
Abstract
Background
Indigenous communities use wild plants to cure human ailments since ancient times; such knowledge has significant potential for formulating new drugs and administering future health care. Considering this, the present study was undertaken to assess use value, diversity, and conservation concerns of medicinal plants used in traditional herbal care system of a marginal hill community in Bageshwar district of Uttarakhand in the Central Himalayan region of India.
Methodology
Extensive surveys were made in 73 villages to gather information on the ethnomedicinal use of plant species used in the traditional herbal healing system. A total of 100 respondents were identified (30 herbal healers called Vaidyas and 70 non-healers/natives) and interviewed using semi-structured questionnaires, target interviews, and group discussion. Some important indices such as the use-value index (UV), relative frequency citation (RFC), cultural importance index (CI), and informant consensus factor (Fic) were calculated for the medicinal plants included in the present study.
Result
It was recorded that the community uses a total of 70 species with 64 genera and 35 families for curing various ailments. Family Lamiaceae recorded the maximum number of medicinal plants. Twenty-one species used most extensively in the traditional health care system. The major parts of the identified plants used for the treatment of various ailments were root/rhizome and leaf. The most common methods used for the preparation of these plants were decoction and infusion. Ocimum basilicum L., Cannabis sativa L., Citrus aurantifolia (Christm) Sw., Curcuma longa L., and Setaria italica L. had the highest rate of use report. RFC value ranged between 0.03 and 0.91 with highest values for Setaria italica, Zingiber officinale, Ocimum basilicum, and Raphanus sativus. The traditional knowledge is passed verbally to generations and needs to be preserved for the future bio-prospecting of plants that could be a potential cure to any future disease.
Conclusion
In recent years, the community has access to modern hospitals and medicinal facilities, although a considerable number still prefer medicinal plants for curing select ailments. It is suggested that these ethnomedicinal species need to be screened and evaluated further for their effectiveness for pharmacological activity. Also, significant efforts are required to conserve traditional knowledge and natural habitats of wild medicinal plants.
Similar content being viewed by others


Background
Medicinal plants have been utilized for the treatment of various diseases since ancient times, thus form an important element of aboriginal curative systems. The Indian Rishis first documented the use of medicinal plants in the form of Samhitas. Charak Samhita (1000–800 BC) and Shushrut Samhita (800–700 BC) by Maharshi Charak and and Maharshi Shashurut, respectively, are the baselines of the Indian Medicinal System. Maharshi Charak mentioned over 500 medicinal plants, out of which 340 plants used in the production of herbal medicine [1, 2]. AYUSH (i.e., Ayurveda, Unani, Siddha, and Homeopathy) is another traditional Indian health care system that is considered a great knowledge base in herbal medicines. Ayurveda reports over 2000 medicinal plant species, Siddha 1121 plant species, Unani 751 species, and homeopathy 422 species [3]. Nearly 70–80% population worldwide still relies on traditional medicinal systems for their primary health care because of their effectiveness, cultural preferences, and lack of modern health care alternatives [4, 5]. The global demand for herbal medicine continues to increase over the past few decades. The earlier studies stated that out of 250,000 flowering plants in the world, only less than 10% have been screened so far for their medicinal potency, and still, 90% remains unexplored [2]. In recent times, there is an increased interest regarding the use of the medicinal plants to develop new drugs and medicines for fulfilling the demand of a growing population [6,7,8]. Therefore, the information on plants of ethnomedicinal importance holds high potential. Uttarakhand Himalaya is a mountainous region in northern India that has a unique geography, rich biological resources, cultural heritage, and diverse climatic conditions which supports the highest number of medicinal plant species [9]. Over two-third population live in rural areas and depend on diverse natural resources to fulfill their need for food, fuel, fodder, timber, medicine, etc. Communities use a large variety of medicinal plants for treating diverse ailments [10, 11]. However, it is strongly being realized that the indigenous knowledge related to herbal medicines is continuously being eroded despite high significance to humanity. The subject needs further research such as documentation of potential medicinal species, analyzing their active constituents, clinical trials for validations, and developing new drugs and medicines [8,9,10,11,12]. Considering this, the present study was undertaken. We argue that sustainable management and conservation of medicinal plants can be achieved when information about their use for treating ailments and traditional herbal practices within particular areas are available. Such information is strongly desired to be preserved from being lost for the use of both the present and the future generations. For the purpose of this study, we selected marginal community and local herbal practitioners (Vaidyas) of Bageshwar district in Uttarakhand state in north India and documented ethnomedicinal plant diversity and traditional medicinal practices being used by them. Efforts were also made to scientifically validate and interpret the data using several indices such as relative frequency citation (RFC), use report (categorical and disease-based), cultural importance index (CI), and informant consensus index (Fic) so as to verify the homogeneity, importance, and the cultural similarity of the medicinal plants in communities. It is expected that the qualitative and quantitative information generated from the study will have immense utility for the conservation and sustainable utilization of medicinal plants as well as for managing the traditional health care system.
