
Abstract
Background
The absence of universal gold standards for screening of gestational diabetes (GDM) has led to heterogeneity in the identification of GDM, thereby impacting the accurate estimation of the prevalence of GDM. We aimed to evaluate the effect of different diagnostic criteria for GDM on its prevalence among general populations of pregnant women worldwide, and also to investigate the prevalence of GDM based on various geographic regions.
Methods
A comprehensive literature search was performed in PubMed, Scopus and Google-scholar databases for retrieving articles in English investigating the prevalence of GDM. All populations were classified to seven groups based-on their diagnostic criteria for GDM. Heterogeneous and non-heterogeneous results were analyzed using the fixed effect and random-effects inverse variance model for calculating the pooled effect. Publication bias was assessed by Begg’s test. The Meta-prop method was used for the pooled estimation of the prevalence of GDM. Meta-regression was conducted to explore the association between prevalence of GDM and its diagnostic criteria. Modified Newcastle–Ottawa Quality Assessment Scale for nonrandomized studies was used for quality assessment of the studies included; the ROBINS and the Cochrane Collaboration’s risk of bias assessment tools were used to evaluate the risk of bias.
Results
We used data from 51 population-based studies, i.e. a study population of 5,349,476 pregnant women. Worldwide, the pooled overall-prevalence of GDM, regardless of type of screening threshold categories was 4.4%, (95% CI 4.3–4.4%). The pooled overall prevalence of GDM in the diagnostic threshold used in IADPSG criteria was 10.6% (95% CI 10.5–10.6%), which was the highest pooled prevalence of GDM among studies included. Meta-regression showed that the prevalence of GDM among studies that used the IADPSG criteria was significantly higher (6–11 fold) than other subgroups. The highest and lowest prevalence of GDM, regardless of screening criteria were reported in East-Asia and Australia (Pooled-P = 11.4%, 95% CI 11.1–11.7%) and (Pooled-P = 3.6%, 95% CI 3.6–3.7%), respectively.
Conclusion
Over the past quarter century, the diagnosis of gestational diabetes has been changed several times; along with worldwide increasing trend of obesity and diabetes, reducing the threshold of GDM is associated with a significant increase in the incidence of GDM. The harm and benefit of reducing the threshold of diagnostic criteria on pregnancy outcomes, women’s psychological aspects, and health costs should be evaluated precisely.
Similar content being viewed by others


Background
Gestational diabetes mellitus (GDM), is one of the most common endocrinopathies during pregnancy which is defined as hyperglycemia at any time in pregnancy based on defined thresholds that are less than those considered for overt diabetes [1]. Placental production of diabetogenic hormones such as human placental lactogen in late pregnancy, leading to progressive insulin resistance; when adaptation β-cell hyperfunctionality during pregnancy fails to compensate maternal insulin resistance, it may lead to gestational diabetes [2, 3]. It is well documented that GDM is associated with adverse maternal and neonatal outcomes [4, 5] as well as lifelong risk of obesity and diabetes in both mother and child later in life [6, 7].
It is estimated that GDM affects around 7–10% of all pregnancies worldwide [8,9,10,11]; however the prevalence is difficult to estimate as rates differ between studies due to prevalence of different risk factors in the population, such as maternal age and BMI, prevalence of diabetes and ethnicity among women [12]. Moreover, screening strategies, testing methods and even diagnostic optimum glycemic thresholds for GDM remain the subject of considerable debate [13].
In this respect, the first definition of GDM was based on maternal risk for developing postpartum diabetes; subsequently, it was defined based on adverse maternal and neonatal outcomes [14]. The study of the Hyperglycaemia and Adverse Pregnancy Outcomes (HAPO) study [15] demonstrated a linear continuous correlation between increasing levels of maternal blood glucose levels on a 75-g oral glucose tolerance test (GTT) and adverse perinatal outcomes without specific threshold. In this respect, potential GDM diagnostic criteria were defined based on the odds ratio (OR) of 1.75, relative to the mean, for specific selected outcomes [15, 16].
In 2010, the International Association of Diabetes in Pregnancy Study Group (IADPSG) [17] endorsed 75-g oral glucose tolerance test, whereas in the United States and some countries GDM usually is screened and diagnosed based on the two-step screening strategy with a 3-h, 100-g OGTT after an abnormal 1-h, 50-g glucose challenge test (GCT). Furthermore, the World Health Organization (WHO) endorses the IADPSG diagnostic criteria for GDM, although the evidence for this recommendation was not very strong and was based on consensus. Nevertheless, this threshold, which was one of the lowest cut points for GDM diagnosis, has the high sensitivity and specificity [18].
However, the absence of evidenced-based and accepted ‘gold standards’ for the diagnosis of gestational diabetes as a screening strategy can lead to a heterogeneity in the identification of GDM in pregnant women [13] which may influence estimation of the prevalence of GDM and related health outcomes, as well as their health costs and quality of life.
The aim of this systematic review and meta-analysis hence was to evaluate the impact of different diagnostic criteria of blood glucose on the prevalence of GDM among general populations of pregnant women worldwide in different geographic regions.
Methods
The ethics committee of the Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, approved this study.
This systematic review and meta-analysis was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [19] to assess the following objectives:
-
To study the pooled prevalence of GDM among general population of pregnant women;
-
To study the pooled prevalence of pregnant women based on the various diagnostic criteria of blood glucose;
-
To study the pooled prevalence of pregnant women based on various GDM screening criteria groups of pregnant women in different geographic regions;
-
To study the association between prevalence of GDM and its diagnostic criteria regardless of the geographic region.
