
Abstract
Background
Models of hypoxemic lung injury caused by lavage-induced pulmonary surfactant depletion are prone to prompt recovery of blood oxygenation following recruitment maneuvers and have limited translational validity. We hypothesized that addition of injurious ventilation following surfactant-depletion creates a model of the acute respiratory distress syndrome (ARDS) with persistently low recruitability and higher levels of titrated “best” positive end-expiratory pressure (PEEP) during protective ventilation.
Methods
Two types of porcine lung injury were induced by lung lavage and 3 h of either protective or injurious ventilation, followed by 3 h of protective ventilation (N = 6 per group). Recruitment maneuvers (RM) and decremental PEEP trials comparing oxygenation versus dynamic compliance were performed after lavage and at 3 h intervals of ventilation. Pulmonary gas exchange function, respiratory mechanics, and ventilator-derived parameters were assessed after each RM to map the course of injury severity and recruitability.
Results
Lung lavage impaired respiratory system compliance (Crs) and produced arterial oxygen tensions (PaO2) of 84±13 and 80±15 (FIO2 = 1.0) with prompt increase after RM to 270–395 mmHg in both groups. After subsequent 3 h of either protective or injurious ventilation, PaO2/FIO2 was 104±26 vs. 154±123 and increased to 369±132 vs. 167±87 mmHg in response to RM, respectively. After additional 3 h of protective ventilation, PaO2/FIO2 was 120±15 vs. 128±37 and increased to 470±68 vs. 185±129 mmHg in response to RM, respectively. Subsequently, decremental PEEP titration revealed that Crs peaked at 36 ± 10 vs. 25 ± 5 ml/cm H2O with PEEP of 12 vs. 16 cmH2O, and PaO2/FIO2 peaked at 563 ± 83 vs. 334 ± 148 mm Hg with PEEP of 16 vs. 22 cmH2O in the protective vs. injurious ventilation groups, respectively. The large disparity of recruitability between groups was not reflected in the Crs nor the magnitude of mechanical power present after injurious ventilation, once protective ventilation was resumed.
Conclusion
Addition of transitory injurious ventilation after lung lavage causes prolonged acute lung injury with diffuse alveolar damage and low recruitability yielding high titrated PEEP levels. Mimicking lung mechanical and functional characteristics of ARDS, this porcine model rectifies the constraints of single-hit lavage models and may enhance the translation of experimental research on mechanical ventilation strategies.
Similar content being viewed by others
Background
The acute respiratory distress syndrome (ARDS) is a leading cause of mortality in perioperative and critically ill patients [1, 2]. Preclinical research that aims at identifying novel and targeted treatment approaches builds on various different experimental models of lung injury. However, none of these models can reflect all the pathological features and clinical characteristics of ARDS [3,4,5].
For example, pulmonary lavage-induced surfactant depletion is a widely used porcine model of acute hypoxemic lung failure. However, rapid recovery of respiratory system compliance (Crs) and blood oxygenation occur with this model after alveolar recruitment [6,7,8,9], indicating that the gas exchange abnormalities reflect collapsed alveoli with otherwise intact alveolar walls and high recruitability. In contrast, the clinical presentation of ARDS in patients typically includes alveolar injury and non-aerated lung tissue with low Crs and limited recruitability [10]. Recruitability expresses the gain of aerated lung tissue following a recruitment maneuver. In patients and laboratory animals alike, high tidal volumes can lead to the inspiratory re-opening of previously atelectatic alveoli and thereby improve oxygenation. These alveoli may, however, re-collapse at end-expiration if PEEP is below the alveolar closing pressure. Such cyclic recruitment/derecruitment is associated with high shear stress contributing to pulmonary inflammation and ventilator-induced lung injury (VILI), which in turn can aggravate ARDS. Based on these considerations, experimental models of acute lung injury with prompt improvement of Crs and oxygenation following recruitment maneuvers may be of limited translational validity. Several research groups have combined pulmonary lavage-induced surfactant depletion with mechanical ventilation of high tidal volumes and low PEEP to produce a type of lung injury with better similarity to human ARDS [11,12,13]. However, in many studies it is difficult to determine the extent to which the lung injury was caused by the lavage-induced surfactant depletion, the mechanical ventilation, or both.
In this study, we tested the effect of recruitment maneuvers on Crs and oxygenation in a porcine model of lavage-induced surfactant depletion with and without the addition of injurious mechanical ventilation. Decremental PEEP trials were implemented to assess if the PEEP at best Crs versus the PEEP at best oxygenation would differ between the two models. In addition, we implemented a software algorithm into the ventilator for the continuous automatic calculation of the mechanical power (MP) in order to estimate the diagnostic value of MP as an indicator of acute lung injury during protective ventilation.
Methods
This study was approved by the institutional animal welfare officer and the state authority for the care and use of animals (Tierversuchskommission, Landesamt für Gesundheit und Soziales, Berlin, Germany; approval number G 0229/18). Twelve male German Landrace pigs (bodyweight (BW) 46 ± 3 kg, mean ± SD) were housed under enriched standardized environmental conditions (22 °C, 12 h light–dark cycle) in groups of two to five at the animal facility of Charité—Universitätsmedizin Berlin (FEM Forschungseinrichtung für Experimentelle Medizin, Tierhaltung). Animals were fed standard chow (Complete feed for pigs, item nbr. 516040, AGRAVIS Ost GmbH, Germany) and fasted for 12 h with free access to water and hay before each experiment.
