
Abstract
Background
Non-alcoholic fatty liver disease (NAFLD) is associated with atrial fibrillation (AF). Insulin resistance (IR) is the main cause of the high prevalence of AF in NAFLD patients. The triglyceride-glucose index (TyG) is a novel IR-related indicator implicated in the incidence and severity of NAFLD. However, the role of TyG in determining the risk for AF in patients with NAFLD remains unclear.
Methods
A retrospective study was conducted on 912 patients diagnosed with NAFLD via ultrasonography. These patients were divided into two groups: (1) NAFLD+ AF and (2) NAFLD+ non-AF. Least Absolute Shrinkage and Selection Operator (LASSO) regression was used to assess the correlation between the TyG index and the high risk for AF. A receiver operating characteristic (ROC) curve was constructed to evaluate the predictive value for the TyG index for AF. Restricted cubic splines (RCS) were used to test the linear correlation between TyG and the risk for AF.
Results
A total of 204 patients with AF and 708 patients without AF were included in this study. The LASSO logistic regression analysis showed that TyG was an independent risk factor for AF (odds ratio [OR] = 4.84, 95% confidence interval [CI] 2.98–7.88, P < 0.001). The RCS showed that the risk for AF increased linearly with TyG over the entire TyG range; this risk was also evident when the patients were analyzed based on sex (P for nonlinear > 0.05). In addition, the correlation between TyG and AF was a consistent finding in subgroup analysis. Furthermore, ROC curve analysis showed that TyG levels combined with traditional risk factors improved the predictive value for atrial fibrillation.
Conclusion
The TyG index is useful in assessing the risk for atrial fibrillation in patients with NAFLD. Patients with NAFLD and increased TyG indices have higher risks for atrial fibrillation. Therefore, TyG indices should be assessed when managing patients with NAFLD.
Similar content being viewed by others

Introduction
Atrial fibrillation (AF) is the most common arrhythmia observed in clinical practice, with a prevalence of approximately 1 to 4%. Even so, the prevalence and incidence of AF are steadily increasing [1]. Patients with a history of AF have an increased risk for an embolic stroke, heart failure, myocardial infarction, dementia, and chronic kidney disease. Therefore, AF is a significant burden for cardiovascular health worldwide [1, 2].
Non-alcoholic fatty liver disease (NAFLD) is the most common liver and metabolic disease worldwide. Recent studies have shown that patients with NAFLD have an increased risk of arrhythmias, including AF and ventricular arrhythmias [3, 4]. Therefore, in specific populations (such as patients with NAFLD), techniques that enable the early detection of AF are very important. Currently, AF is detected using an electrocardiogram (ECG). ECGs are extremely limited in the early detection of AFs. Therefore, alternate techniques are needed to facilitate the early detection of AFs.
Insulin resistance (IR) is an integral part of the pathogenesis of NALFD [5]. IR is implicated in the pathogenesis of AF [6]. Studies have shown that systemic IR caused by NAFLD promotes epicardial fat accumulation. Furthermore, NAFLD-related changes may induce cardiac structure, electrical conduction, and autonomic remodeling. Therefore, NAFLD-related changes increase the likelihood of arrhythmias [7]. Clinical studies have also revealed a similar correlation between IR and AF. A significant correlation between IR and the development of AF, independent of other known risk factors, including obesity, was identified in a previous study [8] using a homeostatic model to assess the degree of IR (HOMA-IR).
The triglyceride–glucose index (TyG), a novel IR-related index, strongly correlates with HOMA-IR and hyperinsulinemia-euglycemic clamp results [9, 10]. TyG has a stable role in identifying and predicting multiple diseases [11,12,13]. Previous studies have shown that the TyG index correlates with the incidence and severity of NAFLD [14, 15]. Nonetheless, the relationship between the TyG index and the incidence of AF in patients remains unclear. Therefore, this study aimed to determine the correlation between the TyG index and the incidence of AF in patients with NAFLD.
