
Abstract
Since Otto Warburg made the first observation that tumor cells exhibit altered metabolism and bioenergetics in the 1920s, many scientists have tried to further the understanding of tumor bioenergetics. Particularly, in the past decade, the application of the state-of the-art metabolomics and genomics technologies has revealed the remarkable plasticity of tumor metabolism and bioenergetics. Firstly, a wide array of tumor cells have been shown to be able to use not only glucose, but also glutamine for generating cellular energy, reducing power, and metabolic building blocks for biosynthesis. Secondly, many types of cancer cells generate most of their cellular energy via mitochondrial respiration and oxidative phosphorylation. Glutamine is the preferred substrate for oxidative phosphorylation in tumor cells. Thirdly, tumor cells exhibit remarkable versatility in using bioenergetics substrates. Notably, tumor cells can use metabolic substrates donated by stromal cells for cellular energy generation via oxidative phosphorylation. Further, it has been shown that mitochondrial transfer is a critical mechanism for tumor cells with defective mitochondria to restore oxidative phosphorylation. The restoration is necessary for tumor cells to gain tumorigenic and metastatic potential. It is also worth noting that heme is essential for the biogenesis and proper functioning of mitochondrial respiratory chain complexes. Hence, it is not surprising that recent experimental data showed that heme flux and function are elevated in non-small cell lung cancer (NSCLC) cells and that elevated heme function promotes intensified oxygen consumption, thereby fueling tumor cell proliferation and function. Finally, emerging evidence increasingly suggests that clonal evolution and tumor genetic heterogeneity contribute to bioenergetic versatility of tumor cells, as well as tumor recurrence and drug resistance. Although mutations are found only in several metabolic enzymes in tumors, diverse mutations in signaling pathways and networks can cause changes in the expression and activity of metabolic enzymes, which likely enable tumor cells to gain their bioenergetic versatility. A better understanding of tumor bioenergetics should provide a more holistic approach to investigate cancer biology and therapeutics. This review therefore attempts to comprehensively consider and summarize the experimental data supporting our latest view of cancer bioenergetics.
Similar content being viewed by others


Introduction
Terrestrial organisms vary in many ways, but one characteristic common to all living organisms is the need for cellular energy. The universal energy currency is ATP. Eukaryotes ranging from yeast to humans generate ATP via glycolysis and oxidative phosphorylation. The term glycolysis comes from the Greek “glyco-,” meaning “sweet,” and “-lysis,” meaning “to split.” The name is apt, as the glycolytic pathway involves the splitting of sugar to produce ATP. Oxidative phosphorylation (OXPHOS) is so named because it combines inorganic phosphate with ADP to form ATP in the presence of oxygen. Human cells can use various fuels, including glucose, amino acids, and fat for ATP production to support cellular function and proliferation. Fuel usage for ATP generation is dependent on the conditions of the body. For example, in healthy, well-fed individuals, skeletal muscle is degraded and regenerated frequently. The amino acid pool in humans remains relatively unchanged. To keep the amino acid pool constant during starvation, the degradation of skeletal muscles increases. This occurs so that the body can continue to provide energy for essential functions. Glutamine and alanine constitute the majority of amino acids released from skeletal muscles during starvation. One consequence of unlimited cancer cell proliferation is likely to make the human body feel starved and respond in a way similar to the body’s response to starvation. Hence, it is conceivable that glutamine can be a preferred fuel for many types of cancer cells. The importance of glutamine in tumor metabolism and bioenergetics is further confirmed by recent metabolomics studies showing that α-ketoglutarate from glutamine can undergo reductive carboxylation to generate citrate, which can be turned into malate for generating NADPH via malic enzyme. This provides an alternative pathway for cancer cells to generate citrate and NADPH for sustaining anabolic reactions. Another noteworthy development in cancer bioenergetics research is the finding that stromal cells in the tumor microenvironment can provide cancer cells with bioenergetic substrates. Below, we consider previous and emerging research results and attempt to provide a holistic and up-to-date view of tumor bioenergetics.
Review
High glycolytic rates occur concomitantly with oxidative phosphorylation (OXPHOS) in cells of most tumors
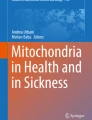
Glycolysis was first studied by Louis Pasteur in an attempt to understand the process of fermentation in 1856 [1]. Glycolysis as we understand it today was finalized by Buchner in 1947 [2]. Glycolysis consumes 2 ATP and produces 4 ATP for a net yield of 2 ATP (Fig. 1). In the absence of oxygen, glycolysis is the metabolic pathway of choice. In the presence of oxygen, however, glycolysis only begins the process of aerobic respiration. In the presence of oxygen, pyruvate is consumed by the tricarboxylic acid (TCA) cycle (Fig. 1). Albert Szent-Gyorgyi made major contributions elucidating the TCA cycle, also known as the Krebs cycle, in the 1920s and 1930s [3–7]. In 1945, coenzyme A was discovered by Fritz Lipmann [8]. However, the most important and well-known contributor to the discovery and understanding of the TCA cycle is Hans Krebs, who discovered that cycle began with citrate [9]. The TCA cycle does not produce ATP directly, although it produces 1 GTP, which is easily converted to ATP (Fig. 1). However, the TCA cycle is extremely important for energy production because it provides the precursor molecules, namely NADH and FADH2, for OXPHOS (Fig. 1). Breakthroughs in OXPHOS were made from 1944 to 1980, beginning with Dickens, McIlwain, Neuberger, Norris, Obrien, and Young and ending with Boyer [10–12]. OXPHOS is the preferred energy-generating method of many life forms, including mammals, in the presence of oxygen. This is because OXPHOS creates up to 38 ATP molecules per one molecule of glucose, as compared to only 2 ATP molecules generated anaerobically by glycolysis (Fig. 1). Both TCA cycle and OXPHOS occur in mitochondria.

The metabolic steps of glycolysis and TCA cycle. The steps involved in glycolysis and TCA cycle are demarcated separately. ATP/GTP utilization or synthesis is shown in green, while NAD+/NADH and FAD/FADH2 are shown in red. Also indicated are the numbers of NADH, FADH2, and ATP/GTP generated when one molecule of glucose is consumed following glycolysis, TCA cycle, and oxidative phosphorylation. Abbreviations: Glucose-6-P glucose 6-phosphate, Fructose-6-P fructose 6-phosphate, Fructose -1,6-bis-P fructose 1,6-bisphosphate, Dihydroxyacetone-P dihydroxyacetone phosphate, Glyceraldehyde-3-P glyceraldehyde 3-phosphate, 1,3-Bis-P-glycerate 1,3-bisphosphoglycerate, 3-P-Glycerate 3-phosphoglycerate, 2-P-Glycerate 2-phosphoglycerate, OXPHOS oxidative phosphorylation
How cancer cells gain sufficient ATP to support their unabated proliferation and function has fascinated many scientists for nearly a century. The German scientist Otto Warburg and co-workers performed the first quantitative study of cancer cell metabolism in the 1920s [13, 14]. They showed that tumor tissues metabolize approximately tenfold more glucose to lactate in a given time than normal tissues, even when presented with enough oxygen to metabolize glucose completely to CO2. This phenomenon is widely known as the Warburg effect and is the origin of the perception that a high glycolytic rate is typical of cancer/tumor cells [15]. The rationale for the high glycolytic rate was that tumor mitochondria have impaired respiration, which is compensated by an unusually high contribution of aerobic glycolysis to sustain ATP generation. The hallmark of aerobic glycolysis is a high rate of lactate production from glucose in the presence of oxygen. Warburg’s observation has motivated generations of cancer biologists and biochemists to refine his hypothesis and provide mechanistic explanations for it.
However, immediately after the publication of Warburg’s paper “On the Origin of Cancer Cells” [15], Weinhouse contested Warburg’s ideas based on results in his laboratory showing that neoplastic tissues have a normal OXPHOS (oxidative phosphorylation) capacity when supplemented with NAD+ [16, 17]. In 1979, Reitzer and co-workers showed that in cultured HeLa cells, more than half of the ATP requirement (determined by comparing 14CO2 production from 14C-glutamine and 14C-lactate production from 14C-glucose) comes from glutamine even when a high concentration (10 mM) of glucose is present [18]. When fructose or galactose is the carbohydrate, glutamine provides greater than 98 % of energy by aerobic oxidation from the TCA cycle. Experimental studies in recent years have confirmed the idea that glutamine is a major nutrient in cancer cells [19–22]. Additionally, ample experimental evidence showed that glutamine is a good substrate for oxidative metabolism in various tumor and cancer cells [23–26]. It is also worth noting that the authors’ lab recently showed that glutamine enables an array of non-small cell lung cancer (NSCLC) cells to increase oxygen consumption substantially when glucose is depleted [27]. Taken together, various studies have shown that glucose and glutamine are key nutrients and fuels for cancer cells [21, 28]. Different cancer cells may exhibit varying dependence on glucose or glutamine [29, 30].
Both glucose and glutamine are important nutrients for many types of cancer cells and tumors
The importance of glutamine as a nutrient and fuel is consistent with the fact it is the most abundant amino acid released from skeletal muscle, and it is the most abundant amino acid in plasma [31]. The importance of glucose and glutamine in cancer metabolism and bioenergetics can be easily gleaned from the architecture of metabolic pathways (Fig. 2). Both glucose and glutamine have dual roles in ATP production and biosynthesis (anabolism). Although glucose can generate ATP via glycolysis, its most prominent function is evidently in anabolism (biosynthesis). As shown in Fig. 2, glucose can generate the precursor ribulose-5-P and the reducing power NADPH via the pentose phosphate pathway. The glycolysis intermediate glyceraldehyde 3-P can yield glycerol-3-P, which serves as a backbone for the synthesis of phosphatidic acid, a precursor for the synthesis of triacylglycerol and phospholipids. Another glycolysis intermediate, 3-P glycerate, is a precursor for serine, which can be used to synthesize ceramide and is a precursor for one-carbon metabolism. Ultimately, pyruvate generated from glucose via glycolysis can be turned into Acetyl CoA and serves as a substrate feeding the TCA cycle. Under conditions permitting mitochondrial respiration, NADH and FADH2 generated from the TCA cycle will lead to high yield of ATP, via the electron transport chain and OXPHOS (Fig. 1).