Materials and methods
Study area
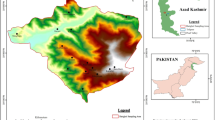
This study aimed to investigate the medicinal species used by the marginal hill community living in remote and high-altitude areas where medical health care facilities are not easily available. These practices are being used since eternity descended from the inherited knowledge of the locals and indigenous population of Uttarakhand. The study was carried out at Bageshwar district (geographical area 1687.8 km2) of Uttarakhand state and lies between latitudes 29° 42′ 40″ to 30° 18′ 56″ N and longitudes 79° 23′ to 80° 10′ E (Fig. 1). The district is situated on the confluence of Gomti river and Saryu river which is a tributary of Kali river. It is bounded by Almora district in the southwest, Chamoli district in the north and northwest, and Pithoragarh district in the east. Administratively, the district is divisible into four Tehsils, viz., Bageshwar, Kapkot, Kanda (Sub-tehsil), and Garur, and three blocks, viz., Bageshwar, Garur, and Kapkot. There are 947 revenue villages, out of which 874 villages are inhabited, and 73 villages are uninhabited. As per the 2011 census, the total population of Bageshwar district is 259,898 (male 48%, female 52%) with 96% living in the rural areas.

Study area and villages in Garur and Kapkot Bolcks of District Bageshwar, Uttarakhand, India
The community of the area is divided into 3 categories, viz., General, Scheduled Class (SC), Scheduled Tribe (ST), and majority of them involved in primary sector (agricultural activities), while some also work in secondary and tertiary sectors, such as private works, businesses, and government jobs. As such, the community is highly marginal with small and scattered land holdings, low production, and low income, therefore, highly dependent on natural resources. Male population out-migrates to earn better livelihoods that lead to continuous increase in fallow lands and culturable waste lands.
Data collection
The study was conducted in 39 villages covering Garur-Ganga valley (23 villages) and Saryu valley (16 villages) of Garur and Kapkot Blocks during 2016–2018. To fulfill the objectives of the study, extensive field visits were made to gather information from traditional herbal healers (Vaidyas) and indigenous people using semi-structured questionnaires, target interviews, and visual interpretation through snowball methodology. A total of 100 respondents were randomly selected for the present study from both valleys, 37 being male and 63 female respondents. Of them, 30 were Vaidyas (male 19, female 11). Female informants were given preference in view of their dominance in villages. The age group of informants varied between 30 and 83 years, although most of them were between 50 and 65 years of age (Fig. 2). The questionnaire contains information about the ethnomedicinal plants with their local name, parts used, habit, ailment treated by medicinal plants, and mode of utilization of herbal formulation. Two general meetings and interviews were also organized at each valley with Vaidyas and natives. The documented medicinal plant species were validated for identification using available literature [13,14,15,16]. The specimens matched with the herbarium lodged in CCRAS-RARI, Tarikhet, Ranikhet, Uttarakhand (acronym RKT), which houses largest medicinal plant herbariums in northern India. A few generally available species were matched with the plant database of Centre for Socio-Economic Development deposited at G.B. Pant National Institute of Himalayan Environment (GBP-NIHE), Almora, Uttarakhand.

Age distribution of respondents
The ethnobotanical analysis
The information on ethnomedicinal important species were recorded including the local names of the species, habit, their uses in different forms, the part used in the medical practice, mode of administration, and the condition of the plant (fresh or dry). The plants were classified into 12 main categories of ailments which were further divided into different respective subcategories based on disease and affected body part. The data were then statistically analyzed for different parameters. To enhance the indicative value of the ethnomedicinal study, suitable quantitative methods and approaches were used in the form of indices, such as relative frequency of citation (RFC), use report (based on illness, based on taxa), cultural importance (CI), and consensus factor of informants (Fic).
Use-report values (UR) provides information on the total number of reported uses for each species. It is similar to the use value of a species, but for use report, the number of events (interviews), the process of asking one informant on one day about the uses they know for one species, is one because the respondents were interviewed only once. And response use values are broken down by the number of uses reported for each plant species part.
