
Abstract
Background
Rest–activity rhythms are directly related to health risks, but there are limited objective methods to assess them. This study aimed to investigate the relationship between rest–activity rhythms and cardiorespiratory fitness (CRF) in middle-aged workers.
Methods
Peak oxygen uptake was measured on a treadmill to assess CRF in 254 middle-aged workers who were divided into low, medium, and high-CRF groups based on tertiles. Participants were asked to wear an accelerometer (activPAL) on their thighs for 1 week, and the logarithmically transformed acceleration data were used for the analysis of a 24-hour rest–activity rhythm. Sex, age, body mass index, occupation, smoking status, and alcohol consumption were used as covariates in Model 1, with Model 2 also including walking count on non-workdays. Repeated measures analysis of variance was used to compare time course of rest–activity rhythms changes on workdays between groups, and post-hoc tests were conducted using Bonferroni’s correlation.
Results
Higher CRF correlated with increased physical activity. In model 1, higher CRF showed improved interdaily stability, but the significant difference disappeared in model 2 after adjusting for non-workday walking counts. A time-course group comparison showed that the high group had significantly higher activity levels than those of the low group from 6:00 to 8:59 and 17:00 to 17:59 and the medium group from 6:00 to 7:59 and 19:00 to 19:59.
Conclusions
Workers who have better rest–activity rhythms and engage in higher levels of physical activity on workdays tend to have higher CRF levels. Regular daily routines, influenced by physical activity during holidays, can positively impact cardiopulmonary endurance.
Similar content being viewed by others

Background
Cardiorespiratory fitness (CRF) is a highly reliable predictor of physical and mental health outcomes and mortality in individuals with or without chronic diseases, including cardiovascular disease and depressive symptoms [1,2,3,4,5].
A 10-year follow-up longitudinal study has revealed that CRF decreases throughout one’s lifespan; however, engaging in sports and/or leisure-time physical activities can help slow down this process [6]. Moreover, increasing physical activity and independently decreasing sedentary behavior are directly associated with higher CRF levels [7]. However, an intervention study that reduced sedentary behavior among middle-aged adults for 1 h per day for 6 months without adding exercise did not affect CRF, while increasing daily activity may increase CRF [8]. Specifically, there is a strong interconnection between the physical activity level and sedentary behavior of workers [9], thereby warranting future studies that focus on occupational cohorts with a substantial prevalence of sedentary behavior at work [9]. Although this may vary according to occupation, workers who spend most of their working hours sitting may have poor CRF [10]. In an epidemiological study using compositional data analysis, reallocation from sedentary behavior to other physical activities (e.g., activities with a low and moderate-to-vigorous intensity) during nonworking time on workdays, including walking to the station, climbing stairs, standing on the train/bus, and engaging in household activities, was favorably associated with cardiometabolic status, which is related to CRF [11], among office workers [12].
Daily circadian synchronization of physiological functioning is essential for the optimal functioning of peripheral organs, including the heart [13]. Prolonged circadian misalignment is associated with increased blood pressure, diminished sleep quality, and an overall increased risk of cardiovascular disease [13]. Specifically, healthy circadian rhythms in adults are independent of physical activity and associated with lower cardiometabolic risk, cardiovascular disease, and mortality [14, 15].
In recent years, accelerometers have become increasingly popular owing to better participant compliance and their ability to measure circadian rhythms, including activity and sleep, over a 24-h protocol [16]. Previous studies with nonparametric analyses used an accelerometer worn on the wrist (e.g., ActiGraph) [17, 18]. These novel approaches have enabled the evaluation of 24-h rest–activity rhythms using accelerometers [19]. However, using wrist movement counts in estimating physical activity (e.g., energy expenditure) may introduce more errors than using other body sites, as there is a significant amount of upper limb gesticulation (e.g., worker’s main activities, such as animated talk, keyboarding, and repetitive desk work) that does not correspond to large body movement [20,21,22,23]. Further studies should focus on accelerometers worn in other locations (e.g., activPAL), which measure 24-h rest–activity rhythms [22, 23].
