
Abstract
Background
To evaluate the effect of upadacitinib on patient-reported outcomes (PROs) in patients with RA who had an inadequate response to csDMARDs.
Methods
Patients in SELECT-NEXT, a randomised controlled trial, were on a background of csDMARDs and received upadacitinib 15 mg and 30 mg or placebo daily for 12 weeks. PROs included Patient Global Assessment of Disease Activity (PtGA), pain, Health Assessment Questionnaire-Disability Index (HAQ-DI), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), duration and severity of morning (AM) joint stiffness, Short Form 36 Health Survey (SF-36), and Work Instability Scale for RA (RA-WIS). Least squares mean (LSM) changes were based on mixed-effect repeated measure models. Percentages of patients reporting improvements ≥ minimum clinically important differences (MCIDs) and scores ≥ normative values and number needed to treat (NNT) were determined; group comparisons used chi-square tests.
Results
Data from 661 patients were analysed. Compared with placebo, patients receiving upadacitinib reported statistically significant improvements (both doses, P < 0.05) in PtGA, pain, HAQ-DI, FACIT-F, duration and severity of AM stiffness, SF-36 (PCS and 6/8 domains), and RA-WIS at week 12. Significantly, more upadacitinib-treated patients (both doses, P < 0.05) reported improvements ≥ MCID in PtGA, pain, HAQ-DI, FACIT-F, AM stiffness, SF-36 (PCS and 4 or 7/8 domains), and RA-WIS and scores ≥ normative values in HAQ-DI, FACIT-F, and SF-36 (PCS and 4 or 5/8 domains). For most PROs, the incremental NNT with upadacitinib to report clinically meaningful improvement from baseline ranged from 4 to 8 patients.
Conclusions
Upadacitinib 15 mg or 30 mg daily for 12 weeks resulted in significant and clinically meaningful improvements in global disease activity, pain, physical function, fatigue, duration and severity of AM stiffness, HRQOL, and work instability among csDMARD-IR patients with RA.
Trial registration
Clinicaltrials.gov, NCT02675426. Retrospectively registered 5 February 2016.
Similar content being viewed by others

Background
Rheumatoid arthritis (RA) is a chronic, inflammatory, and destructive joint disease that is associated with substantial clinical burden [1]. Pain, fatigue, and morning (AM) stiffness are common symptoms associated with RA [2,3,4,5,6] and have an important negative impact on health-related quality of life (HRQOL) [7,8,9] and ability to work [10,11,12]. A recent survey identified pain, fatigue, and independence as the most important domains of RA disease activity that need to improve in patient-perceived remission [13]. Core patient-reported outcomes (PROs) including global assessment of disease, pain, physical function, fatigue, HRQOL, and work stability provide valuable insights into patients’ perspectives on their health status and impact of disease—improvements in PROs are considered important when evaluating the benefits of treatments [14,15,16,17,18]. Capturing the patient experience with these outcomes provides important information that can be used by clinicians to guide treatment decisions [19].
Janus kinase (JAK) inhibitors are a class of orally administered targeted synthetic disease-modifying antirheumatic drugs (tsDMARDs) that have recently received regulatory approval and are under evaluation in randomised controlled trials (RCTs) for the treatment of RA [20,21,22,23]. Upadacitinib, a selective JAK1 inhibitor, has demonstrated efficacy and a favourable benefit-to-risk profile in active RA among patients with inadequate responses to conventional synthetic disease-modifying antirheumatic drugs (csDMARD-IR) in phase 2 and 3 RCTs (NCT02066389; NCT02675426) [24, 25]. To assess the comprehensive benefits of upadacitinib, it is important to understand its impact on patient-centric outcomes. To this end, we examined the effect of two doses (15 mg or 30 mg daily) of upadacitinib versus placebo on PROs in SELECT-NEXT, an RCT assessing the efficacy and safety of upadacitinib in moderately to severely active csDMARD-IR RA patients.