Use-value index (UV) depicts the importance of each species for each informant and calculated by UV = ∑U/N formula where U is the number of uses quoted in each interview by N, number of informants. Use values are high when there are many useful reports for a plant representing its importance and come within reach to zero (0) when the use reports are low [17].
Relative frequency citation (RFC) index reveals the usage importance of a particular species used by different informants. The index is calculated by dividing the total number of informants referring to a particular taxon with the total number of informants (RFC = FC/N) where FC is the total number of informants that referred to the taxon, and N is the total number of informants [18].
Cultural importance index (CI) is estimated for each locality as the summation of Use-Report (UR) in every use category mentioned for a species in the locality divided by the total number of informants. This index provides an implication of the involvement of a particular taxon in the community, and a greater value signifies that a particular is widely distributed among communities. A null value indicates non-existence of the species in the area. CI is calculated as CI = UR/N where UR is the total number of use reports for each species in every category of illness mentioned, and N is the total number of informants [19].
Informant consensus factor (Fic) is used to test the consistency of information knowledge in treating a particular illness category. The values obtained are near one (1) for well-defined selection criteria in the community and/or if the information is exchanged between the informants. A value approaching zero (0) represents that the plants are chosen randomly, and/or there is no information exchanged between the communities about their use. Fic is calculated as Fic = (Nur − Nt)/(Nur − 1), where Nur refers to the number of use reports for a particular use category, and Nt refers to the number of taxa used for a particular use category by all informants [20].
Result and discussion
Ethnomedicinal uses of plants and mode of practice
The residents of different age groups were surveyed to assess the ethnomedicinal uses of plant species (Fig. 2). The survey revealed that a total of 70 medicinal plant species varying from 35 families and 64 genera have been used by the inhabitants of 39 villages for different (Table 1). Family Lamiaceae recorded maximum species (8) followed by Asteraceae (6 species), Fabaceae (5 species), Rosaceae (4 species), and Apiaceae, Liliaceae, Ranunculaceae, Rutaceae, and Zingiberaceae (3 species each). The remaining families were represented with just one or two species. Almost all the species are widely used by the community. Of the total documented medicinal plant species, the herbaceous habit (51 species) was the most dominant life form, followed by the tree (10), shrub (7), and climbers (2 species) (Fig. 3).

Distribution of medicinal plants in different life form
It was interesting to note that nearly 70% population still use prescription of Vaidyas for common ailments, although the Vaidyas were having an age of > 50 years. The diseases cured by Vaidyas comprised fever, stomach problems, cough, cold, headache, etc. The most common plant parts used were root/rhizome, followed by leaf, whole plant, seeds, fruits, flower, and bulb and latex (Fig. 4). The collection of plant parts was very selective keeping into consideration the time of collection, plant matureness, and quantity of use thus ensuring a conservation approach. Vaidyas comprised sound knowledge and a species-specific method of preparing drugs to cure various ailments (Table 2). Making decoction and ingestion was the most common mode of plant part use (Fig. 5). Poultice and cooking were also favored for many medicinal plants. Another mode of application includes cooking and making into powder (9.42%), direct application (7.97%), emulsion and infusion (5.80%), and ointment (2.17%) (Fig. 5). A decoction is the most commonly used method to cure ailments in traditional herbal systems [21,22,23,24,25]. It is considered to extract all potential bioactive compounds after heating [26]. The pleasant taste of the herbal drug can be attuned by adding together honey or sugar [27]. Ingestion and poultice were also common after crushing and/or mixing the plant parts with some solvent for application as paste and Band-Aid. In skeletal, muscle, and dermatological issues, application of plant parts as ointment was most prevalent.

Plant part used in preparation of medicine

Processing of plant parts in preparation of medicine
The community and Vaidyas identify each medicinal plant with a specific vernacular name. For example, Bergenia ciliata is identified by the community with a local name “Pattharchatta” (stone destroyer), and it is used in curing kidney stones. Plantago ovate is called “Jonkpuri” (jonk resembles worms) and is used in the treatment of Ascaris and other worms. Viola betonicifolia named “Garur-Jadi” (Garur means eagle), and it is used as an antidote to treat snake bites. Commonly, the community identifies a native name for species based on its local uses, ecology, physiology, anatomy, pharmacological activity, etc. [28].
It was recorded that the species were used to cure a total of 12 major ailments (Fig. 6). Most species were used for curing gastrointestinal and general health disorders. It was followed by species used for treating dermatological and respiratory problems.