Metabolic fuels for tumor cells. Tumor cells are able to use a variety of bioenergetic substrates, including glutamine, glucose, fatty acids (FA), ketone bodies, and acetate (highlighted by red boxes). These substrates can be provided by stromal cells in the microenvironment. Much of the cellular energy for tumor cells is likely generated by TCA cycle coupled to oxidative phosphorylation. The pathways for the generation and metabolism of these substrates are outlined. Notably, glutamine and glucose can also provide building blocks for the synthesis of many biomolecules. Also indicated in pink are the metabolic enzymes whose mutations are found in various tumors and the accumulated oncometabolites in these tumors
Glutamine is a very versatile nutrient feeding into many pathways for ATP generation, redox homeostasis, and biosynthesis [22]. Firstly, glutamine is the main substrate supporting TCA cycle anaplerosis. Glutamine can be readily turned into α-ketoglutarate, which feeds the TCA cycle (Fig. 2), leading to the generation of NADH and FADH2, which is used to generate ATP via electron transport and OXPHOS (Fig. 1). This can lead to the generation of various TCA cycle intermediates, which can support many biosynthetic reactions and gluconeogenesis. Secondly, under hypoxic conditions or when mitochondria are defective, α-ketoglutarate from glutamine can undergo reductive carboxylation to generate citrate, providing a mechanism to sustain anabolic reactions [32–34] (Fig. 2). Additionally, citrate generated in this way can be turned into malate, which provides another mechanism to generate NADPH via malic enzyme 1 [35, 36]; (Fig. 2).
Cancer cells also exhibit an increased demand for fatty acids, besides glucose and glutamine [37, 38]. Fatty acids can be synthesized endogenously (Fig. 2) or taken up from exogenous sources. In prostate tumors, which import less glucose than other tumors [39], β-oxidation of fatty acids provides an important energy source [40, 41]. Additionally, two recent studies showed that acetate is a bioenergetic substrate for glioblastoma and brain metastases, and it is important for biosynthesis and histone modification in a wide spectrum of tumors [42, 43]. Overall, metabolic phenotypes in cancer cells are plastic, and cancer cells exhibit greater plasticity than normal cells [44].
Stromal cells and adipocytes can provide building blocks and fuels to tumor cells
Like other aspects of cancer biology, our understanding of tumor metabolism is continuously evolving. Particularly in recent years, some researchers have investigated tumor metabolism in the context of the whole tumor microenvironment. These studies suggest a two-compartment model for understanding tumor metabolism [45–49]. In this model, under the education of cancer cells and inflammatory cytokines, stromal cells and adipocytes become “food donors.” Tumor stromal cells principally include cancer-associated fibroblasts (CAFs), tumor endothelial cells (TECs), and tumor-associated macrophages (TAMs). Catabolism in stromal cells and adipocytes provides fuels and building blocks (see Fig. 2) for the anabolic growth of cancer cells via metabolic coupling [48, 49]. For example, by examining MCF7 breast cancer cells cultured alone or co-cultured with nontransformed fibroblasts, Ko et al. showed that CAFs undergo an autophagic program, leading to the generation and secretion of high glutamine levels into the tumor microenvironment [50]. The glutamine released from CAFs fuel cancer cell mitochondrial activity, driving a vicious cycle of catabolism in the tumor stroma and anabolic tumor cell expansion. Likewise, Nieman et al. showed that triglyceride catabolism in adipocytes drives ovarian cancer metastasis by providing fatty acids as mitochondrial fuels [51]. Furthermore, a study by Sotgia et al. suggested that glycolytic stromal cells produce mitochondrial fuels, L-lactate and ketone bodies, which are transferred to oxidative epithelial cancer cells, driving OXPHOS and mitochondrial metabolism [52]. This is strongly supported by their finding that metastatic breast cancer cells amplify OXPHOS and that adjacent stromal cells are glycolytic and lack detectable mitochondria. In essence, these observations and the two-compartment model are still consistent with Warburg’s original observation that tumors show a metabolic shift towards aerobic glycolysis.
The metabolic enzymes found to be mutated in tumors include isocitrate dehydrogenase, succinate dehydrogenase, and fumarate hydratase
With the increased interest in tumor metabolism in recent years, mutations in metabolic enzymes have been intensely studied. To date, the metabolic mutations associated with cancer are found mainly in isocitrate dehydrogenase (IDH), succinate dehydrogenase (SDH), and fumarate hydratase (FH). IDH catalyzes the oxidative decarboxylation of isocitrate to produce α-ketoglutarate (α-KG). In humans, there are three different IDH isoforms: IDH1, IDH2 and IDH3 (Fig. 2). IDH1 is located in the cytosol and peroxisomes, while IDH2 and IDH3 are located in mitochondria. IDH1 and IDH2 use NADP+ as a cofactor, while IDH3 uses NAD+ as a cofactor in the TCA cycle for energy metabolism [53, 54]. All three enzymes convert isocitrate to α-KG.
In 2008, the R132H IDH1 mutation was first found in human glioblastoma multiforme [55]. Subsequently, mutations of the R132 residues were found in leukemic cells of myeloid leukemia (AML) patients [56]. These findings were quickly confirmed by multiple studies involving direct sequencing of IDH1 and its homologue IDH2. Mutations in IDH1 and IDH2 were found in 75 % of grade 2–3 gliomas and secondary glioblastoma, and in about 20 % of AML [57–69]. Additionally, IDH1 and IDH2 mutations were found in several other human tumors, including cartilaginous tumors (75 %), intrahepatic cholangiocarcinoma (10 %), and thyroid carcinomas (16 %) [70–77]. The most common cancer mutations map to single arginine residues in the catalytic pockets: IDH1 (R132) and IDH2 (R172 or R140) [55, 56, 61]. Mutant IDH1/2 forms a dimer with the wild-type protein from the normal allele and displays a neomorphic activity that allows the heterodimeric enzyme to catalyze the reduction of α-KG directly to D-2-hydroxyglutarate (D-2-HG, also known as R-2-HG) in the presence of NADPH [65, 69, 78, 79]. In human glioma with IDH1/2 mutation, the level of D-2-HG accumulates as high as 5–35 mmol L−1 [63, 79, 80].
SDH is a highly conserved protein complex with four subunits: SDHA, SDHB, SDHC, and SDHD. SDHA and SDHB are catalytic subunits, and SDHC and SDHD are ubiquinone-binding and membrane-anchorage subunits. SDH functions in the TCA cycle, and as complex II of the electron transport chain (ETC), catalyzes the oxidation of succinate to fumarate in a reaction that generates FADH2, and donates electrons to the ETC. Mutations in genes encoding SDH subunits and the SDH assembly factor 2 are found in hereditary paraganglioma and pheochromocytoma, as well as in gastrointestinal stromal tumors, renal tumors, thyroid tumors, testicular seminomas, and neuroblastomas [81]. Over 650 reported cases of SDH mutations have been reported, and these mutations significantly reduce SDH activity. In three cases of paragangliomatosis with SDH mutation, succinate accumulated to a high level of 364–517 μmol g−1 protein [82]. Also, Xiao et al. showed that depleting SDH in mice or ectopic expression of tumor-derived SDH mutants resulted in the accumulation of succinate [83].
FH exists as a homotetrameric enzyme that catalyzes the stereospecific and reversible hydration of fumarate to malate. Mutations in the FH gene were first identified in inherited uterine fibroids, skin leiomyoma, and papillary renal cell cancer by a combination of mapping methods [84]. FH mutations were also found in cerebral cavernomas, Leydig cell tumors, and ovarian mucinous cystadenoma with low frequency [85–87]. Over 300 cases of FH mutations have been reported. Like SDH mutations, FH mutations significantly reduce FH activity, resulting in the accumulation of fumarate to a level as high as 417–688 μmol/g protein in hereditary leiomyomatosis and renal cell cancer [82]. The accumulation of fumarate was also observed in cells depleted for FH or expressing a tumor-derived FH mutant [83].
The accumulation of D-2-HG, succinate, and fumarate all lead to impaired activity of a class of enzymes called α-KG-dependent dioxygenases. These oxygenases include prolyl hydroxylase (PHD), which causes HIF1α degradation [88]. Hence, the accumulation of D-2-HG, succinate, and fumarate causes HIF1α accumulation. Other α-KG-dependent dioxygenases include the JMJD family KDMs and the TET family of 5mC hydroxylases, which impact epigenetic events [89]. Ultimately, by impacting cellular processes such as hypoxia response and epigenetic modifications, D-2-HG, succinate, and fumarate promote tumorigenesis. Such metabolites whose abnormal accumulation causes both metabolic and nonmetabolic dysregulation and promotes tumorigenesis are often called oncometabolites. However, there is only limited evidence linking these oncometabolites to metastatic progression. For example, treatment with dimethylfumarate, a cell-permeable form of fumarate, strongly reduces invasion and metastasis formation in melanoma [90–92], although overexpression of FH in a FH-deficient renal cell carcinoma line inhibits cellular migration and invasion [93].