However, only a limited number of studies have investigated the measurement of 24-h rest–activity rhythms using accelerometers worn on the thigh or other locations. In addition, the relationship between 24-h rest–activity rhythms and CRF remains unknown. Based on the results of previous studies [1, 12, 14, 15], we formulated two hypotheses: (1) workers who maintain a regular workday exhibit higher CRF and (2) workers who are more physically active on the workday demonstrate higher CRF.
Methods
Participants and data collection
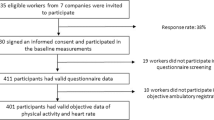
This cross-sectional study was conducted in Japan between June 2016 and March 2022 [24]. All the participants were recruited through a website advertisement. We enrolled participants from Japan’s capital area who were aged between 30 and 59 years old and were employed full-time, meaning they worked for at least 6 h a day and 4 days a week. Additionally, the participants had to have completed a test to measure their CRF (i.e., peak oxygen uptake [VO2peak]) and could not take any drugs that affected their autonomic nervous system (e.g., β-blockers). The participants also had to have no medical conditions that would preclude them from taking the VO2peak test and had to have received medical certification within the past year. The flow of the day of the visit has been described previously [24]. In total, 320 middle-aged adults participated in this study.
We excluded individuals who were shift workers (n = 24), had unclear occupational status (n = 2), provided less than 4 days of accelerometer data (n = 30), or did not wear the accelerometer during the sleep period (n = 10). Ultimately, 254 participants were included in the analysis.
Measurements
Rest–activity rhythm data acquisition and analysis
The participants were required to continuously wear an accelerometer (activPAL™, Pal Technologies Ltd., Glasgow, UK) for more than 7 consecutive days (24 h/day), except during bathing. The accelerometer data were recorded at 15-s intervals (epochs) over 24 h at a sampling rate of 10 Hz. Over the course of the study, the activPAL model transitioned from activPAL 3 C (2016 to 2017) to activPAL micro (2017 to 2019) and finally to activPAL 4 (2019 ~ 2022). However, all raw data were processed using the same standard algorithm (i.e., VANE) by PAL Software Suite version 8 to extract the acceleration data. The raw accelerometer data (i.e., acceleration volume) were computed using PAL Software Suite version 8 (Pal Technologies Ltd., Glasgow, UK) [25, 26]. In addition, study participants were instructed to use a web diary (web application) developed by us to record their bedtimes, wake times on workdays and off-days, the start of work, return home, and exercise. The weekly accelerometer data were exclusively computed based on the data collected during workdays with reference to the web diary. The calculated acceleration data were log-transformed as in previous studies [19] and represented over a 24-h time period (Additional file 1: Figure S1). The GGIR R package (version 2.10.1) was used to characterize and impute missing acceleration data [27]. Data selection and exclusion criteria were based on a previous study [17].
A nonparametric methodological analysis of rest–activity rhythm measures was derived using the nparACT R package (version 0.8) [28], including variables such as interdaily stability (IS), intradaily variability (IV), and relative amplitude (RA). We also calculated the amplitude of acceleration during the 5 h with the lowest activity (L5) and the 10 h with the highest activity (M10), to determine the extent of activity during the rest and active periods [19].
IS describes the invariability of the 24-h rhythm between different days and indicates better coupling/synchronization of the rest–activity rhythm to external zeitgebers. Conversely, IV measures the degree of fragmentation in a rhythm, including the frequency and extent of transitions that may reflect the occurrence of daytime naps and/or nocturnal awakenings. A perfect sine wave would have an IV value close to 0, whereas Gaussian noise would have a value of approximately 2, and a rhythm with a well-defined ultradian period of approximately 2 h could have an even higher value. RA describes the normalized difference between M10 and L5, with higher values indicating a healthy 24-h rhythm, reflecting higher activity during the wake period and relatively lower activity at night [19]. Briefly, a healthy rhythm is characterized by greater activity during active periods and lower activity during rest periods. These indices have been extensively used in the study of rest–activity rhythms and are valuable tools for quantifying the properties of biological rhythms [17, 19, 28] (Fig. 1).