Methods
Research population
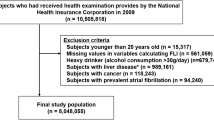
In this study, 912 patients who underwent abdominal ultrasonography (US) and were hospitalized at the Department of Cardiology, Second Hospital of Shanxi Medical University, between July 2021 and July 2022, were retrospectively analyzed. The exclusion criteria were as follows: valvular heart disease or prosthetic valve implantation, ablation of atrial fibrillation, history of alcohol consumption, secondary liver disease (e.g., viral hepatitis or autoimmune liver disease), structural heart disease (e.g., rheumatic heart disease or cardiomyopathy), kidney disease or end-stage renal disease (ESRD), infectious disease, acute infection or malignant tumor history within the last 2 weeks, and incomplete medical records. Finally, 204 patients with nonvalvular AF (127 patients with paroxysmal AF and 77 patients with persistent AF) and 708 patients without AF (sinus rhythm) were included in the study. The study was approved by the Ethics Committee of our hospital and was conducted in accordance with the principles of the Declaration of Helsinki. Due to the retrospective nature of the analysis, the requirement for informed consent was waived.
AF was determined through [16] (1) ECG reports (defined as standard 12-lead ECG recordings showing a ≥ 30-s rhythm of the heart, undiscernible repetitive P-waves, and irregular RR intermittent diagnosis of AF) and (2) patients self-reporting histories of AF with clear physical evidence.
NAFLD was diagnosed [17] based on the criteria recommended by the Chinese Society of Liver Diseases, ultrasound findings of fatty liver, and exclusion of other causes of chronic liver disease. Fatty liver disease was diagnosed in patients with at least two of the following three findings: (1) a diffuse enhancement of the liver near-field echo that was stronger than that of the kidney, (2) a poorly delineated structure of the intrahepatic bile duct, and (3) a gradual attenuation of the far-field echo of the liver.
Clinical and laboratory data
Anthropometric data and parameters including sex, age, height, weight, systolic blood pressure (SBP), diastolic blood pressure (DBP), hypertension (HTN), diabetes mellitus (DM), coronary heart disease (CHD), smoking history, and medication use were collected from electronic medical records. Overnight fasting blood samples were obtained to analyze biochemical variables, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum creatinine (Scr), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), fasting blood glucose (FBG), and other biochemical indicators. The body mass index (BMI) and TyG indices were also calculated. BMI was calculated as the weight (in kilograms) per height squared (in meters), while the TyG index was calculated using the formula ln [TG (mg/dL) × FBG (mg/dL)/2].
Statistical analysis
Statistical analyses were performed using the SPSS version 26.0 software and R version 4.0.1. Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR). Categorical variables were expressed as percentages. The presence and absence of AF were comparatively analyzed in patients. Continuous variables were compared using an independent sample t-test or Mann–Whitney U test. Categorical variables were compared using the Chi-square test or Fisher's exact test. P values were selected based on the results of the homogeneity test of variance. All the variables (including sex, age, BMI, systolic blood pressure, diastolic blood pressure, hypertension, diabetes, coronary heart disease, smoking history, medication history, ALT, AST, Scr, TC, TG, HDL-C, LDL-C, FBG, and TyG) between the two groups were included in the least absolute shrinkage and selection operator (LASSO) regression analysis, with AF as the outcome variable. The regularization parameter λ corresponding to one standard deviation from the minimum mean square error (Mean-Squared-Error) was selected as the most appropriate by cross-validation λ and select indicators with non-zero coefficients for multi-factor binary logistic regression analysis. Receiver operating characteristic (ROC) curves were constructed to evaluate the predictive value of the TyG index for AF. The trend Chi-square test was used to analyze multiple groups of categorical variables. The Kruskal–Wallis test was used to analyze multiple groups of continuous variables. The correlation between the TyG index and AF was evaluated using restricted cubic splines (RCS) with three nodes (10th, 50th, and 90th percentiles). Subgroup analyses were conducted, according to sex, age, BMI, smoking, HTN, diabetes, and CHD, to test the stability of the correlation between the TyG index and AF. Statistical significance was set at P < 0.05 (bilateral).
Results
Baseline characteristics in the AF and non-AF group
Data were collected from 912 patients with NAFLD (561 men and 351 women), including 204 patients with AF and 708 without. The patients had a mean age of 68.78 ± 11.15 and 56.25 ± 10.31 years in the NAFLD with and without AF groups, respectively. Table 1 shows the demographic and clinical characteristics of the groups. There were no significant differences in sex, smoking history, DM, medication use, DBP, ALT, and AST between the groups. The NAFLD with AF group had higher groups of patients with a history of smoking, HTN, DM, higher mean participant ages, higher mean BMI, SBP, Scr, TG, FBG, and TyG levels; and lower HDL-C and LDL-C levels (all P < 0.05) (Fig. 1).