Mitochondrial OXPHOS is essential for ATP generation in most tumor types
As discussed above, mutations in IDH, SDH, and FH may interfere with mitochondrial function and respiration in certain rare tumor types. However, a plethora of studies have shown that mitochondrial function and respiration are critical for many common types of tumors. Over the years, various studies have identified several modes of mitochondrial function in tumorigenesis. For example, mitochondria and cancer are linked through the generation of reactive oxygen species (ROS). Notably, mitochondria generate much of the endogenous cellular ROS through mitochondrial OXPHOS. Under normal physiological conditions, ROS production is highly regulated, at least in part, by complex I [94–98]. When the electron transport chain (ETC) is inhibited by an OXPHOS gene mutation, the ETC electron carriers accumulate excessive electrons, which can be passed directly to O2 to generate superoxide anion (O2 −). The O2 − generated by complex I is released into the mitochondrial matrix and is converted to H2O2 by the mitochondrial manganese superoxide dismutase (MnSOD). The O2 − generated from complex III is released into the mitochondrial intermembrane space and is converted to H2O2 by copper/zinc superoxide dismutase (Cu/ZnSOD). Mitochondrial H2O2 can then diffuse into other cellular compartments. Mitochondrial ROS are important signaling molecules and potent mitogens [99–101]. Increased production of ROS has long been observed to be a hallmark of many tumors and cancer cell lines [102, 103]. The mechanisms by which ROS promote tumorigenesis have been reviewed extensively elsewhere [95, 104, 105]. Additionally, it is well known that ROS can inhibit tumor progression by inducing apoptosis, and many anti-cancer agents act by generating ROS and inducing cancer cell death [106, 107]. However, this is beyond the scope of this review and is therefore not discussed further here.
Another link of mitochondria to tumorigenesis is OXPHOS. Although it has long been believed that the glycolytic phenotype in cancer is due to defective mitochondrial OXPHOS, as proposed by Otto Warburg [15], this view has been challenged since it was proposed [17]. Many lines of experimental evidence have shown that the function of mitochondrial OXPHOS in most tumors is intact. For example, Guppy and co-workers showed that in the MCF-7 breast cancer cell line, ATP production is 80 % oxidative and 20 % glycolytic [108]. Rodriguez-Enriquez et al. showed that in AS-30D hepatoma tumor cells, cellular ATP is mainly provided by OXPHOS [109]. Furthermore, Rodriguez-Enriquez et al. showed that in both human HeLa and rodent AS-30D fast-growing tumor cells, mitochondria respiration is the predominant source of ATP in both cell types (66–75 %), in spite of an active glycolysis [110]. In glucose-free medium with glutamine, proliferation of both lines is diminished by 30 %, but OXPHOS and the cytosolic ATP level are increased by 50 %. In glutamine-free medium with glucose, proliferation, OXPHOS, and ATP concentration are diminished drastically. In 2004, Zu and Guppy reviewed a plethora of experimental studies regarding glycolytic and oxidative contribution to ATP production in a wide array of tumor cells [111]. Their analyses of previous data showed that the vast majority of tumor cells generate ATP via oxidative phosphorylation.
Notably, a recent study has linked OXPHOS to oncogene ablation-resistant pancreatic cancer cells [112]. Viale et al. showed that a subpopulation of dormant tumor cells surviving oncogene ablation, responsible for tumor relapse, relies on OXPHOS for survival. Furthermore, recent experimental studies have identified transcription factors that promote mitochondrial biogenesis and OXPHOS in cancer cells. For example, LeBleu and co-workers identified the transcription coactivator peroxisome proliferator-activated receptor gamma, coactivator 1alpha (PPARGC1A or PGC-1α) as the transcription factor promoting mitochondrial biogenesis and OXPHOS in cancer cells [113]. They showed that migratory/invasive cancer cells favor mitochondrial respiration and increased ATP production. There is a strong correlation between PGC-1α expression in invasive cancer cells and the formation of distant metastases. In another study, Mauro et al. showed that NF-κB plays a role in metabolic adaptation in cancer by upregulating OXPHOS [114].
Mitochondrial transfer provides a mechanism for restoring OXPHOS in tumor cells defective in mitochondrial respiration and for promoting tumor progression
Importantly, a recent study involving mtDNA transfer between normal and tumor cells provided further evidence supporting the importance of OXPHOS in cancer progression [115]. Tan et al. showed that tumor cells without mitochondrial DNA (mtDNA) exhibit delayed tumor growth and that tumor formation is associated with the acquisition of mtDNA from host cells [115]. By following mtDNA acquisition in the 4T1 breast carcinoma model, Tan and colleagues found that stable cell lines derived from primary subcutaneous tumors that grew from 4T1ρ0 cells showed partial recovery of mitochondrial respiration and an intermediate lag to tumor growth. Cell lines from circulating tumor cells and from lung metastases showed further and staged recovery of mitochondrial respiration, and tumor growth more similar to that of parental 4T1 cells. They demonstrated that restored mitochondrial respiration is critical for the tumorigenic potential of cancer cells without mtDNA [115]. Interestingly, the role of mitochondrial transfer has been observed in canine transmissible venereal tumor (CTVT), which is a highly adapted cancer and is transmitted as an allograft during coition [116]. Rebbeck et al. analyzed mtDNA in 37 transmissible venereal tumors in dogs and comparable mtDNA regions from 15 host animals and 43 published canine mtDNA sequences [117]. Their analyses suggested that these tumors have periodically acquired mitochondria from their hosts, perhaps over a period of 11,000 years when this tumor type originated [116, 117]. It was estimated that the transfer of mitochondria into malignant cells with heavily mutated mtDNA occurs once in about 100 years [117]. Clearly, ample experimental evidence exists to demonstrate the importance of mitochondrial respiration in the progression of many cancers.
Heme is an essential factor for the proper functioning of OXPHOS complexes and directly regulates many molecular and cellular processes
Mitochondrial respiration is carried out by the OXPHOS complexes I–V (Fig. 3) [118]. Complex I, the NADH-coenzyme Q reductase or NADH dehydrogenase, is constituted of 45 polypeptides, of which seven (ND-1, -2, -3, -4, -4L, -5, and -6) are encoded by the mtDNA, and the rest are encoded by nuclear DNA [119, 120]. Complex II, succinate-coenzyme Q reductase or succinate dehydrogenase, contains four nDNA-encoded protein subunits. Complex III, cytochrome bc1 complex or ubiquinol-cytochrome c oxidoreductase, contains 11 subunits, of which one (cytochrome b) is encoded by the mtDNA. Complex IV, cytochrome c reductase, is composed of 13 subunits, of which three (CO-I, -II, and -III) are from the mtDNA. Complex V, ATP synthase, contains approximately 16 subunits, of which two (ATP-6 and -8) are from the mtDNA. Complexes I, III, IV, and V retain mtDNA-encoded protein subunits and transport protons (Fig. 3). Importantly, three complexes, II, III, and IV, require heme for proper functioning. Particularly, multiple subunits in complexes III and IV require heme as a prosthetic group, and different forms of heme are present (Fig. 3) [121].

The function and composition of mitochondrial OXPHOS complexes I–V. Shown here are the directions of electron and proton transport by the OXPHOS complexes. Also indicated are the origins of DNA encoding the subunits and the hemes needed for complexes II–IV. nDNA nuclear DNA, mtDNA mitochondrial DNA
The function of heme as a prosthetic group in proteins and enzymes involved in the transport, storage, and utilization of oxygen is well-known [122]. Furthermore, heme directly regulates the expression of proteins and enzymes involved in using oxygen [123]. In humans, heme plays essential roles in many physiological processes, including erythropoiesis, neurogenesis, cell growth and differentiation [123–125]. Heme constitutes 95 % of functional iron in the human body, as well as two-thirds of the average person’s iron intake in developed countries. In the human body, erythroid and hepatic cells use the most heme. Most, if not all, human cells need a basal level of heme for survival. Mammalian cells can synthesize heme endogenously in the mitochondria, or they can import heme from the circulation via heme transporters (Fig. 4) [ [126] and references therein]. In mammalian cells, intracellular heme is used to synthesize various hemoproteins, such as cytochromes, or it can be degraded by heme oxygenase (Fig. 4) [127]. It is also worth noting that heme can serve as a regulatory and signaling molecule and directly regulate transcription, translation, and cell growth and differentiation [125]. For example, in erythroid precursor cells, heme regulates the transcription of globin chains and heme oxygenase genes by modulating the activity of transcriptional regulators, such as NF-E2 and Bach1 [128–131]. Additionally, heme regulates the translation of globin chains by directly controlling the activity of the heme-regulated eIF-2α kinase (HRI) [132, 133]. These mechanisms ensure the coordination of globin chain synthesis with heme synthesis. In neuronal cells, heme can modulate the activity of the NMDA receptor and the Ras-ERK1/2 signaling pathway [134–137]. Furthermore, heme directly regulates the activity of the nuclear receptors REV-ERBα and REV-ERBβ [138, 139], microRNA processing protein DiGeorge critical region-8 (DGCR8) [140], and ion channels (SloBK potassium channel and epithelial sodium channel ENaCs) [141–143], in an array of mammalian cells (Fig. 4).

