RD, Szczech LA. Association of blood pressure increases during hemodialysis with 2-year mortality in incident hemodialysis patients: a secondary analysis of the Dialysis Morbidity and Mortality Wave 2 Study. Am J Kidney Dis. 2009;54(5):881–90.
Van Buren PN, Kim C, Toto RD, Inrig JK. The prevalence of persistent intradialytic hypertension in a hemodialysis population with extended follow-up. Int J Artif Organs. 2012;35(12):1031–8. doi:10.5301/ijao.5000126;10.5301/ijao.5000126.
Agarwal R, Light RP. Intradialytic hypertension is a marker of volume excess. Nephrol Dial Transplant. 2010;25(10):3355–61. doi:10.1093/ndt/gfq210.
Locatelli F, Cavalli A, Tucci B. The growing problem of intradialytic hypertension. Nat Rev Nephrol. 2010;6(1):41–8. doi:10.1038/nrneph.2009.200.
Agarwal R, Andersen MJ, Pratt JH. On the importance of pedal edema in hemodialysis patients. Clin J Am Soc Nephrol. 2008;3(1):153–8. doi:10.2215/CJN.03650807.
Van Biesen W, Williams JD, Covic AC, Fan S, Claes K, Lichodziejewska-Niemierko M, et al. Fluid status in peritoneal dialysis patients: the European Body Composition Monitoring (EuroBCM) study cohort. PLoS One. 2011;6(2):e17148.
Davies SJ, Davenport A. The role of bioimpedance and biomarkers in helping to aid clinical decision-making of volume assessments in dialysis patients. Kidney Int. 2014;86(3):489–96. doi:10.1038/ki.2014.207.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The Northern Alberta Renal Program of Alberta Health Services provided financial support for the study. Fresenius provided the bio-impedance equipment for the study, however, had no role in the design of the study, the recruitment of patients, the data analysis, and the report. Ms. Kalainy has obtained travel support from Fresenius to present part of her data at the Am. Soc. Nephrology Meeting in Atlanta in 2013.
Authors’ contributions
SK performed the measurements, analyzed the data, and drafted the manuscript. RR assisted in the study design, performed the measurements, and edited the manuscript. KJ edited the manuscript. NP assisted in data analysis and edited the manuscript. BB designed this study, assisted in data analysis, and drafted the manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kalainy, S., Reid, R., Jindal, K. et al. Fluid volume expansion and depletion in hemodialysis patients lack association with clinical parameters. Can J Kidney Health Dis 2, 54 (2015). https://doi.org/10.1186/s40697-015-0090-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40697-015-0090-5