TyG level of patients in the atrial fibrillation (AF) group and non-AF group
LASSO regression screening results
Based on cross-validation, when λ = 0.026, the results of screening AF-related indicators with non-zero coefficients from the above 20 item variables through the LASSO regression algorithm were: gender, age, BMI, DM, Scr, TC, TyG (Additional file 1: Table S1; Figs. 2, 3).

Regularization parameter λ screening process

Changes in coefficients for 20 variables when the regularization parameter λ changes
Univariate and multivariate analysis of AF and TyG in NAFLD
The multivariate LASSO logistic regression analysis showed that TyG was significantly correlated with the prevalence of AF (Table 2). In the absence of adjustments, each unit increase in TyG correlated with a 2.71-fold increase in the risk of AF (odds ratio [OR] = 2.71, 95% confidence interval [CI] 1.93–3.81, P < 0.001). After adjusting for variables screened by the LASSO regression algorithm (gender, age, BMI, DM, Scr, TC), a one-unit increase in TyG increased the risk of AF by 4.84 (OR = 4.84, 95% CI 2.98–7.88, P < 0.001). In addition, the study identified that the correlation between TyG and AF was significantly stronger than that of other clinical variables (Fig. 4; Additional file 1: Table S2).

Forest plots of independent factors associated with atrial fibrillation (AF) in non-alcoholic fatty liver disease (NAFLD)
To understand the relationship between TyG levels and AF in patients with NAFLD, TyG levels were grouped into quartiles. The average TyG index of the four groups were 8.39 ± 0.20, 8.78 ± 0.83, 9.09 ± 0.99 and 9.57 ± 0.27. Statistically significant differences were noted among the four groups in the rates of AF, age, HT, DM, CHD, SBP, ALT, AST, TC, TG, HDL-C, LDL-C, utilization rate of antidiabetic drugs and FBG (all P < 0.05) (Table 3).
For further logistic analysis, the TyG level in the first quartile was set as the control group. The LASSO logistic regression algorithm showed that even after full adjustment, the third and fourth risk of AF remained 1.93 and 4.34 times that of the first quartile (OR = 1.93, 95% CI 1.07–3.49, P = 0.030), (OR = 4.34, 95% CI 2.37–7.94, P < 0.001). However, the OR value for the second quartile was not statistically significant (OR = 1.20, 95% CI 0.66–2.17, P = 0.553). Second, the trend test showed a a trend in AF incidence between TyG quartiles (P for trend < 0.001) (Fig. 5). In conclusion, increased TyG levels correlated with an increased risk for AF. This correlation persisted in the subgroup analysis by sex (P for trend < 0.001) (Fig. 6).

Prevalence of atrial fibrillation (AF) in patients with non-alcoholic fatty liver disease (NAFLD) at different quartiles of triglycerides-glucose index (TyG)

Incidence of atrial fibrillation (AF) based on the sex-subgroup triglycerides-glucose index (TyG) index quartile
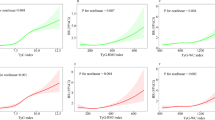
Our study further used RCS to prove the correlation between TyG and AF, and the results are shown in Fig. 7. There was a linear increase in the risk for AF with increasing TyG levels across the entire TyG range. Furthermore, the log-likelihood test demonstrated significant linearity (P nonlinear = 0.122). After grouping by sex, this linear trend was consistent.

Association between triglycerides-glucose index (TyG) index and atrial fibrillation (AF) was shown using restricted cubic splines (RCS) with three segments of the 10th, 50th and 90th percentiles of the TyG index, adjusting for age, sex, body mass index (BMI), Diabetes mellitus (DM), total cholesterol (TC), and serum creatinine (Scr)
Subgroup analysis of the correlation between the TyG index and AF
We performed several stratified analyses to further assess the robustness of the relationship between the TyG index and AF. As shown in Fig. 8, after grouping according to sex, age, BMI, smoking, HTN, DM, and CHD, TyG was associated with a high AF risk in all subgroups, and no interaction was found in any of the subgroup analyses (P for interaction > 0.05).