Distribution of medicinal plants in different ailments category
Lamiaceae has been the most dominating family for ethnomedicinal uses in the trans-Himalayan zone of Nepal [29] and Garhwal Himalaya in India as well [30]. Although the people in remote areas are still dependent on the traditional herbal cure system, it is being practiced by a few elderly people only. The young generation is not interested to take up this profession given minimal profit [3, 10, 12]. The common plant parts used in the present study are similar to other investigations [31,32,33,34,35]. The roots being the storage part of the plant contain valuable bioactive compounds [36]. Apart from the root part, leaves also contain a high concentration of health-beneficial secondary metabolites, phytochemicals, and essential oils, which contribute significantly to phototherapy or treatment of various health disorders [37,38,39,40]. The study reports 60% more species than reported earlier for the area under investigation [41,42,43,44,45].
Quantitative analysis of ethnomedicinal information
The use value of important ethnomedicinal species was also calculated to depict the number of uses reported by the informants related to the utility of a species for a specific ailment or different ailments (Tables 1 and 3). Two forms of use reports were analyzed; the URc defines the use of a particular species to cure specific ailments as reported by all the informants, while URd reports the sum of all the uses for a particular disease/ailment. Ocimum basilicum, Cannabis sativa, Citrus aurantifolia, Curcuma longa, and Setaria italica have been top positioned in terms of use-reports and different ailments cured.
The usefulness of a species can be represented through its RFC value, which ranged 0.03 to 0.91 for different species (Table 1). Species with maximum RFC value were Setaria italica, Zingiber officinale, Ocimum basilicum, and Raphanus sativus which depict their higher use, while those with the least value comprised Duchesnea indica and Thalictrum foliosum.
The cultural importance index (CIs) specifies the distribution and importance of species in traditional herbal system, and the value ranged from 0.03 to 0.97. A total of 21 species have been identified as the most commonly used (Table 3). Ocimum basilicum, Cannabis sativa, and Citrus aurantifolia registered the highest cultural importance in the traditional herbal cure system. Low CI values specify that these species are either least used, or their use is declining in traditional herbal cure system [46].
An analysis of the informant consensus factor (Fic) for 12 broad treatment categories ranged between 0.92 and 1.0 (Table 4). The data revealed high homogeneity as per local people for all treatments. The immuno-regulatory category was assigned the value 1 due to the presence of only one taxon in the particular category. Apart from this, hepatic health care and urogenital categories obtained the value of 0.98 indicating well-defined criteria among the local population and non-random selection of species for the ailment category. Asparagus recemosus, Glycine max, Hordeum vulgare, Polygonatum cirrhifolium, Punica granatum, Raphanus sativus, and Urtica dioica not only used in hepatic health care but also provide nutritive benefits and warm potency, particularly at higher altitude areas. These species are commonly used in the daily food habit of the local community. Also, a higher value of Fic verifies the distribution of the different species used for a specific ailment. The urogenital category, with only 4 taxa included, comes second in terms of CI as there is a widely accepted notion of using these species for such disorders. The higher value of informant consensus factor for all the ailment categories also implies that the documented species are the most commonly used in traditional healing system.
The gastrointestinal ailments comprised of 695 use reports from the total categories with a medicinal importance index value of 30.22 (Table 4). Some most sought species in this category are Cannabis sativa, Citrus aurantifolia, Angelica galuca, Ajuga parviflora, and Emblica officinalis. These species are placed following their use reports mentioned during data collection. In the category of general health care, 22 species are being used with 524 numbers of use-reports and medical importance of 23.82. The species indicated with the highest number of use-reports are Ocimum basilicum, Citrus aurantifolia, Curcuma longa, Ajuga parviflora, and Picrorhiza kurrooa based on user reports. The dermatological category ranks third with 21 taxa in use and a use-report value of 617 and medicinal importance of 29.82. The main species employed for this category based on the use reports are Setaria italica, Eupatorium adenophorum, and Artemisia martima. Although the hepatic health cure category comprised of only 8 taxa, it has a medicinal importance index value of 45.50, which is highest of all the categories since the species used under the category are of daily usage and are often included in daily food products with nutritive values. The species include Glycine max, Hordeum vulgare, Punica granatum, Urtica dioica, Polygonatum cirrhifolium, etc. In other works carried out in Uttarakhand, they have reported these medicinal plants and use different plant parts in a different ratio to cure disease or aliments [16, 30, 31, 41,42,43, 45, 47,48,49].