Methods
Study design and participants
Full details of the study design of SELECT-NEXT (ClinicalTrials.gov, NCT02675426) were reported previously [24]. Patients were randomly assigned (2:2:1:1) to receive either upadacitinib 15 mg or 30 mg or placebo daily for 12 weeks while continuing background csDMARD therapy. After the initial 12-week placebo-controlled period, patients taking placebo received 15 mg or 30 mg of upadacitinib daily, according to the prespecified randomisation assignment. Patients, investigators, and the funder were masked to the treatment allocations. This report is based on post hoc analyses data collected during the placebo-controlled period of SELECT-NEXT. Study participants were ≥ 18 years of age, had active RA for ≥ 3 months, and received csDMARDs for ≥ 3 months with stable doses for ≥ 4 weeks before study entry and inadequate responses to ≥ 1 of the following csDMARDs: methotrexate (MTX), sulfasalazine, or leflunomide. The protocol allowed for enrolment of ≤ 20% with intolerance to at most one biologic DMARD (bDMARD); bDMARD-IR patients were excluded. The protocol was approved by the independent ethics committees or institutional review boards at all study sites. All participants provided written informed consent before enrolment. The RCT was conducted in accordance with the ethical principles that have their origin in the current Declaration of Helsinki and consistent with International Conference on Harmonisation Good Clinical Practice and Good Epidemiology Practices, along with all applicable local regulatory requirements. All patient data were de-identified and complied with patient confidentiality requirements.
Patient-reported outcomes
PROs were secondary outcome measures in the SELECT-NEXT trial. Patient Global Assessment of Disease Activity (PtGA) and the patient’s assessment of pain were measured using visual analogue scales (VAS) of 0 to 100 mm, with higher scores indicating greater disease activity and worse pain. Reductions of ≥ 10 mm in both PtGA and pain scores are the minimum clinically important difference (MCID). Physical function was assessed by the Health Assessment Questionnaire-Disability Index (HAQ-DI) [26, 27], with higher scores indicating worse physical function and greater disability; a reduction of ≥ 0.22 units is the MCID [28, 29], and a score ≤ 0.25 is the normative value [30]. Fatigue was assessed by the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) scale; scores range from 0 to 52, with higher scores indicating less fatigue [31], an increase of ≥ 4.0 points is defined as MCID [28], and a score of 43.6 as normative [32]. HRQOL was evaluated using the Medical Outcomes Short Form 36 Health Survey (SF-36), which assesses eight domains (Physical Functioning [PF], Role-Physical [RP], Bodily Pain [BP], General Health [GH], Vitality [VT], Social Functioning [SF], Role-Emotional [RE], and Mental Health [MH]), scored from 0 to 100 and aggregated into the physical component summary (PCS) and mental component summary (MCS) measures [33, 34], with normative values of 50 and standard deviations of 10. The SF-36 domain scores were compared with age- and gender-matched norms. Higher SF-36 scores indicate better health; the MCID is an increase of ≥ 2.5 points for SF-36 PCS and MCS and ≥ 5.0 points for individual SF-36 domains [28, 29]. Euro Qol 5-Dimension 5-Level Questionnaire (EQ-5D-5 L) was also used to assess HRQOL. EQ-5D-5 L has two components: a 0 to 100-mm VAS where 0 represents the worst imaginable health state and 100 represents the best imaginable health state and an index score, which has a maximum score of 1 representing the best health state [35, 36]. AM stiffness severity was reported on a numeric scale of 0 to 10, with higher scores indicating greater severity. Duration of AM joint stiffness was reported by the patient as the length of time, in minutes, that AM joint stiffness lasted on the day before each study visit. Because no values for MCID are reported in the literature, the proposed MCID for AM stiffness severity was defined as a reduction of ≥ 1 point, and the minimal important difference (MID) for AM stiffness duration was proxied at half the standard deviation of the mean baseline values. The Work Instability Scale for RA (RA-WIS) identifies patients at risk for disability-associated work instability, defined as a mismatch between an individual’s functional capabilities and job demands because of RA [37]. RA-WIS scores range from 0 to 23, with higher scores indicating a greater risk of work disability; scores < 10 are considered low risk, and MCID is a reduction of ≥ 5 points [38].
Statistical analyses
Changes from baseline at weeks 4 and 12, 95% confidence intervals, and nominal P values were analysed using a mixed-effect repeated measures model with unstructured variance-covariance matrix including treatment, visit, treatment-by-visit interaction, and prior bDMARD use as fixed factors and baseline value as a covariate. The assumptions of linear regression were checked and met for all outcomes included in the study except for AM stiffness duration and EQ-5D-5 L. Linear regression models were implemented for the analysis of AM stiffness duration and EQ-5D-5 L outcomes for consistency; given the large sample size, estimates are unlikely to be biassed. The results were expressed as least squares mean (LSM) changes. The baseline values and LSM changes for SF-36 domains were transformed based on the mean and standard deviation of the 1998 general US population. Analyses were performed in the full analysis set of all randomly assigned patients who received at least one dose of study drug.
