
Abstract
Mesenchymal gastrointestinal cancers are represented by the gastrointestinal stromal tumors (GISTs) which occur throughout the whole gastrointestinal tract, and affect human health and economy globally. Curative surgical resections and tyrosine kinase inhibitors (TKIs) are the main managements for localized GISTs and recurrent/metastatic GISTs, respectively. Despite multi-lines of TKIs treatments prolonged the survival time of recurrent/metastatic GISTs by delaying the relapse and metastasis of the tumor, drug resistance developed quickly and inevitably, and became the huge obstacle for stopping disease progression. Immunotherapy, which is typically represented by immune checkpoint inhibitors (ICIs), has achieved great success in several solid tumors by reactivating the host immune system, and been proposed as an alternative choice for GIST treatment. Substantial efforts have been devoted to the research of immunology and immunotherapy for GIST, and great achievements have been made. Generally, the intratumoral immune cell level and the immune-related gene expressions are influenced by metastasis status, anatomical locations, driver gene mutations of the tumor, and modulated by imatinib therapy. Systemic inflammatory biomarkers are regarded as prognostic indicators of GIST and closely associated with its clinicopathological features. The efficacy of immunotherapy strategies for GIST has been widely explored in pre-clinical cell and mouse models and clinical experiments in human, and some patients did benefit from ICIs. This review comprehensively summarizes the up-to-date advancements of immunology, immunotherapy and research models for GIST, and provides new insights and perspectives for future studies.
Similar content being viewed by others


Introduction
Mesenchymal gastrointestinal cancers are represented by the gastrointestinal stromal tumors (GISTs) which occur throughout the whole gastrointestinal tract, and affect human health and economy globally [1]. The annual incidence of GIST worldwide is about 10–15 per million [2], which is much higher in East Asia than that as compared to North America [2, 3]. About 20–30% of GIST patients exhibit malignant behaviors [4], and the five-year survival rate of malignant GIST patients is around 35–65% [4], which seriously threatens human health.
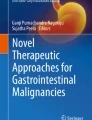
Although primary GISTs can occur anywhere throughout the gastrointestinal tract (Fig. 1A), most of them originate from the stomach (60%) and small intestine (30%), and they can also be found in duodenum (4–5%), rectum (2–4%), colon (1–2%) and oesophagus (< 1%) [5,6,7]. Extragastrointestinal stromal tumor (eGIST) is extremely rare. Metastasis is common in advanced GIST which usually metastasized to liver (50–65%) and peritoneum (20–43%), and less frequently to lymph node (< 6%), bone (< 6%) and lung (< 2%), with other sites relatively rare [8,9,10].

The anatomic and genomic distribution of GIST. A The anatomic locations of primary and metastatic GISTs. Primary GISTs usually originate from stomach and small intestine, and metastasize to liver or peritoneum. B The genomic profiles of GISTs. KIT and PDGFRA signaling are activated by their natural ligands SCF and PDGF respectively in physiological conditions, but are constitutively activated by oncogenic mutations and in a ligand independent manner in GISTs. According to the driver mutations, GISTs can be broadly classified as KIT-mutant GISTs, PDGFRA-mutant GISTs and KIT/PDGFRA-WT GISTs, and the last one could be further divided into SDH-deficient and SDH-competent GISTs based on the expression of succinate dehydrogenase. GIST: gastrointestinal stromal tumor; PDGFRA: platelet-derived growth factor receptor alpha; WT: wild type; EC: ligand-binding extracellular domain; TM: transmembrane domain; JM: intracellular juxtamembrane domain; TK: tyrosine kinase domain; SDH: succinate dehydrogenase; SCF: stem cell factor; PDGF: platelet-derived growth factor
GISTs are widely recognized to originate from the interstitial cells of Cajal (ICCs), the pacemaker cells located within the gastrointestinal wall, and are mainly caused by driver gene mutations. Mutations of KIT and platelet-derived growth factor receptor alpha (PDGFRA), which cause the constitutive activation of the KIT and PDGFRA signaling pathway, respectively, in a ligand-independent manner, are the major molecular mechanisms of the occurrence and progression of GIST [11, 12]. Both KIT and PDGFRA are homologous type III receptor tyrosine kinases consisting of five immunoglobulin (Ig)-like domains (Fig. 1B), namely ligand-binding extracellular domain (EC), transmembrane domain (TM), intracellular juxtamembrane domain (JM) and two tyrosine kinase domain (TK) [13]. According to the driver genes’ mutations, GISTs can be grossly divided into KIT-mutant GISTs, PDGFRA-mutant GISTs and KIT/PDGFRA-wild type (WT) GISTs (Fig. 1B).