Subgroup analysis for the association between triglycerides-glucose index (TyG) and atrial fibrillation (AF)
ROC analysis of the TyG index
ROC analysis between TyG and the incidence of AF evaluated the usefulness of TyG in predicting AF in patients with NAFLD. The area under the curve (AUC) for only TyG was 0.615 (95% CI 0.569–0.660, P < 0.001). After introducing LASSO regression screening factors (including age, sex, BMI, DM, TC, and Cr), the ability of TyG to predict AF significantly improved, and an AUC of 0.857 (95% CI 0.827–0.887, P < 0.001) was observed (Fig. 9).

Receiver operating characteristic (ROC) curve analysis of the predictive power of triglycerides-glucose index (TyG) for atrial fibrillation (AF). TyG Model The new model integrates risk factors for LASSO regression screening (sex, age, body mass index [BMI], Diabetes mellitus [DM], total cholesterol [TC], and serum creatinine [Scr])
Discussion
NAFLD is a public health problem that affects approximately one-third of the adult population [18]. Studies have shown that the clinical burden of NAFLD includes liver-related morbidity and mortality. In addition, evidence showing that NAFLD is a multisystem disease that confers a high risk of cardiovascular disease independent of traditional risk factors is increasing [19]. Importantly, the multisystem nature of NAFLD correlates with nonischemic heart disease, particularly changes in cardiac electrophysiology. AF is the most common type of chronic cardiac arrhythmia worldwide. Since life expectancy is increasing, the lifetime incidence of AF is simultaneously increasing. An increasing incidence of AF correlates with a higher risk of embolic stroke and heart failure [20, 21]. Recent epidemiological evidence has shown that NAFLD increases the risk of cardiovascular disease and AF [22]. In a cohort study of 334 280 individuals, Roh et al. [23] found that NAFLD assessed using the fatty liver index independently correlated with an increased risk of new-onset AF in the healthy Korean population. In addition, the results of this study confirm that NAFLD can lead to AF in the absence of intermediate events such as DM, HTN, heart failure, or myocardial infarction. A large-scale observational study [3] that included patients from national examination centers in China in 2022 confirmed that NAFLD correlates with a significantly higher risk of AF in a cross-sectional population and longitudinal cohort. In a meta-analysis [24] of 19 studies involving 7,012,960 patients, NAFLD was independently associated with a higher risk of AF.
As mentioned above, although the presence of NAFLD increases the risk of AF, the underlying mechanism for this correlation is unknown. Dyslipidemia, IR, an inflammatory environment, and the renin-angiotensin system activation are currently considered pathophysiological mechanisms linking AF and NAFLD [7].
NAFLD is defined as excessive fat accumulation in the liver after an imbalance in lipid acquisition and consumption when the liver's metabolic capacity is overwhelmed [25]. IR is an integral part of NAFLD pathogenesis and is closely related to hepatic lipid metabolism pathways [26]. However, evidence shows that IR caused by NAFLD does not only occur in the liver. Furthermore, this IR strongly correlates with non-hepatic tissue IR and is unrelated to obesity [25, 27]. The liver is the center of systemic lipid and glucose metabolism. In addition, the liver synthesizes and releases various metabolites that transmit metabolic signals that potentially cause systemic IR [3].
In contrast, elevated fetuin-A and selenoprotein P levels have been observed in patients with NAFLD. These molecules may cause systemic IR by directly targeting insulin signaling and indirectly affecting glucose and lipid metabolism [28, 29]. This systemic IR state can cause excessive accumulation of fatty acids and triglycerides in cardiomyocytes. This accumulation results in a phenomenon known as “cardiac lipotoxicity.” Cardiac lipotoxicity induces cellular dysfunction, cardiomyocyte apoptosis and impairs myocardial metabolism. These changes may lead to cardiomyocyte function and structure alterations and thus increase the risk of arrhythmias [30,31,32].
Additionally, an association between IR and AF was reported in animal experiments. Studies have shown that IR causes atrial structural remodeling and abnormal intracellular calcium homeostasis, thereby increasing the likelihood of AF [33]. Animal studies have also shown that IR induces the impaired transport and expression of the major cardiac subtype glucose transporter type (GLUT)4 and the novel subtype GLUT8. This increases the vulnerability and propensity for spontaneous AF [34]. Clinical studies have also demonstrated a correlation between IR and AF. Wang et al. [35] found that patients with IR had an increased incidence of recurring AF after radiofrequency catheter ablation. Lee et al. [8] found a strong correlation between IR and AF in patients without diabetes during a median follow-up of 12.3 years. Moreover, a cohort study and in vitro experiments [36] found that using the insulin sensitizer metformin reduced the risk of AF in patients with type 2 diabetes. Therefore, metformin might attenuate tachycardia-induced myolysis and oxidative stress in atrial cells.
