
Abstract
Objectives
Effects of aging and leisure time physical activity (LPA) might influence the effect of occupational physical activity (OPA) on risk for cardiovascular disease (CVD). This study was conducted to determine whether OPA affects CVD after controlling the effects of LPA and other risk factors for CVD such as job stress.
Methods
Participants were 131 male Korean manual workers. Tests for heart rate variability (HRV) were conducted for five minutes in the morning at work. We defined OPA as the combined concept of relative heart rate ratio (RHR), evaluated using a heart rate monitor.
Results
Whereas high OPA was not related to any HRV items in the younger age group, high OPA was associated with an increased number of low-value cases among all HRV items in older workers. Exercise had beneficial effects only in the younger group. After controlling for exercise and other risk factors, the odds ratios of the root-mean square of the difference of successive normal R-R intervals (rMSSD) and high frequency band power (HF) among the older age and high OPA group compared with the younger age and low OPA group were 64.0 and 18.5, respectively. Social support and shift work were independent risk factors in HRV.
Conclusions
OPA in aging workers increases CVD risks. This study provides support for the need for protection of aging workers from physical work overload, and indicates the need for further study of optimal limits of OPA.
Similar content being viewed by others


Introduction
The global burden of cardiovascular disease (CVD) is extremely high, with CVD being involved in approximately one-third of all deaths worldwide [1]. One way to reduce the risk of CVD is through physical activity: both leisure time physical activity (LPA) and occupational physical activity (OPA) are thought to reduce cardiovascular risk by decreasing incidence of coronary heart disease and stroke [2, 3]. Although there is support for the conclusion that OPA is beneficial for CVD, the evidence is limited to mild to moderate OPA [2, 4, 5]. With respect to high OPA, previous studies have shown conflicting results ranging from protective [2] to no effects on CVD [4], and even some adverse consequences on cardiovascular health [5].
The burden of OPA on an individual worker varies according to their physical work capacity (PWC) [6]. PWC is largely dependent on age, and PWC has been shown to decrease rapidly after the age of 45 [7]. While the evidence suggests that the effects of OPA on health would differ for groups under and over age 45 years, there are currently no studies that directly compare the different effects of OPA on these two age groups. Given that LPA has also been shown to affect an individual’s cardiovascular health, it is conceivable that LPA and OPA might both have varying effects on health according to age. While a previous study reported on the paradoxical effects of OPA and LPA on health, no prior investigations have considered the importance of aging on OPA and LPA related health changes [8].
Heart rate variability (HRV) is valuable non-invasive tool that can be used to check the balance of the autonomic nervous system in the heart [9, 10]. As HRV is inversely related to hypercholesterolemia [11], hypertension [12], coronary atherosclerosis [13], and stroke [14], HRV can be regarded as a preclinical marker for CVDs. Although several studies have reported the effects of job stress on HRV [15, 16], few have addressed the relationship between HRV and high OPA. Additionally, while other occupational risk factors for HRV have been investigated including the presence of lead [17], manganese [18], and work shift, as well as general risk factors such as smoking [19] no studies focusing on OPA have adjusted for these risk factors.
The purposes of the current study was to evaluate the effects of high OPA on HRV according to age, investigate the different effects of OPA on HRV in relation to LPA, and evaluate the effects of high OPA on HRV after controlling for LPA and other risk factors for HRV.
Materials and methods
Study population
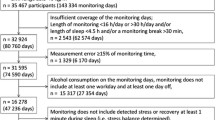
Five companies participated in this research, which was conducted from June 2003 to May 2004. One occupational physician and one industrial hygienist used a survey to select study participants from a group of manual workers, who were recruited based on similar OPA levels. The companies included foundry work(total manual workers: n = 169, study participants: n = 21), ship-building (total manual workers: n = 987, study participants: n = 46), car engine assembly (total manual workers: n = 489, study participants: n = 84), ship engine manufacture (total manual workers: n = 321, study participants: n = 30), and railway vehicle manufacture (total manual workers: n = 474, study participants: n = 43). The total number of participants in the study was 224; all participants were male. We exclude77 participants who did not undergo the heart rate monitor (HRM) evaluation that was used to assess OPA. Because the study was focused on occupational physical factors, we excluded participants with known risk for HRV, such as hypertension or diabetes mellitus patients (n = 7), and contact with metal fumes or organic solvents exposure cases (n = 9) to control for manganese and lead exposure. Before the study began, written informed consents were obtained from all participants. Ethical concerns for the current study were reviewed by the medical research institute of Pusan National University Hospital.