About 70–80% of GISTs have KIT gene mutations [14,15,16] with the most common mutation sites on exon 11 (65–80%) and exon 9 (6–10%), followed by exon 13 (1–2%), exon 17 (< 1%) and exon 8 (< 1%) [14,15,16]. Around 10–15% of GISTs have PDGFRA gene mutations [14,15,16] with the common mutation sites on exon 18 (5–14%), exon 12 (< 2%) and exon 14 (< 1%) [14,15,16]. The other GISTs without KIT or PDGFRA mutations (10–15%) are defined as KIT/PDGFRA-WT GISTs, which include succinate dehydrogenase-deficient GIST (SDH-deficient GIST) (< 10%) that caused by SDHA/B/C/D mutations or SDHC promotor hypermethylation modifications, and succinate dehydrogenase-competent GIST (SDH-competent GIST) (< 5%) that caused by other somatic gene mutations or gene fusions, such as neurofibromatosis type 1 (NF1) (< 2%), B-raf proto-oncogene (BRAF) (< 1%) and rat sarcoma viral oncogene (RAS) (< 1%) gene mutations, and other GISTs with unknown mutations [15, 17, 18].
Before the approval of imatinib in the treatment of GIST, GIST was known to be insensitive to traditional chemotherapies [19,20,21], and the management of primary localized GISTs relied heavily on surgical resections. However, about 40–50% of high-risk GIST patients developed local recurrences or metastatic diseases within 5 years after the surgery [8, 22, 23] and their prognosis was very poor with the median overall survival (mOS) of only 12–19 months [8]. In 2002, imatinib was approved for the treatment of recurrent/metastatic or unresectable GISTs and quickly became the standard first-line therapy which dramatically improved the median progression-free survival (mPFS) and mOS [24, 25]. Unfortunately, not all GIST patients benefited from imatinib therapy, those with KIT/PDGFRA-WT genotype and PDGFRA-D842V mutations responded poorly to the treatment. In addition, due to secondary mutations of KIT, most of the imatinib-sensitive patients developed resistance to imatinib within 2 years [26,27,28]. Recently, the Food and Drug Administration (FDA) of the United States approved sunitinib, regorafenib and ripretinib as the second-, third- and fourth-line drugs for GIST, respectively, which prolong the mPFS of metastatic or recurrent patients with 5.6 [29], 4.8 [30] and 6.3 [31] months, respectively. Avapritinib was also recently approved by the FDA, and the mPFS is 29.5 months in metastatic PDGFRA-D842V GIST patients [32], and 3.7 months in non-D842V GIST patients [33].
Certainly, the discovery of imatinib and the successive tyrosine kinase inhibitors (TKIs) in the past two decades have revolutionized the management of recurrent/metastatic or unresectable GISTs and provided additional survival benefit for patients by delaying metastasis and recurrence. However, due to the primary and secondary resistance, TKIs often have short-lived disease control and very limited efficacy, and thus most GIST patients ultimately became refractory to these treatments. Therefore, novel therapeutic targets and drugs are urgently necessary to circumvent the resistance and further improve treatment efficacy. Fortunately, immune checkpoint inhibitors (ICIs) have achieved great success recently in various malignant tumors, and some patients can even be cured. GIST microenvironment has been demonstrated to be populated by a large amount of tumor-infiltrating immune cells, which play an essential role in tumor surveillance and may be exploited to remove imatinib resistant tumor cell clones, thereby enhancing the antitumor effect of imatinib. Unfortunately, in early phase trials, heavily pretreated GIST patients only showed moderate responses to therapeutic antibodies against programmed cell death protein 1 (PD1) and cytotoxic T-lymphocyte antigen 4 (CTLA-4) [34, 35], and the mechanisms of these treatments are obscure. This article will systematically review the research progress of immuno-oncology, immunotherapy and research models of GIST, and discuss the difficulties encountered in immunotherapy, so as to provide new insights into the development of more effective immunotherapies for GIST.