Search strategy
A comprehensive literature search was conducted in PubMed [including Medline], Web of Science, Google scholar and Scopus databases for retrieving original articles published in English language on the prevalence and incidence of gestational diabetes for all articles up to January 2018. Further, a manual search in the references list of studies included and other relevant reviews was used to maximize the identification of eligible studies. The following MeSH terms keywords, alone or in combination, were used for the search: “gestational diabetes” OR “gestational diabetes mellitus” OR “pregnancy induced diabetes” OR “gestational hyperglycemia,” OR “gestational glucose intolerance” AND “incidence” OR “prevalence” OR “epidemiology”.
Selection criteria, study selection and data extraction
Studies were eligible if (I) they had population based design, (II) universally assessed the prevalence of GDM (III) and provided accurate screening strategies and thresholds of blood sugar in those screening test. We excluded non-original studies including reviews, commentaries, editorials, letters, meeting abstracts, case reports or any papers that did not provide accurate and clear data.
The screening of titles, abstracts and full-text articles was conducted independently by authors (SBG and MA), for determining final eligibility criteria. Disagreements were resolved through discussions with senior investigator (FRT). The general characteristics of the studies including “the first author name, journal, publication year, country of study, years of sampling, study design, sample size, population characteristics including age and BMI, PCOS definition, GDM screening strategy, GDM criteria and laboratory values of blood sugar tests, study quality assessment and prevalence of GDM were extracted from the studies included and assessed. To prevent extraction and data entry errors, a control check between the final data used in the meta-analysis and the original publications was performed by all authors.
Study subgroups
To facilitate clinical interpretation of the results for statistically significant findings, all studies included were further classified to 7 groups based on the GDM screening strategy and the nearest threshold of blood sugar in the screening test as follows:
-
Group 1 or IADPSG definition, screened based on OGTT with 75 g 2-h. Threshold: one value > 92, 180 and 153 mg/dL for fasting, 1, 2 and 3 h;
-
Group 2, screened based on OGTT with 75 g 2-h. Threshold: one value > 100 and 144 mg/dL for fasting and 2 h;
-
Group 3, screened based on OGTT with 75 g 2-h. Threshold: one value > 110 and 140 mg/dL for fasting, 1 and 2 h;
-
Group 4, screened based on OGTT with 75 g 2-h. Threshold: value > 180 mg/dL for 2 h.
-
Group 5, screened based on GCT with 50 g 1-h GCT, Threshold: values > 140 mg/dL following OGTT with 100 g 3-h. Threshold: two value > 95, 180, 155 and 140 mg/dL for fasting, 1, 2 and 3 h or GCT with 50 g 1-h GCT, Threshold: values > 140 mg/dL following OGTT with 75 g 3-h. Threshold: two values > 95, 180, 155 and 140 mmol/L for fasting, 1, 2 and 3 h;
-
Group 6, screened based on Glucose challenge test (GCT) with 50 g 1-h, Threshold: 140 mg/dL following oral glucose tolerance test (OGTT) with 100 g 3-h. Threshold: two values > 105 or 190, 155, 165 and 145 mg/dL for fasting, 1, 2 and 3 h;
-
Group 7, screened based on OGTT with 100 g 3-h. Threshold: one value > 120, 175, 155 and 140 mg/dL for fasting, 1, 2 and 3 h.
Quality assessment and risk of bias
Quality of the studies was critically appraised for their methodology and results presentation. Two reviewers (SBG and MA) who were blinded to study author, journal name and institution evaluated the quality of the studies independently. The quality of observational studies was also assessed using the modification of the Newcastle–Ottawa Quality Assessment Scale for nonrandomized studies (NRS) [20] which evaluates the quality of published nonrandomized studies in terms of selection, comparability and outcomes. Studies with scores above 6 were considered as high quality, 3-5 as moderate and those with scores below than 3 as low quality.
We also evaluated risk of bias for studies included, using the ROBINS for NRS [21] and Cochrane Collaboration’s tool for assessing risk of bias for other methodological studies [22]. Five domains related to risk of bias were assessed in each cross-sectional study including: bias in assessment of exposure, bias in development of outcome of interest in case and controls, bias in selection of cases, bias in selection of controls, and bias in control of prognostic variable. In addition, 7 domains related to risk of bias were assessed bias in selection of exposed and non-exposed cohort, bias in assessment of exposure, bias in presence of outcome of interest at start of study, bias in control of prognostic variables, bias in the assessment of the presence or absence of prognostic factors, bias in the assessment of outcome, bias in adequacy regarding follow up of cohorts. Authors’ judgments were categorized as ‘‘low risk,’’ ‘‘high risk,’’ and ‘‘unclear risk’’ of bias (probably low or high risk of bias) [22].
Statistical analysis
The software package STATA (version 12; STATA Inc., College Station, TX, USA) was applied to conduct statistical analysis. Heterogeneity between studies was assessed using I2 index and P > 0.05 was interpreted as heterogeneity. Heterogeneous and non-heterogeneous results were analyzed using the fixed effects and random-effects inverse variance models for calculating the pooled effect. Publication bias was assessed by Begg’s test. The Meta-prop method was used for pooled estimation of GDM prevalence. Meta-regression was conducted to explore the association between prevalence of GDM and its diagnostic criteria. In this respect, we used the HAPO definition criteria for screening with group 4 as the reference group for comparison.
In addition, meta-analysis of pooled prevalence of GDM was performed in the subgroups of some different geographical regions of countries, based on different GDM diagnostic classifications. P > 0.05 was set as significance level.