Occupational physical activity
OPA was checked using HRM (Polar Electro Co, Finland, S810TM). HRMs were attached to the participants’ chest during work. A work diary was also implemented, which was checked by researchers to determine daily work time and rest time. Relative heart ratio (RHR) was calculated using the following equation:
Maximum heart rate (HRmax) was obtained using a cycle ergometer (Combi Co., Korea, Aerobike 75XL II®). We defined OPA as a combination of RHR and number of working hours per day, as suggested by Wu and Wang [20]. OPA was divided into high and low as follows: high OPA was defined as RHR ≥ 16.0 (%) with work time ≥ 12 h, or 16.0 (%) ≤ RHR < 20 (%) with 10 h ≤ work time < 12 h, or 20.0 (%) ≤ RHR < 24.5 (%) with 8 h ≤ work time < 10 h, or RHR ≥ 24.5 (%) with work time > 8 h. All other combinations of RHR and work time were defined as low OPA.
Heart rate variability
All participants were required to refrain from drinking alcohol one day before the HRV test. Tobacco smoking and coffee drinking were also prohibited 30 min before HRV testing. Tests were conducted in a noise-free environment from 9 ~ 10 A.M. after a 30-min rest. HRV was tested for five minutes using the SA-2000E (Medicore, Korea, SA-2000E) according to the guidelines of the task force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology (20). Data were divided into time domain and frequency domain. Time domain was composed of the standard deviation of the normal to normal (NN) interval (SDNN), the square root of the mean squared differences of successive NN intervals (rMSSD), and the proportion of successive NN intervals greater than 50 ms (pNN50%). The frequency domain was composed of very low-frequency spectral power (VLF), total spectral power (TP), low-frequency power (LF), high-frequency power (HF), and LF/HF ratio in both ms2 and normalized units. Because the Task Force recommends not using pNN50, TP, and VLF from short-term measures, we used SDNN, rMSSD, LF, HF, and LF/HF ratio for the final analyses [21]. Because low HRV is associated with poor health, we divided HRV results into low and normal groups using proposed reference values for short-term HRV [22].
Questionnaire
A structured questionnaire was administered before the HRM and HRV tests. Demographics, health behavior including frequency of exercise during weekdays representing LPA, and work-related variables were assessed. The Korean version of the Job Content Questionnaire (JCQ) was used to check job stress. Validity and reliability of the Korean version of the JCQ have been evaluated elsewhere [23]. The Chronbach’s alpha values for job demand, decision latitude, and social support were 0.66, 0.59, and 0.86 in the current study, respectively. Each items of the JCQ were dichotomized by the median score.
Statistical analysis
Statistical analyses were conducted using SAS (version 9.3), with a significance level 0.05. Missing data for each variable were not considered in the analyses. Dependent measures were the dichotomous variables (low and normal) for each HRV items. Cochran Armitage trend tests were conducted to assess the relationship between categorical variables. Statistical analyses with a null value in the column position or raw total could not be conducted (identified as “not applicable”). After evaluation of the relationship between age, OPA, and exercise (LPA), multiple logistic regressions were used to adjust for exercise and other risk factors. Statistically significant variables related to HRV in univariate analyses were then used in multiple logistic regressions. To identify the combined effect of aging and OPA, four groups were used in the multiple logistic regressions: younger age and low OPA, younger age and high OPA, older age and low OPA, and older age and high OPA. Due to small numbers in some of the categories, data reduction by merging groups of variables was conducted for logistic regression.
Results
Relationship between demographic, health, and work-related variables with HRV
The results of trend tests between variables and time domain of HRV items are listed below. Older age group and lower social support were associated with increased cases of low SDNN. For frequency domain, older age and heavier alcohol use had more instances of low LF. Older age, higher body mass index (BMI), heavier alcohol drinking, and shift workers, and lower social support groups had more cases of low LF:HF ratio. However, lower social support was associated with fewer instances of low LF:HF ratio (Table 1).
Effects of OPA on HRV according to age and exercise respectively
To evaluate whether OPA effects on HRV differs between younger and older workers, we conducted trend tests between OPA and HRV items by each age group. In younger participants, no HRV items were associated with OPA. In older individuals, higher OPA groups had significantly more cases of low SDNN, rMSSD, HF, and HF/LF ratio. Trend tests between OPA and HRV by exercise showed inconsistent results: in the high exercise group, high OPA was significantly linked to greater instances of low rMSSD significantly. However, in the no exercise group, individuals with high OPA had significantly more cases of low LF, HF, and LF:HF ratio significantly (Table 2).