The TyG index is a simple and reliable surrogate marker for IR. TyG has a high sensitivity (96.5%) and specificity (85.0%) in the diagnosis of IR compared to normoglycemic hyperinsulinemic clamp. Therefore, TyG may be widely used as a marker for IR in clinical practice [37]. Numerous studies have reported that the TyG index reflects the state of IR in the body and correlates with inflammation, metabolic disorders, abnormal coagulation function, and thrombosis [38,39,40]. Studies have also revealed the association between the TyG index and AF incidence. Shi et al. [41] found a significant linear association between the TyG index and AF incidence in a diabetic population. Ling et al. [42] demonstrated that the TyG index was an independent predictor of new-onset AF after percutaneous coronary intervention (PCI), followed by Wei et al. [43] in 409 cases of hypertrophic obstructive myocardium undergoing septal muscle resection A significant association was found between TyG levels and the risk of postoperative AF in these patients. Although it is an effective predictor of NAFLD [44], its relationship with AF in patients with NAFLD remains unclear.
Our results showed a significant correlation between TyG and AF levels in the NAFLD population. In addition, this study found that age and BMI in the AF group were significantly higher than those in the non-AF group. This indicates that age and elevated BMI may increase the risk of atrial fibrillation, which is consistent with previous studies [45]. In addition, baseline data showed that BMI was higher than normal in both the AF and non-AF groups, which may be related to NAFLD and systemic IR. Previous studies [46] showed that obesity is an independent risk factor for NAFLD, which correlates with an increased prevalence and severity of NAFLD. However, NAFLD has been diagnosed in patients with normal BMIs [47]. The result of the TyG index might vary depending on the BMI. Therefore, we performed a subgroup analysis based on BMI, which showed that TyG index was significantly associated with the prevalence of atrial fibrillation even in non-obese subjects (BMI < 24 kg/m2). Overall, these results indicate the potential of the TyG index as a predictor of AF in patients with NAFLD.
In contrast, a meta-analysis [48] showed that serum TC, LDL-C, and HDL-C levels were negatively associated with AF risk, but there was no significant association between TG levels and event AF. These results were consistent with experimental results.
Logistic regression is the most widely used regression model in medical research. Multicollinearity may lead to fluctuations in the regression results and poor model stability [49]. To solve this, variables may be added or subtracted using stepwise regression to obtain a valid set of predictive variables. However, stepwise regression cannot completely overcome severe multicollinearity in the model. LASSO regression effectively addresses the issue of multicollinearity in the model. It compresses unimportant regression coefficients to zero by introducing a penalty term into the model. Therefore, higher prediction accuracy and generalization abilities are obtained at the cost of an estimation bias [50]. In the AF-related regression model, including all variables in the model may lead to a correlation between each variable of the linear model and influence the stability of the model and the estimated distortion. Therefore, we introduce the LASSO regression model that filters variables, selects representative variables, and various related prediction models to establish the correlation with AF and reduce the model’s instability and estimation distortion caused by multicollinearity.
A large sex difference in AF was noted. The mechanisms, etiology, response to treatment, stroke risk, and outcomes differed significantly between the sexes [51]. Therefore, in further studies, the impact of sex on the influence of TyG on AF incidence should be assessed. However, our results showed that the risk of AF increased linearly with an increase in TyG over the entire TyG range. When grouped by sex, the trend remained unchanged.
This study had several limitations. First, this study was a cross-sectional study with a small sample; The low prevalence of atrial fibrillation among study participants limits the extrapolation of current results to different types of atrial fibrillation, and a single center and small sample size may lead to bias; Second, we relied on a single ECG and patient self-report for the definition of AF. Therefore, the accuracy of the AF diagnosis may have been affected. Third, we did not differentiate between paroxysmal and persistent AF. Whether there is a difference in the relationship between TyG levels and the incidence of different AF types requires further investigation. Fourth, similar to other observational epidemiological studies, residual confounding caused by unincluded covariates may have biased the results. For example, our variables did not include information on electrolyte disturbances or medications that increase the risk of AF. Finally, because this was a cross-sectional study, the results showed that the TyG index was positively associated with AF in patients with NAFLD but could not claim predictive value. Future large-scale multicenter prospective studies are required to verify the predictive power of the TyG index for the risk of AF in patients with NAFLD.