Results
Search results, study selection, study characteristics, and quality assessment
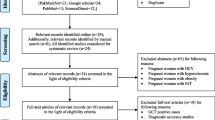
Additional file 1: Figure S1 illustrates the flow diagram of the search strategy and study selection. The search strategy yielded 3396 potentially relevant articles. According to the selection inclusion criteria, 338 articles were identified for further full-text assessment. Finally, we included 51 population-based studies which included data of 5,349,476 pregnant women for the meta-analysis. Table 1 presents the summary of studies assessing the prevalence of GDM.
Details of the quality assessment of studies included are presented in Additional file 1: Tables S1, S2. Twenty-six studies were classified as high [16, 23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47], and 25 as moderate [8, 48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71]; no study had low quality. A total of 33.3% studies were cross-sectional and 66.6% were prospective or retrospective cohorts published between 1993 and 2017. Thirty-five studies were cohort [8, 16, 23, 25,26,27, 30,31,32,33,34, 38,39,40, 42, 43, 45, 46, 48, 50, 51, 54, 55, 57, 60,61,62,63,64,65,66, 69, 71, 72] and 16 cross-sectional [24, 28, 29, 35,36,37, 41, 44, 47, 49, 52, 53, 56, 67, 68, 70]. Fourteen (27.4%) studies, classified as group 1 [16, 33, 35, 37, 39, 42, 49, 59, 60, 62, 68,69,70,71] used IADPSG; 6 (11.7%) as group 2 [24, 41, 43, 47, 50, 54], 11 (21.5%) as group 3 [28, 31, 55,56,57,58, 63,64,65,66,67], 2 (3.9%) as group 4 [36, 53], 11 (21.5%) as group 5 [23, 27, 30, 32, 38, 40, 44,45,46, 51, 52], 4 (7.8%) as group 6 [8, 29, 34, 48] and 3 (5.8%) as group 7 [25, 26, 61].
In addition, 13 studies were conducted in the USA and Canada [8, 25, 29, 30, 32, 34, 38, 44, 46, 48, 51, 57, 60], five in Australia [24, 41, 43, 50, 54], seven in China and Japan [26, 33, 35, 45, 47, 52, 71], 9 in north Europe [31, 36, 42, 53, 55, 59, 61, 62, 68], six in India, Bangladesh and Sri Lanka [37, 49, 56, 64, 65, 67] and 10 were from other countries [23, 27, 28, 39, 40, 58, 63, 66, 69, 70], including Bahrain, Israel, Croatia, Argentina, Brazil, Ethiopia and Saudi Arabia. One study by the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study Cooperative Research Group was originally performed in nine countries [16].
Considering the amount of literature included, except for USA, Canada and Australia, the most commonly used threshold in Asia and Europe was IADPSG. Australians were screened based on their national criteria (group 2). The most prevalent criteria used in USA and Canada was the method used for group 5.
Meta-analysis and meta-regression of outcomes
Worldwide, the pooled overall prevalence of GDM among pregnant women, regardless of type of screening criteria categories was 4.4%, (Pooled overall P = 4.4%, 95% CI 4.3–4.4%). The overall pooled prevalence (95% CI) of GDM among different groups, depending on the diagnosis criteria used, is presented in Table 2. I2 index showed that except for subgroup 7, no significant heterogeneity were detected in the meta-analysis.
The pooled prevalence of GDM in subgroup 1 was 10.6% (Pooled P = 10.6%, 95% CI 10.5–10.6%) which was the highest pooled prevalence of GDM among studies included. Moreover, the lowest prevalence of GDM was 2.2% in subgroup of 4 (Pooled overall P = 2.2%, 95% CI 2.2–2.3%) that used the cut of value of > 180 mg/dL for 2 h in OGTT-75 g glucose (Fig. 1). In this respect, the results of meta-regression showed that, exception for group 3, the prevalence of GDM among study that used the IADPSG criteria was significantly higher (6–11 fold) than other subgroups (Table 3) and (Additional file 1: Figure S2).

Forest plot of pooled Prevalence in subgroup of GDM diagnostic thresholds
Table 4 showed the pooled analysis of prevalence of GDM in various GDM screening criteria groups among pregnant women in different geographic regions. The highest and lowest prevalence of GDM, regardless of screening criteria, reported in East Asia and Australia was (Pooled P = 11.4%, 95% CI 11.1–11.7%) and (Pooled P = 3.6%, 95% CI 3.6–3.7%), respectively (Additional file 1: Figures S3–S7).
We performed a subgroup analysis based on the various threshold groups for screening in different geographic regions (Table 4). In this respect, the prevalence of GDM, based on the IADPSG criteria was (Pooled P = 15.2%, 95% CI 14.7–15.7%), (Pooled P = 7.8%, 95% CI 7.6–8.1%) and (Pooled overall P = 10.8, 95% CI 10.7–10.8%) respectively. USA, Canada and Australia did not use the IADPSG criteria most of the time. The pooled prevalence of GDM in USA and Canada, that mostly used criterion No. 5, were 5.4%; (Pooled P = 5.4%, 95% CI 5.4–5.4%) and in Australia screened based on criterion No. 2, was 3.6%, (Pooled P = 3.6%, 95% CI 3.6–3.7%). We did not have sufficient studies to perform meta-analyses in other regions.