Examples of different rest and activity rhythms among female office workers of the same age. Bars indicate hourly data for the workday. IS, interdaily stability; IV, intradaily variability; RA, relative amplitude; L5, amplitude of acceleration during the 5 h with the lowest activity; M10, amplitude of acceleration during the 10 h with the highest activity
Cardiorespiratory fitness
The participants underwent a graded exercise test on a treadmill (AR200; Minato Medical Science, Osaka, Japan) following the Bruce protocol to directly measure their VO2peak. Throughout the test, an open-circuit computerized indirect calorimeter (AE-310 S, Minato Medical Science, Osaka, Japan) was used to continuously measure ventilation and expired gases, whereas heart rate was monitored using an electrocardiogram (Life Scope, Nihon Kohden, Tokyo, Japan). Moreover, the rate of perceived exertion was recorded using the Borg 6–20 scale.
VO2peak was determined as the highest 30-s average VO2 value that met at least three of the following four criteria: (1) a respiratory exchange ratio exceeding 1.10; (2) a maximal heart rate within 10 beats per minute of the age-predicted maximum; (3) a rate of perceived exertion exceeding 17; and (4) a plateau in VO2 despite further increases in workload [24, 29]. The measurement methods and other details are explained in a previous study [24].
Potential confounders
As potential confounding factors, we included age (continuous variable), sex (male or female), body mass index (BMI) (continuous variable), alcohol consumption (never, 1–2 times/month, 1–2 times/week, 3–4 times/week, 5–6 times/week, and daily), smoking history (past/never or current), walking count on non-workdays measured as active Pal, and occupational information.
The occupation data were classified based on the Japanese Standard Occupational Classification [30] into various categories, including managers, clerical workers, marketing professionals, service and sales personnel, manual laborers, healthcare professionals, education professionals, technicians and researchers, security personnel, agricultural/forestry and fishery workers, manufacturing personnel, transport and machinery workers, construction and mining workers, and others. We reclassified the occupation data into five categories: (1) clerical support; (2) services and sales; (3) professionals; (4) skilled agricultural, forestry, and fishery workers and plant/machine operators and assemblers; and (5) others.
Statistical analyses
To remove the influence of sex and age [31, 32], we stratified the patients into 5-year age increments (30–34, 35–39, 40–44, 45–49, 50–54, and 55–59 years old). Subsequently, we defined tertiles of VO2peak into the low (32.6 ± 4.4 ml/kg/min, n = 80), moderate (38.2 ± 4.4 ml/kg/min, n = 91), and high groups (44.9 ± 5.5 ml/kg/min, n = 83) (Table 1).
To compare the three groups as independent variables with participant characteristics as dependent variables, we used a one-way analysis of variance with Bonferroni post-hoc tests for continuous variables and the chi-squared test for categorical variables. An analysis of covariance (ANCOVA) trend test was conducted to examine the trend of rest–activity rhythm variables as dependent variables, with the three groups as independent variables. To ensure accurate analysis and account for potential confounding factors related to non-workday physical activity, three models were utilized: an unadjusted model, Model 1 (adjusted for age, sex, BMI, alcohol consumption, smoking history, and occupational information), and Model 2 (which included all the factors in Model 1 and walking count on non-workdays). In this study, time-course changes were analyzed with groups as independent variables and rest–activity rhythms as dependent variables over a 24-hour period, using repeated-measures ANCOVA while controlling for age, sex, BMI, alcohol consumption, smoking history, and occupation information. The Bonferroni correction was performed as a post-hoc test. For this, the acceleration data for rest–activity rhythms were calculated in 15-s epoch increments and reported as an hourly average. All statistical analyses were performed using the Statistical Package for the Social Sciences version 26.0 (IBM Corporation, Armonk, NY, USA). Statistical significance was set at P < 0.05 (two-tailed).