Systemic inflammation in GIST
Inflammation plays a vital role in tumorigenesis, tumor progression, invasion, metastasis and angiogenesis [36]. Therefore, tumor‐promoting inflammation is recognized as one of the hallmarks of cancers [37]. The malignant phenotypes of tumor cells stimulated the infiltration of inflammatory cells [38], while the destruction of tumor cells via physical or chemical strategies usually caused the generalized and nonspecific systemic inflammatory responses which were characterized by thrombocytosis, neutrophilia, lymphocytopenia [39]. Increasing evidence suggested that some hematological biomarkers based on the number of blood leukocytes and platelets, for example, NLR, PLR, PNI, MLR, NWR, MWR, LWR, PWR, NAR, LMR, HALP, SII and so on (the meanings of these abbreviations were presented in Table 1), reflecting the systemic inflammatory response of the host. Given that these systemic inflammatory biomarkers are accessible, reproducible and cost-effective, and are associated with patients’ prognosis of various kinds of cancers, they are often used to predict the survival outcome and treatment responses, as well as to help clinicians to determine appropriate therapeutic schemes for patients [40, 41]. In GIST, several inflammatory hematological biomarkers, which are detailed in Table 1, has been proven to be closely related to the clinical outcomes and clinicopathological features.
To date, the underlying mechanisms of systemic inflammation in promoting tumor progression and influencing the prognosis of cancer patients remain to be elucidated [60, 72]. Several potential mechanisms have been proposed and may help to explain some clinical observations. First, thrombocytosis is associated with poor prognosis of cancer patients. As a reservoir of secreted proteins, platelets in the blood are able to secrete a variety of growth factors, cytokines and chemokines, which in turn, promote tumor growth, survival, metastasis and angiogenesis [76]. Moreover, platelets have also been demonstrated to infiltrate into tumor microenvironment and directly interact with tumor cells [77], to help circulating tumor cells to adhere to endothelial cells, and thereby to establish a niche prior to metastasis [78]. Second, peripheral neutrophil is an indicator for acute and chronic inflammation [79]. On the one hand, neutrophil promotes angiogenesis and progression of tumors [79] through secreting tumor growth promoting factors, such as vascular endothelial growth factor (VEGF) [80, 81], matrix metalloproteinase [82, 83], hepatocyte growth factor (HGF) [84], interleukin 6 (IL-6) [85] and IL-8 [86]. On the other hand, high neutrophil counts suppress immune system of the host via restraining the cytolytic activity of immune cells, including lymphocytes, activated T cells and natural killer cells [87]. In addition, neutrophil has also been found to promote tumorigenesis by inhibiting the functions of T cells through reactive oxygen species (ROS) and arginase-1 [88, 89]. Last but not least, lymphocytes are crucial for the cell-mediated antitumor immune response. Lymphocytes inhibit the proliferation and metastasis of tumor cells by inducing cytotoxic cell death and cytokine secretion [90]. Peripheral lymphocytes are closely related to tumor-infiltrating lymphocytes (TILs); the lower the circulating lymphocytes count, the lower the infiltrating lymphocytes level, which eventually leads to the decreased antitumor activity and poor prognosis [91]. Therefore, the blood lymphocytes counts reflect the degree of responsiveness of the host to the clinical managements [92, 93].