Conclusion
The results showed that TyG levels in NAFLD patients with AF were significantly higher than in non-AF patients with AF. TyG level is a simple and easy-to-obtain parameter that can be used in clinical practice to predict the risk of AF in patients with NAFLD. Therefore, this indicator should be assessed in managing patients with NAFLD.
Data availability
The original contributions of this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Abbreviations
- AF:
-
Atrial fibrillation
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate + aminotransferase
- CHD:
-
Coronary heart disease
- CVD:
-
Cardiovascular disease
- DBP:
-
Diastolic blood pressure
- DM:
-
Diabetes mellitus
- FBG:
-
Fasting blood glucose
- HDL-C:
-
High density lipoprotein cholesterol
- HT:
-
Hypertension
- IR:
-
Insulin resistance
- LDL-C:
-
Low-density lipoprotein cholesterol
- NAFLD:
-
Non-alcoholic fatty liver disease
- Scr:
-
Serum creatinine
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- TyG:
-
Triglycerides-glucose index
References
Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. 2021;16:217–21.
Staerk L, Sherer JA, Ko D, Benjamin EJ, Helm RH. Atrial fibrillation: epidemiology, pathophysiology, and clinical outcomes. Circ Res. 2017;120:1501–17.
Chen Z, Liu J, Zhou F, Li H, Zhang XJ, She ZG, et al. Nonalcoholic fatty liver disease: an emerging driver of cardiac arrhythmia. Circ Res. 2021;128:1747–65.
Alon L, Corica B, Raparelli V, Cangemi R, Basili S, Proietti M, et al. Risk of cardiovascular events in patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis. Eur J Prev Cardiol. 2022;29:938–46.
Eslam M, Sanyal AJ, George J. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158:1999–2014.
Polovina M, Krljanac G, Asanin M, Seferovic PM. Crouching tiger, hidden dragon: insulin resistance and the risk of atrial fibrillation. Eur J Prev Cardiol. 2020;27:1931–3.
Haghbin H, Gangwani MK, Ravi S, Perisetti A, Aziz M, Goyal H, et al. Nonalcoholic fatty liver disease and atrial fibrillation: possible pathophysiological links and therapeutic interventions. Ann Gastroenterol. 2020;33:603–14.
Wang Z, Wang YJ, Liu ZY, Li Q, Kong YW, Chen YW, et al. Correction to: Effect of insulin resistance on recurrence after radiofrequency catheter ablation in patients with atrial fibrillation. Cardiovasc Drugs Ther. 2022. https://doi.org/10.1007/s10557-022-07333-z.
Ramdas NV, Satheesh P, Shenoy MT, Kalra S. Triglyceride Glucose (TyG) Index: a surrogate biomarker of insulin resistance. J Pak Med Assoc. 2022;72:986–8.
Selvi N, Nandhini S, Sakthivadivel V, Lokesh S, Srinivasan AR, Sumathi S. Association of Triglyceride-Glucose Index (TyG index) with HbA1c and insulin resistance in type 2 diabetes mellitus. Maedica. 2021;16:375–81.
Shi YY, Zheng R, Cai JJ, Qian SZ. The association between triglyceride glucose index and depression: data from NHANES 2005–2018. BMC Psychiatry. 2021;21:267.
Lv L, Zhou Y, Chen X, Gong L, Wu J, Luo W, et al. Relationship between the TyG index and diabetic kidney disease in patients with type-2 diabetes mellitus. Diabetes Metab Syndr Obes. 2021;14:3299–306.
Park K, Ahn CW, Lee SB, Kang S, Nam JS, Lee BK, et al. Elevated TyG index predicts progression of coronary artery calcification. Diabetes Care. 2019;42:1569–73.
Khan RS, Bril F, Cusi K, Newsome PN. Modulation of insulin resistance in nonalcoholic fatty liver disease. Hepatology. 2019;70:711–24.