The percentages of patients reporting improvements in PRO scores from baseline to week 12 ≥ MCID or scores ≥ normative values (age- and gender-matched for SF-36 only) at week 12 were compared between active treatment groups and placebo. Non-responder imputation was used when PRO data were missing. Comparisons between active treatment groups and placebo were made using chi-square tests. For each PRO, the incremental numbers needed to treat (NNTs) to achieve clinically meaningful improvements from baseline (≥ MCID or MID) were calculated as the reciprocal of the response rate differences between the active treatment groups and placebo. Times to response from baseline to week 12 were assessed for pain, HAQ-DI, and AM stiffness using Kaplan-Meier analysis. Median times to response were calculated for each dose group; comparisons between the groups used log-rank tests. P < 0.05 was considered significant.
Results
Study population
A total of 661 patients with active RA were randomised and treated (221 received upadacitinib 15 mg; 219 received upadacitinib 30 mg; 221 received placebo); of these, 618 (93%) completed the placebo-controlled 12-week period (14 patients in the placebo group, 11 patients in the upadacitinib 15-mg group, and 18 patients in the upadacitinib 30-mg group discontinued). Baseline characteristics were balanced across the 3 groups (Table 1). At baseline, 61% of patients had received MTX only, 21% a combination of MTX and another csDMARD, and 19% with only a csDMARD other than MTX. Thirteen percent of patients had prior bDMARD exposure; these patients were either intolerant or had < 3 months exposure to bDMARDs. Patients with an inadequate response to bDMARDs were excluded from entry. Across the groups, Disease Activity Score 28 using C-reactive protein (DAS28[CRP]) ranged from 5.6 to 5.7 and Clinical Disease Activity Index (CDAI) ranged from 37.8 to 38.6 indicating high baseline disease activity in this population.
Baseline mean PtGA scores ranged from 60.3 to 63.1, mean pain scores from 61.5 to 64.1, mean HAQ-DI scores from 1.4 to 1.5, and FACIT-F from 27.5 to 28.3 across the treatment groups (Table 2). Baseline HRQOL scores (as measured by SF-36 and EQ-5D-5 L) were low. SF-36 PCS was approximately 2.0 standard deviations (SD) < normative values of 50 indicating substantial impairment at baseline (Fig. 1). SF-36 MCS was approximately 0.5 SD less. SF-36 domain scores were low, so that baseline SF-6D utility scores, based on mean scores across all 8 domains [39, 40], were 0.57 in all 3 groups compared with 0.763 in the age/gender-matched normative population. The largest decrements from age and gender norms in both upadacitinib and placebo populations were in physical function (PF, − 33.3 to − 34.7), role physical (RP, − 32.7 to − 34.8), and bodily pain (BP, − 30.9 to − 32.4) domains. Baseline AM stiffness duration ranged from 129 to 152 min and severity from 6.1 to 6.2 (Table 2).

Baseline and post-treatment scores at week 12 across all Short Form 36 Health Survey domains. Baseline (BL) and SF-36 domain scores are relative to age- and gender-adjusted norms (A/G norms) for the general US population. a PBO. b UPA 15 mg. c UPA 30 mg. d Combined. In the combined spydergrams, most of the UPA 30-mg results are covered up by the UPA 15-mg results. BL values and SF-36 domain scores were re-scored from 0 to 100. No further transformations were applied for this analysis. BP, Bodily Pain; GH, General Health; MH, Mental Health; PBO, placebo; PF, Physical Functioning; RE, Role-Emotional; RP, Role-Physical; SF, Social Functioning; UPA, upadacitinib; VT, Vitality; Wk, week
Change from baseline
Statistically significant (P < 0.001) LSM changes from baseline to week 12 were reported with both upadacitinib 15 mg and 30 mg compared with placebo for all PROs (P < 0.001) except SF-36 MH with 15 mg, and SF-36 MCS, RE, and MH with 30 mg (Table 3). Duration of AM stiffness was reduced 63 to 67% from baseline after initiating upadacitinib.
Statistically significant LSM changes ([95% CI], P < 0.001) from baseline were reported as early as week 1 for PtGA (upadacitinib—15 mg, − 10.92 [− 13.87, − 7.97]; 30 mg, − 13.74 [− 16.67, − 10.80] versus placebo, − 3.17 [− 6.07, − 0.27], both P < 0.001), pain (upadacitinib—15 mg, − 11.38 [− 14.22, − 8.54]; 30 mg, − 13.80 [− 16.63, − 10.98] versus placebo, − 4.62 [− 7.41, − 1.82], both P < 0.001), HAQ-DI (upadacitinib—15 mg, − 0.25 [− 0.31, − 0.19]; 30 mg, − 0.24 [− 0.30, − 0.18] versus placebo, − 0.14 [− 0.19, − 0.08], both P < 0.001), AM stiffness severity (upadacitinib—15 mg, − 1.15 [− 1.42, − 0.88]; 30 mg, − 1.25 [− 1.52, − 0.98] versus placebo, − 0.40 [− 0.67, − 0.13], both P < 0.001), and AM stiffness duration (upadacitinib—30 mg, − 32.21 [− 46.49, − 17.94] versus placebo, − 9.75 [− 23.96, 4.47], P = 0.013).