Immune cell landscape of GIST
Several studies have explored the immune landscape of GIST and found that almost all GIST samples are infiltrated with variable amounts of immune cells [94,95,96]. Macrophages and T lymphocytes are the most common immune cells in GIST [94, 95, 97,98,99,100,101,102,103,104] and are representatively illustrated in Fig. 2A; although some studies showed that the former is more abundant than the latter [97, 101, 104], others reported the opposite [94, 96, 98, 102, 105,106,107,108]. Such discrepancies may be explained by the different anatomical tumor sites [94, 109], metastatic status [97, 98, 101, 109,110,111] and driver gene mutations [99, 112]. Moreover, there are also some less abundant immune cells infiltrated in GIST, including natural killer (NK) cells, B lymphocytes, dendritic cells (DCs), natural killer T (NKT) cells, gamma delta (γδ) T cells, neutrophils, eosinophils and mast cells, etc. [42, 94, 96, 100, 101, 103, 106, 113,114,115]. The intratumoral distribution patterns of immune cells in GIST are variable; they are mainly diffusely distributed around blood vessels with a small amount distributed in aggregates [94, 96, 100, 101, 105]. Immune cells infiltrated in GIST have been shown to be associated with patients’ clinicopathological features, and have predictive values. Since DC cells [97], myeloid-derived suppressor cells (MDSCs) [97] and neutrophils [42] are rarely present and reported in GIST, this article will focus on the infiltration of macrophages, T lymphocytes, NK cells and B cells and their relationship of the clinicopathological characteristics of GIST patients.

The immune microenvironment of GIST. A GIST is mainly infiltrated with T cells and M2 macrophages, and less frequently by NK, B and DC cells. Approximately half of the GISTs harbor intratumoral tertiary lymphoid structures which were enriched with T cells and B cells. B Gross comparisons of the immune cell infiltration between different groups. Immune cells seem to be enriched in metastatic GIST (especially liver metastasis), non-gastric GIST and PDGFRA-mutant GIST and the margin area of the GIST. GIST: Gastrointestinal stromal tumor; NK: natural killer cell; MΦ: macrophages; M1: M1 that macrophages are classically activated; M2: M2 macrophages that are alternatively activated; DC: dendritic cell; Th1: T helper type 1 cell; Th2: T helper type 2 cell; γδ T cell: gamma delta T cell with T cell receptors (TCRs) composed of γ- and δ-chains
Tumor-associated macrophages
Tumor-associated macrophages (TAMs) are one of the most common inflammatory cells in the microenvironment of GIST [97], and can be classified as classically activated (M1) and alternatively activated (M2) macrophages. M1 macrophages exert antitumor activity through phagocytizing tumor cells, presenting tumor cell antigens to T cells and producing proinflammatory cytokines; on the contrary, M2 macrophages, by suppressing inflammatory responses, recruiting Treg cells, and stimulating angiogenesis, promote the tumor progression. In untreated primary GIST, the polarization of TAMs in the microenvironment is controversial, with either M2 [102] or M1 macrophage [116] considered to be the major cell subtypes. Whereas in metastatic and imatinib-treated GISTs, M2 macrophage is the most enriched subtype [97, 113, 116, 117] with high expression level of major histocompatibility complex class II (MHC-II) molecules [97]. Previous studies have demonstrated that the amount of CD68+ macrophages (both M1 and M2) was positively correlated with RFS [118, 119] and risk grade of GIST [94, 95], but the ratio of CD163+ macrophages (M2 only) to CD68+ macrophages showed a negative correlation with RFS [118, 119]. However, some studies reported that there were no significant correlations between macrophages counts and RFS [106], or the prognosis [94] of GIST. The M2 macrophage was positively associated with the expression of ETS variant 1 (ETV1) which was highly expressed on GIST cells, and ETV1 inhibition was found to depress the malignant progression of GIST via suppressing the M2 polarization of macrophages [120]. Li et al. identified a group of macrophage-like circulating tumor cells (ML-CTC) [121, 122]featured by the expression of both CD68 (macrophage cell marker) and KIT (GIST cell marker) in metastatic GIST, and proposed that these cells may be used to predict the relapse and metastasis of GIST in future studies [122].
Tumor-infiltrating T lymphocytes
T lymphocytes in GISTs are mainly CD3+ T cells, including CD8+ T, CD4+ T and a small amount of Foxp3+ T-regulatory (Treg) cells [97, 99, 123]. CD3+ T cells in GIST have been demonstrated to be highly activated and enriched in MHC-I positive regions of tumors [99]. CD3+ T cells populated in GIST showed a negative correlation with the tumor size [99], positive correlations with RFS [99, 106, 109], improved PFS [99] and OS [109], and thus CD3+ T cell infiltration possess certain prognostic values. While, some other studies demonstrated controversial results, Cameron et al. reported that the infiltration of CD3+ T cells was positively correlated with cell proliferation index [101] and high risk GISTs [101], and was not associated with metastasis [124] or survival [125] in GIST.