The signaling and structural functions of heme in human cells. Human cells can synthesize heme de novo in mitochondria (the first and rate-limiting enzyme is ALAS, 5-aminolevulinate synthase) or import heme via heme transporters, such as HRG1 and HCP1. Inside cells, heme serves as a prosthetic group in numerous enzymes and proteins that transport, store, or use oxygen, such as mitochondrial cytochromes and cytochrome P450. Additionally, heme directly regulates the activity of diverse cellular signaling and regulatory molecules, such as Bach1, Rev-ERBα, and Rev-ERBβ (transcriptional regulators), as well as DGCR8 (an essential miRNA processing factor) in the nucleus. Heme also regulates HRI (the heme-regulated inhibitor kinase controlling protein synthesis) and the Ras-ERK signaling pathway in the cytoplasm. Furthermore, heme regulates the activity of the NMDA receptor, the SloBK potassium channel, and the ENaCs sodium channel on the cell membrane
Elevated heme flux and function are critical for the proliferation and function of non-small cell lung cancer cells
Interestingly, it has long been observed that inhibiting heme synthesis in various cancer cell lines suppresses cell proliferation and induces apoptosis [144–146]. However, it is not clear how heme deficiency impacts normal cells. This was clarified recently by a study carried out in the authors’ laboratory [147]. In this study, we took advantage of a matched pair of cell lines representing the normal, nonmalignant bronchial epithelial and non-small cell lung cancer (NSCLC) cells developed from the same patient [148, 149]. Using this pair of cell lines and several other NSCLC lines, we examined the differences in bioenergetic activities in normal and cancer cells. We found that the rates of both glucose and oxygen consumption in NSCLC cells are elevated, with the elevation of oxygen consumption greater than glucose consumption [147]. Next, we showed that the rate of heme synthesis is increased significantly in the NSCLC cells, compared to the normal lung cells. Additionally, we showed that the expression level of the rate-limiting heme synthetic enzyme, ALAS1, is highly elevated in NSCLC cells and tumors. Further, the levels of two heme transporters HCP1 and HRG1 [150, 151] are dramatically increased in NSCLC cells and tumors, compared to the normal cells [147]. The increased availability of heme is expected to intensify the production of oxygen-utilizing hemoproteins. Indeed, we found that the levels of cytoglobin, cytochrome c, cytochrome P450 CYP1B1, and Cox-2 are significantly increased in NSCLC cells and tumors [147]. Our results revealed that both heme biosynthesis and uptake are intensified to enhance heme availability for the production of oxygen-utilizing hemoproteins in cancer cells and xenograft tumors [147].
Increased levels of heme and oxygen-utilizing hemoproteins presumably contribute to intensified oxygen consumption in cancer cells. Conversely, depleting heme in cancer cells is expected to cause a lack of hemoproteins, leading to reduced oxygen consumption and cellular energy generation. Indeed, we found that oxygen consumption in the NSCLC cells is selectively reduced when cells are cultured in heme-depleted medium [147]. In contrast, heme depletion in the medium does not affect oxygen consumption in normal cells. Further, we showed that lowering heme levels strongly suppresses NSCLC cell proliferation, colony formation, and migration [147]. Together, our results showed that heme availability is significantly increased in cancer cells and tumors, which leads to elevated production of hemoproteins, resulting in intensified oxygen consumption and cellular energy production for fueling cancer cell progression [147].
The selective importance of heme in tumor cell proliferation and function is also consistent with the previous observation that NSCLC cells require serum (containing heme) for maintenance and proliferation, whereas the normal lung cells survive and proliferate better with growth factors in the absence of serum [148, 149]. Further, the preferential requirement of NSCLC cells for heme is in complete agreement with the critical roles of heme in mitochondrial respiratory chain complexes. As shown in Fig. 4, OXPHOS complexes II, III, and IV all require heme for proper functioning. By logical reasoning, tumor cells that depend mainly on OXPHOS for ATP generation should require elevated levels of heme and hemoproteins for proliferation and function.
Clonal evolution and genetic heterogeneity likely contribute to the remarkable versatility of tumor cells in the use of bioenergetic substrates
In recent years, whole-genome and whole-exome sequencing studies have provided an ever-expanding survey of somatic aberrations in cancers [152–156]. Such large-scale sequencing studies have revealed a high degree of genetic heterogeneity among patients with the same type of cancer, namely inter-tumor heterogeneity, and that within a single tumor or sample, namely intra-tumor heterogeneity [157–165]. For example, Gerlinger et al. found that over half the mutations in primary tumor and its various metastases of the same advanced renal cell carcinoma are different [166]. Likewise, several groups have demonstrated the vast heterogeneous mutational landscape of pancreatic cancer by analyzing data from whole-genome and whole-exome sequencing [167–169]. Additionally, Ellsworth et al. found genomic heterogeneity within primary breast carcinomas and among regional LN metastases [170]. They concluded that metastasis is a complex process influenced by primary tumor heterogeneity and variability in the timing of dissemination. Furthermore, Leiserson et al. performed a pan-cancer analysis of mutated networks in 3281 samples from 12 cancer types from the Cancer Genome Atlas (TCGA) [171]. They identified 16 significantly mutated subnetworks that comprise well-known cancer signaling pathways as well as subnetworks with less characterized roles in cancer, including cohesin, condensin, and others. In a comprehensive review, Vogelstein et al. summarized the genes altered in a high percentage of tumors and a much larger number of genes altered infrequently [163]. They reported ~140 driver genes whose intragenic mutations can promote or drive tumorigenesis. These driver genes can be classified into 12 signaling pathways that regulate three core cellular processes: cell fate, cell survival, and genome maintenance.
Data from these large-scale cancer genome sequencing studies also support clonal evolution as the mechanism responsible for generating intra-tumor heterogeneity (ITH). Clonal evolution was initially proposed by Nowell [172]. It refers to the process in which cancer cells accumulate genetic and epigenetic changes over time, giving rise to new subclones. It suggests that cancer evolves by a process of clonal expansion, diversification, and selection within the tissue ecosystems. Clonal evolution can be linear evolution or branched evolution [158, 159]. Evidence of clonal evolution is found in many tumors. For example, evaluation of genomic heterogeneity within primary breast carcinomas and among axillary LN metastases indicated that multiple clonal cell lineages exist in every primary tumor and between many metastatic deposits from the same patient [170]. Two recent studies revealed substantial intra-tumoral heterogeneity within lung adenocarcinomas [173, 174]. Cancer evolution and tumor heterogeneity likely contribute to tumor recurrence and the emergence of drug-resistant disease [175–177]. Under therapeutic pressure, those tumor clones that are most adaptive or resistant to treatment will be selected. These clones will then dominate and populate the tumor rendering it highly resistant to the given therapy. Further, some of these resistance pathways lead to multidrug resistance, generating an even more difficult clinical problem to overcome. Likewise, high mutational heterogeneity and subclonal mutation fraction can lead to increased likelihood of tumor recurrence.
Very likely, changes in tumor cell bioenergetic characteristics accompany tumor progression, recurrence, and drug resistance. Tumor cells are remarkably versatile in their ability to adapt to and take advantage of the environment to support their proliferation and function. Firstly, tumor cells use a variety of fuels, including glucose, glutamine, fatty acids, ketone bodies, and acetate [37–43]. Secondly, tumor cells from the same type of tumors can exhibit great variations in metabolic and bioenergetic phenotypes. Notably, different NSCLC cell lines exhibit a wide range of dependence on glutamine [30]. These cell lines also show a varying degree of increased oxygen consumption rates, as well as heme synthesis and uptake rates. Evidently, tumor cells adapt to the environment and adopt specific bioenergetic features in order to take advantage of whatever fuels are available. For example, tumor cells in an environment rich in adipocytes would likely adapt to preferentially use fatty acids, while tumor cells in an environment rich in myocytes may adapt to preferentially use glutamine. Clonal evolution enables different tumor cells to adopt metabolic and bioenergetic phenotypes fit to their environment. Such variations in tumor bioenergetic characteristics are likely underpinned by genetic heterogeneity. That is, the aforementioned diverse mutations in signaling pathways and networks would ultimately impact the expression and activity of metabolic enzymes, thereby enabling tumor cells to adopt specific bioenergetic features fit for their unique environment.
Conclusions
Recent advances in cancer research have clarified many issues relating to tumor bioenergetics. Some important points include the following: (1) High glycolytic rates in tumors and mitochondrial respiration often operate simultaneously in tumors. Increased glycolysis most likely contributes building blocks for biosynthesis. (2) Glutamine is the preferred oxidative fuel for tumor cells. (3) Tumor cells can use a range of fuels including glucose, glutamine, fatty acids, and acetate. (4) Mutations in metabolic enzymes are found mainly in three enzymes involved in the TCA cycle. (5) Mitochondrial respiration can be restored by mitochondrial transfer in tumor cells defective in OXPHOS, and it is critical for the initiation and metastasis of diverse tumors. (6) Elevated heme flux and function lead to intensified oxygen consumption in NSCLC cells, fueling cancer cell proliferation, migration, and colony formation. (7) Lowered heme availability selectively diminishes the proliferation and function of NSCLC cells. (8) Clonal evolution contributes to a high degree of genetic heterogeneity in tumors, which likely underpin metabolic and bioenergetic versatility of tumor cells, as well as tumor recurrence and drug resistance. Evidently, clonal evolution likely enables NSCLC cells to enhance heme synthesis and uptake, in order to increase their cellular energy generation. Heme coordinates the production and function of OXPHOS complexes. Hence, increasing heme availability provides an effective way to upregulate OXPHOS complexes and mitochondrial respiration for energy generation. It is likely that this mechanism involving elevated heme flux and function operates in other types of tumors besides NSCLC tumors to promote tumor development and progression.
Recent research has also provided ample evidence showing that many types of tumors indeed consume larger amounts of glucose, compared to normal tissues, as Warburg originally observed [15]. However, his hypothesis that tumor mitochondria have impaired respiration is largely incorrect for most types of tumors, as discussed extensively in this review. The observed large increases in glucose consumption in tumor tissues can be attributed to increased demand for building blocks in tumor cells and to increased glucose consumption in stromal cells, which in turn provide oxidative fuels, such as lactate, to tumor cells. Nonetheless, Warburg’s original observation has motivated generations of scientists to better understand tumor bioenergetics, and this will undoubtedly lead to a more holistic approach in cancer research and therapeutics.