Publication bias and risk of bias
There was no substantial publication bias for meta-analyses based on the Begg’s test (Tables 2 and 4). Overall most of studies were judged as having low risk of bias for the evaluated domains; details are presented in Additional file 1: Figures S8, S9; as shown most cross-sectional and case–control studies had a low risk of bias in the assessment of exposure, development of outcome of interest in case and controls and selection of cases, approximately one-third of them had a high risk of bias in control of prognostic variables and selection of controls.
In addition, cohort studies had a low risk of bias for selection of exposed and non-exposed cohorts, assessment of exposure, presence of outcome of interest at start of study, outcome assessment, and adequacy of follow up of cohorts; however one-third of them had a high risk of bias in controlling prognostic variables and assessment of the presence or absence of prognostic factors and 3% of them had a high risk of bias in presence of outcome of interest at initiation of study.
Discussion
The current meta-analysis of population based studies provided data on the impact of various thresholds of diagnostic GDM criteria on prevalence of GDM. Results of the meta-analysis showed that using lower glucose level thresholds as recommended by the IADPSG, identified significantly higher numbers (6–11 fold) of women with GDM, compared to other diagnostic criteria; in this respect, except for USA, Canada and Australia, this criteria was the most commonly used screening method worldwide. The highest prevalence of GDM was found in south Asia, where approximately 2 in ten women were diagnosed with GDM.
Despite the wide range of recommendations and guidelines for detection of women with GDM adopted by expert international societies [17, 73,74,75,76,77,78,79,80], there is strong controversy over the identification of GDM. Both the screening methods and diagnostic criteria vary among obstetricians and endocrine societies and more commonly even between regions within a single country. Screening approaches was include universal or targeted high risk screening, screening methods including fasting plasma glucose, random glucose and oral glucose challenge, diagnostic criteria including one steps or two, amount of the 75 g or 100 g glucose load, the duration of the test for 2 or 3 h, as well as the glucose threshold values, and whether 1 or 2 high glucose values are all used.
On the basis of the of Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study [16], the International Association of Diabetes and Pregnancy Study Groups (IADPSG) suggested that a 75-g OGTT be performed and that GDM be diagnosed if any one of the following is observed: fasting plasma glucose > 92 mg/dL, 1 h: 180 mg/dL and 2 h: 153 mg/dL [17] selected based on the odds ratio of 1.75-fold, the mean for outcomes of the HAPO study. Although the IADPSG recommendations are the first evidence-based, large-scale guideline for GDM and are now widely used around the world, lack of sufficient data on the increased effectiveness in improving feto-maternal outcomes has led to the use of different criteria, which are often based on expert opinion and have all not been to acceptable universally.
However, the more stringent criteria of IADPSG, lead to higher prevalence of GDM among pregnant women and potentially increase the costs of care for many pregnant women worldwide [81]. Considering the fact that majority of births annually occur in low- and low–middle income countries with limited resources, the cost-effectivity of this definition must be precisely defined on short-term pregnancy and neonatal outcomes, as well as long-term cardio-metabolic benefits for mother and offspring and the cost effectiveness of treatment [82].
In addition, the diagnosis of GDM and its treatment is stressful situation can be accompanied by serious psychological challenges for women and their families due to the complex interaction between psychological factors based on patients experience [83, 84]. While not recognizing the GDM is associated with adverse pregnancy outcomes; over-diagnosis may leads to psychological stress, unnecessary treatments and impaired quality of life. Maternal concerns about one’s own and unborn health status may strong negative effects on the maternal health status, diminishing overall quality of life (QoL). Marchetti et al. in a systematic review, showed that QoL among women with GDM, is significantly worse in both the short and long term health status [72]. Moreover, a “diabetic” label carries familial and social stigma especially in gender biased cultures, possibly leading to conflict among families [83].
One of our main findings was the estimation of the prevalence of GDM worldwide. There are two documented meta-analyses that evaluated the prevalence of GDM; Eades et al. describes a meta-analysis of primary research data reporting the prevalence of gestational diabetes mellitus in the general pregnant population in Europe; they reported that the overall prevalence of GDM was 5.4% (95% CI 3.8–7.8%) [85]. In another recent meta-analysis, Nguyen et al. reported that the pooled prevalence of GDM in Eastern and Southeastern Asia was 10.1% (95% CI 6.5–15.7%), whereas those were across nations [9]. Results of both these studies are comparable with our meta-analysis. However, the first review was limited to developed countries in Europe which may have had a different prevalence of GDM from developing countries even in Europe. The second review were not references the population based studies and both of studies did not evaluate the effect of diagnostic criteria on GDM prevalence.
The present review has the strength of a large sample size with population-based design studies involving approximately five and a half million women, using different methods for screening and diagnosis of GDM and consistency of method, quality, and focus. However, there are some limitations that need to be considered when interpreting the results of this meta-analysis. This study focused on evaluating the prevalence of GDM based on different criteria and did not assess the impact of diagnostic criteria on maternal and neonatal outcomes, which is a limitation. In addition, most of the included studies did not report the maternal age and BMI; we could not adjust for these confounders in our analysis. Moreover, we included studies that used the universal screening strategy; so countries with a low prevalence, that mostly used the targeted high-risk screening strategy was not included in our meta-analysis, which may lead to overestimation of the prevalence of GDM in low prevalent areas e.g. north Europe. In addition, most of the included studies did not exclude the twin or multiple pregnancy in their report and some even reported the proportion of deliveries affected by GDM. However, since multiple pregnancies constitute approximately 3% of births [86, 87], it seems that could not confound the results. However, due to the lack of data available for some regions, we could not perform subgroup analysis in some areas. In addition, it should be noted that in the last quarter century, the definition of GDM has been changed several time. Moreover, the increasing trend of obesity and diabetes may increase the prevalence of gestational diabetes; and can lead to heterogeneity of data.