Guo W, Lu J, Qin P, Li X, Zhu W, Wu J, et al. The triglyceride-glucose index is associated with the severity of hepatic steatosis and the presence of liver fibrosis in non-alcoholic fatty liver disease: a cross-sectional study in Chinese adults. Lipids Health Dis. 2020;19:218.
Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373–498.
Jian-Gao F. Guidelines for management of nonalcoholic fatty liver disease: an updated and revised edition. Zhonghua Gan Zang Bing Za Zhi. 2010;18:163–6.
Targher G, Byrne CD, Tilg H. NAFLD and increased risk of cardiovascular disease: clinical associations, pathophysiological mechanisms and pharmacological implications. Gut. 2020;69:1691–705.
Byrne CD, Targher G. NAFLD: a multisystem disease. J Hepatol. 2015;62:S47–64.
Rahman F, Kwan GF, Benjamin EJ. Global epidemiology of atrial fibrillation. Nat Rev Cardiol. 2014;11:639–54.
Lloyd-Jones DM, Wang TJ, Leip EP, Larson MG, Levy D, Vasan RS, et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation. 2004;110:1042–6.
Käräjämäki AJ, Hukkanen J, Ukkola O. The association of non-alcoholic fatty liver disease and atrial fibrillation: a review. Ann Med. 2018;50:371–80.
Roh J, Lee J, Lee H, Yoon Y, Kim M, Kim Y, et al. Association between non-alcoholic fatty liver disease and risk of new-onset atrial fibrillation in healthy adults. Liver Int. 2020;40:338–46.
Gong H, Liu X, Cheng F. Relationship between non-alcoholic fatty liver disease and cardiac arrhythmia: a systematic review and meta-analysis. J Int Med Res. 2021;49:675859294.
Chen Z, Yu Y, Cai J, Li H. Emerging molecular targets for treatment of nonalcoholic fatty liver disease. Trends Endocrinol Metab. 2019;30:903–14.
Muzurović E, Mikhailidis DP, Mantzoros C. Non-alcoholic fatty liver disease, insulin resistance, metabolic syndrome and their association with vascular risk. Metab Clin Exp. 2021;119:154770.
Bai L, Li H. Innate immune regulatory networks in hepatic lipid metabolism. J Mol Med. 2019;97:593–604.
Yan F, Zhang X, Wang W, Ji Y, Wang P, Yang Y, et al. The E3 ligase tripartite motif 8 targets TAK1 to promote insulin resistance and steatohepatitis. Hepatology. 2017;65:1492–511.
Watt MJ, Miotto PM, De Nardo W, Montgomery MK. The liver as an endocrine organ-linking NAFLD and insulin resistance. Endocr Rev. 2019;40:1367–93.
Peterson LR. Obesity and insulin resistance: effects on cardiac structure, function, and substrate metabolism. Curr Hypertens Rep. 2006;8:451–6.
Alpert MA, Karthikeyan K, Abdullah O, Ghadban R. Obesity and cardiac remodeling in adults: mechanisms and clinical implications. Prog Cardiovasc Dis. 2018;61:114–23.
Wende AR, Symons JD, Abel ED. Mechanisms of lipotoxicity in the cardiovascular system. Curr Hypertens Rep. 2012;14:517–31.
Jiao N, Baker SS, Chapa-Rodriguez A, Liu W, Nugent CA, Tsompana M, et al. Suppressed hepatic bile acid signalling despite elevated production of primary and secondary bile acids in NAFLD. Gut. 2018;67:1881–91.
Chan Y, Chang G, Lai Y, Chen W, Chang S, Hung L, et al. Atrial fibrillation and its arrhythmogenesis associated with insulin resistance. Cardiovasc Diabetol. 2019;18:125.
Maria Z, Campolo AR, Scherlag BJ, Ritchey JW, Lacombe VA. Dysregulation of insulin-sensitive glucose transporters during insulin resistance-induced atrial fibrillation. Biochim Biophys Acta Mol Basis Dis. 2018;1864:987–96.
Chang S, Wu L, Chiou M, Liu J, Yu K, Kuo C, et al. Association of metformin with lower atrial fibrillation risk among patients with type 2 diabetes mellitus: a population-based dynamic cohort and in vitro studies. Cardiovasc Diabetol. 2014;13:123.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, Martínez-Abundis E, Ramos-Zavala MG, Hernández-González SO, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95:3347–51.