Instrumentation
After intramuscular premedication with azaperone (3 mg/kg BW), atropine (0.03 mg/kg BW), ketamine (25 mg/kg BW) and xylazine (3.5 mg/kg BW) at 8:00 AM, a custom-made face mask was fitted on the snout for insufflation of ~ 10 L/min oxygen. A venous cannula (18–20 G, Braunüle®, B. Braun, Germany) was then inserted into an ear vein, a bolus of 500 ml of a balanced crystalloid solution (Sterofundin®, B. Braun, Germany) was administered and followed by continuous infusion of 4 ml/kg/h. Fractional boluses of 100 µg fentanyl were injected (no more than 1000 µg total) to titrate analgesia and sedation. The face mask was connected to the ventilator (EVE®, Fritz Stephan GmbH, Germany, CPAP-ASB mode) to provide assisted spontaneous breathing with PEEP 2 cmH2O, pressure support 5 cmH2O, and flow trigger 2 L/min. Subsequently, animals were placed supine for surgical tracheostomy after local anesthesia with infiltration of at least 10 mL of 2% lidocaine. After insertion of the tracheal cannula (9.0 ID tube; Mallinckrodt™; Covidien Deutschland GmbH, Neustadt, Germany), 5–10 mg/kg BW of propofol were injected. Then, the ventilator was connected to initiate pressure-controlled ventilation with volume guarantee (DUOPAP, EVE®, Fritz Stephan GmbH, Germany) and the following settings: fraction of inspired oxygen (FIO2) 1.0, tidal volume (VT) 9 ml/kg BW, PEEP 7 cmH2O, inspiratory to expiratory time ratio (I:E) 1:2 and respiratory rate (RR) adjusted to achieve an end-expiratory partial pressure of carbon dioxide (PaCO2) of 35–40 mmHg. Anesthesia was maintained with a continuous infusion of thiopentone (20 mg/kg/h) and fentanyl (7 µg/kg/h). Invasive instrumentation was performed as described previously [14]. Briefly, vascular catheters were placed into the femoral artery, and through the external jugular vein into the superior vena cava and the pulmonary artery for continuous monitoring of arterial, central venous and pulmonary artery pressures, and for the quantification of thermodilution cardiac output (Vigilance®, Type VGS1, Baxter, Edwards Lifesciences LLC, Irvine, USA). Finally, a suprapubic urinary catheter (14 Ch Latex Balloon Catheter, Dahlhausen & Co. GmbH, Germany) was established. Hemodynamic and respiratory parameters were recorded continuously using Powerlab™ (Model 8/30) with software LabChart™ 7.3.7 Pro (ADInstruments GmbH, Specbach, Germany).
Protocol
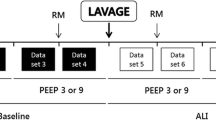
Figure 1 depicts the experimental protocol. A 60 min baseline ventilation period was completed in pressure-controlled mode (DUOPAP) with low VT of 6 ml/kg BW, PEEP 7 cmH2O, I:E 1:2, and RR adjusted to maintain PaCO2 at 37–45 mmHg. Next, surfactant-depletion was induced by a pulmonary lavage procedure (see below). Animals were then randomized (bag of lots) to undergo a 3 h period (ventilation phase 1) of either protective or injurious ventilation (N = 6 per group). Protective ventilation consisted of a low VT (6 ml/kg) and tabular PEEP strategy following the rules of the ARDSNet (NIH NHLBI ARDS Network) protocol [15, 16]. To this end, an automated closed-loop mechanical ventilation algorithm adherent to the ARDSNet protocol was developed and used in this study to apply protective ventilation. Injurious ventilation consisted of a non-automated high VT (17 ml/kg), low PEEP (2 cmH2O) strategy with RR of 12/min to prevent hypocapnia. These high tidal volumes produced a peak inspiratory pressure (PIP) of around 50 cmH2O, which corresponds to the upper pressure limit that was applied during the alveolar recruitment maneuvers in both groups (see below). The 3 h period of either protective or injurious ventilation was followed by additional 3 h of automated protective closed-loop ventilation (ventilation phase 2).
Recruitment maneuvers (RM) were performed at three instances during the course of the protocol: (i) after pulmonary lavage (RM1); (ii) after initial 3 h of protective vs. injurious ventilation (RM2); (iii) after final 3 h of protective ventilation (RM3). Pulmonary gas exchange function, respiratory mechanics, and ventilator-derived parameters were assessed after each RM to map the course of injury severity and pulmonary recruitability. Each RM was followed by a decremental PEEP trial to identify the PEEP associated with either the maximum Crs or the maximum oxygenation (“best PEEP”). A cardioplegic bolus of potassium chloride was used to kill animals in deep anesthesia (bolus: 500 µg of fentanyl, 1000 mg thiopentone) at the end of the protocol. Lung tissue sample underwent histopathological assessment for signs of lung injury.
Pulmonary lavage procedure
Lavage-induced surfactant depletion was performed to induce acute lung injury (ALI) in all animals as described in detail elsewhere [9, 14]. Briefly, after neuromuscular blockade with pancuronium bromide (0.15 mg/kg BW i.v. bolus), repetitive lavages were performed using warm 0.9% saline until PaO2 at FIO2 1.0 and PEEP 6 cmH2O was below 100 mmHg for 10 min.
Alveolar recruitment maneuver and decremental PEEP trial
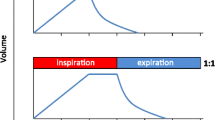
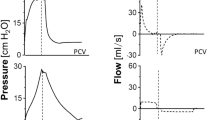
A pressure-controlled ventilator mode was used for the recruitment maneuver and PEEP trial. First, a PEEP of 12 cmH2O was applied. The RR was then set to 20/min and ΔP (PIP − PEEP) to 20cmH2O. PEEP was then increased in steps of 2–4 cmH2O every 5 breaths until 24 cmH2O was reached. Then, ΔP was increased to apply a peak inspiratory pressure of 50 cmH2O at PEEP 24 cmH2O for 5 respiratory cycles. Immediately thereafter, PEEP 15 cmH2O and VT 6 ml/kg BW were applied for 5 min, to allow the assessment of pulmonary function parameters (blood gas analysis), respiratory mechanics (dynamic Crs and MP, and hemodynamics including cardiac output under standardized conditions. Next, for the purpose of equal volume history, the lungs were ventilated with VT 10 ml/kg, PEEP 0 cmH2O, RR 10/min, I:E 1:1 for 10 respiratory cycles, followed by a brief disconnection from the ventilator (5 s). Then, a decremental PEEP titration was performed to identify the maximum PaO2 and maximum dynamic Crs under these conditions: while keeping a constant ΔP of 14 cmH2O and RR of 20/min, PEEP was set at 12 cmH2O and was then increased to 24 cmH2O in steps of 4 cmH2O per every 5 respiratory cycles. A stepwise reduction of PEEP by 2 cmH2O, again with a constant ΔP of 14 cmH2O, was performed at intervals of 10 min. The titration was stopped when a minimum PEEP of 6 cmH2O or a PaO2/FIO2 ratio of less than 80 mmHg was reached. All measurements were performed at the end of each step.