Results
The average number of days with valid accelerometer data was 6.2 ± 0.9 days. The participants’ average VO2peak was 38.6 ± 6.9 ml/kg/min, and 44.5% of the total participants were female. Table 2 shows the notable variations in BMI, VO2peak, and walking count on workdays and non-workdays among the CRF groups. However, no significant differences were observed in occupational status among the CRF groups.
In all models, higher CRF was associated with higher M10 values. Conversely, IS values tended to show better outcomes with higher CRF, but the significant difference disappeared in model 2, which accounted for walking counts on non-workdays. Similarly, the unadjusted model indicated that higher cardiopulmonary endurance was associated with better RA values, but the significant difference disappeared in models 1 and 2 (Table 3).
The rest–activity data over time showed significant effects of time (P < 0.001), group (P = 0.016), and interaction (P < 0.001). The post-hoc test results showed that the high-CRF group was significantly more active at 6:00–8:59 and 17:00–17:59 (all P < 0.05) compared with that of the low-CRF group (Fig. 2). In addition, the high-CRF group was significantly more active at 6:00–7:59 and 19:00–20:59 compared with that of the medium-CRF group (all P < 0.05) (Fig. 2). However, no significant differences were observed during nighttime (21:00–5:59) and working time (9:00–16:59) among the groups (Fig. 2).

Time course of 24 h rest–activity rhythm during workdays. The time course of 24 h rest–activity rhythm during workdays indicated an average of 1 h using two-way analysis of covariance; #Significant difference between the low-CRF group and the high-CRF group; *Significant difference between the medium-CRF group and the high-CRF group; VO2peak was stratified by sex and age into tertiles: low (32.6 ± 4.4 ml/kg/min, n = 80), moderate (38.2 ± 4.4 ml/kg/min, n = 91), and high groups (44.9 ± 5.5 ml/kg/min, n = 83). CRF, cardiorespiratory fitness; VO2peak, peak oxygen uptake
Discussion
This study examined the relationship between rest–activity rhythms and CRF levels in middle-aged workers. Rest–activity rhythms were measured using an accelerometer worn on the thigh. The participants with higher levels of CRF were more active, regardless of whether it was a workday or not, compared with those with lower levels of CRF (Table 2).
The present study results showed that workers with higher CRF tended to have more regular workdays, supporting our first hypothesis (IS in Model 1, Table 3). However, the amount of exercise on non-workdays may also play a role (IS in Model 2, Table 3), suggesting that individuals with irregular lifestyle patterns can offset their impact on CRF through weekend exercise [33].
Furthermore, the results support the second hypothesis, indicating that workers with higher weekday physical activity may maintain elevated CRF levels regardless of the amount of physical activity outside of the weekday (M10 in Table 3). Specifically, participants with higher levels of CRF exhibited higher M10 values and were notably more active during their commute to work and during equivalent leisure time after work compared to those of workers with low or medium CRF (Table 3; Fig. 2).
The present study is one of the few studies to investigate the 24-hour rhythm of individuals with high CRF who are engaged in the workforce, using accelerometers to objectively assess their rest–activity rhythm, with a focus on workdays. The findings from this study partly align with previous research results, which has shown a favorable association between physical activity during non-work hours on weekdays and cardiometabolic status related to CRF and mortality [11,12,13,14,15].
A previous observational study demonstrated that sleep duration was negatively associated with CRF in younger adults [34]. However, the sleep-related variable L5 (similar to wake after sleep onset) was not significantly related to CRF. This can be attributed to the fact that the sleep patterns examined in this study are specifically limited to workdays; therefore, the evaluation of sleep duration is not based on individual preference or choice. CRF is a highly reliable predictor of cardiovascular disease [1,2,3,4,5, 11,12,13,14,15]. Additionally, engaging in both vigorous and light physical activities toward the end of a workday is positively associated with enhancing employees’ self-efficacy while working, which in turn benefits their work roles [35].