Responder analysis
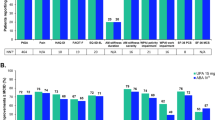
At week 12, significantly (P < 0.05) more upadacitinib-treated (15 mg and 30 mg) patients reported improvements ≥ MCID in PtGA, pain, HAQ-DI, FACIT-F, duration and severity of AM stiffness, RA-WIS, SF-36 PCS, and SF-36 MCS (15 mg only) and seven of eight SF-36 domains with 15 mg and four of eight SF-36 domains with 30 mg (Fig. 2a, b). Across most PROs, NNTs ranged from four to eight patients; NNTs ≤ 10 are considered clinically meaningful [41].

Percentage of patients reporting improvements ≥ MCID at week 12. a Patient’s Global Assessment of Disease Activity (PtGA), pain, Health Assessment Questionnaire-Disability Index (HAQ-DI), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), morning (AM) joint stiffness duration, AM stiffness severity, Work Instability Scale for RA (RA-WIS), and Short Form 36 Health Survey (SF-36). b SF-36 individual domains. Baseline values and SF-36 domains were re-scored from 0 to 100. ***P < 0.001, **P < 0.01, *P < 0.5 for upadacitinib versus placebo. BP, Bodily Pain; GH, General Health; MCID, minimum clinically important difference; MCS, mental component summary; MH, Mental Health; NNT, number needed to treat; PBO, placebo; PCS, physical component summary; PF, Physical Functioning; RE, Role-Emotional; RP, Role-Physical; SF, Social Functioning; UPA, upadacitinib; VAS, visual analogue scale; VT, Vitality
Patients treated with either dose of upadacitinib had a median time to response of 1 week for pain compared with 4 weeks for placebo; time to response for HAQ-DI and AM stiffness severity was also shorter for upadacitinib-treated patients (1 week for both upadacitinib doses versus 2 weeks for placebo).
Few patients in any group reported PRO scores ≥ normative values at baseline. The number of patients ranged from 2 (1%) for SF-36 PCS in the upadacitinib 30-mg group to 89 (41%) for SF-36 MCS in the upadacitinib 30-mg group (Fig. 3a). At week 12, the percentage of patients reporting scores ≥ normative values ranged from 18% (SF-36 PCS) to 57% (RA-WIS) with upadacitinib 15 mg and 15% (SF-36 PCS) to 50% (SF-36 MCS) with upadacitinib 30 mg, compared with 8% (SF-36 PCS) to 46% (SF-36 MCS) with placebo (Fig. 3a). Differences between the active and placebo treatment groups were statistically significant (P < 0.05) in HAQ-DI, FACIT-F, and SF-36 PCS with both upadacitinib doses versus placebo. Across SF-36 domains, the percentages of patients reporting scores ≥ normative values at 12 weeks ranged from 18% (RP) to 40% (RE) with upadacitinib 15 mg and 20% (RP) to 40% (VT, RE, and MH) with upadacitinib 30 mg, compared with 8% (RP) to 34% (RE and MH) with placebo, statistically significant (P < 0.05) in PF, RP, BP, and VT for both upadacitinib doses and GH with 30 mg (Fig. 3b).

Patients reporting scores ≥ normative values at baseline and week 12. a Health Assessment Questionnaire-Disability Index (HAQ-DI), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), Work Instability Scale for RA (RA-WIS), and Short Form 36 Health Survey (SF-36) PCS and MCS. b SF-36 individual domains. Baseline values and SF-36 domains were re-scored from 0 to 100. ***P < 0.001, **P < 0.01, *P < 0.5 for upadacitinib versus placebo. BL, baseline; BP, Bodily Pain; GH, General Health; MCS, mental component summary; MH, Mental Health; PBO, placebo; PCS, physical component summary; PF, Physical Functioning; RE, Role-Emotional; RP, Role-Physical; SF, Social Functioning; UPA, upadacitinib; VT, Vitality; Wk, week
Discussion
Upadacitinib treatment resulted in significant and clinically meaningful improvements in patient-reported disease activity, pain, physical function, fatigue, HRQOL, AM stiffness, and work instability in csDMARD-IR patients with RA. Improvements in PtGA, pain, HAQ-DI, and AM stiffness were reported as early as week 1. Patients not only reported improved PtGA, pain, HAQ-DI, AM stiffness, and FACIT scores, but also reported improvement in SF-36 domain scores that support these outcomes (PF, RP, BP, GH, and VT). There appears to be little difference in the treatment responses between the upadacitinib 15-mg and 30-mg doses, consistent with the reported primary efficacy results [24]. Most PROs assessed resulted in NNTs ≤ 10, which are generally considered favourable [41] and demonstrate the value of upadacitinib treatment for csDMARD-IR patients with RA.