Conclusion
Over the past quarter century, the diagnosis of gestational diabetes has been changed several times; there is still no general consensus about it. International communities have adopted different diagnostic methods and thresholds. Along with a worldwide increasing trend of obesity and diabetes, reducing the threshold for diagnosis of GDM are associated with a significant increase in the incidence of GDM. The harm and benefit of reducing the threshold of diagnostic criteria on pregnancy outcomes, women’s psychological aspects, and health costs should be evaluated precisely.
Abbreviations
- GDM:
-
gestational diabetes mellitus
- HAPO:
-
hyperglycaemia and adverse pregnancy outcomes
- OGTT:
-
oral glucose tolerance test
- OR:
-
odds ratio
- IADPSG:
-
International Association of Diabetes in Pregnancy Study Group
- WHO:
-
World Health Organization
- GCT:
-
glucose challenge test
References
http://apps.who.int/iris/bitstream/handle/10665/85975/WHO_NMH_MND_13.2_eng.pdf; jsessionid = FD8DC8872A84924274CB92855D70888A?sequence = 1. Accessed 12 Oct 2018.
Barbour LA, McCurdy CE, Hernandez TL, Kirwan JP, Catalano PM, Friedman JE. Cellular mechanisms for insulin resistance in normal pregnancy and gestational diabetes. Diabetes Care. 2007;30:S112–9.
Genevay M, Pontes H, Meda P. Beta cell adaptation in pregnancy: a major difference between humans and rodents? Diabetologia. 2010;53:2089–92.
Wendland EM, Torloni MR, Falavigna M, Trujillo J, Dode MA, Campos MA, et al. Gestational diabetes and pregnancy outcomes—a systematic review of the World Health Organization (WHO) and the International Association of Diabetes in Pregnancy Study Groups (IADPSG) diagnostic criteria. BMC Pregnancy Childbirth. 2012;12:23.
Farrar D, Simmonds M, Bryant M, Sheldon TA, Tuffnell D, Golder S, et al. Hyperglycaemia and risk of adverse perinatal outcomes: systematic review and meta-analysis. BMJ. 2016;354:i4694.
Kim SY, Sharma AJ, Callaghan WM. Callaghan, gestational diabetes and childhood obesity: what is the link? Curr Opin Obstet Gynecol. 2012;24:376–81.
Garcia-Vargas L, Addison SS, Nistala R, Kurukulasuriya D, Sowers JR. Gestational diabetes and the offspring: implications in the development of the cardiorenal metabolic syndrome in offspring. Cardiorenal Med. 2012;2:134–42.
Xiong X, Saunders LD, Wang FL, Demianczuk NN. Gestational diabetes mellitus: prevalence, risk factors, maternal and infant outcomes. Int J Gynaecol Obstet. 2001;75:221–8.
Nguyen CL, Pham NM, Binns CW, Duong DV, Lee AH. Prevalence of gestational diabetes mellitus in eastern and southeastern Asia: a systematic review and meta-analysis. J Diabetes Res. 2018;2018:6536974.
Ferrara A. Increasing prevalence of gestational diabetes mellitus: a public health perspective. Diabetes Care. 2007;30:S141–6.
Adam S, Rheeder P. Screening for gestational diabetes mellitus in a South African population: prevalence, comparison of diagnostic criteria and the role of risk factors. S Afr Med J. 2017;107:523–7.
Lin PC, Hung CH, Chan TF, Lin KC, Hsu YY, Tzeng YL. The risk factors for gestational diabetes mellitus: a retrospective study. Midwifery. 2016;42:16–20.
Cheung NW, Moses RG. Gestational diabetes mellitus: is it time to reconsider the diagnostic criteria? Diabetes Care. 2018;41:1337–8.
Jacklin PB, Maresh MJ, Patterson CC, Stanley KP, Dornhorst A, Burman-Roy S, et al. A cost-effectiveness comparison of the NICE 2015 and WHO 2013 diagnostic criteria for women with gestational diabetes with and without risk factors. BMJ Open. 2017;7:e016621.
HAPO Study Cooperative Research Group, Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358:1991–2002.
Sacks DA, Hadden DR, Maresh M, Deerochanawong C, Dyer AR, Metzger BE, et al. Frequency of gestational diabetes mellitus at collaborating centers based on IADPSG consensus panel-recommended criteria: the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study. Diabetes Care. 2012;35:526–8.
International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33:676–82.
Bhavadharini B, Uma R, Saravanan P, Mohan V. Screening and diagnosis of gestational diabetes mellitus—relevance to low and middle income countries. Clin Diabetes Endocrinol. 2016;2:13.
Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(264–9):W64.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute; 2009. Available in March 2016.
Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions, vol. 4. New York: Wiley; 2011.
Al Mahroos S, Nagalla DS, Yousif W, Sanad H. A population-based screening for gestational diabetes mellitus in non-diabetic women in Bahrain. Ann Saudi Med. 2005;25:129–33.
Anna V, van der Ploeg HP, Cheung NW, Huxley RR, Bauman AE. Sociodemographic correlates of the increasing trend in prevalence of gestational diabetes mellitus in a large population of women between 1995 and 2005. Diabetes Care. 2008;31:2288–93.
Baptiste-Roberts K, Nicholson WK, Wang NY, Brancati FL. Gestational diabetes and subsequent growth patterns of offspring: the National Collaborative Perinatal Project. Matern Child Health J. 2012;16:125–32.