Relative workload (e.g., heart rate reserve) determines the acute and long-term physiological effects of physical activity at work. Increasing CRF decreases the relative workload and reduces the risk of cardiovascular disease and all-cause mortality, as reported in a previous study [36]. Hence, the physical activity level of workers may affect their physical and mental health, which may in turn affect their CRFs. Another concept is the physical activity paradox, which suggests that higher levels of physical activity during work increase the risk of cardiovascular disease [36,37,38]. However, our results contradicted this paradox, possibly because previous studies primarily focused on blue-collar workers, whereas our study largely involved white-collar workers (93.8%). In Japan, there is a phenomenon known as overwork-related sudden death, or “karoshi,” which is associated with cerebrovascular, cardiac, and psychiatric conditions. Cardiovascular and cerebrovascular diseases are highly interconnected, and comorbidities or complications from both diseases can result in high mortality rates [39]. The findings of this study suggest that engaging in physical activity during non-working hours on workdays may protect against cardiovascular disease.
Some previous studies have revealed a relatively high agreement between ActiGraph and activPAL recordings in free-living conditions [40,41,42], although there are also some arguments that activPAL may be slightly less sensitive than ActiGraph; moreover, activPAL may underestimate or overestimate sleep duration compared with that using ActiGraph [43, 44]. This disagreement is based on the cutoff point for determining moderate-to-vigorous physical activity and the appropriate algorithm for measuring sleep using accelerometers [45]. A systematic review has stated that it is essential to use accelerometers worn at various sites for 24 h to accurately measure rest–activity rhythms [22, 23]. Our results, which calculated rest–activity rhythms on a timeline (Additional file 1: Figure S1), appear to be similar to those of a previous study [19]; however, future studies should confirm the agreement between ActiGraph and ActivPAL rest–activity rhythm measurements.
Our study has some limitations. First, the sample size was small. Thus, although our analysis was adjusted for occupational status and other potential confounders, future studies should focus on individual differences, including sex, age, and occupational status. Second, we used prior studies [31, 32] to stratify participants to minimize the effects of sex and age; however, caution should be exercised in generalizing our results because of potential sampling bias in the selection of participants. Finally, owing to the limited duration of measurement (i.e., consecutive 7 days), the investigation of rest–activity rhythms during non-workdays was not feasible [23]. We adjusted the number of steps to account for the influence of non-workday exercise habits; however, there was still a positive correlation between the number of steps taken on non-workdays and workdays (r = 0.345, P < 0.001), which raises the possibility of over-adjustment. Thus, future studies should aim to conduct measurements over a period of > 2 weeks to accurately assess rest–activity rhythms during non-workdays.
Conclusions
Participants who have healthy daily rest–activity rhythms and are more physically active during working hours have higher levels of CRF. Notably, the amount of physical activity while attending and leaving work on workdays and leisure time after work may also have significant effects on the CRF levels of working individuals.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author (seol.jaehoon.ge@u.tsukuba.ac.jp) on reasonable request.
Abbreviations
- CRF:
-
Cardiorespiratory fitness
- VO2peak :
-
Peak oxygen uptake
- ANCOVA:
-
Analysis of covariance
- BMI:
-
Body mass index
- IS:
-
Interdaily stability
- IV:
-
Intradaily variability
- L5:
-
Amplitude of acceleration during the 5 h with the lowest activity
- M10:
-
Amplitude of acceleration during the 10 h with the highest activity
References
Franklin BA, Eijsvogels TMH, Pandey A, Quindry J, Toth PP. Physical activity, cardiorespiratory fitness, and cardiovascular health: a clinical practice statement of the ASPC Part I: bioenergetics, contemporary physical activity recommendations, benefits, risks, extreme exercise regimens, potential maladaptations. Am J Prev Cardiol. 2022;12:100424.