Change history
02 March 2018
In this Correction, the authors would like to acknowledge that the original publication of the article “A holistic view of cancer bioenergetics: mitochondrial function and respiration play fundamental roles in the development and progression of diverse tumors” [1] was supported by CPRIT (Cancer Prevention & Research Institute of Texas) Grant RP160617.
Abbreviations
- ALAS1:
-
5′-aminolevulinate synthase 1
- ETC:
-
electron transport chain
- HCP1:
-
heme carrier protein 1
- HIF1α:
-
hypoxia-inducible factor 1α
- HRG1:
-
heme-responsive gene 1
- HRI:
-
heme-regulated eIF-2α kinase
- IDH:
-
isocitrate dehydrogenase
- NMDA:
-
N-methyl-D-aspartate
- NSCLC:
-
non-small cell lung cancer
- OXPHOS:
-
oxidative phosphorylation
- ROS:
-
reactive oxygen species
- SDH:
-
succinate dehydrogenase
References
Pasteur L (1860) Mémoire sur la Fermentation Alcoolique. Imprimerie de Mallet-Bachelier, Paris
Buchner T (1947) Uber ein phosphat ubertragendes Garungsferment. Biochim Biophys Acta 1:292–314
von Szent-Gyorgyi A (1925) Zellatmung IV. Mitteilung: Uber den Oxydationsmechanismus der Kartoffeln. Biochemische Zeitschrift 162:399–412
von Szent-Gyorgyi A (1927) Zellatmung V. Mitteilung: Uber den Oxydationsmechanismus einiger Pflanzen. Biochemische Zeitschrift 181:425–432
Gozsy B, Szent-Gyorgyi A (1934) Uber den Mechanismus der Hauptatmung des Taubenbrustmuskels. Hoppe-Seyler’s Zeitschrift fur physiologische Chemie 224(1–2):1–10
Annau E, Banga I, Gozsy B, Huszak St, Laki K, Straub FB, Szent-Gyorgyi A (1935) Uber die Bedeutung der Fumarsaure fur die Tierische Gewebsatmung: Einleitung Ubersicht Methoden. Hoppe-Seyler’s Zeitschrift fur physiologische Chemie 236(1):1–20
Annau E, Banga I, Blazso A, Bruckner V, Laki K, Straub FB, Szent-Gyorgyi A (1936) Uber die Bedeutung der Fumarsaure fur die Tierische GewebsatmungEinleitung, Ubersicht, Methoden III Mitteilung. Hoppe-Seyler’s Zeitschrift fur physiologische Chemie 244:105–116
Lipmann F (1953) On chemistry and function of coenzyme A. Bacteriol Rev. 17(1):1–16
Krebs HA (1940) The citric acid cycle and the Szent-Gyorgyi cycle in pigeon breast muscle. Biochem J 34(5):775–779
Dickens F, McIlwain H, Neuberger A, Norris FW, O’Brien JRP, Young FG (1944) Biochemistry. Annu Rep Prog Chem 41:230–271. doi:10.1039/AR9444100230
Boyer PD, Ariki M (1980) 18O-probes of phosphoenzyme formation and cooperativity with sarcoplasmic reticulum ATPase. Fed Proc. 39(7):2410–2414
Boyer PD, Cross RL, Momsen W (1973) A new concept for energy coupling in oxidative phosphorylation based on a molecular explanation of the oxygen exchange reactions. Proc Natl Acad Sci 70(10):2837–2839
Koppenol WH, Bounds PL, Dang CV (2011) Otto Warburg’s contributions to current concepts of cancer metabolism. Nat Rev Cancer 11(5):325–337
Warburg O, Wind F, Negelein E (1927) The metabolism of tumors in the body. J Gen Physiol 8(6):519–530
Warburg O (1956) On the origin of cancer cells. Science 123(3191):309–314
Wenner CE, Weinhouse S (1953) Metabolism of neoplastic tissue III Diphosphopyridine nucleotide requirements for oxidations by mitochondria of neoplastic and non-neoplastic tissues. Cancer Res 13(1):21–26
Weinhouse S (1956) On respiratory impairment in cancer cells. Science 124(3215):267–269
Reitzer LJ, Wice BM, Kennell D (1979) Evidence that glutamine, not sugar, is the major energy source for cultured HeLa cells. J Biol Chem 254(8):2669–2676
Anastasiou D, Cantley LC (2012) Breathless cancer cells get fat on glutamine. Cell Res 22(3):443–446
DeBerardinis RJ, Cheng T (2010) Q’s next: the diverse functions of glutamine in metabolism, cell biology and cancer. Oncogene 29(3):313–324
Ward PS, Thompson CB (2012) Metabolic reprogramming: a cancer hallmark even warburg did not anticipate. Cancer Cell 21(3):297–308
Hensley CT, Wasti AT, DeBerardinis RJ (2013) Glutamine and cancer: cell biology, physiology, and clinical opportunities. J Clin Invest. 123(9):3678–3684
Kovacevic Z, Morris HP (1972) The role of glutamine in the oxidative metabolism of malignant cells. Cancer Res 32(2):326–333
Lanks KW, Hitti IF, Chin NW (1986) Substrate utilization for lactate and energy production by heat-shocked L929 cells. J Cell Physiol 127(3):451–456
Goossens V, Grooten J, Fiers W (1996) The oxidative metabolism of glutamine. A modulator of reactive oxygen intermediate-mediated cytotoxicity of tumor necrosis factor in L929 fibrosarcoma cells. J Biol Chem 271(1):192–196
Fan J, Kamphorst JJ, Mathew R, Chung MK, White E, Shlomi T et al (2013) Glutamine-driven oxidative phosphorylation is a major ATP source in transformed mammalian cells in both normoxia and hypoxia. Mol Syst Biol. 9:712
Hooda J, Alam MM, Zhang L (2015) Evaluating the Association of Heme and Heme Metabolites with Lung Cancer Bioenergetics and Progression. Metabolomics 5(3):1000150
Vander Heiden MG (2009) Cantley LC, Thompson CB. Understanding the Warburg effect: the metabolic requirements of cell proliferation. Science 324(5930):1029–1033
Griguer CE, Oliva CR, Gillespie GY (2005) Glucose metabolism heterogeneity in human and mouse malignant glioma cell lines. J Neurooncol 74(2):123–133
van den Heuvel AP, Jing J, Wooster RF, Bachman KE (2012) Analysis of glutamine dependency in non-small cell lung cancer: GLS1 splice variant GAC is essential for cancer cell growth. Cancer Biol Ther 13(12):1185–1194
Bergstrom J, Furst P, Noree LO, Vinnars E (1974) Intracellular free amino acid concentration in human muscle tissue. J Appl Physiol 36(6):693–697
Wise DR, Ward PS, Shay JE, Cross JR, Gruber JJ, Sachdeva UM et al (2011) Hypoxia promotes isocitrate dehydrogenase-dependent carboxylation of alpha-ketoglutarate to citrate to support cell growth and viability. Proc Natl Acad Sci U S A. 108(49):19611–19616
Metallo CM, Gameiro PA, Bell EL, Mattaini KR, Yang J, Hiller K et al (2012) Reductive glutamine metabolism by IDH1 mediates lipogenesis under hypoxia. Nature 481(7381):380–384
Mullen AR, Wheaton WW, Jin ES, Chen PH, Sullivan LB, Cheng T et al (2012) Reductive carboxylation supports growth in tumour cells with defective mitochondria. Nature 481(7381):385–388
Son J, Lyssiotis CA, Ying H, Wang X, Hua S, Ligorio M et al (2013) Glutamine supports pancreatic cancer growth through a KRAS-regulated metabolic pathway. Nature 496(7443):101–105
Schulze A, Harris AL (2012) How cancer metabolism is tuned for proliferation and vulnerable to disruption. Nature 491(7424):364–373
Zaidi N, Lupien L, Kuemmerle NB, Kinlaw WB, Swinnen JV, Smans K (2013) Lipogenesis and lipolysis: the pathways exploited by the cancer cells to acquire fatty acids. Prog Lipid Res 52(4):585–589
Menendez JA, Lupu R (2007) Fatty acid synthase and the lipogenic phenotype in cancer pathogenesis. Nat Rev Cancer 7(10):763–777
Price DT, Coleman RE, Liao RP, Robertson CN, Polascik TJ, DeGrado TR (2002) Comparison of [18 F] fluorocholine and [18 F] fluorodeoxyglucose for positron emission tomography of androgen dependent and androgen independent prostate cancer. J Urol 168(1):273–280
Liu Y, Zuckier LS, Ghesani NV (2010) Dominant uptake of fatty acid over glucose by prostate cells: a potential new diagnostic and therapeutic approach. Anticancer Res 30(2):369–374
Zha S, Ferdinandusse S, Hicks JL, Denis S, Dunn TA, Wanders RJ et al (2005) Peroxisomal branched chain fatty acid beta-oxidation pathway is upregulated in prostate cancer. Prostate 63(4):316–323
Comerford SA, Huang Z, Du X, Wang Y, Cai L, Witkiewicz AK et al (2014) Acetate dependence of tumors. Cell 159(7):1591–1602
Mashimo T, Pichumani K, Vemireddy V, Hatanpaa KJ, Singh DK, Sirasanagandla S et al (2014) Acetate is a bioenergetic substrate for human glioblastoma and brain metastases. Cell 159(7):1603–1614
Berridge MV, Herst PM, Tan AS (2010) Metabolic flexibility and cell hierarchy in metastatic cancer. Mitochondrion 10(6):584–588
Bonuccelli G, Tsirigos A, Whitaker-Menezes D, Pavlides S, Pestell RG, Chiavarina B et al (2010) Ketones and lactate “fuel” tumor growth and metastasis: evidence that epithelial cancer cells use oxidative mitochondrial metabolism. Cell Cycle 9(17):3506–3514