Leng J, Shao P, Zhang C, Tian H, Zhang F, Zhang S, et al. Prevalence of gestational diabetes mellitus and its risk factors in Chinese pregnant women: a prospective population-based study in Tianjin, China. PLoS ONE. 2015;10:e0121029.
Chodick G, Elchalal U, Sella T, Heymann AD, Porath A, Kokia E, Shalev V. The risk of overt diabetes mellitus among women with gestational diabetes: a population-based study. Diabet Med. 2010;27:779–85.
Erjavec K, Poljičanin T, Matijević R. Impact of the implementation of new WHO diagnostic criteria for gestational diabetes mellitus on prevalence and perinatal outcomes: a population-based study. J Pregnancy. 2016;2016:2670912.
Ferrara A, Hedderson MM, Quesenberry CP, Selby JV. Prevalence of gestational diabetes mellitus detected by the national diabetes data group or the carpenter and coustan plasma glucose thresholds. Diabetes Care. 2002;25:1625–30.
Hedderson MM, Darbinian JA, Ferrara A. Disparities in the risk of gestational diabetes by race-ethnicity and country of birth. Paediatr Perinat Epidemiol. 2010;24:441–8.
Jenum AK, Mørkrid K, Sletner L, Vangen S, Torper JL, Nakstad B, et al. Impact of ethnicity on gestational diabetes identified with the WHO and the modified International Association of Diabetes and Pregnancy Study Groups criteria: a population-based cohort study. Eur J Endocrinol. 2012;166:317–24.
Lawrence JM, Contreras R, Chen W, Sacks DA. Trends in the prevalence of pre-existing diabetes and gestational diabetes mellitus among a racially/ethnically diverse population of pregnant women, 1999–2005. Diabetes Care. 2008;31:899–904.
Leng J, Liu G, Zhang C, Xin S, Chen F, Li B, et al. Physical activity, sedentary behaviors and risk of gestational diabetes mellitus: a population-based cross-sectional study in Tianjin, China. Eur J Endocrinol. 2016;174:763–73.
Magee MS, Walden CE, Benedetti TJ, Knopp RH. Influence of diagnostic criteria on the incidence of gestational diabetes and perinatal morbidity. JAMA. 1993;269:609–15.
Mizuno S, Nishigori H, Sugiyama T, Takahashi F, Iwama N, Watanabe Z, et al. Association between social capital and the prevalence of gestational diabetes mellitus: an interim report of the Japan Environment and Children’s Study. Diabetes Res Clin Pract. 2016;120:132–41.
Lindqvist M, Persson M, Lindkvist M, Mogren I. No consensus on gestational diabetes mellitus screening regimes in Sweden: pregnancy outcomes in relation to different screening regimes 2011 to 2012, a cross-sectional study. BMC Pregnancy Childbirth. 2014;14:185.
Bhavadharini B, Mahalakshmi MM, Anjana RM, Maheswari K, Uma R, Deepa M, et al. Prevalence of gestational diabetes mellitus in urban and rural Tamil Nadu using IADPSG and WHO 1999 criteria (WINGS 6). Clin Diabetes Endocrinol. 2016;2:8.
Pu J, Zhao B, Wang EJ, Nimbal V, Osmundson S, Kunz L, et al. Racial/ethnic differences in gestational diabetes prevalence and contribution of common risk factors. Paediatr Perinat Epidemiol. 2015;29:436–43.
Schmidt MI, Duncan BB, Reichelt AJ, Branchtein L, Matos MC, e Forti AC, et al. Gestational diabetes mellitus diagnosed with a 2-h 75-g oral glucose tolerance test and adverse pregnancy outcomes. Diabetes Care. 2001;24:1151–5.
Sella T, Shalev V, Elchalal U, Chovel-Sella A, Chodick G, et al. Screening for gestational diabetes in the 21st century: a population-based cohort study in Israel. J Matern Fetal Neonatal Med. 2013;26:412–6.
Shand AW, Bell JC, McElduff A, Morris J, Roberts CL. Outcomes of pregnancies in women with pre-gestational diabetes mellitus and gestational diabetes mellitus; a population-based study in New South Wales, Australia, 1998–2002. Diabet Med. 2008;25:708–15.
Sommer C, Mørkrid K, Jenum AK, Sletner L, Mosdøl A, Birkeland KI. Weight gain, total fat gain and regional fat gain during pregnancy and the association with gestational diabetes: a population-based cohort study. Int J Obes. 2014;38:76–81.
Tan HLE, Luu J, Caswell A, Holliday E, Attia J, Acharya S. Impact of new International Association of Diabetes and Pregnancy Study Groups (IADPSG) diagnostic criteria on perinatal outcomes in a regional tertiary hospital in New South Wales, Australia. Diabetes Res Clin Pract. 2017;134:191–8.
Wang Y, Chen L, Xiao K, Horswell R, Besse J, Johnson J, et al. Increasing incidence of gestational diabetes mellitus in Louisiana, 1997–2009. J Womens Health. 2012;21:319–25.
Yang H, Wei Y, Gao X, Xu X, Fan L, He J, et al. Risk factors for gestational diabetes mellitus in Chinese women—a prospective study of 16 286 pregnant women in China. Diabet Med. 2009;26:1099–104.
Yeung RO, Savu A, Kinniburgh B, Lee L, Dzakpasu S, Nelson C, et al. Prevalence of gestational diabetes among Chinese and South Asians: a Canadian population-based analysis. J Diabetes Complicat. 2017;31:529–36.