A correlation analysis was done among RFC, CI, UR, number of species used in treating different ailments, informant consensus factor (Fic), and medical importance. No evidence of any correlation was observed in most of the parameters; a highly positive correlation was only observed in the number of taxa used and the number of use reports (0.963). Also, there has been a moderately positive correlation observed between Fic and RFC which is of no significance in the study as both the parameters have been described differently.
Some species are also used in ethnoveterinary purposes for curing domestic animals. Ajuga parviflora is used to cure throat infection, Coriandrum sativum against poison, and Taraxacum officinale, Verbascum thapsus, and Viola canescens to increase lactation in milking animals.
The weakening of traditional ethnobotanical knowledge
It is alarming to note that there has been a continued decline in traditional ethnobotanical knowledge in the target area (Fig. 7). An analysis of community perception on change in use pattern of medicinal plants in 2018 and a decade earlier (i.e., 2008) revealed that there is less number of species used for curing different ailments in recent years (Table 5). People are moving away from traditional herbal cure system, and the young generation has no interest in the traditional customs and values. Earlier, the people of remote areas preferred to consult with Vaidyas for primary healthcare, but in the last decade, since there is an increase in accessibility, availability, and affordability towards the allopathic medicinal system, the local community is also opting for such options. Despite that 57% of the total respondents believe that these plants are highly effective, 30% found moderately effective, while only 13% feel it less effective (Fig. 8). Interestingly, to cure selective diseases in children, such as Juga (removal of Ascaris), Chupad (heavy cough), and Kasar (constipation), still people prefer traditional cure systems as it has no side effects. During the study, it was observed that the Vaidyas do not share their knowledge; they believed that the treatment will not be effective if they share the knowledge with anybody. In the changing lifestyle and socioeconomic scenarios, most of the inhabitants are reluctant to live with their traditional heritage leading to the vanishing of the knowledge [58].

Past (2008) and present (2018) use of plants in traditional health care system

Community view points on effectiveness of traditional health care system
Conclusions
Community knowledge on the use and management of wild plant resources has always been integral to the survival, sustenance, and adaptation of human cultures [47, 53, 58]. This study revealed 70 medicinal plant species being used by the local marginal community of which 21 are the most extensively used species to treat various ailments. The significance of the traditional herbal healing system is highly relevant due to its effectiveness. It is cost-effective and based on local resources and still only means of cure for marginal communities in remote localities of Uttarakhand. With population growth and lack of health care, there is a need to adhere to the locally available resources to be utilized for general health care and provisioning of suitable side-effect free treatment to the communities. The community still uses these species; however, the level of use is decreasing because of upcoming modern allopathic based health care services. At the same time, there is also a decline in the number of local Vaidyas and herbal practitioners. This is because of increased access to modern hospitals and medicinal facilities in recent times. This possesses a significant challenge to the continuity of the traditional herbal cure system. The impoverishment of such knowledge may lead to an enormous loss to the scientific community. The ethnomedicinal knowledge and information provided in this study are of significant value for scientific validation, product development, conservation, and policy planners for sustainable management of medicinal plants and traditional herbal cure system. It is suggested to explore and establish linkage between traditional health practices and modern health care systems. It can be done by testing bioactive compound and biological activity of most preferred plant species and assessing the safety and efficacy of the local herbal formulation. Such an investigation may lead to many new and novel drug discovery. It is also recommended that the natural habitats of medicinal plants should be protected for the conservation of valuable gene pool and to control the exploitation of species. Since ethnomedicinal information is strongly linked to local livelihoods, culture, and environment, it is strongly recommended to further continue studying the subject to serve humanity with healthier and operative health care measures.
Availability of data and materials
The authors already included all data in the manuscript collected during the field surveys. The documented medicinal plant species were deposited at Centre of Socio-economic Development (CSED), GBPNIHE, Kosi-Katarmal, Almora, Uttarakhand.
References
Kala CP. Medicinal plants conservation and enterprise development. Med Plants. 2009;1(2):79–95.
L.K Rai LK, Prasad P, Sharma E. Conservation threats to some important medicinal plants of Sikkim Himalaya. Biol Conser. 2000; 93(1):27-33.
Kala CP, Dhyani PP, Sajwan BS. Developing the medicinal plants sector in northern India: challenges and opportunities. J Ethnobiol Ethnomed. 2006;2(1):32.
Caniago I, Siebert S. Medicinal plants ecology, knowledge and conservation in Kalimantan, Indonesia. Econ Bot. 1998; 52:229-250.