Kokkinos P, Faselis C, Samuel IBH, Pittaras A, Doumas M, Murphy R, et al. Cardiorespiratory fitness and mortality risk across the spectra of age, race, and sex. J Am Coll Cardiol. 2022;80:598–609.
Stamatakis E, Ahmadi MN, Gill JMR, Thøgersen-Ntoumani C, Gibala MJ, Doherty A, et al. Association of wearable device-measured vigorous intermittent lifestyle physical activity with mortality. Nat Med. 2022;28:2521–9.
Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med. 2002;346:793–801.
Williams PT. Physical fitness and activity as separate Heart Disease risk factors: a meta-analysis. Med Sci Sports Exerc. 2001;33:754–61.
Bahls M, Ittermann T, Ewert R, Stubbe B, Völzke H, Friedrich N, et al. Physical activity and cardiorespiratory fitness–a ten-year follow-up. Scand J Med Sci Sports. 2021;31:742–51.
Kulinski JP, Khera A, Ayers CR, Das SR, de Lemos JA, Blair SN et al. Association between cardiorespiratory fitness and accelerometer-derived physical activity and sedentary time in the general population. Mayo Clin Proc. 2014;89:1063-71.
Norha J, Sjöros T, Garthwaite T, Laine S, Saarenhovi M, Kallio P, et al. Effects of reducing sedentary behavior on cardiorespiratory fitness in adults with metabolic syndrome: a 6-month RCT. Scand J Med Sci Sports. 2023;33:1452–61.
Smith L, McCourt O, Sawyer A, Ucci M, Marmot A, Wardle J, et al. A review of occupational physical activity and sedentary behaviour correlates. Occup Med (Lond). 2016;66:185–92.
Gerber M, Lindwall M, Lindegård A, Börjesson M, Jonsdottir IH. Cardiorespiratory fitness protects against stress-related symptoms of burnout and depression. Patient Educ Couns Patient ed. 2013;93:146–52.
Nichols S, Taylor C, Page R, Kallvikbacka-Bennett A, Nation F, Goodman T, et al. Is cardiorespiratory fitness related to cardiometabolic health and all-cause mortality risk in patients with coronary Heart Disease? A CARE CR study. Sports Med Open. 2018;4:22.
Kitano N, Kai Y, Jindo T, Fujii Y, Tsunoda K, Arao T, et al. Association of domain-specific physical activity and sedentary behavior with cardiometabolic health among office workers. Scand J Med Sci Sports. 2022;32:1224–35.
Hower IM, Harper SA, Buford TW. Circadian rhythms, exercise, and cardiovascular health. J Circadian Rhythms. 2018;16:7.
Yang L, Feng H, Chen J, Kwok Wing Y, Benedict C, Tan X, et al. Association of circadian rest-activity rhythms with Cardiovascular Disease and mortality in type 2 Diabetes. Diabetes Res Clin Pract. 2023;197:110262.
Westerterp-Plantenga MS, Drummen M, Tischmann L, Swindell N, Stratton G, Raben A, et al. Circadian rhythm parameters and physical activity associated with cardiometabolic risk factors in the PREVIEW lifestyle study. Obes (Silver Spring). 2023;31:744–56.
Liu F, Wanigatunga AA, Schrack JA. Assessment of physical activity in adults using wrist accelerometers. Epidemiol Rev. 2022;43:65–93.
Palmer JR, Wang C, Kong D, Cespedes M, Pye J, Hickie IB, et al. Rest-activity rhythms and tract specific white matter lesions in older adults at risk for cognitive decline. Mol Psychiatry. 2022;27:3410–6.
Mayeli A, LaGoy AD, Smagula SF, Wilson JD, Zarbo C, Rocchetti M, et al. Shared and distinct abnormalities in sleep-wake patterns and their relationship with the negative symptoms of schizophrenia spectrum disorder patients. Mol Psychiatry. 2023;28:2049–57.