Pavlides S, Whitaker-Menezes D, Castello-Cros R, Flomenberg N, Witkiewicz AK, Frank PG et al (2009) The reverse Warburg effect: aerobic glycolysis in cancer associated fibroblasts and the tumor stroma. Cell Cycle 8(23):3984–4001
Icard P, Kafara P, Steyaert JM, Schwartz L, Lincet H (2014) The metabolic cooperation between cells in solid cancer tumors. Biochim Biophys Acta 1846(1):216–225
Lisanti MP, Martinez-Outschoorn UE, Sotgia F (2013) Oncogenes induce the cancer-associated fibroblast phenotype: metabolic symbiosis and “fibroblast addiction” are new therapeutic targets for drug discovery. Cell Cycle 12(17):2723–2732
Martinez-Outschoorn UE, Lisanti MP, Sotgia F (2014) Catabolic cancer-associated fibroblasts transfer energy and biomass to anabolic cancer cells, fueling tumor growth. Semin Cancer Biol 25:47–60
Ko YH, Lin Z, Flomenberg N, Pestell RG, Howell A, Sotgia F et al (2011) Glutamine fuels a vicious cycle of autophagy in the tumor stroma and oxidative mitochondrial metabolism in epithelial cancer cells: implications for preventing chemotherapy resistance. Cancer Biol Ther 12(12):1085–1097
Nieman KM, Kenny HA, Penicka CV, Ladanyi A, Buell-Gutbrod R, Zillhardt MR et al (2011) Adipocytes promote ovarian cancer metastasis and provide energy for rapid tumor growth. Nat Med 17(11):1498–1503
Sotgia F, Whitaker-Menezes D, Martinez-Outschoorn UE, Flomenberg N, Birbe RC, Witkiewicz AK et al (2012) Mitochondrial metabolism in cancer metastasis: visualizing tumor cell mitochondria and the “reverse Warburg effect” in positive lymph node tissue. Cell Cycle 11(7):1445–1454
Frezza C, Pollard PJ, Gottlieb E (2011) Inborn and acquired metabolic defects in cancer. J Mol Med (Berl). 89(3):213–220
Yang H, Ye D, Guan KL, Xiong Y (2012) IDH1 and IDH2 mutations in tumorigenesis: mechanistic insights and clinical perspectives. Clin Cancer Res 18(20):5562–5571
Parsons DW, Jones S, Zhang X, Lin JC, Leary RJ, Angenendt P et al (2008) An integrated genomic analysis of human glioblastoma multiforme. Science 321(5897):1807–1812
Mardis ER, Ding L, Dooling DJ, Larson DE, McLellan MD, Chen K et al (2009) Recurring mutations found by sequencing an acute myeloid leukemia genome. N Engl J Med 361(11):1058–1066
Balss J, Meyer J, Mueller W, Korshunov A, Hartmann C, von Deimling A (2008) Analysis of the IDH1 codon 132 mutation in brain tumors. Acta Neuropathol 116(6):597–602
Bleeker FE, Lamba S, Leenstra S, Troost D, Hulsebos T, Vandertop WP et al (2009) IDH1 mutations at residue p. R132 [IDH1(R132)] occur frequently in high-grade gliomas but not in other solid tumors. Hum Mutat 30(1):7–11
Hartmann C, Meyer J, Balss J, Capper D, Mueller W, Christians A et al (2009) Type and frequency of IDH1 and IDH2 mutations are related to astrocytic and oligodendroglial differentiation and age: a study of 1,010 diffuse gliomas. Acta Neuropathol 118(4):469–474
Watanabe T, Nobusawa S, Kleihues P, Ohgaki H (2009) IDH1 mutations are early events in the development of astrocytomas and oligodendrogliomas. Am J Pathol 174(4):1149–1153
Yan H, Parsons DW, Jin G, McLendon R, Rasheed BA, Yuan W et al (2009) IDH1 and IDH2 mutations in gliomas. N Engl J Med 360(8):765–773
Chou WC, Hou HA, Chen CY, Tang JL, Yao M, Tsay W et al (2010) Distinct clinical and biologic characteristics in adult acute myeloid leukemia bearing the isocitrate dehydrogenase 1 mutation. Blood 115(14):2749–2754
Dang L, Jin S, Su SM (2010) IDH mutations in glioma and acute myeloid leukemia. Trends Mol Med. 16(9):387–397
Gravendeel LA, Kloosterhof NK, Bralten LB, van Marion R, Dubbink HJ, Dinjens W et al (2010) Segregation of non-p.R132H mutations in IDH1 in distinct molecular subtypes of glioma. Hum Mutat 31(3):E1186–E1199
Gross S, Cairns RA, Minden MD, Driggers EM, Bittinger MA, Jang HG et al (2010) Cancer-associated metabolite 2-hydroxyglutarate accumulates in acute myelogenous leukemia with isocitrate dehydrogenase 1 and 2 mutations. J Exp Med 207(2):339–344
Ho PA, Alonzo TA, Kopecky KJ, Miller KL, Kuhn J, Zeng R et al (2010) Molecular alterations of the IDH1 gene in AML: a children’s oncology group and southwest oncology group study. Leukemia 24(5):909–913
Tefferi A, Lasho TL, Abdel-Wahab O, Guglielmelli P, Patel J, Caramazza D et al (2010) IDH1 and IDH2 mutation studies in 1473 patients with chronic-, fibrotic- or blast-phase essential thrombocythemia, polycythemia vera or myelofibrosis. Leukemia 24(7):1302–1309
Wagner K, Damm F, Gohring G, Gorlich K, Heuser M, Schafer I et al (2010) Impact of IDH1 R132 mutations and an IDH1 single nucleotide polymorphism in cytogenetically normal acute myeloid leukemia: SNP rs11554137 is an adverse prognostic factor. J Clin Oncol 28(14):2356–2364
Ward PS, Patel J, Wise DR, Abdel-Wahab O, Bennett BD, Coller HA et al (2010) The common feature of leukemia-associated IDH1 and IDH2 mutations is a neomorphic enzyme activity converting alpha-ketoglutarate to 2-hydroxyglutarate. Cancer Cell 17(3):225–234
Amary MF, Bacsi K, Maggiani F, Damato S, Halai D, Berisha F et al (2011) IDH1 and IDH2 mutations are frequent events in central chondrosarcoma and central and periosteal chondromas but not in other mesenchymal tumours. J Pathol. 224(3):334–343
Pansuriya TC, van Eijk R, d’Adamo P, van Ruler MA, Kuijjer ML, Oosting J et al (2011) Somatic mosaic IDH1 and IDH2 mutations are associated with enchondroma and spindle cell hemangioma in Ollier disease and Maffucci syndrome. Nat Genet 43(12):1256–1261
Borger DR, Tanabe KK, Fan KC, Lopez HU, Fantin VR, Straley KS et al (2012) Frequent mutation of isocitrate dehydrogenase (IDH)1 and IDH2 in cholangiocarcinoma identified through broad-based tumor genotyping. Oncologist. 17(1):72–79
Wang P, Dong Q, Zhang C, Kuan PF, Liu Y, Jeck WR et al (2013) Mutations in isocitrate dehydrogenase 1 and 2 occur frequently in intrahepatic cholangiocarcinomas and share hypermethylation targets with glioblastomas. Oncogene 32(25):3091–3100
Hemerly JP, Bastos AU, Cerutti JM (2010) Identification of several novel non-p.R132 IDH1 variants in thyroid carcinomas. Eur J Endocrinol 163(5):747–755
Murugan AK, Bojdani E, Xing M (2010) Identification and functional characterization of isocitrate dehydrogenase 1 (IDH1) mutations in thyroid cancer. Biochem Biophys Res Commun. 393(3):555–559
Kang MR, Kim MS, Oh JE, Kim YR, Song SY, Seo SI et al (2009) Mutational analysis of IDH1 codon 132 in glioblastomas and other common cancers. Int J Cancer 125(2):353–355
Gaal J, Burnichon N, Korpershoek E, Roncelin I, Bertherat J, Plouin PF et al (2010) Isocitrate dehydrogenase mutations are rare in pheochromocytomas and paragangliomas. J Clin Endocrinol Metab 95(3):1274–1278
Dang L, White DW, Gross S, Bennett BD, Bittinger MA, Driggers EM et al (2009) Cancer-associated IDH1 mutations produce 2-hydroxyglutarate. Nature 462(7274):739–744
Kalinina J, Carroll A, Wang L, Yu Q, Mancheno DE, Wu S et al (2012) Detection of “oncometabolite” 2-hydroxyglutarate by magnetic resonance analysis as a biomarker of IDH1/2 mutations in glioma. J Mol Med (Berl). 90(10):1161–1171
Elkhaled A, Jalbert LE, Phillips JJ, Yoshihara HA, Parvataneni R, Srinivasan R et al (2012) Magnetic resonance of 2-hydroxyglutarate in IDH1-mutated low-grade gliomas. Sci Transl Med. 4(116):1165
Bardella C, Pollard PJ, Tomlinson I (2011) SDH mutations in cancer. Biochim Biophys Acta 1807(11):1432–1443
Pollard PJ, Briere JJ, Alam NA, Barwell J, Barclay E, Wortham NC et al (2005) Accumulation of Krebs cycle intermediates and over-expression of HIF1alpha in tumours which result from germline FH and SDH mutations. Hum Mol Genet 14(15):2231–2239
Xiao M, Yang H, Xu W, Ma S, Lin H, Zhu H et al (2012) Inhibition of alpha-KG-dependent histone and DNA demethylases by fumarate and succinate that are accumulated in mutations of FH and SDH tumor suppressors. Genes Dev 26(12):1326–1338
Tomlinson IP, Alam NA, Rowan AJ, Barclay E, Jaeger EE, Kelsell D et al (2002) Germline mutations in FH predispose to dominantly inherited uterine fibroids, skin leiomyomata and papillary renal cell cancer. Nat Genet 30(4):406–410