Kuniyal CP, Bisht VK, Negi JS, Bhatt VP, Bisht DS, Butola JS, Sundriyal RC, Singh SK. Progress and prospect in the integrated development of medicinal and aromatic plants (MAPs) sector in Uttarakhand. Western Himalaya. Environ Develop Sustaina. 2015;17(5):1141–62.
Rossato SC, Leitao-Filho H, Gegossi A. Ethnobotany of caicaras of the Atlantic forest coast (Brazil). Econ Bot. 1999;53:387–95.
Hanazaki N, Tamashiro JY, Leitao-Filho H, Gegossi A. Diversity of plant uses in two caicaras communities from the Atlantic forest coast. Brazil. Biodivers Conserv. 2000;9:597–615.
Gazzaneo LR, Paiva de Lucena RF, Paulino de Albuquerque U. Knowledge and use of medicinal plants by local specialists in a region of Atlantic Forest in the state of Pernambuco (Northeastern Brazil). J Ethnobiol Ethnomed. 2005; 1(1):9.
Saha D, Sundriyal M, Sundriyal RC. Diversity of food composition and nutritive analysis of edible wild plants in multi-ethnic tribal land, Northeast India: an important facet for food supply. Indian Journal of Traditional Knowledge. 2014;13(4):698–705.
Kala CP. Status and conservation of rare and endangered medicinal plants in the Indian trans-Himalaya. Biol Conserv. 2000;93:371–9.
Bisht VK, Kandari LS, Negi JS, Bhandari AK, Sundriyal RC. Traditional use of medicinal plants in district Chamoli, Uttarakhand. India. Jour Med Pl Res. 2013;7(15):918–29.
Kala CP. Current status of medicinal plants used by traditional Vaidyas in Uttaranchal State of India. Ethnobotany Research Applications. 2005;3:267–78.
Osmaston AE. A forest flora for Kumaun. Dehradun, India: International Book Distributors; 1926.
Naithani BD. Flora of Chamoli. Botanical Survey of India, Vol. 1 and 2. Dehradun, India. 1985.
Kirtikar KR, Basu BD. Indian medicinal plants. Bishan Singh Mahendra Pal Singh, Dehradun. 1994;1994.
Gaur RD. Flora of the District Garhwal: North West Himalaya (with ethnobotanical notes). Srinagar, Garhwal: Transmedia; 1999.
Phillips O, Gentry AH, Reynel C, Wilkin P, Galvez DBC. Quantitative ethno-medicine and Amazonian conservation. Biodivers Conserv Biol. 1994;8:225–48.
Tardio J, Pardo-de-Santayana M. Cultural importance indices: a comparative analysis based on the useful wild plants of southern Cantabria (northern Spain). Econ Bot. 2008;62(1):24–39.
Pardo-de-Santayana M, Tardio J, Blanco E, Carvalho AM, Lastra JJ, San Miguel E, Morales R. Traditional knowledge of wild edible plants used in the northwest of the Iberian Peninsula (Spain and Portugal): a comparative study. J Ethnobiol Ethnomed. 2007;3:27.
Trotter RT, Logan MH. Informant consensus: a new approach for identifying potentially effective medicinal plants. In: Etkin NL, editor. Plants in indigenous medicine and diet: biobehavioural approaches. Bedfort hills, New York: Redgrave Publishers. 1986; 91-112.
Gurdal B, Kultur S. An ethnobotanical study of medicinal plants in Marmaris (Mugla, Turkey). J Ethnopharmacol. 2013;146(1):113–26.
Ahmad M, Sultana S, Fazl-i-Hadi S, Ben Hadda T, Rashid S, Zafar M, Khan MA, Khan MPZ, Yaseen G. An ethnobotanical study of medicinal plants in high mountainous region of Chail valley (district swat-Pakistan). J Ethnobiol Ethnomed. 2014;10(1):36.
Tugume P, Kakudidi EK, Buyinza M, Namaalwa J, Kamatenesi M, Mucunguzi P, Kalema J. Ethnobotanical survey of medicinal plant species used by communities around Mabira Central Forest Reserve. Uganda. J EthnobiolEthnomed. 2016;12(1):5.
Umair M, Altaf M, Abbasi AM. An ethnobotanical survey of indigenous medicinal plants in Hafizabad district. Punjab-Pakistan. PloS one. 2017;12(6):e0177912.
Farooq A, Amjad MS, Ahmad K, Altaf M, Umair M, Abbasi AM. Ethnomedicinal knowledge of the rural communities of Dhirkot, Azad Jammu and Kashmir. Pakistan. J Ethnobiol Ethnomed. 2019;15:45.