Neikrug AB, Chen IY, Palmer JR, McCurry SM, Von Korff M, Perlis M, et al. Characterizing behavioral activity rhythms in older adults using actigraphy. Sens (Basel). 2020;20:549.
Halonen JI, Pulakka A, Pentti J, Kallio M, Koskela S, Kivimäki M, et al. Cross-sectional associations of neighbourhood socioeconomic disadvantage and greenness with accelerometer-measured leisure-time physical activity in a cohort of ageing workers. BMJ Open. 2020;10:e038673.
Mannini A, Intille SS, Rosenberger M, Sabatini AM, Haskell W. Activity recognition using a single accelerometer placed at the wrist or ankle. Med Sci Sports Exerc. 2013;45:2193–203.
Stevens ML, Gupta N, Inan Eroglu EI, Crowley PJ, Eroglu B, Bauman A, et al. Thigh-worn accelerometry for measuring movement and posture across the 24-hour cycle: a scoping review and expert statement. BMJ Open Sport Exerc Med. 2020;6:e000874.
Edwardson CL, Winkler EAH, Bodicoat DH, Yates T, Davies MJ, Dunstan DW, et al. Considerations when using the activPAL monitor in field-based research with adult populations. J Sport Health Sci. 2017;6:162–78.
Matsuo T, So R, Murai F. Improved VO2max estimation by combining a multiple regression model and linear extrapolation method. J Cardiovasc Dev Dis. 2022;10:9.
Buchan DS, Baker JS. Development and evaluation of sedentary time cut-points for the activPAL in adults using the GGIR R-package. Int J Environ Res Public Health. 2023;20:2293.
PAL Technologies Ltd., PAL FAMILY. https://www.palt.com/pals/. Accessed 6 November 2023.
Migueles JH, Rowlands AV, Huber F, Sabia S, van Hees VT, GGIR. A research community–driven open source R package for generating physical activity and sleep outcomes from multi-day raw accelerometer data. J Meas Phys Behav. 2019;2:188–96.
Blume C, Santhi N, Schabus M. nparACT’ package for R: a free software tool for the non-parametric analysis of actigraphy data. MethodsX. 2016;3:430–5.
Howley ET, Bassett DR Jr, Welch HG. Criteria for maximal oxygen uptake: review and commentary. Med Sci Sports Exerc. 1995;27:1292–301.
Hiyoshi A, Fukuda Y, Shipley MJ, Bartley M, Brunner EJ. A new theory-based social classification in Japan and its validation using historically collected information. Soc Sci Med. 2013;87:84–92.
So R, Murai F, Fujii M, Watanabe S, Matsuo T. Association of sitting time and cardiorespiratory fitness with Cardiovascular Disease risk and healthcare costs among office workers. Ind Health. 2023;61:368–78.
Kokkinos P, Faselis C, Myers J, Sui X, Zhang J, Blair SN. Age-specific exercise capacity threshold for mortality risk assessment in male veterans. Circulation. 2014;130:653–8.
Dos Santos M, Ferrari G, Lee DH, Rey-López JP, Aune D, Liao B, et al. Association of the Weekend Warrior and other leisure-time physical activity patterns with all-cause and cause-specific mortality: a nationwide cohort study. JAMA Intern Med. 2022;182:840–8.
Fernström M, Fernberg U, Hurtig-Wennlöf A. The importance of cardiorespiratory fitness and sleep duration in early CVD prevention: BMI, resting heart rate and questions about sleep patterns are suggested in risk assessment of young adults, 18–25 years: the cross-sectional lifestyle, biomarkers and Atherosclerosis (LBA) study. BMC Public Health. 2020;20:1715.
Ten Brummelhuis LL, Calderwood C, Rosen CC, Gabriel AS. Is physical activity before the end of the workday a drain or a gain? Daily implications on work focus in regular exercisers. J Appl Psychol. 2022;107:1864–77.