Effects of exercise on HRV according to age
Trend tests between exercise and HRV by age group revealed that among younger individuals, those who got less exercise had more cases of low rMSSD and HF. However, there was no association between exercise and HRV items in older participants (Table 3).
Effects of OPA on HRV according to age and exercise combined
To evaluate whether OPA effects on HRV differed according to age and exercise, trend tests between OPA and HRV items by each age and exercise category were conducted. In younger individuals, those with no exercise and high OPA had more cases of low LF and HF. In older individuals, exercise frequency did not seem to influence the effects of OPA on HRV. In the old age and frequent exercise group (≥3 times per week), high OPA was associated with more instances of low SDNN, rMSSD, and HF. Due to small sample size, only HF/LF ratio reached significance in the old age and moderate exercise group (1-2 times per week) with high OPA. In the old age and no exercise group, statistical analyses could not be conducted due to null values in the raw total column. Notably, there were no workers in the old age and no exercise group who had high OPA (Table 4).
Combined effects of OPA and age on HRV adjusting exercise and other risk factors
After controlling for exercise and other risk factors in the univariate analysis, younger workers with low OPA were used as a reference group with which to compare the other three groups. Odds ratio (OR) of rMSSD and HF of the older age and high OPA group compared with the younger age and low OPA group were 64.0 and 18.5, respectively. Exercise had a protective effect on rMSSD with an OR of 0.2. Social support had protective effect on SDNN with OR of 0.3. BMI and shiftwork were independent risk factors for the HF/LF ratio. In a multiple logistic analysis, social support was not significantly related to the LF:HF ratio (Table 5).
Discussions
In the current study, the effects of OPA on HRV significantly differed according to age. Whereas high OPA was not related with any HRV items in the younger age group, high OPA increased the occurrence of low cases in all HRV items except LF (borderline significance) in older participants. After adjusting for exercise and other risk factors by multiple logistic regression analysis, high OPA in older individuals compared with low OPA in younger individuals was related to an increase in the number of cases of low rMSSD and HF in HRV. In constant with these findings, a previous study showed that LPA and mild-to-moderate OPA decreased the likelihood of a myocardial infarction (MI), while heavy OPA was not associated with a reduced risk [5]. We showed an increased risk of HRV from OPA, especially in aging workers. Whereas the previous study assessed OPA using subjective questionnaire, we used an objective measure of RHR. However, reports from the previous study that increasing OPA from mild to heavy elevates the risk for MI is in line with the findings from the current study (statistically significant in the model I adjusted for age, sex, and socio-economic status).
As rMSSD and HF are considered a reflection of vagal outflow [21, 24], high OPA might causes a repression of parasympathetic nervous system (PNS) activity. Decreased PNS activity has been explained by a gradual atrophy of the system due to cumulative fatigue [25], and it is widely established that HRV decreases with age [26]. Previous studies on the effects of exercise on HRV show differing results according to activity level. Moderate exercise increases HRV HF due to cardiovascular adaptation to aerobic training [27]. On the contrary, long term physical overtraining decreases rMSSD, LF, and HF [28]. In the current study, exercise has beneficial effects only in the younger group. Previous studies have also shown different beneficiary effects of exercise on HRV according to age, with younger individuals showing a greater increase of HRV after training [27]. Thus this study shows that high OPA has similar effects as over-exercising with the adverse effects of OPA in old age possibly explained by a gradual exhaustion of PNS activity and loss of cardiovascular adaptation.
In current study, social support and shift work were independent occupational risk factors on HRV. Social support can act as a buffer, improving adaptation to changing and stressful situations [29]. Conversely, altered circadian rhythm from night shift work can cause adverse changes in HRV [30, 31]. One of the most interesting finding from this study is that all older workers with high OPA exercise regularly. This may be explained in several ways, one of which may be the small number of participants over the age of 45. An alternative explanation is the healthy survival effect, in which older individuals who work in strenuous OPA conditions needs to build up physical fitness in order to survive in the workplace, while physically weaker workers would have left the high OPA work job. If the latter explanation is correct, measures should be taken to protect aging workers in physical and social contexts.