CD8+ T lymphocytes are the key lymphocytes to kill cancer cells and to achieve a response to anti-PD1 antibody treatment [126]. GISTs have been found to harbor a high infiltration level of CD8+ T cells [127], and nearly all GIST samples have CD8+ T cells [108], but the cell number in GIST is much lower than those in non-small cell lung cancer (NSCLC) [34]. CD8+ T lymphocytes in GIST have been shown to be positively correlated with RFS [106, 109, 118, 119, 128] and OS [109, 128]. In PD-L1+IDO+ GIST patients, CD3+CD8+ T lymphocytes were negatively correlated with the tumor size [124]. Dickkopf 4 (DKK4) is highly expressed in high-risk GISTs and negatively correlated with the number of intratumoral CD8+ T cells [129]; GIST cells directly inhibit the migration and infiltration of CD8+ T cells by secreting DKK4 [129]. As for CD4+ T cells, they are also infiltrated in nearly all GIST samples, but the number is less abundant than those of CD8+ T cells [108]. So far, the prognostic value of CD4+ T cell infiltration in GIST has not been well documented. In KitV558Δ/+ mouse GISTs, γδ T cells were found to be present in GIST, accounting for about 2% of immune cells in GIST [115], and promote the antitumor immunity through IL17A secretion [115].
Treg cells, which inhibit antitumor immune response, are relatively rare in GIST [97], although seem to be higher than in other sarcomas [123]. Treg cells infiltrated in GIST showed a negative correlation with PFS [99] but a positive correlation with high risk GISTs [98, 99, 130], and no association between Treg cell infiltration and GIST metastasis was found [124]. In addition, the infiltration of Treg cells in GIST is positively correlated with that of M2 macrophages, suggesting that the immunosuppressive effect of the latter may be attributed to Treg cells recruitment [130]. The CD8+ T/Foxp3+ Treg cell ratio in GIST is much lower than in cervical cancer [131], which suggests a strong immune suppression in GIST microenvironment [97].
Tumor-infiltrating NK cells
NK cells belong to the innate immune system and are the first-line defense against infection and tumors. They can target cells with low MHC-I expression, serving as an important supplement to the cell-mediated antitumor immunity. Different from other solid tumors [132, 133], NK cells are abundant in GISTs [99, 102, 108, 134] and are more likely to enrich in gastric GISTs [99]; around 42.1% of GISTs have CD56+ NK cells [108] and around 25% of CD45+ leukocytes are CD3−CD56+ NK cells [134]. NK cells infiltrated in GISTs are positively correlated with PFS [99, 128, 133], RFS [99, 106, 109], OS and prognosis [101, 109, 128], but negatively correlated with high risk GISTs [99], proliferation index [101, 134] and metastases [134]. In addition, the level of interferon γ (IFNγ), secreted by NK cells, was also positively associated with better survival of GIST patients [133, 135]. NK cells play an important role in the metastasis of GIST [136]. With the use of NK or T cell-depleting monoclonal antibodies on mouse model, it has been shown that NK cells exert antitumor activity mainly in the process of metastasis, but not in the primary tumors [137].
NK cells express several receptors, such as natural killer cell p30-related protein (NKp30) and NKp46, which endow NK cells with distinct functions. NKp30 has three major isoforms, namely NKp30A, NKp30B and NKp30C. NKp30A and NKp30B receptors mediate cytotoxicity and generation of IFNγ/tumor necrosis factor alpha (TNFα), respectively, whereas NKp30C induces the production of immunosuppressive cytokine IL-10 [132,133,134]. Compared with those from healthy volunteers, peripheral blood mononuclear cells (PBMCs) from GIST patients express lower levels of natural cytotoxicity triggering receptor 1 (NCR1, encoding NKp46), NKp30A and NKp30B, while the NKp30C level is comparable between these two groups [138]. In GIST, NK cells predominantly express the immunosuppressive NKp30C isoform [99, 134] whose expression level shows negative correlations with OS and prognosis [133, 134]. B7-H6, a ligand of NKp30, is widely expressed in GIST [99, 133, 134, 139]; its soluble form, sB7-H6, is negatively associated with DFS and prognosis in metastatic GIST [133]. Baculoviral IAP repeat-containing protein 3 (BIRC3) and Tumor necrosis factor receptor (TNFR) associated factor 1 (TRAF1) are highly expressed in NK cells, and their expressions are correlated with NKp30C level [140], suggesting that BIRC3 and TRAF1 are involved in the regulation of NK cell activity in GIST. In addition, the transcription of BIRC3 induced by TNFα reduces the expression of NKp46, the activation receptor [140], thereby weakening the antitumor effect of NK cells and promoting the metastasis and dissemination of GIST, resulting in poor prognosis [140]. The presence of membrane-bound transforming growth factor β (TGFβ) in Treg cells downregulates the expression of natural killer group 2 member D (NKG2D) receptor in NK cells, which directly inhibits the cytotoxicity of the latter [141]. Depletion of Treg cells in mouse exacerbates the proliferation and cytotoxicity of NK cells [141].