Zhang F, Dong L, Zhang CP, Li B, Wen J, Gao W, et al. Increasing prevalence of gestational diabetes mellitus in Chinese women from 1999 to 2008. Diabet Med. 2011;28:652–7.
Aljohani N, Rempel BM, Ludwig S, Morris M, McQuillen K, Cheang M, et al. Gestational diabetes in Manitoba during a twenty-year period. Clin Invest Med. 2008;31:E131–7.
Arora GP, Thaman RG, Prasad RB, Almgren P, Brøns C, Groop LC, et al. Prevalence and risk factors of gestational diabetes in Punjab, north India—results from a population screening program. Eur J Endocrinol. 2015;173:257–67.
Moses RG, Morris GJ, Petocz P, San Gil F, Garg D, et al. The impact of potential new diagnostic criteria on the prevalence of gestational diabetes mellitus in Australia. Med J Aust. 2011;194:338–40.
Ferrara A, Kahn HS, Quesenberry CP, Riley C, Hedderson MM. An increase in the incidence of gestational diabetes mellitus: Northern California, 1991–2000. Obstet Gynecol. 2004;103:526–33.
Gao XL, Wei YM, Yang HX, Xu XM, Fan L, He J, et al. Difference between 2 h and 3 h 75 g glucose tolerance test in the diagnosis of gestational diabetes mellitus (GDM): results from a national survey on prevalence of GDM. Front Med China. 2010;4:303–7.
Ignell C, Claesson R, Anderberg E, Berntorp K. Trends in the prevalence of gestational diabetes mellitus in southern Sweden, 2003–2012. Acta Obstet Gynecol Scand. 2014;93:420–4.
Ishak M, Petocz P. Gestational diabetes among Aboriginal Australians: prevalence, time trend, and comparisons with non-Aboriginal Australians. Ethn Dis. 2003;13:55–60.
Janghorbani M, Stenhouse E, Jones RB, Millward A. Gestational diabetes mellitus in Plymouth, UK: prevalence, seasonal variation and associated factors. J Reprod Med. 2006;51:128–34.
Jesmin S, Akter S, Akashi H, Al-Mamun A, Rahman MA, Islam MM, et al. Screening for gestational diabetes mellitus and its prevalence in Bangladesh. Diabetes Res Clin Pract. 2014;103:57–62.
Kalamegham R, Nuwayhid BS, Mulla ZD. Prevalence of gestational fasting and postload single dysglycemia in Mexican–American women and their relative significance in identifying carbohydrate intolerance. Am J Perinatol. 2010;27:697–704.
McCarthy AD, Curciarello R, Castiglione N, Tayeldín MF, Costa D, Arnol V, et al. Universal versus selective screening for the detection, control and prognosis of gestational diabetes mellitus in Argentina. Acta Diabetol. 2010;47:97–103.
Melchior H, Kurch-Bek D, Mund M. The prevalence of gestational diabetes: a population-based analysis of a nationwide screening program. Dtsch Arztebl Int. 2017;114:412–8.
Murphy NJ, Bulkow LR, Schraer CD, Lanier AP. Prevalence of diabetes mellitus in pregnancy among Yup’ik Eskimos, 1987–1988. Diabetes Care. 1993;16:315–7.
Ostlund I, Hanson U. Occurrence of gestational diabetes mellitus and the value of different screening indicators for the oral glucose tolerance test. Acta Obstet Gynecol Scand. 2003;82:103–8.
O’Sullivan EP, Avalos G, O’Reilly M, Dennedy MC, Gaffney G, Dunne F, et al. Atlantic diabetes in pregnancy (DIP): the prevalence and outcomes of gestational diabetes mellitus using new diagnostic criteria. Diabetologia. 2011;54:1670–5.
Schmidt MI, Matos MC, Reichelt AJ, Forti AC, de Lima L, Duncan BB. Prevalence of gestational diabetes mellitus—do the new WHO criteria make a difference? Diabet Med. 2000;17:376–80.
Seshiah V, Balaji V, Balaji MS, Paneerselvam A, Arthi T, Thamizharasi M, et al. Gestational diabetes mellitus manifests in all trimesters of pregnancy. Diabetes Res Clin Pract. 2007;77:482–4.
Seshiah V, Balaji V, Balaji MS, Paneerselvam A, Arthi T, Thamizharasi M, et al. Prevalence of gestational diabetes mellitus in South India (Tamil Nadu): a community based study. J Assoc Physicians India. 2008;56:329–33.
Seyoum B, Kiros K, Haileselase T, Leole A. Prevalence of gestational diabetes mellitus in rural pregnant mothers in northern Ethiopia. Diabetes Res Clin Pract. 1999;46:247–51.
Sudasinghe BH, Ginige PS, Wijeyaratne CN. Prevalence of gestational diabetes mellitus in a suburban district in Sri Lanka: a population based study. Ceylon Med J. 2016;61:149–53.
Tamayo T, Tamayo M, Rathmann W, Potthoff P. Prevalence of gestational diabetes and risk of complications before and after initiation of a general systematic two-step screening strategy in Germany (2012–2014). Diabetes Res Clin Pract. 2016;115:1–8.
Trujillo J, Vigo A, Duncan BB, Falavigna M, Wendland EM, Campos MA, et al. Impact of the International Association of Diabetes and Pregnancy Study Groups criteria for gestational diabetes. Diabetes Res Clin Pract. 2015;108:288–95.