Assessing the effect of upadacitinib on pain, physical function, fatigue, and AM stiffness is important because these outcomes directly impact HRQOL by reducing patients’ ability to perform daily activities and providing barriers to maintaining employment [42,43,44]. The Work Productivity and Activity Impairment Questionnaire (WPAI) is often used to assess work productivity [45]; however, this measure mainly assesses the time missed from work and impairment while working. Assessing work instability may be a more meaningful measure as it provides a means of screening for possible work disability and an opportunity for individuals to engage in early job retention interventions. In our study, we examined the effect of upadacitinib on work instability using RA-WIS, which identifies patients at risk of work absence or job transitions because of RA [37]. Job transitions are ways in which patients adapt to remain employed and include reducing work hours, taking a short leave of absence, or changing jobs or occupations [10]. Upadacitinib treatment markedly reduced the proportion of patients at risk of work instability. Fatigue is difficult to treat [46, 47], and there is strong evidence for an association between fatigue and other outcomes important from the patient perspective, such as pain, physical function, and depression [6, 43, 48]. This post hoc analysis demonstrated clinically meaningful improvements in fatigue as well as pain and physical function with upadacitinib treatment in csDMARD-IR patients with RA.
This RCT has several strengths of note. Several validated PROs reflecting different aspects of the patient experience were assessed in this study. The analyses performed in this study were comprehensive in nature as they not only examined the changes from baseline but also the proportion of patients reporting improvements ≥ MCID/MID criteria and population norms as well as the time to response for important patient-centric outcomes, such as pain and physical function. The use of MCID or MID criteria to measure response provides a context of how clinically meaningful these improvements are from a patient’s perspective. In addition, assessing the proportion of patients with improvements that reach normative values is a more stringent assessment criterion than MCID, and our results show that a statistically significant proportion of csDMARD-IR patients with RA reported this level of improvement with upadacitinib treatment.
This RCT also has limitations to be considered when interpreting the results. PROs were collected at fixed visits; therefore, responses were unavailable at other time points; however, differences in the outcomes occurred early and were maintained at week 12. The generalisability of these results to patients with milder disease may be limited because patients had moderately to severely active disease at enrolment. The method used to impute missing data (non-response imputation) assumes that missing PRO scores are associated with non-responses, which are stringent conditions and may underestimate the true rate of response.
Conclusions
Upadacitinib 15 mg and 30 mg daily resulted in rapid and clinically meaningful improvements in the outcomes important to patients including disease activity (per PtGA), pain, physical function, fatigue, HRQOL, AM stiffness, and work instability among csDMARD-IR patients with RA.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
09 June 2020
An amendment to this paper has been published and can be accessed via the original article.
Abbreviations
- AM:
-
Morning
- bDMARD:
-
Biologic disease-modifying antirheumatic drug
- BP:
-
Bodily pain
- CI:
-
Confidence interval
- csDMARD:
-
Conventional synthetic disease-modifying antirheumatic drug
- CCP:
-
Cyclic citrullinated peptide
- CDAI:
-
Clinical Disease Activity Index
- CRP:
-
C-reactive protein
- DAS28-CRP:
-
Disease Activity Score 28 using C reactive protein
- EQ-5D-5L:
-
Euro Qol 5-Dimension 5-Level Questionnaire
- FACIT-F:
-
Functional Assessment of Chronic Illness Therapy-Fatigue
- GH:
-
General Health
- HAQ-DI:
-
Health Assessment Questionnaire-Disability Index
- HRQOL:
-
Health-related quality of life
- IR:
-
Inadequate response
- JAK:
-
Janus kinase
- LSM:
-
Least squares mean
- MCID:
-
Minimum clinically important difference
- MCS:
-
Mental component summary
- MH:
-
Mental Health
- MID:
-
Minimal important difference
- MTX:
-
Methotrexate
- NNT:
-
Number needed to treat
- PBO:
-
Placebo
- PCS:
-
Physical component summary
- PF:
-
Physical Functioning
- PRO:
-
Patient-reported outcome
- PtGA:
-
Patient Global Assessment of Disease Activity
- RA:
-
Rheumatoid arthritis
- RA-WIS:
-
Work Instability Scale for RA
- RCT:
-
Randomised controlled trial
- RE:
-
Role-Emotional
- RF:
-
Rheumatoid factor
- RP:
-
Role-Physical
- SD:
-
Standard deviation
- SF:
-
Social functioning
- SF-36:
-
Short Form 36 Health Survey
- tsDMARD:
-
Targeted synthetic biologic disease-modifying antirheumatic drug
- UPA:
-
Upadacitinib
- VAS:
-
Visual analogue scale
- VT:
-
Vitality
- WPAI:
-
Work Productivity and Activity Impairment Questionnaire
References
Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388:2023–38.