Automated closed-loop mechanical ventilation system
We designed an automated closed-loop mechanical ventilation algorithm and ventilator system to apply protective ventilation adherent to the ARDSNet protocol [7, 8, 15]. Here, all components of the software, actuators and devices of the closed-loop physiological feedback algorithm were integrated into a mechanical ventilator system (EVE®, Fritz Stephan GmbH, Germany). The system outputs were designed to automatically adjust VT, PEEP, RR, I:E and FIO2 independently. System inputs were derived from an integrated capnograph and pulse oximeter for the continuous measurement of exhaled CO2 concentration and peripheral oxyhemoglobin saturation (SpO2), respectively. Briefly, an SpO2 target of 88–95% and the “higher PEEP/lower FIO2” table were used to adjust FIO2 and PEEP [16]. VT of 6 ml/kg BW was delivered in a pressure-controlled mode (DUOPAP) with decelerating gas flow, and was automatically reduced to 5 or 4 ml/kg BW when PIP exceeded 30 cmH2O. The system received manual input of arterial pH (pHa) once every 30 min. At pHa < 7.30 or > 7.45, the closed-loop system repetitively adjusted RR in steps of ± 5 /min, respectively. Maximum RR was limited at 35 /min.
Calculation of the mechanical power
Gattinoni et al. proposed MP as a unified variable to encapsulate all ventilator-related causes of lung injury [17]. The original equation described by Gattinoni et al. is, however, only applicable to volume-controlled ventilation with constant inspiratory flow. Since this study used a ventilation mode with decelerating flow, the simplified equation for MP proposed by Becher et al. for pressure-controlled ventilation was used:
This simple equation was shown to correlate well with the true MP and to be acceptable for clinical purpose [18]. The other equations for MP calculation during pressure-controlled ventilation proposed by Becher et al. and Van der Meijden et al. are computationally more costly, with only a small improvement in fit [18, 19].
Statistical analysis
For statistical computing, we used R version 4.0.3 (http://R-project.org) and GraphPad Prism software (GraphPad Software, Version 9.0.2, La Jolla, CA). All values are presented as means ± standard deviation (SD). Due to the rather small sample sizes, we used nonparametric ranking methods for making inference. Continuous variables of the two independent groups at discrete time points (e.g., after lavage or RM 1–3; in Figs. 2, 3, and 4) were compared using Mann–Whitney U test. Nonparametric longitudinal data analysis was performed with a two-way ANOVA-type statistic implemented in the Nonparametric Analysis for Longitudinal Data (nparLD) package [20]. The inter-group (group effect) and intra-group variables (time effect) were analyzed to identify main and interaction effects on the outcome parameters shown in all Table and Fig. 5. The associated treatment effect is the so-called relative treatment effect (RTE) which is the proportion of data from the entire data set being smaller (or equal) than the values in a subgroup or at an individual time point. Interpretation of RTEs is explained in more detail in Additional file 1: Table S1. Missing values in group B (lavage-induced surfactant depletion followed by injurious HVT ventilation) during PEEP trials 2 and 3 are caused by the termination criterion (PaO2 < 80 mmHg). Consequently, the PEEP trials were excluded from the inferential longitudinal analysis. A two-tailed p-value < 0.05 was considered statistically significant. A series of sample size calculations (power 0.8, α = 0.05) based on different outcome parameters with variance estimated or known from previous experiments, suggested a group size between 6 and 10. Due to the ability to detect significant differences in the level of injury at interim analysis, we concluded experimentation after n = 6 per group.
Results
Effects of lavage-induced surfactant depletion
The pulmonary lavage procedure consistently produced severe hypoxemia and hypercapnia (both PaO2 and PaCO2 around 80 mmHg at FIO2 1.0, VT 6 ml/kg BW, PEEP 6 cmH2O), lower Crs, higher PIP, ΔP and mean pulmonary artery pressure (mPAP) compared to baseline, reflecting acute lung injury in both groups (Table 1, Fig. 2). A subsequent recruitment maneuver (RM1) ending with a VT 6 ml/kg BW and PEEP 15 cmH2O, restored PaO2, Crs and ΔP to a large extent (Table 1, Fig. 2).

Experimental protocol. Anesthetized pigs underwent lavage-induced surfactant depletion followed by either low (LVT; N = 6) or high (HVT; N = 6) tidal volume ventilation during ventilation phase 1 (3 h). LVT ventilation was resumed in ventilation phase 2 (3 h) in both groups. Recruitment maneuvers (RM) and PEEP trials were performed at three instances throughout the protocol to assess injury, recruitability, and “best PEEP”. For more details see “Methods” Section in the main text

Respiratory mechanics and function. Dynamic compliance of the respiratory system (Crs) and arterial partial pressure of oxygenation (PaO2) were assessed in anesthetized pigs at baseline, after lavage-induced surfactant depletion, and after consecutive recruitment maneuvers (RM) at 3 h intervals. Group A, N = 6: continuous automated protective low tidal volume ventilation (LVT). Group B, N = 6: 3 h of injurious high tidal volume ventilation (HVT) prior to RM 2, resumption of protective low tidal volume ventilation for 3 h prior to RM 3. Two animals died after injurious HVT and RM 2, i.e., Group B, N = 4 at RM 3. For experimental protocol, see Fig. 1. Scatter plots with horizontal (means) and error bars (SD). **p < 0.01, Mann–Whitney U test

Ventilation-induced deviation from lavage-induced impairment of respiratory mechanics and function. Dynamic compliance of the respiratory system (Crs) and arterial partial pressure of oxygenation (PaO2) were assessed in anesthetized pigs after lavage-induced surfactant depletion, and after consecutive recruitment maneuvers (RM) at 3 h intervals. Figure depicts the relative deviation of Crs and PaO2 (obtained after RM) from the respective values after initial lavage. Group A, N = 6: continuous automated protective low tidal volume ventilation (LVT). Group B, N = 6: 3 h of injurious high tidal volume ventilation (HVT) prior to RM 2, resumption of protective low tidal volume ventilation for 3 h prior to RM 3. Two animals died after injurious HVT and RM 2, i.e., Group B, N = 4 at RM 3. For experimental protocol, see Fig. 1. Scatter/bar plots with horizontal (means) and error bars (SD). **p < 0.01, Mann–Whitney U test

