
Abstract
Objective
Iodine-131 (I-131) radioactive iodine therapy (RAI) after total thyroidectomy is the standard treatment for patients with differentiated thyroid cancer (DTC). We investigated the relationship between the quantitative parameters of the iodine uptake and the disappearance of the accumulation in the thyroid bed in adjuvant therapy using a 1.11 GBq or 3.70 GBq dose of I-131.
Methods
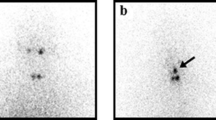
We retrospectively analyzed the cases of 40 patients with DTC who were treated with RAI at our institution between April 2017 and August 2019. The patients were treated with the I-131 dose of 1.11 GBq (n = 25) or 3.70 GBq (n = 15) after total thyroidectomy. The I-131 whole-body scan and hybrid single-photon emission computed tomography/X-ray computed tomography (SPECT/CT) were performed 3 days after RAI. Using image analysis software, we measured the standardized uptake value (SUV) and absolute radioactivity concentration (kBq/ml) on the target lesions with the highest uptake in the thyroid bed.
Results
The median period from RAI to the evaluation of the absence of uptake of the thyroid bed was 6.75 months. After RAI, uptake of the thyroid bed disappeared in 26 of the 40 patients. The disappearance rate was significantly higher in the 3.70 GBq group than in the 1.11 GBq group (86.7% vs. 52.0%, respectively; p = 0.029). However, there were no significant differences in the values of kBq/ml or SUV between the 1.11 GBq group and 3.70 GBq group. On the other hand, the group in which the uptake disappeared after RAI showed significantly higher kBq/ml max and kBq/ml mean values than the group in which the uptake did not disappear after RAI (p = 0.028, p = 0.032, respectively). The SUVmax and SUVmean also tended to be higher in the disappeared-uptake group than the not-disappeared-uptake group, but the differences were not significant (p = 0.166, p = 0.176, respectively).
Conclusions
The quantitative evaluation might be useful as one of the predictive indicators of the disappearance of the accumulation of radioactive iodine in the thyroid bed.





Similar content being viewed by others


References
The Japanese clinical practice guidelines for the management of thyroid tumor 2018. J JAES JSTS. 36:46–56.
Dong F, Li L, Bian Y, Li G, Han X, Li M, et al. Standardized uptake value using thyroid quantitative SPECT/CT for the diagnosis and evaluation of graves’ disease: a prospective multicenter study. Biomed Res Int. 2019. https://doi.org/10.1155/2019/7589853.
Ross JC, Vilić D, Sanderson T, Vöö S, Dickson J. Does quantification have a role to play in the future of bone SPECT? Eur J Hybrid Imaging. 2019;3:8.
Vija AH, Bartenstein PS, Froelich JW, Kuwert T, Macapinlac H, Daignault CP, et al. ROC study and SUV threshold using quantitative multi-modal SPECT for bone imaging. Eur J Hybrid Imaging. 2019;3:10.
Jun M, Alexander HV. Evaluation of quantitation accuracy for xSPECT. IEEE Nucl Sci Symp Conf Rec. 2015. https://doi.org/10.1109/NSSMIC.2015.7582030.
De Laroche R, Robin P, Schick U, Le Roux PY, Querellou S, Guezennec C, et al. Therapeutic response assessment of bone metastatic prostate carcinoma treated by abiraterone using x-SPECT Quant®: preliminary results. J Nucl Med. 2016;57(suppl 1):1422.
De Laroche R, Bourhis D, Robin P, Delcroix O, Querellou S, Malhaire JP, et al. Feasibility study and preliminary results of prognostic value of bone SPECT-CT quantitative indices for the response assessment of bone metastatic prostate carcinoma to abiraterone. Front Med. 2019;6:342.
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;21:1–133.
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American thyroid association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214.
Huang YT, Ravi Kumar AS, Bhuta S. 18F-FDG PET/CT as a semiquantitative imaging marker in HPV-p16-positive oropharyngeal squamous cell cancers. Nucl Med Commun. 2015;36:16–20.
Mazzaferri EL, Robbins RJ, Spencer CA, Braverman LE, Pacini F, Wartofsky L, et al. A consensus report of the role of serum thyroglobulin as a monitoring method for low-risk patients with papillary thyroid carcinoma. J Clin Endocrinol Metab. 2003;88:1433–41.
Kanda Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48:452–8.
Fallahi B, Beiki D, Takavar A, Fard-Esfahani A, Gilani KA, Saghari M, et al. Low versus high radioiodine dose in postoperative ablation of residual thyroid tissue in patients with differentiated thyroid carcinoma: a large randomized clinical trial. Nucl Med Commun. 2012;33:275–82.
Watanabe K, Uchiyama M, Fukuda K. The outcomes of I-131 ablation therapy for intermediate and high-risk differentiated thyroid cancer using a strict definition of successful ablation. Jpn J Radiol. 2017;35:505–10.
Acknowledgments
This work was supported in part by JSPS KAKENHI Grant Number 20K08075 and 19H03600.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Konishi, K., Ishiba, R., Ikenohira, T. et al. The relationship between the quantitative evaluation of thyroid bed uptake and the disappearance of accumulation in adjuvant radioactive iodine therapy for differentiated thyroid cancer. Ann Nucl Med 35, 159–166 (2021). https://doi.org/10.1007/s12149-020-01546-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-020-01546-8