El Amri J, El Badaoui K, Zair T, Bouharb H, Chakir S, Alaoui T. Ethnobotanical study of medicinal plants in the region El Hajeb (Central Morocco). J Res Biol. 2015;4(8):1568–80.
Boudjelal A, Henchiri C, Sari M, Sarri D, Hendel N, Benkhaled A, Ruberto G. Herbalists and wild medicinal plants in M’Sila (North Algeria): an ethnopharmacology survey. J Ethnopharmacol. 2013;148(2):395–402.
Singh H. Importance of local names of some useful plants in ethnobotanical study. Indian J Tradit Knowledge. 2008;7(2):365–70.
Shandesh B, Chaudhary RP, Quave CL, Taylor RSL. The use of medicinal plants in the transhimalayan arid zone of Mustang district. Nepal. J Ethnobiol Ethnomed. 2010;6:14.
Kumar M, Mehraj A, Sheikh MA, Bussmann RW. Ethnomedicinal and ecological status of plants in Garhwal Himalaya. India. J Ethnobiol Ethnomed. 2011;7:32.
Malik ZA, Bhat JA, Ballabha A, Bussmann RW. Ethnomedicinal plants traditionally used in health care practices by inhabitants of Western Himalaya. J Ethnopharmacolog. 2015;172:133–44.
Bhat JA, Kumar M, Bussmann RW. Ecological status and traditional knowledge of medicinal plants in Kedarnath Wildlife Sanctuary of Garhwal Himalaya. India. J. Ethnobiol Ethnomed. 2013;9:1.
Kunwar RM, Nepal BK, Kshetri HB, Rai SK, Bussmann RW. Ethnomedicine in Himalaya: a case study from Dolpa, Humla. Jumla and Mustang districts of Nepal. J. Ethnobiol Ethnomed. 2006;2:27.
Kunwar RM, Shrestha KP, Bussmann RW. Traditional herbal medicine in Far-west Nepal: a pharmacological appraisal. J. Ethnobiol Ethnomed. 2010;6:35.
Kunwar RM, Mahat L, Acharya RP, Bussmann RW. Medicinal plants, traditional medicine, markets and management in far-west Nepal. J. Ethnobiol. Ethnomed. 2013;9:24.
Moore PD. Trials in bad taste. Nature. 1994;370:410–1.
Keter LK, Mutiso PC. Ethnobotanical studies of medicinal plants used by traditional health practitioners in the management of diabetes in lower eastern province. Kenya. J. Ethnopharmacol. 2012;139:74–80.
Quave CL, Pieroni AA. Reservoir of ethnobotanical knowledge informs resilient foodsecurity and health strategies in the Balkans. Nature Plants. 2015;1(2):14021.
Mahmood A, Mahmood A, Malik RN, Shinwari ZK. Indigenous knowledge of medicinal plants from Gujranwala district. Pakistan. J Ethnopharmacol. 2013;148(2):714–23.
Bano A, Ahmad M, Hadda TB, Saboor A, Sultana S, Zafar M, Khan MPZ, Arshad M, Ashraf MA. Quantitative ethnomedicinal study of plants used in the skardu valley at high altitude of Karakoram-Himalayan range. Pakistan. J Ethnobiol Ethnomed. 2014;10(1):43.
Bisht VK, Rana CS, Negi JS, Bhandari AK, Purohit V, Kuniyal CP, Sundriyal RC. Lamiaceous ethno-medico-botanicals in Uttarakhand Himalaya. India. Jour Med Pl Res. 2012;6(26):4281–91.
Sundriyal RC. Medicinal plant cultivation and conservation in the Himalaya: an agenda for action. Indian Forester. 2005;131(3):410–24.
Singh P, Attri BL. Survey on traditional uses of medicinal plants of Bageshwar valley (Kumaun Himalaya) of Uttarakhand. India. Intern J Conserv Sci. 2014;5(2):223–34.
Tewari S, Paliwal AK, Joshi B. Medicinal use of some common plants among people of Garur Block of District Bageshwar, Uttarakhand. India. Octa J Biosci. 2014;2(1):32–5.
Bhatt D, Arya D, Chopra N, Upreti BM, Joshi GC, Tewari LM. Diversity of ethnomedicinal plant: a case study of Bageshwar district Uttarakhand. Journal of Medicinal Plants Studies. 2017;5(2):11–24.
Tuttolomondo T, Licata M, Leto C, Bonsangue G, Gargano ML, Venturella G, La Bella S. Popular uses of wild plant species for medicinal purposes in the Nebrodi Regional Park (north-eastern Sicily, Italy). J Ethnopharmacol. 2014;157:21–37.