Decremental PEEP trials: identification of “best PEEP”. PEEP trials with decrements of 2 from 24 to 6 cmH2O were performed at three instances following a recruitment maneuver (RM) in anesthetized pigs which had undergone combined lavage-induced surfactant depletion and therapeutic ventilation. Group A, N = 6: continuous automated protective low tidal volume ventilation (LVT). Group B, N = 6: 3 h of injurious high tidal volume ventilation (HVT) prior to PEEP trial 2, resumption of protective low tidal volume ventilation for 3 h prior to PEEP trial 3. Two animals died after injurious HVT and RM 2, i.e., Group B, N = 4 at PEEP trial 2 and 3. For experimental protocol, see Fig. 1 and “Methods” Section. Line graphs depict the group means of Crs and PaO2 obtained at each PEEP level. PEEP values at the maximum mean Crs and maximum mean PaO2 (red vertical dotted lines) are consistently disparate within each group and differ between groups. Adjacent scatter plots depict the PEEP values at maximum Crs and PaO2 of each individual animal and the means ± SD thereof. *p < 0.05, **p < 0.01, Mann–Whitney U test

Tidal volume and mechanical power in combined lavage and ventilator-induced lung injury. Tidal volume (VT) and mechanical power (MP) of ventilation were assessed in anesthetized and surfactant-depleted pigs which underwent either an automated closed-loop protective low tidal volume (6 ml/kg BW LVT) and tabular PEEP ventilation strategy (group A) or non-automated injurious high tidal volume ventilation (HVT) with VT of 17 ml/kg BW and PEEP 2 cmH2O (group B) during ventilation phase 1. Ventilation phase 2 consisted of automated LVT ventilation in both groups (N = 6 each). Two animals died after injurious HVT and RM 2, i.e., Group B, N = 4 during ventilation phase 2. For experimental protocol, see Fig. 1 and “Methods” Section. For calculation of the MP, the simplified equation proposed by Becher et al. for pressure-controlled ventilation is used (see “Methods” Section in the main text). Means ± SD; p-values indicate significant group effects and were calculated using two-way ANOVA-type nparLD package (see Table 2, associated relative treatment effects (RTE) see Additional file 1: Table S2a). For more statistical details refer to main text
Lung injury severity and recruitability after protective versus injurious ventilation
Subsequent to lavage and RM1, longitudinal analysis of pulmonary function and ventilator-derived parameters revealed significant group and time effects (Table 2): 3 h of protective vs. injurious ventilation (ventilation phase 1) with ΔP of 17 ± 3 vs. 49 ± 8 cmH2O, PEEP 11 ± 3 vs. 2 ± 0.5 cmH2O, PIP of 28 ± 5 vs. 51 ± 9 cmH2O, and MP of 28 ± 11 vs. 47 ± 10 J/min, resulted in Crs (20.8 ± 7.1 vs. 18.8 ± 3.3 ml/cmH2O) and PaO2/FIO2 (104 ± 26 vs. 154 ± 123 mmHg) of similar magnitude (Table 2). Following additional 3 h of protective ventilation (ventilation phase 2) with tabular PEEP of 11 ± 5 vs. 17 ± 3 cmH2O, ΔP was 15 ± 4 vs. 19 ± 3 cmH2O, PIP 26 ± 4 vs. 35 ± 4 cmH2O, and MP 24.7 ± 5.6 vs. 35.3 ± 3.0 J/min. Again, Crs (23.7 ± 7.1 vs. 21.5 ± 4.2 ml/cmH2O) and PaO2/FIO2 (120 ± 15 vs. 128 ± 37 mmHg) were similar in both groups that had previously received either protective or injurious ventilation, respectively (Table 2). Longitudinal analysis of injury severity was extended to the assessment of pulmonary compliance and oxygenation after RMs (Table 1, Figs. 2 and 3). In the group receiving pulmonary lavage followed by protective ventilation, RM 2 and 3 revealed instantaneous recruitability with complete restoration of Crs and normalization of PaO2/FIO2 ratios (> 300 mmHg), but persistence of hypercapnia. In contrast, in the group that had received pulmonary lavage and injurious ventilation, RM 2 and 3 failed to restore Crs and PaO2, leaving pulmonary function significantly impaired. Figure 3 depicts the relative deviation of Crs and PaO2 (obtained after RM) from the respective values after initial lavage: a progressive gain in compliance and oxygenation can be observed along the time course in the protective ventilation group.
This model of lavage-induced surfactant depletion and injurious ventilation caused significant histopathological damage (Fig. 6) and CT abnormalities (Fig. 7) typical of ARDS.

Histopathology. Representative tissue sections stained with hematoxylin/eosin of the right lower lung lobe of pigs after lavage-induced surfactant depletion and subsequent protective A, B or injurious C, D mechanical ventilation. High magnification fields (B, D, × 400) correspond to red box on low magnification field (A, C, × 100). Note the condensed histoarchitecture and signs of diffuse alveolar damage present after lavage and injurious ventilation (C, D), including septal thickening (*), massive interstitial ( →) and intra-alveolar ( >) infiltration of neutrophils, intra-alveolar erythrocytes (∆), protein strands (#), and disruption of the alveolar integrity ( +). In contrast, more aerated surface area with preserved alveolar architecture ( +), identification of type I pneumocytes (»), and less alveolar damage is present after lavage and protective ventilation (A, B). Septal thickening, neutrophil infiltration, and intra-alveolar protein strands occurred to a much lower extent

Computed tomography. Representative computed tomography (CT) images of the basal lungs segments of a pig following lavage-induced surfactant depletion and 3 h of injurious ventilation. Images were taken during ventilation with PEEP of 15 vs. 6 mbar and a VT of 6 mL/kg body weight. Ground glass opacities ( >), interlobar and intralobular septal thickening (→) are representative of the severity of lung injury. Note the significant increase of atelectatic regions (*) as a sign of derecruitment in the dependent lung areas upon PEEP reduction
Identification of maximum Crs and oxygenation
Decremental PEEP trials revealed (i) that the PEEP levels producing either maximum Crs or maximum PaO2 were consistently disparate within each group; (ii) that these “best PEEP” levels were different between the two groups, and (iii) that the inter-group difference of “best oxygenation PEEP” increased progressively over time (Fig. 4, Additional file 1: Table S3–S5): in the group receiving lavage and protective ventilation, PEEP was 16, 14, and 16 cmH2O to achieve maximum PaO2 of 514 ± 49, 508 ± 90, and 563 ± 83 mmHg, respectively, after PEEP trials 1, 2 and 3. At the same time, “best PEEP” to achieve maximum Crs of 26.0 ± 3.4, 29.7 ± 8.0, and 35.5 ± 10.3 ml/cmH2O was 12 cmH2O, consistently, after all three PEEP trials. In the group receiving lavage and injurious ventilation, PEEP was 20, 18, and 22 cmH2O to achieve maximum PaO2 of 467 ± 55, 346 ± 62, and 334 ± 148 mmHg, respectively, after PEEP trials 1, 2 and 3. At the same time, “best PEEP” to achieve maximum Crs of 24.3 ± 6.2, 28.7 ± 4.7, and 24.8 ± 5.3 ml/cmH2O was 16 cmH2O, consistently, after all three PEEP trials.