Tumor-infiltrating B lymphocytes and tertiary lymphoid structures
The tumor-infiltrating B cells in tertiary lymph nodes are crucial in antitumor immune responses; they contribute to humoral antitumor responses through antibody-dependent cellular cytotoxicity (ADCC) and complement-dependent cytotoxicity (CDC). B lymphocytes are present in GIST [94, 105] and may be more prevalent in isolated intratumoural lymphoid aggregates [96]. B lymphocytes are negatively correlated with the tumor size [105] but positively correlated with RFS [106, 109] and OS [109] in GIST. However, Cameron et al. reported the opposite findings showing that the B lymphocytes are less infiltrated in GIST and mainly located in metastatic GIST, which showed positive correlations with cell proliferation index, recurrence risk and metastasis [101].
Tertiary lymphoid structures (TLSs), which usually comprise a T cell zone and a B cell follicular zone, are ectopic lymphoid aggregates that are widely present in various cancer types [142]. As diagrammed in Fig. 2A, Tumor-infiltrating TLSs were found in 44.9%-52.2% GISTs [143], and their outer layers were mainly composed of CD4+ T and CD8+ T cells while the inner layers were mostly composed of B cells [143]. TLSs were found to be associated with low risk GISTs, longer survival time, RFS and lower imatinib resistance [143], and thus may be a novel therapeutic strategy for imatinib-resistant GIST patients [143]. No difference was found in the morphology of TLSs between different types of GISTs with various driver gene mutations [143], but PDGFRA-mutant GISTs were more likely to have TLSs when compared to KIT-mutant GISTs and WT GISTs [143]. Further analysis showed that TLS+ PDGFRA-mutant GIST patients had the best survival outcome while TLS− KIT-mutant patients had the worst OS [143].
Immune cell infiltration and metastasis
As shown in Fig. 2B, The infiltration level of immune cells is closely related to the metastatic status of GIST [111]. In primary GISTs, the amount of CD68+ macrophages is higher than that of CD3+ T-cells, whereas the opposite is the case in metastatic GISTs [101]. Metastatic GISTs harbor more M2 macrophages [111], which are approximately twice as many as those of primary GISTs [97], suggesting that M2 macrophages promote the tumor progression. Moreover, the numbers of infiltrated CD3+ T [101], B [101, 110] and NK cells [101, 110] are also much higher in metastatic GISTs than in primary GISTs [101]. At the tumor margin, local non-metastatic GISTs exhibit more CD8+ T and Foxp3+ Treg cells than metastatic GISTs [109]. In addition, the infiltration levels of immune cells are also closely associated with the metastatic sites of GIST. When compared with peritoneal metastases, liver metastases have more CD3+ T, CD56+ NK and CD20+ B cells, but CD68+ macrophages are comparable [101].
Immune cell infiltration and anatomic sites
The infiltration levels of immune cells are related to the anatomic sites of GISTs as different lesions have distinct microenvironment (Fig. 2B). Gastric GISTs possess the most immune cell infiltration while eGISTs have the least infiltration [94]. When compared with non-gastric GISTs, gastric GISTs harbor less CD8+ T [103, 109] and CD3+ T cells [101] but more NKp46+ NK cells [99]. Besides, more CD8+ T, CD3+ T, CD4+ T and NKp46+ NK cells are found at the edge of tumors compared to tumor centers [109].