Wahabi H, Fayed A, Esmaeil S, Mamdouh H, Kotb R. Prevalence and complications of pregestational and gestational diabetes in Saudi women: analysis from Riyadh Mother and Baby cohort study (RAHMA). Biomed Res Int. 2017;2017:6878263.
Zhu WW, Yang HX, Wang C, Su RN, Feng H, Kapur A. High prevalence of gestational diabetes mellitus in Beijing: effect of maternal birth weight and other risk factors. Chin Med J. 2017;130:1019–25.
Marchetti D, Carrozzino D, Fraticelli F, Fulcheri M, Vitacolonna E. Quality of life in women with gestational diabetes mellitus: a systematic review. J Diabetes Res. 2017;2017:7058082.
World Health Organization. Diagnostic criteria and classification of hyperglycaemia first detected in pregnancy. Geneva: World Health Organization; 2013.
American Diabetes Association. Classification and diagnosis of diabetes. Diabetes Care. 2017;40:S11–24.
National Institute for Health and Care Excellence. NICE guideline. Diabetes in pregnancy: management from preconception to the postnatal period (NG3). London: NICE. http://www.nice.org.uk/guidance/ng3/resources/diabetesin-pregnancy-management-of-diabetes-and-itscomplications-from-preconception-to-the-postnatal-period-51038446021. Accessed 23 July 2017.
Hoffman L, Nolan C, Wilson JD, Oats JJ, Simmons D. Gestational diabetes mellitus-management guidelines—The Australasian Diabetes in Pregnancy Society. Med J Aust. 1998;169:93–7.
ACOG. Committee on practice bulletins—obstetrics. ACOG Practice Bulletin No. 190: gestational diabetes mellitus. Obstet Gynecol. 2018;131:e49–64.
American Diabetes Association. Classification and diagnosis of diabetes: standards of medical care in diabetes—2018. Diabetes Care. 2018;41:S13–27.
Blumer I, Hadar E, Hadden DR, Jovanovič L, Mestman JH, Murad MH, et al. Diabetes and pregnancy: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2013;98:4227–49.
National Collaborating Centre for Women’s and Children’s Health (UK). Health, Diabetes in pregnancy: management of diabetes and its complications from preconception to the postnatal period. 2015.
Gillespie P, O’Neill C, Avalos G, Dunne FP, ALANTIC DIP Collaborators. New estimates of the costs of universal screening for gestational diabetes mellitus in Ireland. Ir Med J. 2012;105(5 Suppl):15–8.
Brown FM, Wyckoff J. Application of one-step IADPSG versus two-step diagnostic criteria for gestational diabetes in the real world: impact on health services, clinical care, and outcomes. Curr Diab Rep. 2017;17:85.
Kalra B, Gupta Y, Baruah MP. Renaming gestational diabetes mellitus: a psychosocial argument. Indian J Endocrinol Metab. 2013;17:S593–5.
Kalra S, Baruah MP, Gupta Y, Kalra B. Gestational diabetes: an onomastic opportunity. Lancet Diabetes Endocrinol. 2013;1:91.
Eades CE, Cameron DM, Evans JMM. Prevalence of gestational diabetes mellitus in Europe: a meta-analysis. Diabetes Res Clin Pract. 2017;129:173–81.
Collins J. Global epidemiology of multiple birth. Reprod Biomed Online. 2007;15:45–52.
Heino A, Gissler M, Hindori-Mohangoo AD, Blondel B, Klungsøyr K, Verdenik I, et al. Variations in multiple birth rates and impact on perinatal outcomes in Europe. PLoS ONE. 2016;11:e0149252.
Authors’ contributions
SBG was involved in study design, search in databases, quality assessment, study selection, data extraction, data analysis, manuscript drafting, and critical discussion. FRT conceptualized the study and was involved in study design, quality assessment, data analysis, revising manuscript, and critical discussion. MA contribute in quality assessment, data extraction, critical discussion, and manuscript drafting. RBY contributed in statistical analysis, interpreting data and manuscript drafting. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to acknowledge Ms. Niloofar Shive for critical editing of English grammar and syntax of the manuscript.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was approved by the ethics committee of the Research Institute for Endocrine Sciences and a written informed consent was obtained from all subjects before initiation of the study.
Funding
None.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1.
Table S1. Quality assessment of studies included using the Newcastle–Ottawa Quality Assessment Scale for cohort studies. Table S2. Quality assessment of included studies using the Newcastle–Ottawa Quality Assessment Scale for cross-sectional study. Figure S1. Flow chart of the literature search for the systematic review and meta-analysis. Figure S2. Bubble plot of Prevalence GDM vs. GDM diagnostic criteria*. Figure S3. Forest plot of Pooled Prevalence for region A in subgroup of GDM diagnostic criteria. Figure S4. Forest plot of Pooled Prevalence for region B in subgroup of GDM diagnostic criteria. Figure S5. Forest plot of Pooled Prevalence for region C in subgroup of GDM diagnostic criteria. Figure S6. Forest plot of Pooled Prevalence for region D in subgroup of GDM diagnostic criteria. Figure S7. Forest plot of Pooled Prevalence for region E in subgroup of GDM diagnostic criteria. Figure S8. Risk of bias in cross-sectional studies. Figure S9. Risk of bias in cohort studies.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Behboudi-Gandevani, S., Amiri, M., Bidhendi Yarandi, R. et al. The impact of diagnostic criteria for gestational diabetes on its prevalence: a systematic review and meta-analysis. Diabetol Metab Syndr 11, 11 (2019). https://doi.org/10.1186/s13098-019-0406-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13098-019-0406-1