Invasiveness of ventilation and mechanical power (M P) calculation
Figure 5 depicts the different levels of VT and MP applied during protective versus injurious ventilation, caused by different settings of VT (Fig. 5), PEEP and RR (Table 2), according to the protocol. Automatic adjustment of these settings occurred during automated protective closed-loop ventilation. Note that after resumption of automated protective ventilation during the final 3 h (ventilation phase 2), PEEP (Table 2) and MP (Fig. 5) remain higher in the group coming off injurious ventilation as compared to the group having received protective ventilation only. However, no such difference is reflected in the MP, when calculated immediately after RM 2 and 3 at arbitrary standard conditions of PEEP 15 cmH2O and VT 6 ml/kg BW (Table 1).
Hemodynamics
Mean PAP (mPAP), pulmonary vascular resistance (PVR) and cardiac output (CO) were comparable at baseline. All of these parameters increased after lavage and RM (Table 1). Consistently, a significant group effect was found over the course of the PVR during protective and injurious ventilation periods and after RMs (Tables 1 and 2), resulting in higher values in the injurious as compared to the protective ventilation group.
Two animals died of hypoxemia and cardio-circulatory decompensation during the PEEP trial following RM 2 in the injurious ventilation group.
Discussion
Summary statement
Models of acute lung injury induced by pulmonary lavages are constrained by their short-lived and incomplete imitation of the pulmonary function characteristics of ARDS, because of the ease of re-opening surfactant-depleted alveoli through application of high peak and positive end-expiratory pressures, which then cause prompt improvements in arterial oxygenation. We found that transitory injurious high tidal–low PEEP ventilation of surfactant-depleted lungs produces a type of sustained lung injury characterized by low recruitability, high levels of titrated PEEP, and oxygenation impairment consistent with mild-to-moderate ARDS during protective ventilation. This model rectifies the constraints of single-hit models employing either only high VT ventilation or only surfactant-depletion and provides a more realistic means to study the clinical effect of protective ventilation strategies, and can be used to verify the functionality of automated protective closed-loop ventilation.
Methodological considerations
Recently, significant advances have been made in the engineering of automated physiological closed-loop control systems of mechanical ventilation [21]. These systems shall ensure optimal gas exchange and prevention of VILI. In this context, investigators must pay special attention to choosing the model best suited to test the clinical performance of these systems [22]. The clinical relevance of simple VILI models, in which mechanical ventilation is the sole method used to generate injury, is sometimes questioned as these models typically require very high VT (up to 30–40 ml/kg BW which is beyond clinical practice) before the shear stresses are high enough to cause injury of an otherwise healthy lung [23, 24]. Lung overinflation as a result of high VT, can cause significant changes in the composition and function of surfactant, as surfactant is squeezed out of the alveolus, which in turn contributes to alveolar instability, cyclic opening and closing, and concomitant inflammation [25]. In contrast, in an injured lung, where the synthesis, distribution and function of surfactant are already impaired, such as after lavage, acid aspiration or secondary to pneumonia and ARDS, injurious shear stress due to overstretching and atelectrauma can occur at much lower VT. Therefore, the intention of this investigation was to characterize a model which combines pulmonary lavage with injurious ventilation to induce a type of lung injury that includes the pathophysiological features of both surfactant depletion or dysfunction, and mechanical stress and strain from ventilation. This model should emulate the clinical situation of patients with ARDS. Importantly, after induction of injury the model was evaluated during standard protective ventilation conditions, in this case with automated closed-loop ventilation. Since this model was destined for the testing of automated protective ventilation strategies, the evaluation of the model was focused around (I) the recruitability of the injured lung; (II) the identification of the PEEP levels producing either the maximum PaO2 or the maximum Crs (“best PEEP”) and III) the MP resulting from automated protective ventilation under these conditions:
Recruitability
Recruitment of atelectatic lung regions and mechanical ventilation with a PEEP level targeting the prevention of end-expiratory alveolar collapse to abrogate the high shear forces present during cyclic recruitment/decruitment of alveoli, is a pathophysiologically sound “open lung” concept [26]. However, it is important to note that evidence from large clinical trials shows that the routine use of higher PEEP and/or RMs did not reduce mortality in unselected patients with ARDS [27, 28]. In particular, pulmonary recruitability with prompt and large improvements of gas exchange is not a characteristic of the majority of patients with ARDS [10]. In line with these findings, our model of combined lavage and injurious ventilation generated limited recruitability and long-lasting impairment of gas exchange and therefore emulates the pulmonary function characteristics of ARDS better than lavage or VILI alone. Moreover, compared to pulmonary lavage alone, addition of injurious ventilation was associated with higher PVR and higher ∆P during and beyond the injurious ventilation phase (Table 2). This difference persisted after RMs 2 and 3, and was associated with higher pulmonary artery pressures and greater hypercapnia than in the group with pulmonary lavage and protective ventilation (Table 1). Therefore, beyond the limited recruitability and sustained hypoxemia, our model also emulates the clinical characteristics of hypercapnic lung failure with pulmonary hypertension, which both have distinct biological and physiological effects in ARDS [29]. In addition, our data show that the impairment of oxygenation and pulmonary compliance, induced by pulmonary lavage alone, progressively faded while the animals received automated protective ventilation with low VT and tabular PEEP (ARDSNet strategy): after 6 h of protective ventilation a PaO2/FIO2 ratio of 445±144 mmHg at PEEP 6 cmH2O no longer indicated the presence of ALI or ARDS in this group. Consequently, simple models of lavage-induced surfactant depletion may tend to overestimate the therapeutic effects of recruitment maneuvers and lung-protective ventilation strategies, and therefore are not ideal to evaluate the functionality of automated closed-loop and other protective ventilation strategies.