Stevens ML, Crowley P, Holtermann A, Mortensen OS, Korshøj M. Cardiorespiratory fitness, occupational aerobic workload and age: workplace measurements among blue-collar workers. Int Arch Occup Environ Health. 2021;94:503–13.
Holtermann A, Hansen JV, Burr H, Søgaard K, Sjøgaard G. The health paradox of occupational and leisure-time physical activity. Br J Sports Med. 2012;46(4):291–5. https://doi.org/10.1136/bjsm.2010.079582.
Holtermann A, Schnohr P, Nordestgaard BG, Marott JL. The physical activity paradox in Cardiovascular Disease and all-cause mortality: the contemporary Copenhagen General Population Study with 104 046 adults. Eur Heart J. 2021;42(15):1499–511. https://doi.org/10.1093/eurheartj/ehab087.
Nakai M, Iwanaga Y, Sumita Y, Wada S, Hiramatsu H, Iihara K, et al. Associations among cardiovascular and cerebrovascular Diseases: analysis of the nationwide claims-based JROAD-DPC dataset. PLoS ONE. 2022;17:e0264390.
Jones MA, Diesel SJ, Gibbs BB, Whitaker KM. Concurrent agreement between ActiGraph and activPAL for measuring physical activity in pregnant women and office workers. J Meas Phys Behav. 2022;5:69–75.
Ridgers ND, Salmon J, Ridley K, O’Connell E, Arundell L, Timperio A. Agreement between activPAL and ActiGraph for assessing children’s sedentary time. Int J Behav Nutr Phys Act. 2012;9:15.
Pfister T, Matthews CE, Wang Q, Kopciuk KA, Courneya K, Friedenreich C. Comparison of two accelerometers for measuring physical activity and sedentary behaviour. BMJ Open Sport Exerc Med. 2017;3:e000227.
Radtke T, Rodriguez M, Braun J, Dressel H. Criterion validity of the ActiGraph and activPAL in classifying posture and motion in office-based workers: a cross-sectional laboratory study. PLoS ONE. 2021;16:e0252659.
Hidde MC, Lyden K, Broussard JL, Henry KL, Sharp JL, Thomas EA, et al. Comparison of activPAL and actiwatch for estimations of time in bed in free-living adults. J Meas Phys Behav. 2022;5:97–102.
Leister KR, Garay J, Barreira TV. Validity of a novel algorithm to detect bedtime, wake time, and sleep time in adults. J Meas Phys Behav. 2022;5:76–84.
Acknowledgements
We extend our gratitude to Hanae Kondou and Ari Nakamura for their dedicated efforts in the data collection. We thank the researchers and staff members of the National Institute of Occupational Safety and Health in Japan who offered funding and clerical support for this study. Moreover, the authors would like to thank Editage (www.editage.jp) for English-language editing.
Funding
This study was supported by Industrial Disease Clinical Research Grants from the Japanese Ministry of Health, Labour and Welfare (Grant numbers: 150903-01 and 180902-01). The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
JS, RS, and TM designed the research. RS, FM, and TM contributed to data collection. JS performed the formal analysis. JS wrote the first draft of the manuscript. JS, RS, FM, and TM substantially contributed to the interpretation of the results and provided feedback on the main manuscript. All authors revised the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All participants provided signed informed consent, and no monetary compensation was provided. This study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Ethics Committee of the National Institute of Occupational Safety and Health, Japan (Approval number: H2744).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
12889_2023_17580_MOESM1_ESM.docx
Additional file 1: Figure S1. Rest and activity pattern of the entire sample (n = 254) aggregated to a single 24-h period
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Seol, J., So, R., Murai, F. et al. Relationship between rest–activity rhythms and cardiorespiratory fitness in middle-aged workers: a cross-sectional study with non-parametric analysis using accelerometers worn on the thigh. BMC Public Health 24, 62 (2024). https://doi.org/10.1186/s12889-023-17580-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-17580-w