Campione E, Terrinoni A, Orlandi A, Codispoti A, Melino G, Bianchi L et al (2007) Cerebral cavernomas in a family with multiple cutaneous and uterine leiomyomas associated with a new mutation in the fumarate hydratase gene. J Invest Dermatol. 127(9):2271–2273
Carvajal-Carmona LG, Alam NA, Pollard PJ, Jones AM, Barclay E, Wortham N et al (2006) Adult leydig cell tumors of the testis caused by germline fumarate hydratase mutations. J Clin Endocrinol Metab 91(8):3071–3075
Ylisaukko-oja SK, Cybulski C, Lehtonen R, Kiuru M, Matyjasik J, Szymanska A et al (2006) Germline fumarate hydratase mutations in patients with ovarian mucinous cystadenoma. Eur J Hum Genet 14(7):880–883
Zhao S, Lin Y, Xu W, Jiang W, Zha Z, Wang P et al (2009) Glioma-derived mutations in IDH1 dominantly inhibit IDH1 catalytic activity and induce HIF-1alpha. Science 324(5924):261–265
Yang H, Xiong Y, Guan K (2013) Metabolic alteration in tumorigenesis. Sci China Life Sci. 56(12):1067–1075
Loewe R, Valero T, Kremling S, Pratscher B, Kunstfeld R, Pehamberger H et al (2006) Dimethylfumarate impairs melanoma growth and metastasis. Cancer Res 66(24):11888–11896
Valero T, Steele S, Neumuller K, Bracher A, Niederleithner H, Pehamberger H et al (2010) Combination of dacarbazine and dimethylfumarate efficiently reduces melanoma lymph node metastasis. J Invest Dermatol. 130(4):1087–1094
Yamazoe Y, Tsubaki M, Matsuoka H, Satou T, Itoh T, Kusunoki T et al (2009) Dimethylfumarate inhibits tumor cell invasion and metastasis by suppressing the expression and activities of matrix metalloproteinases in melanoma cells. Cell Biol Int 33(10):1087–1094
Sudarshan S, Shanmugasundaram K, Naylor SL, Lin S, Livi CB, O’Neill CF et al (2011) Reduced expression of fumarate hydratase in clear cell renal cancer mediates HIF-2alpha accumulation and promotes migration and invasion. PLoS One 6(6):e21037
Kushnareva Y, Murphy AN, Andreyev A (2002) Complex I-mediated reactive oxygen species generation: modulation by cytochrome c and NAD(P) + oxidation-reduction state. Biochem J 368(2):545–553
Sullivan LB, Chandel NS (2014) Mitochondrial reactive oxygen species and cancer. Cancer Metab. 2:17
McCord JM (2000) The evolution of free radicals and oxidative stress. Am J Med 108(8):652–659
Hansen JM, Go YM, Jones DP (2006) Nuclear and mitochondrial compartmentation of oxidative stress and redox signaling. Annu Rev Pharmacol Toxicol 46:215–234
Genova ML, Pich MM, Biondi A, Bernacchia A, Falasca A, Bovina C et al (2003) Mitochondrial production of oxygen radical species and the role of Coenzyme Q as an antioxidant. Exp Biol Med. 228(5):506–513
Lander HM (1997) An essential role for free radicals and derived species in signal transduction. Faseb J. 11(2):118–124
Gupta SC, Hevia D, Patchva S, Park B, Koh W, Aggarwal BB (2012) Upsides and downsides of reactive oxygen species for cancer: the roles of reactive oxygen species in tumorigenesis, prevention, and therapy. Antioxid Redox Signal 16(11):1295–1322
Burdon RH (1995) Superoxide and hydrogen peroxide in relation to mammalian cell proliferation. Free Radic Biol Med 18(4):775–794
Szatrowski TP, Nathan CF (1991) Production of large amounts of hydrogen peroxide by human tumor cells. Cancer Res 51(3):794–798
Ishikawa K, Takenaga K, Akimoto M, Koshikawa N, Yamaguchi A, Imanishi H et al (2008) ROS-generating mitochondrial DNA mutations can regulate tumor cell metastasis. Science 320(5876):661–664
Sabharwal SS, Schumacker PT (2014) Mitochondrial ROS in cancer: initiators, amplifiers or an Achilles’ heel? Nat Rev Cancer 14(11):709–721
Singh KK (2006) Mitochondria damage checkpoint, aging, and cancer. Ann N Y Acad Sci 1067:182–190
Ozben T (2007) Oxidative stress and apoptosis: impact on cancer therapy. J Pharm Sci 96(9):2181–2196
Fang J, Seki T, Maeda H (2009) Therapeutic strategies by modulating oxygen stress in cancer and inflammation. Adv Drug Deliv Rev 61(4):290–302
Guppy M, Leedman P, Zu X, Russell V (2002) Contribution by different fuels and metabolic pathways to the total ATP turnover of proliferating MCF-7 breast cancer cells. Biochem J 364(Pt 1):309–315
Rodriguez-Enriquez S, Torres-Marquez ME, Moreno-Sanchez R (2000) Substrate oxidation and ATP supply in AS-30D hepatoma cells. Arch Biochem Biophys 375(1):21–30
Rodriguez-Enriquez S, Vital-Gonzalez PA, Flores-Rodriguez FL, Marin-Hernandez A, Ruiz-Azuara L, Moreno-Sanchez R (2006) Control of cellular proliferation by modulation of oxidative phosphorylation in human and rodent fast-growing tumor cells. Toxicol Appl Pharmacol 215(2):208–217
Zu XL, Guppy M (2004) Cancer metabolism: facts, fantasy, and fiction. Biochem Biophys Res Commun. 313(3):459–465
Viale A, Pettazzoni P, Lyssiotis CA, Ying H, Sanchez N, Marchesini M et al (2014) Oncogene ablation-resistant pancreatic cancer cells depend on mitochondrial function. Nature 514(7524):628–632
LeBleu VS, O’Connell JT, Gonzalez Herrera KN, Wikman H, Pantel K, Haigis MC et al (2014) PGC-1alpha mediates mitochondrial biogenesis and oxidative phosphorylation in cancer cells to promote metastasis. Nat Cell Biol 16(10):992–1003
Mauro C, Leow SC, Anso E, Rocha S, Thotakura AK, Tornatore L et al (2011) NF-kappaB controls energy homeostasis and metabolic adaptation by upregulating mitochondrial respiration. Nat Cell Biol 13(10):1272–1279
Tan AS, Baty JW, Dong LF, Bezawork-Geleta A, Endaya B, Goodwin J et al (2015) Mitochondrial genome acquisition restores respiratory function and tumorigenic potential of cancer cells without mitochondrial DNA. Cell Metab 21(1):81–94
Strakova A, Murchison EP (2015) The cancer which survived: insights from the genome of an 11000 year-old cancer. Curr Opin Genet Dev 30:49–55
Rebbeck CA, Leroi AM, Burt A (2011) Mitochondrial capture by a transmissible cancer. Science 331(6015):303
Wallace DC, Fan W, Procaccio V (2010) Mitochondrial energetics and therapeutics. Annu Rev Pathol 5:297–348
Efremov RG, Baradaran R, Sazanov LA (2010) The architecture of respiratory complex I. Nature 465(7297):441–445
Efremov RG, Sazanov LA (2011) Structure of the membrane domain of respiratory complex I. Nature 476(7361):414–420
Kim HJ, Khalimonchuk O, Smith PM, Winge DR (2012) Structure, function, and assembly of heme centers in mitochondrial respiratory complexes. Biochim Biophys Acta 1823(9):1604–1616
Bock KW, De Matteis F, Aldridge WN (1978) Heme and Hemoproteins. Springer-Verlag, New York
Padmanaban G, Venkateswar V, Rangarajan PN (1989) Haem as a multifunctional regulator. Trends Biochem Sci 14(12):492–496
Chen JJ, London IM (1995) Regulation of protein synthesis by heme-regulated eIF-2 alpha kinase. Trends Biochem Sci 20(3):105–108
Zhang L (2011) HEME BIOLOGY: The Secret Life of Heme in Regulating Diverse Biological Processes: World Scientific
Hooda J, Shah A, Zhang L (2014) Heme, an essential nutrient from dietary proteins, critically impacts diverse physiological and pathological processes. Nutrients. 6(3):1080–1102
Anderson KE, Sassa S, Bishop DF, Desnick RJ (2001) Disorders of heme biosynthesis X-linked sideroblastic anemia and the porphyrias. In: Scriver CR, Beaudt AL, Sly WS, Valle D, Barton C, Kinzler KW (eds) The metabolic and molecular bases of inherited disease, 3rd edn. The McGraw-Hill Companies Inc, New York, pp 2991–3062
Sassa S (1996) Novel effects of heme and heme-related compounds in biological systems. Current Med Chem. 3:273–290
Suzuki H, Tashiro S, Hira S, Sun J, Yamazaki C, Zenke Y et al (2004) Heme regulates gene expression by triggering Crm1-dependent nuclear export of Bach1. EMBO J 23(13):2544–2553
Zenke-Kawasaki Y, Dohi Y, Katoh Y, Ikura T, Ikura M, Asahara T et al (2007) Heme induces ubiquitination and degradation of the transcription factor Bach1. Mol Cell Biol 27(19):6962–6971
Hira S, Tomita T, Matsui T, Igarashi K, Ikeda-Saito M (2007) Bach1, a heme-dependent transcription factor, reveals presence of multiple heme binding sites with distinct coordination structure. IUBMB Life 59(8–9):542–551
Uma S, Matts RL, Guo Y, White S, Chen JJ (2000) The N-terminal region of the heme-regulated eIF2alpha kinase is an autonomous heme binding domain. Eur J Biochem 267(2):498–506