Hewlett S, Cockshott Z, Byron M, Kitchen K, Tipler S, Pope D, et al. Patients’ perceptions of fatigue in rheumatoid arthritis: overwhelming, uncontrollable, ignored. Arthritis Rheum. 2005;53:697–702.
Kirwan JR, Hewlett S. Patient perspective: reasons and methods for measuring fatigue in rheumatoid arthritis. J Rheumatol. 2007;34:1171–3.
da Silva JA, Phillips S, Buttgereit F. Impact of impaired morning function on the lives and well-being of patients with rheumatoid arthritis. Scand J Rheumatol Suppl. 2011;125:6–11.
Halls S, Dures E, Kirwan J, Pollock J, Baker G, Edmunds A, et al. Stiffness is more than just duration and severity: a qualitative exploration in people with rheumatoid arthritis. Rheumatology (Oxford). 2015;54:615–22.
Pollard LC, Choy EH, Gonzalez J, Khoshaba B, Scott DL. Fatigue in rheumatoid arthritis reflects pain, not disease activity. Rheumatology (Oxford). 2006;45:885–9.
Matcham F, Scott IC, Rayner L, Hotopf M, Kingsley GH, Norton S, et al. The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: a systematic review and meta-analysis. Semin Arthritis Rheum. 2014;44:123–30.
Strand V, Khanna D. The impact of rheumatoid arthritis and treatment on patients’ lives. Clin Exp Rheumatol. 2010;28:S32–40.
Taylor PC, Moore A, Vasilescu R, Alvir J, Tarallo M. A structured literature review of the burden of illness and unmet needs in patients with rheumatoid arthritis: a current perspective. Rheumatol Int. 2016;36:685–95.
Tang K, Beaton DE, Gignac MA, Lacaille D, Zhang W, Bombardier C. The Work Instability Scale for rheumatoid arthritis predicts arthritis-related work transitions within 12 months. Arthritis Care Res (Hoboken). 2010;62:1578–87.
Sokka T, Kautiainen H, Pincus T, Verstappen SM, Aggarwal A, Alten R, et al. Work disability remains a major problem in rheumatoid arthritis in the 2000s: data from 32 countries in the QUEST-RA study. Arthritis Res Ther. 2010;12:R42.
Westhoff G, Buttgereit F, Gromnica-Ihle E, Zink A. Morning stiffness and its influence on early retirement in patients with recent onset rheumatoid arthritis. Rheumatology (Oxford). 2008;47:980–4.
van Tuyl LH, Sadlonova M, Hewlett S, Davis B, Flurey C, Goel N, et al. The patient perspective on absence of disease activity in rheumatoid arthritis: a survey to identify key domains of patient-perceived remission. Ann Rheum Dis. 2017;76:855–61.
Nikiphorou E, Radner H, Chatzidionysiou K, Desthieux C, Zabalan C, van Eijk-Hustings Y, et al. Patient global assessment in measuring disease activity in rheumatoid arthritis: a review of the literature. Arthritis Res Ther. 2016;18:251.
Orbai AM, Bingham CO 3rd. Patient reported outcomes in rheumatoid arthritis clinical trials. Curr Rheumatol Rep. 2015;17:28.
Boers M, Kirwan JR, Wells G, Beaton D, Gossec L, d’Agostino MA, et al. Developing core outcome measurement sets for clinical trials: OMERACT filter 2.0. J Clin Epidemiol. 2014;67:745–53.
Kirwan JR, Tugwell PS. Overview of the patient perspective at OMERACT 10--conceptualizing methods for developing patient-reported outcomes. J Rheumatol. 2011;38:1699–701.