PEEP titration
Application of PEEP is currently the primary strategy to minimize dynamic strain caused by alveolar recruitment/derecruitment in mechanically ventilated patients with ARDS. Multiple methods have been tested and been reviewed elsewhere [30]. The concept of “best PEEP” was coined by Suter et al. and defined as the level of maximum oxygen delivery (DO2) in patients with ARDS [31]. They found that the individual “best PEEP (DO2)” was associated with the maximal respiratory system compliance. This is in contrast to our data, where maximal DO2 (Additional file 1: Tables S3–S5) was not associated with PEEP values at the maximum of Crs (Fig. 4). Of importance, Suter et al. performed incremental PEEP trials, whereas, in the present model, we performed decremental PEEP trials. Due to potential impairment of venous return and compression of small alveolar vessels, PEEP can affect DO2 as much as it affects cardiac output and right ventricular stroke volume [32, 33]. Likewise, when PEEP is reduced, such as in a decremental PEEP trial, cardiac output will increase due to enhanced venous return and reduced alveolar vascular compression. In line with these pathophysiological considerations, we observed cardiac output increasing and PVR decreasing during the decremental PEEP trials in our model. Finally, our data confirm that the PEEP levels required for maximum PaO2 are consistently higher than the PEEP required to reach maximum Crs, which is a characteristic feature of ARDS in patients [31]. In our model, the difference between the two “best PEEP” levels of maximum PaO2 vs. Crs after pulmonary lavage (Δ = 4 cmH2O in PEEP trial 1) was most pronounced after high VT ventilation had induced additional injury, and protective ventilation had been resumed (Δ = 6 cmH2O in PEEP trial 3). The general concept and provision for these disparate PEEP levels is of high relevance in the clinical setting: while low VT is almost consistently associated with lower PaO2 than more invasive ventilation strategies [15], the target of maximizing oxygenation through high PEEP, categorical recruitment maneuvers, and higher VT can result in excessive mortality [27, 28].
Mechanical power
Recently, VILI has been related to the mechanical power (MP) of ventilation [34]. MP represents the amount of energy per unit of time transferred from the ventilator to the respiratory system and lung tissue [17, 35]. MP and can be calculated as the product of the respiratory rate, VT and the sum of PEEP and ΔP [18]. In patients receiving invasive ventilation, high MP of ventilation is independently associated with higher in-hospital mortality and several other outcomes [36,37,38]. In our model, injurious ventilation following pulmonary lavage exposed the lungs to higher MP than protective ventilation, and this is mainly caused by the higher magnitude of the VT. Of note, once protective ventilation was resumed, and therefore VT was ~ 6 ml/kg BW in both groups, MP remained higher in the group that had previously received lavage and injurious ventilation as compared to the group with lavage and protective ventilation (Fig. 5). The higher MP reflects the extent of lung injury caused by injurious ventilation, and can be attributed to the higher peak, end-expiratory and driving pressures that ensued when the automated protective ventilation algorithm (adherent to the rules of the ARDSNet protective ventilation strategy) was applied subsequent to injurious ventilation (Table 2). Only after a RM at 3 h after the resumption of protective ventilation and when lung mechanics were assessed under arbitrary uniform ventilation conditions (VT 6 ml/kg BW, PEEP 15 cmH2O), MP reached a comparable level in both groups (Table 1). While these findings challenge the notion that MP may reflect injury severity, they support that high MP can be reflective of injurious ventilation. However, to estimate the clinical relevance of MP, i.e., the “intensity” of mechanical ventilation—which is outside the aims and scope of the present model—it should be normalized to the size of the ventilated pulmonary surface area [34]. Taking into account that MP reflects the synergy of various different ventilator parameters which may predispose to lung injury associated with mechanical ventilation, further studies are needed to clarify how MP should guide the choice of ventilator settings.
Limitations
Since the primary focus of our work was to evaluate the pulmonary function characteristics of the model, and its applicability to serve as a test model for automated protective ventilation strategies, edema formation and biomarkers of inflammation were not evaluated. In addition, since decremental PEEP trials were performed at constant ΔP, we cannot exclude that fluctuations of VT had an impact on the assessment of Crs and oxygenation. Finally, when interpreting pulmonary artery pressure, PVR, and cardiac output obtained during PEEP trials, it must be taken into account that significant hypercapnia occurred at high PEEP levels (Additional file 1: Table S3–S5).
Conclusion
In summary, we demonstrate that addition of transitory injurious ventilation to surfactant-depleted lungs and subsequent resumption of protective ventilation causes prolonged acute lung injury with low recruitability yielding high titrated PEEP levels. Mimicking the characteristics of lung function and oxygenation impairment of mild-to-moderate ARDS, this porcine model rectifies the constraints of simpler models and provides a more realistic means that may facilitate the translation of experimental research on mechanical ventilation strategies, including closed-loop automated protective ventilation systems. Such systems help advance the evolution of sophisticated personalized protective ventilation strategies in the future.
Availability of data and materials
The datasets used and/or analyzed during the current study are included within the article are available from the corresponding author on reasonable request.