Jain A, Sundriyal M, Roshnibala S, Kotoky R, Kanjilal PB, Singh HB, Sundriyal RC. Dietary use and conservation concern of edible wetland plants at Indo-Burma hotspot: a case study from northeast India. Jour Ethnobiol Ethnomed. 2011;7:7–29.
Pandey K, Pandey S. Indigenous medicines of Raji tribes of Uttarakhand. Indian J Tradit Knowledge. 2010;9(1):131–3.
Joshi M, Kumar M, Bussmann RW. Ethnomedicinal uses of plant resources of the Haigad watershed in Kumaun Himalaya. J Medicinal and Aromatic Plant Science and Biotechnology. 2010;4(1):43–6.
Samal PK, Dhyani PP, Dollo M. Indigenous medicinal practices of Bhotia tribal community in Indian Central Himalaya. Indian J Tradit Knowledge. 2010;9(1):140–4.
Saha D, Sundriyal RC. Utilization of non-timber forest products in humid tropics: consumption pattern, contribution to rural income and forest revenue. Forest Policy and Economics. 2012;14:28–40.
Samal PK, Shah A, Tiwari SC, Agrwal DK. Indigenous healthcare practices and their linkages with bioresources conservation and socio-economic development in Central Himalayan region of India. Indian J Tradit Knowledge. 2004;3(1):12–26.
Singh A, Nautiyal MC, Kunwar RM, Bussmann RW. Ethnomedicinal plants used by local inhabitants of Jakholi block, Rudraprayag district, Western Himalaya. India. J Ethnobiol Ethnomed. 2017;13:49.
Uprety Y, Poude RC, Gurung J, Chettri N, Chaudhary RP. Traditional use and management of NTFPs in Kangchenjunga Landscape: implications for conservation and livelihoods. Jour Ethnobiol Ethnomed. 2016;12:19.
Jalal JS, Garkoti SC. Medicinal plants used in the cure of stomach disorders in Kumaon Himalaya, Uttarakhand. India. Academia J Medicinal Plants. 2013;1(7):116–21.
Garbyal SS, Aggarwal KK, Babu CR. Traditionally used medicinal plants in Dharchula Himalayas of Pithoragarh district. Uttaranchal. Indian J Tradit Knowledge. 2005;4(2):199–207.
Mehta PS, Negi KS, Ojha SN, Rayal A, Verma SK. Herbal based traditional practices used by the Bhotias and Gangwals of the central Himalayan region, Uttarakhand. India. J. Nanotechnol. 2013;2(1):83–96.
Maikhuri RK, Nautiyal S, Rao KS, Saxena KG. Medicinal plant cultivation and biosphere reserve management: a case study from the Nanda Devi Biosphere Reserve. Himalaya. Curr Sci. 1998;74(2):157–63.
Acknowledgements
We owe our gratitude to the people of Garur-Ganga valley and Saryu valley of District Bageshwar, Uttarakhand, who shared the valuable information and knowledge. The authors thankfully acknowledge the facilities received from GBPNIHE, Kosi-Katarmal, Almora, India, for undertaking this work. We are thankful to DST, Govt. of India for the financial assistance provided under a NMSHE, Task Force 5 sponsored project entitled “Network program on the convergence of traditional knowledge system for sustainable development in the Indian Himalayan Region.” We sincerely thank Dr Deepshikha Arya, Research Officer, CCRAS-RARI, Ranikhet, for her support to help in identifying the plant species, as well as Prof. S.C. Garkoti, JNU for his constant support and cooperation.
Funding
The study has been funded by Department of Science and Technology, Govt. of India under National Action Plan for Climate Change (NAPCC) through National Mission on Sustaining Himalayan Ecosystems (Task Force 5-Network programme on the convergence of traditional knowledge system for sustainable development in the Indian Himalayan Region).
Author information
Authors and Affiliations
Contributions
SNO, DT, and AA planned and performed the study and field survey, wrote the draft manuscript, and analyzed the data, and RCS revised the manuscript and data analysis. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
During field work, prior consent of the informants was taken conducting these studies. This was done to adhere to the ethical standards of community participation in scientific research.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ojha, S.N., Tiwari, D., Anand, A. et al. Ethnomedicinal knowledge of a marginal hill community of Central Himalaya: diversity, usage pattern, and conservation concerns. J Ethnobiology Ethnomedicine 16, 29 (2020). https://doi.org/10.1186/s13002-020-00381-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13002-020-00381-5