Sanderson T, Morris M, Calnan M, Richards P, Hewlett S. What outcomes from pharmacologic treatments are important to people with rheumatoid arthritis? Creating the basis of a patient core set. Arthritis Care Res (Hoboken). 2010;62:640–6.
Fautrel B, Alten R, Kirkham B, de la Torre I, Durand F, Barry J, et al. Call for action: how to improve use of patient-reported outcomes to guide clinical decision making in rheumatoid arthritis. Rheumatol Int. 2018;38:935–47.
Burmester GR, Blanco R, Charles-Schoeman C, Wollenhaupt J, Zerbini C, Benda B, et al. Tofacitinib (CP-690,550) in combination with methotrexate in patients with active rheumatoid arthritis with an inadequate response to tumour necrosis factor inhibitors: a randomised phase 3 trial. Lancet. 2013;381:451–60.
Genovese MC, Kremer J, Zamani O, Ludivico C, Krogulec M, Xie L, et al. Baricitinib in patients with refractory rheumatoid arthritis. N Engl J Med. 2016;374:1243–52.
Kavanaugh A, Kremer J, Ponce L, Cseuz R, Reshetko OV, Stanislavchuk M, et al. Filgotinib (GLPG0634/GS-6034), an oral selective JAK1 inhibitor, is effective as monotherapy in patients with active rheumatoid arthritis: results from a randomised, dose-finding study (DARWIN 2). Ann Rheum Dis. 2017;76:1009–19.
Westhovens R, Taylor PC, Alten R, Pavlova D, Enriquez-Sosa F, Mazur M, et al. Filgotinib (GLPG0634/GS-6034), an oral JAK1 selective inhibitor, is effective in combination with methotrexate (MTX) in patients with active rheumatoid arthritis and insufficient response to MTX: results from a randomised, dose-finding study (DARWIN 1). Ann Rheum Dis. 2017;76:998–1008.
Burmester GR, Kremer JM, Van den Bosch F, Kivitz A, Bessette L, Li Y, et al. Safety and efficacy of upadacitinib in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying anti-rheumatic drugs (SELECT-NEXT): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2018;391:2503–12.
Genovese MC, Smolen JS, Weinblatt ME, Burmester GR, Meerwein S, Camp HS, et al. Efficacy and safety of ABT-494, a selective JAK-1 inhibitor, in a phase IIb study in patients with rheumatoid arthritis and an inadequate response to methotrexate. Arthritis Rheumatol. 2016;68:2857–66.
Bruce B, Fries JF. The Health Assessment Questionnaire (HAQ). Clin Exp Rheumatol. 2005;23:S14–8.
Ramey D, Fries JF, Singh G. The Health Assessment Questionnaire 1995 – status and review. 2nd ed. Philadelphia: Lippincott-Raven; 1996.
Kitchen H, Hansen B, Abetz L, Højbjerre L, Strandber-Larsen M. Patient-reported outcome measures for rheumatoid arthritis: minimal important differences review. Arthritis Rheum. 2013;65(Suppl 10):abstract 2268.
Strand V, Boers M, Idzerda L, Kirwan JR, Kvien TK, Tugwell PS, et al. It’s good to feel better but it’s better to feel good and even better to feel good as soon as possible for as long as possible. Response criteria and the importance of change at OMERACT 10. J Rheumatol. 2011;38:1720–7.
Krishnan E, Sokka T, Hakkinen A, Hubert H, Hannonen P. Normative values for the Health Assessment Questionnaire disability index: benchmarking disability in the general population. Arthritis Rheum. 2004;50:953–60.
Cella D, Yount S, Sorensen M, Chartash E, Sengupta N, Grober J. Validation of the functional assessment of chronic illness therapy fatigue scale relative to other instrumentation in patients with rheumatoid arthritis. J Rheumatol. 2005;32:811–9.
Kavanaugh A, Gladman DD, Edwards CJ, Poder A, Lioté F, Bird P, et al. Apremilast, an oral phosphodiesterase 4 inhibitor, is associated with long-term (104-week) improvmeent in fatigue in patients with psoriatic arthritis: pooled results from 3 phase III, randomized, controlled trials. Ann Rheum Dis. 2016;75(Suppl 2):346.
Ware JE Jr, Sherbourne CD. The MOS 36-item Short-Form Health Survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473–83.
Brazier JE, Harper R, Jones NM, O’Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ. 1992;305:160–4.
Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20:1727–36.
Shaw JW, Johnson JA, Coons SJ. US valuation of the EQ-5D health states: development and testing of the D1 valuation model. Med Care. 2005;43:203–20.