This study has several limitations. Causal relationships are difficult to determine from cross sectional study design. In addition, the number of study subjects included is too small to evaluate all of the original hypotheses, especially for the effects of high OPA in relation to low exercise in the older age group. Further, although we used objective marker to check OPA, we were not able to use objective tools to evaluate LTA, which could have resulted in a misclassification of LTA. Well-designed longitudinal studies with larger samples using objective measures of OPA and LTA are needed to examine the remaining questions. Although the techniques of HRV have been standardized, there are many problems to solve [21]. Five minute methods are strength to evaluate in a short time, while it is less accurate than 24 h method. Also there are intra-personal variations according to diurnal rhythm, breathing status, coffee, and smoking. Also there still have some grey area of normality and interpretation among time and frequency domains [21, 22]. Although we tried to reduce those problems including restriction of evaluation time and atmosphere, coffee and smoking, those limitation might influence results. Although we evaluated OPA with objective methods, we could not fully evaluate work characteristics among 5 occupational groups. Because detailed work characteristics might be different between groups, the objective OPA might have been misclassified in some degree.
Despite these limitations, this study revealed adverse effects of high OPA in older age workers. Prolonged working hour and excessive OPA are major occupational problems in Korea, with corresponding increases in the compensable CVD [32]. As adverse HRV is a preclinical biomarker for CVD including coronary heart disease, stroke, dysrhythmia, and sudden death [2, 21], the findings of this study potentially indicate that high OPA could cause CVD. This study showed adverse effects of high OPA on health by examining work environment using RHR and working hours to calculate OPA, as suggested by a prior investigation [20]. The results of this study suggest the need for reducing physical work load, or the number of working hours if work load can not be reduced, according to the work limit suggested in the previous study. These findings are especially important for workers over the age of 45. This study also indicates the need for further research into optimal OPA in workers.
Conclusions
This study showed adverse effects of high OPA on health by examining work environment using RHR and working hours to calculate OPA. The results of this study suggest the need for reducing physical workload, or the number of working hours if workload cannot be reduced, according to the occupational exposure limit. These findings are especially important for workers over the age of 45. This study also indicates the need for further research into optimal OPA in workers.
References
Deaton C, Froelicher ES, Wu LH, Ho C, Shishani K, Jaarsma T. The global burden of cardiovascular disease. Eur J Cardiovasc Nurs. 2011;10 Suppl 2:S5–13.
Li J, Siegrist J. Physical activity and risk of cardiovascular disease-a meta-analysis of prospective cohort studies. Int J Environ Res Public Health. 2012;9:391–407.
Shin SY, Lee CG, Song HS, Kim SH, Lee HS, Jung MS, et al. Cardiovascular diseases risk of bus drivers in a city of Korea. Ann Occup Environ Med. 2013;25:34. doi:10.1186/2052-4374-25-34.
Mozumdar A, Liguori G, DuBose K. Occupational physical activity and risk of coronary heart disease among active and non-active working-women of North Dakota: a Go Red North Dakota Study. Anthropol Anz. 2012;69:201–19.
Held C, Iqbal R, Lear SA, Rosengren A, Islam S, Mathew J, et al. Physical activity levels, ownership of goods promoting sedentary behaviour and risk of myocardial infarction: results of the INTERHEART study. Eur Heart J. 2012;33:452–66.
De Zwart BC, Frings-Dresen MH, van Dijk FJ. Physical workload and the aging worker: a review of the literature. Int Arch Occup Environ Health. 1995;68:1–12.
Ilmarinen J. Aging workers. Occup Environ Med. 2001;58:546–52.
Holtermann A, Hansen JV, Burr H, Søgaard K, Sjøgaard G. The health paradox of occupational and leisure-time physical activity. Br J Sports Med. 2012;46:291–5.
Xhyheri B, Manfrini O, Mazzolini M, Pizzi C, Bugiardini R. Heart rate variability today. Prog Cardiovasc Dis. 2012;55(3):321–31.
Choi BK, Schnall PL, Dobson M, Garcia-Rivas J, Kim HY, Zaldivar F, et al. Very long (>48 hours) shifts and cardiovascular strain in firefighters: a theoretical framework. Ann Occup Environ Med. 2015;26:5. doi:10.1186/5652-4374-26-5.
Christensen JH, Toft E, Christensen MS, Schmidt EB. Heart rate variability and plasma lipids in men with and without ischemic heart disease. Atherosclerosis. 1999;145:181–6.
Singh JP, Larson MG, Tsuji H, Evans JC, O’Donnell CJ, Levy D. Reduced heart rate variability and new-onset hypertension: insights into pathogenesis of hypertension: the Framingham Heart Study. Hypertension. 1998;32:293–7.