Abbreviations
- ALI::
-
Acute lung injury
- ARDS::
-
Acute respiratory distress syndrome
- ARDSNet::
-
Acute Respiratory Distress Syndrome Network
- BW::
-
Body weight
- Crs::
-
Dynamic compliance of the respiratory system
- CO::
-
Cardiac output
- DO2::
-
Delivery of oxygen
- ΔP::
-
Pressure difference, the “delta pressure” = driving pressure = PIP − PEEP
- FIO2::
-
Fraction of inspired oxygen
- HVT::
-
High tidal volume
- I:E::
-
Inspiratory-to-expiratory time ratio
- LVT::
-
Low tidal volume
- MP::
-
Mechanical power
- mPAP::
-
Mean pulmonary artery pressure
- PaO2::
-
Arterial partial pressure of oxygen
- PaCO2::
-
Arterial partial pressure of carbon dioxide
- PEEP::
-
Positive end-expiratory pressure
- PIP::
-
Peak inspiratory pressure
- PVR:
-
Pulmonary vascular resistance
- pHa::
-
Arterial pH
- RM::
-
Recruitment maneuver
- RR::
-
Respiratory rate
- SpO2 :
-
Peripheral oxyhemoglobin saturation
- V-V ECMO::
-
Veno-venous extracorporeal membrane oxygenation
- VILI::
-
Ventilator-induced lung injury
- VT::
-
Tidal volume
References
Williams GW, Berg NK, Reskallah A, Yuan X, Eltzschig HK (2021) Acute respiratory distress syndrome. Anesthesiology 134(2):270–282. https://doi.org/10.1097/ALN.0000000000003571
Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A, Investigators LS, Group ET (2016) Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 315(8):788–800. https://doi.org/10.1001/jama.2016.0291
Matute-Bello G, Downey G, Moore BB, Groshong SD, Matthay MA, Slutsky AS, Kuebler WM, Acute Lung Injury in Animals Study G (2011) An official American Thoracic Society workshop report: features and measurements of experimental acute lung injury in animals. Am J Respir Cell Mol Biol 44(5):725–738. https://doi.org/10.1165/rcmb.2009-0210ST
Tonelli AR, Zein J, Adams J, Ioannidis JP (2014) Effects of interventions on survival in acute respiratory distress syndrome: an umbrella review of 159 published randomized trials and 29 meta-analyses. Intensive Care Med 40(6):769–787. https://doi.org/10.1007/s00134-014-3272-1
Slutsky AS, Villar J, Pesenti A (2016) Happy 50th birthday ARDS! Intensive Care Med 42(5):637–639. https://doi.org/10.1007/s00134-016-4284-9
Russ M, Kronfeldt S, Boemke W, Busch T, Francis RC, Pickerodt PA (2016) Lavage-induced surfactant depletion in pigs as a model of the acute respiratory distress syndrome (ARDS). J Vis Exp. https://doi.org/10.3791/53610
Pomprapa A, Schwaiberger D, Pickerodt P, Tjarks O, Lachmann B, Leonhardt S (2014) Automatic protective ventilation using the ARDSNet protocol with the additional monitoring of electrical impedance tomography. Crit Care 18(3):R128. https://doi.org/10.1186/cc13937
Schwaiberger D, Pickerodt PA, Pomprapa A, Tjarks O, Kork F, Boemke W, Francis RCE, Leonhardt S, Lachmann B (2018) Closed-loop mechanical ventilation for lung injury: a novel physiological-feedback mode following the principles of the open lung concept. J Clin Monit Comput 32(3):493–502. https://doi.org/10.1007/s10877-017-0040-0
Lachmann B, Robertson B, Vogel J (1980) In vivo lung lavage as an experimental model of the respiratory distress syndrome. Acta Anaesthesiol Scand 24(3):231–236. https://doi.org/10.1111/j.1399-6576.1980.tb01541.x
Gattinoni L, Caironi P, Cressoni M, Chiumello D, Ranieri VM, Quintel M, Russo S, Patroniti N, Cornejo R, Bugedo G (2006) Lung recruitment in patients with the acute respiratory distress syndrome. N Engl J Med 354(17):1775–1786. https://doi.org/10.1056/NEJMoa052052
Matute-Bello G, Frevert CW, Martin TR (2008) Animal models of acute lung injury. Am J Physiol Lung Cell Mol Physiol 295(3):L379-399. https://doi.org/10.1152/ajplung.00010.2008
Broche L, Perchiazzi G, Porra L, Tannoia A, Pellegrini M, Derosa S, Sindaco A, Batista Borges J, Degrugilliers L, Larsson A, Hedenstierna G, Wexler AS, Bravin A, Verbanck S, Smith BJ, Bates JH, Bayat S (2017) Dynamic mechanical interactions between neighboring airspaces determine cyclic opening and closure in injured lung. Crit Care Med 45(4):687–694. https://doi.org/10.1097/CCM.0000000000002234
Borges JB, Costa EL, Suarez-Sipmann F, Widstrom C, Larsson A, Amato M, Hedenstierna G (2014) Early inflammation mainly affects normally and poorly aerated lung in experimental ventilator-induced lung injury*. Crit Care Med 42(4):e279-287. https://doi.org/10.1097/CCM.0000000000000161
Russ M, Boerger E, von Platen P, Francis RCE, Taher M, Boemke W, Lachmann B, Leonhardt S, Pickerodt PA (2021) Surfactant depletion combined with injurious ventilation results in a reproducible model of the acute respiratory distress syndrome (ARDS). J Vis Exp. https://doi.org/10.3791/62327
Syndrome ARD, N, Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A, (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 342(18):1301–1308. https://doi.org/10.1056/NEJM200005043421801
Brower RG, Lanken PN, MacIntyre N, Matthay MA, Morris A, Ancukiewicz M, Schoenfeld D, Thompson BT, National Heart L, Blood Institute ACTN (2004) Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 351(4):327–336. https://doi.org/10.1056/NEJMoa032193
Gattinoni L, Tonetti T, Cressoni M, Cadringher P, Herrmann P, Moerer O, Protti A, Gotti M, Chiurazzi C, Carlesso E, Chiumello D, Quintel M (2016) Ventilator-related causes of lung injury: the mechanical power. Intensive Care Med 42(10):1567–1575. https://doi.org/10.1007/s00134-016-4505-2
Becher T, van der Staay M, Schadler D, Frerichs I, Weiler N (2019) Calculation of mechanical power for pressure-controlled ventilation. Intensive Care Med 45(9):1321–1323. https://doi.org/10.1007/s00134-019-05636-8
van der Meijden S, Molenaar M, Somhorst P, Schoe A (2019) Calculating mechanical power for pressure-controlled ventilation. Intensive Care Med 45(10):1495–1497. https://doi.org/10.1007/s00134-019-05698-8
Noguchi K, Gel YR, Brunner E, Konietschke F (2012) nparLD: an R software package for the nonparametric analysis of longitudinal data in factorial experiments. J Stat Softw 50(12):1–23. https://doi.org/10.18637/jss.v050.i12
Platen PV, Pomprapa A, Lachmann B, Leonhardt S (2020) The dawn of physiological closed-loop ventilation-a review. Crit Care 24(1):121. https://doi.org/10.1186/s13054-020-2810-1
Bastarache JA, Blackwell TS (2009) Development of animal models for the acute respiratory distress syndrome. Dis Model Mech 2(5–6):218–223. https://doi.org/10.1242/dmm.001677
Veskemaa L, Graw JA, Pickerodt PA, Taher M, Boemke W, Gonzalez-Lopez A, Francis RCE (2021) Tert-butylhydroquinone augments Nrf2-dependent resilience against oxidative stress and improves survival of ventilator-induced lung injury in mice. Am J Physiol Lung Cell Mol Physiol 320(1):L17–L28. https://doi.org/10.1152/ajplung.00131.2020