Gilworth G, Chamberlain MA, Harvey A, Woodhouse A, Smith J, Smyth MG, et al. Development of a work instability scale for rheumatoid arthritis. Arthritis Rheum. 2003;49:349–54.
Revicki D, Cifaldi MA, Safikhani S, Chen N, Ganguli A. Responsiveness and minimal important difference of the rheumatoid arthritis-work instability scale (RA-WIS). Ann Rheum Dis. 2013;72:A867.
Ara R, Brazier J. Deriving an algorithm to convert the eight mean SF-36 dimension scores into a mean EQ-5D preference-based score from published studies (where patient level data are not available). Value Health. 2008;11:1131–43.
Ara R, Brazier J. Predicting the short form-6D preference-based index using the eight mean short form-36 health dimension scores: estimating preference-based health-related utilities when patient level data are not available. Value Health. 2009;12:346–53.
Siwek J, Newman DH. Introducing medicine by the numbers: a collaboration of the NNT group and AFP. Am Fam Physician. 2015;91:434–5.
Breedveld FC, Han C, Bala M, van der Heijde D, Baker D, Kavanaugh AF, et al. Association between baseline radiographic damage and improvement in physical function after treatment of patients with rheumatoid arthritis. Ann Rheum Dis. 2005;64:52–5.
Wolfe F, Michaud K. Predicting depression in rheumatoid arthritis: the signal importance of pain extent and fatigue, and comorbidity. Arthritis Rheum. 2009;61:667–73.
Lacaille D, White MA, Backman CL, Gignac MA. Problems faced at work due to inflammatory arthritis: new insights gained from understanding patients’ perspective. Arthritis Rheum. 2007;57:1269–79.
Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4:353–65.
Walter MJM, Kuijper TM, Hazes JMW, Weel AE, Luime JJ. Fatigue in early, intensively treated and tight-controlled rheumatoid arthritis patients is frequent and persistent: a prospective study. Rheumatol Int. 2018;38:1643–50.
van Steenbergen HW, Tsonaka R, Huizinga TW, Boonen A, van der Helm-van Mil AH. Fatigue in rheumatoid arthritis; a persistent problem: a large longitudinal study. RMD Open. 2015;1:e000041.
Nikolaus S, Bode C, Taal E, van de Laar MA. Fatigue and factors related to fatigue in rheumatoid arthritis: a systematic review. Arthritis Care Res (Hoboken). 2013;65:1128–46.
Acknowledgements
Medical writing assistance was provided by Joann Hettasch, PhD, of JK Associates, Inc., a member of the Fishawack Group of Companies, Conshohocken, PA, and was funded by AbbVie.
Funding
This work was supported by AbbVie. The study sponsor participated in the interpretation of data, review, and approval of the article.
Author information
Authors and Affiliations
Contributions
All authors contributed to the conception and design; acquisition, analysis, and interpretation of the data; and drafting of the manuscript. All authors revised the manuscript for important intellectual content, approved the final version to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol was approved by the independent ethics committees or institutional review boards at all study sites. All participants provided written informed consent before enrolment. The RCT was conducted in accordance with the ethical principles that have their origin in the current Declaration of Helsinki and consistent with International Conference on Harmonisation Good Clinical Practice and Good Epidemiology Practices, along with all applicable local regulatory requirements. All patient data were de-identified and complied with patient confidentiality requirements.
Consent for publication
Not applicable.
Competing interests
VS is a consultant for AbbVie, Amgen, AstraZeneca, BMS, Celgene, Genentech, GSK, Janssen, Lilly, Novartis, Pfizer, Regeneron, Sanofi, and UCB, and is involved in the advisory boards for AbbVie, Amgen, AstraZeneca, BMS, Celgene, Genentech, GSK, Janssen, Lilly, Novartis, Pfizer, Regeneron, Sanofi, and UCB. JP is a consultant for AbbVie, Amgen, BMS, Celltrion, GSK, Lilly, Merck, Novartis, Pfizer, Roche, Sandoz, Sanofi, and UCB. NT, AF, HSC, AP, AG, and MF are employees of AbbVie and may own AbbVie stock or stock options. DG is an employee of Analysis Group, Inc., which received consulting fees from AbbVie for this study. MS is a consultant for AbbVie, BMS, Eli Lilly, JNJ, and UCB, and is a member of the speaker bureau for AbbVie and BMS.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Strand, V., Pope, J., Tundia, N. et al. Upadacitinib improves patient-reported outcomes in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying antirheumatic drugs: results from SELECT-NEXT. Arthritis Res Ther 21, 272 (2019). https://doi.org/10.1186/s13075-019-2037-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13075-019-2037-1