Huikuri HV, Jokinen V, Syvänne M, Nieminen MS, Airaksinen KE, Ikäheimo MJ, et al. Heart rate variability and progression of coronary atherosclerosis. Arterioscler Thromb VascBiol. 1999;19:1979–85.
Kwon DY, Lim HE, Park MH, Oh K, Yu SW, Park KW, et al. Carotid atherosclerosis and heart rate variability in ischemic stroke. Clin Auton Res. 2008;18:355–7.
Clays E, De Bacquer D, Crasset V, Kittel F, de Smet P, Kornitzer M, et al. The perception of work stressors is related to reduced parasympathetic activity. Int Arch Occup Environ Health. 2011;84:185–91.
Lee KH, Yoon K, Ha M, Park J, Cho SH, Kang D. Heart rate variability and urinary catecholamines from job stress in Korean male manufacturing workers according to work seniority. Ind Health. 2010;48:331–8.
Gajek J, Zysko D, Chlebda E. Heart rate variability in workers chronically exposed to lead. Kardiol Pol. 2004;61:21–30.
Barrington WW, Angle CR, Willcockson NK, Padula MA, Korn T. Autonomic function in manganese alloy workers. Environ Res. 1998;78:50–8.
Kobayashi F, Watanabe T, Akamatsu Y, Furui H. Acute effects of cigarette smoking on the heart rate variability of taxi drivers during work. Scand J Work Environ Health. 2005;31:360–6.
Wu HC, Wang MJ. Relationship between maximum acceptable work time and physical workload. Ergon. 2002;45:280–9.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur Heart J. 1996;17:354–81.
Nunan D, Sandercock GR, Brodie DA. A quantitative systemic review of normal values for short-term heart rate variability in health adults. Pacing Clin Electrophysiol. 2010;33:1407–17.
Eum KD, Li J, Jhun HJ, Park JT, Tak SW, Karasek R, et al. Psychometric properties of the Korean version of the job content questionnaire: data from health care workers. Int Arch Occup Environ Health. 2007;80:497–504.
Fei L, Copie X, Malik M, Camm J. Short- and long-term assessment of heart rate variability for risk stratification after acute myocardial infarction. Am J Cardiol. 1996;77:681–4.
Pichot V, Bourin E, Roche F, Garet M, Gaspoz JM, Duverney D, et al. Quantification of cumulated physical fatigue at the workplace. Pflugers Arch. 2002;445:267–72.
Elsenbrunch S, Harnish MJ, Orr WC. Heart rate variability during waking and sleep in healthy males and females. Sleep. 1999;22:1067–71.
Carter JB, Banister EW, Blaber AP. The effect of age and gender on heart rate variability after endurance training. Med Sci Sports Exerc. 2003;35:1333–40.
Earnest CP, Jurca R, Church TS, Chicharro JL, Hoyos J, Lucia A. Relation between physical exertion and heart rate variability characteristics in a professional cyclists during the Tour of Spain. Br J Sports Med. 2004;38:568–75.
Shin YS, Byun JS, Kim SH, Shin JH, Choi BY, Nam JH, et al. Difference of the heart rate variability according to the social support level in a county. Korean J Psychosom Med. 2012;20:59–65. Korean.
Togo F, Takahashi M. Heart rate variability in occupational health –a systematic review. Ind Health. 2009;47:589–602.
Ishii N, Dakeishi M, Sasaki M, Iwata T, Murata K. Cardiac autonomic imbalance in female nurses with shift work. Auton Neurosci. 2005;122:94–9.
Lee KH, Kim JE, Kim YK, Kang DM, Yun MJ, Park SG, et al. Long working hours and emotional well-being in Korean manufacturing industry employees. Ann Occup Environ Med. 2013;25:25–38.
Acknowledgement
This study was supported by Medical Research Institute Grant (2003-22), Pusan National University Hospital.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contribution
Kang DM participated in the study design and writing. Kim YK performed field study and writing. Hwang YS performed field study. Kim JE, Cho BM performed statistical analysis and reviewed the article. Hong TJ interpreted the data of HRV. Lee YH reviewed and revised the article. Sung BM performed filed study and writing. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kang, D., Kim, Y., Kim, J. et al. Effects of high occupational physical activity, aging, and exercise on heart rate variability among male workers. Ann of Occup and Environ Med 27, 22 (2015). https://doi.org/10.1186/s40557-015-0073-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40557-015-0073-0