Francis RC, Vaporidi K, Bloch KD, Ichinose F, Zapol WM (2011) Protective and detrimental effects of sodium sulfide and hydrogen sulfide in murine ventilator-induced lung injury. Anesthesiology 115(5):1012–1021. https://doi.org/10.1097/ALN.0b013e31823306cf
Verbrugge SJ, Bohm SH, Gommers D, Zimmerman LJ, Lachmann B (1998) Surfactant impairment after mechanical ventilation with large alveolar surface area changes and effects of positive end-expiratory pressure. Br J Anaesth 80(3):360–364. https://doi.org/10.1093/bja/80.3.360
Lachmann B (1992) Open up the lung and keep the lung open. Intensive Care Med 18(6):319–321. https://doi.org/10.1007/BF01694358
Ball L, Serpa Neto A, Trifiletti V, Mandelli M, Firpo I, Robba C, Gama de Abreu M, Schultz MJ, Patroniti N, Rocco PRM, Pelosi P, Network PNPV (2020) Effects of higher PEEP and recruitment manoeuvres on mortality in patients with ARDS: a systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials. Intensive Care Med Exp 8(Suppl 1):39. https://doi.org/10.1186/s40635-020-00322-2
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial I, Cavalcanti AB, Suzumura EA, Laranjeira LN, Paisani DM, Damiani LP, Guimaraes HP, Romano ER, Regenga MM, Taniguchi LNT, Teixeira C, Pinheiro de Oliveira R, Machado FR, Diaz-Quijano FA, Filho MSA, Maia IS, Caser EB, Filho WO, Borges MC, Martins PA, Matsui M, Ospina-Tascon GA, Giancursi TS, Giraldo-Ramirez ND, Vieira SRR, Assef M, Hasan MS, Szczeklik W, Rios F, Amato MBP, Berwanger O, Ribeiro de Carvalho CR (2017) Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) vs low PEEP on mortality in patients with acute respiratory distress syndrome: a randomized clinical trial. JAMA 318(14):1335–1345. https://doi.org/10.1001/jama.2017.14171
Morales-Quinteros L, Camprubi-Rimblas M, Bringue J, Bos LD, Schultz MJ, Artigas A (2019) The role of hypercapnia in acute respiratory failure. Intensive Care Med Exp 7(Suppl 1):39. https://doi.org/10.1186/s40635-019-0239-0
Nieman GF, Satalin J, Andrews P, Aiash H, Habashi NM, Gatto LA (2017) Personalizing mechanical ventilation according to physiologic parameters to stabilize alveoli and minimize ventilator induced lung injury (VILI). Intensive Care Med Exp 5(1):8. https://doi.org/10.1186/s40635-017-0121-x
Suter PM, Fairley B, Isenberg MD (1975) Optimum end-expiratory airway pressure in patients with acute pulmonary failure. N Engl J Med 292(6):284–289. https://doi.org/10.1056/NEJM197502062920604
Feihl F, Broccard AF (2009) Interactions between respiration and systemic hemodynamics. Part I: basic concepts. Intensive Care Med 35(1):45–54. https://doi.org/10.1007/s00134-008-1297-z
West JB (1985) Respiratory physiology—the essentials, 3rd edn. Wiliam & Wilkins, Baltimore
Silva PL, Ball L, Rocco PRM, Pelosi P (2019) Power to mechanical power to minimize ventilator-induced lung injury? Intensive Care Med Exp 7(Suppl 1):38. https://doi.org/10.1186/s40635-019-0243-4
Cressoni M, Gotti M, Chiurazzi C, Massari D, Algieri I, Amini M, Cammaroto A, Brioni M, Montaruli C, Nikolla K, Guanziroli M, Dondossola D, Gatti S, Valerio V, Vergani GL, Pugni P, Cadringher P, Gagliano N, Gattinoni L (2016) Mechanical power and development of ventilator-induced lung injury. Anesthesiology 124(5):1100–1108. https://doi.org/10.1097/ALN.0000000000001056
Serpa Neto A, Deliberato RO, Johnson AEW, Bos LD, Amorim P, Pereira SM, Cazati DC, Cordioli RL, Correa TD, Pollard TJ, Schettino GPP, Timenetsky KT, Celi LA, Pelosi P, Gama de Abreu M, Schultz MJ, Investigators PN (2018) Mechanical power of ventilation is associated with mortality in critically ill patients: an analysis of patients in two observational cohorts. Intensive Care Med 44(11):1914–1922. https://doi.org/10.1007/s00134-018-5375-6
Zhang Z, Zheng B, Liu N, Ge H, Hong Y (2019) Mechanical power normalized to predicted body weight as a predictor of mortality in patients with acute respiratory distress syndrome. Intensive Care Med 45(6):856–864. https://doi.org/10.1007/s00134-019-05627-9
Tonna JE, Peltan I, Brown SM, Herrick JS, Keenan HT, University of Utah Mechanical Power Study G (2020) Mechanical power and driving pressure as predictors of mortality among patients with ARDS. Intensive Care Med 46(10):1941–1943. https://doi.org/10.1007/s00134-020-06130-2
Acknowledgements
Not applicable.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was funded by the German Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung), funding directive “KMU-innovativ: Medizintechnik”, Grant 13GW0240C. There was no participation of the funding body in the design of the study, the collection, analysis, and interpretation of data or the writing of the manuscript.
Author information
Authors and Affiliations
Contributions
Study conception: PAP, RCEF, WB, AP, SL, RK. Experimental design: PAP, MR, LH, PvP, RK. Animal experiments and data acquisition: MR, MT, EB, PAP, LH, PvP. Engineering and technical integration of software and hardware for closed-loop ventilation and calculation of mechanical power: PvP, LH, AP, RK. Analysis and interpretation of data: PAP, EB, FK, JAG, MR, MT, BL, RCEF. Drafting of manuscript: EB, MR, PAP, PvP, RCEF. Critical revision: WB, JAG, RK, BL, SL. All authors read and approved the final manuscript..
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All experiments were in accordance with the guidelines of the European and German Society of Laboratory Animal Science and were approved by the state authority for the care and use of animals (LAGeSo, Berlin, Germany; Approval G0229/18).
Consent for publication
Not applicable.
Competing interests
RK is an employee of EKU Elektronik GmbH, Germany. LH and WB are employees of Fritz Stephan GmbH, Germany. Otherwise, the authors have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Relative treatment effect values of respiratory and hemodynamic parameters of Tab. 1. Table S2. Relative treatment effect values of respiratory and hemodynamic parameters during low and high tidal volume ventilation. Table S3–S5. PEEP-Titration.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Boerger, E., Russ, M., von Platen, P. et al. Induction of severe hypoxemia and low lung recruitability for the evaluation of therapeutic ventilation strategies: a translational model of combined surfactant-depletion and ventilator-induced lung injury. ICMx 10, 32 (2022). https://doi.org/10.1186/s40635-022-00456-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40635-022-00456-5