Rafie-Kolpin M, Chefalo PJ, Hussain Z, Hahn J, Uma S, Matts RL et al (2000) Two heme-binding domains of heme-regulated eukaryotic initiation factor-2alpha kinase. N terminus and kinase insertion. J Biol Chem 275(7):5171–5178
Sengupta A, Hon T, Zhang L (2005) Heme deficiency suppresses the expression of key neuronal genes and causes neuronal cell death. Brain Res Mol Brain Res 137(1–2):23–30
Zhu Y, Hon T, Ye W, Zhang L (2002) Heme deficiency interferes with the Ras-mitogen-activated protein kinase signaling pathway and expression of a subset of neuronal genes. Cell Growth Differ 13(9):431–439
Chernova T, Nicotera P, Smith AG (2006) Heme deficiency is associated with senescence and causes suppression of N-methyl-D-aspartate receptor subunits expression in primary cortical neurons. Mol Pharmacol 69(3):697–705
Chernova T, Steinert JR, Guerin CJ, Nicotera P, Forsythe ID, Smith AG (2007) Neurite degeneration induced by heme deficiency mediated via inhibition of NMDA receptor-dependent extracellular signal-regulated kinase 1/2 activation. J Neurosci 27(32):8475–8485
Raghuram S, Stayrook KR, Huang P, Rogers PM, Nosie AK, McClure DB et al (2007) Identification of heme as the ligand for the orphan nuclear receptors REV-ERBalpha and REV-ERBbeta. Nat Struct Mol Biol 14(12):1207–1213
Yin L, Wu N, Curtin JC, Qatanani M, Szwergold NR, Reid RA et al (2007) Rev-erbalpha, a heme sensor that coordinates metabolic and circadian pathways. Science 318(5857):1786–1789
Faller M, Matsunaga M, Yin S, Loo JA, Guo F (2007) Heme is involved in microRNA processing. Nat Struct Mol Biol 14(1):23–29
Tang XD, Xu R, Reynolds MF, Garcia ML, Heinemann SH, Hoshi T (2003) Haem can bind to and inhibit mammalian calcium-dependent Slo1 BK channels. Nature 425(6957):531–535
Wang S, Publicover S, Gu Y (2009) An oxygen-sensitive mechanism in regulation of epithelial sodium channel. Proc Natl Acad Sci U S A. 106(8):2957–2962
Sahoo N, Goradia N, Ohlenschlager O, Schonherr R, Friedrich M, Plass W et al (2013) Heme impairs the ball-and-chain inactivation of potassium channels. Proc Natl Acad Sci U S A. 110(42):E4036–E4044
Weinbach EC, Ebert PS (1985) Effects of succinylacetone on growth and respiration of L1210 leukemia cells. Cancer Lett 26(3):253–259
Ye WZ, Zhang L (2004) Heme controls the expression of cell cycle regulators and cell proliferation in HeLa Cells. Biochem Biophys Res Commun. 315:546–554
Ye WZ, Zhang L (2004) Heme Deficiency Causes Apoptosis But Does Not Increase ROS Generation in HeLa Cells. Biochem Biophys Res Commun. 319:1065–1071
Hooda J, Cadinu D, Alam MM, Shah A, Cao TM, Sullivan LA et al (2013) Enhanced heme function and mitochondrial respiration promote the progression of lung cancer cells. PLoS ONE 8(5):e63402
Ramirez RD, Sheridan S, Girard L, Sato M, Kim Y, Pollack J et al (2004) Immortalization of human bronchial epithelial cells in the absence of viral oncoproteins. Cancer Res 64(24):9027–9034
Whitehurst AW, Bodemann BO, Cardenas J, Ferguson D, Girard L, Peyton M et al (2007) Synthetic lethal screen identification of chemosensitizer loci in cancer cells. Nature 446(7137):815–819
Latunde-Dada GO, Takeuchi K, Simpson RJ, McKie AT (2006) Haem carrier protein 1 (HCP1): expression and functional studies in cultured cells. FEBS Lett 580(30):6865–6870
Rajagopal A, Rao AU, Amigo J, Tian M, Upadhyay SK, Hall C et al (2008) Haem homeostasis is regulated by the conserved and concerted functions of HRG-1 proteins. Nature 453(7198):1127–1131
Network CGA (2012) Comprehensive molecular characterization of human colon and rectal cancer. Nature 487(7407):330–337
Network CGA (2014) Comprehensive molecular characterization of urothelial bladder carcinoma. Nature 507(7492):315–322
Network CGA (2012) Comprehensive molecular portraits of human breast tumours. Nature 490(7418):61–70
Network CGA (2014) Comprehensive molecular profiling of lung adenocarcinoma. Nature 511(7511):543–550
Network CGA (2013) Genomic and epigenomic landscapes of adult de novo acute myeloid leukemia. N Engl J Med 368(22):2059–2074
Gruber M, Wu CJ (2014) Evolving understanding of the CLL genome. Semin Hematol 51(3):177–187
Guieze R, Wu CJ (2015) Genomic and epigenomic heterogeneity in chronic lymphocytic leukemia. Blood 126(4):445–453
Devarakonda S, Morgensztern D, Govindan R (2015) Genomic alterations in lung adenocarcinoma. Lancet Oncol. 16(7):e342–e351
Chang DK, Grimmond SM, Biankin AV (2014) Pancreatic cancer genomics. Curr Opin Genet Dev 24:74–81
McGranahan N, Swanton C (2015) Biological and therapeutic impact of intratumor heterogeneity in cancer evolution. Cancer Cell 27(1):15–26
De Sousa EMF, Vermeulen L, Fessler E, Medema JP (2013) Cancer heterogeneity–a multifaceted view. EMBO Rep 14(8):686–695
Vogelstein B, Papadopoulos N, Velculescu VE, Zhou S, Diaz LA Jr, Kinzler KW (2013) Cancer genome landscapes. Science 339(6127):1546–1558
Wyatt AW, Mo F, Wang Y, Collins CC (2013) The diverse heterogeneity of molecular alterations in prostate cancer identified through next-generation sequencing. Asian J Androl. 15(3):301–308
Shibata D (2012) Cancer. Heterogeneity and tumor history. Science. 336(6079):304–305
Gerlinger M, Rowan AJ, Horswell S, Larkin J, Endesfelder D, Gronroos E et al (2012) Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med 366(10):883–892
Biankin AV, Waddell N, Kassahn KS, Gingras MC, Muthuswamy LB, Johns AL et al (2012) Pancreatic cancer genomes reveal aberrations in axon guidance pathway genes. Nature 491(7424):399–405
Alexandrov LB, Nik-Zainal S, Wedge DC, Aparicio SA, Behjati S, Biankin AV et al (2013) Signatures of mutational processes in human cancer. Nature 500(7463):415–421
Yachida S, Jones S, Bozic I, Antal T, Leary R, Fu B et al (2010) Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature 467(7319):1114–1117
Ellsworth RE, Toro AL, Blackburn HL, Decewicz A, Deyarmin B, Mamula KA et al (2015) Molecular Heterogeneity in Primary Breast Carcinomas and Axillary Lymph Node Metastases Assessed by Genomic Fingerprinting Analysis. Cancer Growth Metastasis. 8:15–24
Leiserson MD, Vandin F, Wu HT, Dobson JR, Eldridge JV, Thomas JL et al (2015) Pan-cancer network analysis identifies combinations of rare somatic mutations across pathways and protein complexes. Nat Genet 47(2):106–114
Nowell PC (1976) The clonal evolution of tumor cell populations. Science 194(4260):23–28
de Bruin EC, McGranahan N, Mitter R, Salm M, Wedge DC, Yates L et al (2014) Spatial and temporal diversity in genomic instability processes defines lung cancer evolution. Science 346(6206):251–256
Zhang J, Fujimoto J, Wedge DC, Song X, Seth S, Chow CW et al (2014) Intratumor heterogeneity in localized lung adenocarcinomas delineated by multiregion sequencing. Science 346(6206):256–259
Gerlinger M, Swanton C (2010) How Darwinian models inform therapeutic failure initiated by clonal heterogeneity in cancer medicine. Br J Cancer 103(8):1139–1143
Greaves M, Maley CC (2012) Clonal evolution in cancer. Nature 481(7381):306–313
Yates LR, Campbell PJ (2012) Evolution of the cancer genome. Nat Rev Genet 13(11):795–806
Authors’ contributions
Literature research: MMA, SL, KEF, and LZ; Literature analysis and organization: LZ; Manuscript preparation: MMA, SL, KEF, and LZ. All authors read and approved final manuscript.
Acknowledgements
Research on cancer biology in the Zhang lab is supported by funds from The Cecil H and Ida Green Distinguished Chair.
Competing interests
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Additional information
Md Maksudul Alam and Sneha Lal contributed equally to this work
A correction to this article is available online at https://doi.org/10.1186/s40169-018-0186-5.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Alam, M.M., Lal, S., FitzGerald, K.E. et al. A holistic view of cancer bioenergetics: mitochondrial function and respiration play fundamental roles in the development and progression of diverse tumors. Clin Trans Med 5, 3 (2016). https://doi.org/10.1186/s40169-016-0082-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40169-016-0082-9