Demirci I, Haymana C, Candemir B, Meric C, Yuksel B, Eser M, et al. Triglyceride-glucose index levels in patients with congenital hypogonadotropic hypogonadism and the relationship with endothelial dysfunction and insulin resistance. Endokrynol Pol. 2021;72:232–7.
Ahn S, Lee J, Lee J. Inverse association between triglyceride glucose index and muscle mass in Korean adults: 2008–2011 KNHANES. Lipids Health Dis. 2020;19:243.
Jiang Z, Zhu J, Shen H, Zhao S, Tang Y, Tang S, et al. A high triglyceride-glucose index value is associated with an increased risk of carotid plaque burden in subjects with prediabetes and new-onset type 2 diabetes: a real-world study. Front Cardiovasc Med. 2022;9:832491.
Shi W, Qin M, Wu S, Xu K, Zheng Q, Liu X. Usefulness of triglyceride-glucose index for detecting prevalent atrial fibrillation in a type 2 diabetic population. Postgrad Med. 2022;134:820–8.
Ling Y, Fu C, Fan Q, Liu J, Jiang L, Tang S. Triglyceride-glucose index and new-onset atrial fibrillation in ST-segment elevation myocardial infarction patients after percutaneous coronary intervention. Front Cardiovasc Med. 2022;9:838761.
Wei Z, Zhu E, Ren C, Dai J, Li J, Lai Y. Triglyceride-glucose index independently predicts new-onset atrial fibrillation after septal myectomy for hypertrophic obstructive cardiomyopathy beyond the traditional risk factors. Front Cardiovasc Med. 2021;8:692511.
Zheng R, Du Z, Wang M, Mao Y, Mao W. A longitudinal epidemiological study on the triglyceride and glucose index and the incident nonalcoholic fatty liver disease. Lipids Health Dis. 2018;17:262.
Ma M, Zhi H, Yang S, Yu EY, Wang L. Body mass index and the risk of atrial fibrillation: a Mendelian randomization study. Nutrients. 2022;14:1878.
Lu FB, Hu ED, Xu LM, Chen L, Wu JL, Li H, et al. The relationship between obesity and the severity of non-alcoholic fatty liver disease: systematic review and meta-analysis. Expert Rev Gastroenterol Hepatol. 2018;12:491–502.
Maier S, Wieland A, Cree-Green M, Nadeau K, Sullivan S, Lanaspa MA, et al. Lean NAFLD: an underrecognized and challenging disorder in medicine. Rev Endocr Metab Disord. 2021;22:351–66.
Guan B, Li X, Xue W, Tse G, Waleed KB, Liu Y, et al. Blood lipid profiles and risk of atrial fibrillation: a systematic review and meta-analysis of cohort studies. J Clin Lipidol. 2020;14:133–42.
Bayman EO, Dexter F. Multicollinearity in logistic regression models. Anesth Analg. 2021;133:362–5.
Hu JY, Wang Y, Tong XM, Yang T. When to consider logistic LASSO regression in multivariate analysis? Eur J Surg Oncol. 2021;47:2206.
Westerman S, Wenger N. Gender differences in atrial fibrillation: a review of epidemiology, management, and outcomes. Curr Cardiol Rev. 2019;15:136–44.
Acknowledgements
We sincerely thank the arrhythmia team of the Second Hospital of Shanxi Medical University for supporting our work.
Funding
This work was supported by the National Natural Science Foundation of China (Grant No. 81970391), “Four a batch of” talent of Shanxi Province (2021RC08), and the Excellent Youth Foundation of Shanxi Province (Grant Number 201901D211504).
Author information
Authors and Affiliations
Contributions
YZ and LB: study design; YZ and LW: data analysis; XQ, LW, and JZ: manuscript drafting; YZ, LW, and XQ: data collection; LW, JZ, and WZ: manuscript revision; LB: review and final approval. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Medical Ethics Committee of Shanxi Medical University, which waived the need for written informed consent due to the retrospective study design.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Additional tables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, Y., Wang, L., Qi, J. et al. Correlation between the triglyceride-glucose index and the onset of atrial fibrillation in patients with non-alcoholic fatty liver disease. Diabetol Metab Syndr 15, 94 (2023). https://doi.org/10.1186/s13098-023-01012-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-023-01012-1