Immune microenvironment and driver gene mutations
The infiltration of immune cells and the expression of immune-related genes differ between GISTs driven by different mutations, and are grossly illustrated in Fig. 2B. The infiltration levels of immune cells of KIT/PDGFRA-WT GISTs are still controversial. Sun et al. reported that KIT/PDGFRA-WT GISTs had more CD8+ T cells than KIT- and PDGFRA-mutant GISTs [103]; however, Gasparotto et al. reported the opposite which showed that the former had less T cells, including CD3+ T, CD4+ T and CD8+ T cells [104], and expressed lower levels of MHC-I and immune checkpoint molecules [104].
When compared with KIT-mutant GISTs, PDGFRA-mutant GISTs harbor a higher infiltration level of immune cells [104, 112], especially that of CD8+ T cells, and display a higher cytolytic activity [112]. PDGFRA-mutant GISTs highly express C-X-C motif chemokine ligand 14 (CXCL14) [112] and enhance immune surveillance by recruiting DC, NK and CD8+ T cells and upregulating MHC-I molecules levels [144]. Moreover, PDGFRA-mutant GISTs increase the expression of C–C motif chemokine ligand 2 (CCL2) through NF-kB (nuclear factor kappa-light-chain-enhancer of activated B cells) signaling [104], which helps to recruit macrophages to GIST microenvironment [145]. Given that PDGFRA-mutant GISTs have the strongest immune-related gene expression signatures, exhibit more neoepitopes that could be presented by MHC-I molecules, express more immune checkpoint molecules, and possess higher immunogenicity, they may respond better to immunotherapy [112], and these features may also at least partially explain why PDGFRA-mutant GISTs have a more favorable disease outcome [112, 146,147,148].
PDGFRA-D842V mutation, which hampers the binding of imatinib via changing the conformation of the kinase domain of PDGFRA [149, 150], is the most common genetic mutation leading to the primary resistance to imatinib. Many research studies have shown that PDGFRA-D842V GISTs have more immune cells infiltration and higher cytolytic activity than non-D842V GISTs [98, 112, 149, 151]. Moreover, PDGFRA-D842V GISTs also express higher levels of interferons and chemokines, as well as PD1 and programmed death-ligand 1 (PD-L1), and has more driver-derived neoepitopes that could be presented by MHC-I molecules [98, 112, 149].
Until now, limited research studies have examined the impact of KIT mutational subtypes on GIST microenvironment. In KIT-mutant GISTs, intestinal GISTs have been shown to have more immune cells infiltration than non-intestinal GISTs [104]. In localized GISTs, it was found that the number of NK cells in KIT-WT GISTs is threefold higher than that in KIT-mutant GISTs (with Exon-11 mutation) [99].
Immune checkpoint, MHC and other immune related genes
PD1/PD-L1
PD1 and its ligand PD-L1 are expressed on the surface of immune cells and tumor cells, respectively; the binding of PD-L1 to PD1 causes inhibition or diminution of the immune cell function, which, in turn, leads to immune escape and promotes tumor progression.
In GIST, PD-L1 is mainly present on tumor cells and a few in leukocytes [35], independent of the mutant types of the driver genes [35]. Its expression shows high heterogeneity in GIST [35, 152]; about 16.3%-69.0% of GIST samples present PD-L1 expression [34, 96, 98, 103, 105, 109, 123, 124], and in the same sample, there might be less than 10% of tumor cells express PD-L1 [34]. Overall, the expression level of PD-L1 in GIST is relatively low [34, 35, 104, 123], though it is higher than that in other kinds of sarcoma [123]. PD-L1 expression has been demonstrated to be correlated with clinicopathological features with predicting values [103, 152], but the results are controversial. Some studies showed that PD-L1+ GISTs have more immune cells infiltration [103, 105, 125], and PD-L1 expression in GIST was negatively correlated with tumor size [98, 103], mitotic index [103], high risk GISTs [152] and metastasis [152], and was positively correlated with improved RFS [103], suggesting that high PD-L1 expression is associated with antitumor immune response and better prognosis. However, other studies found that PD-L1 expression was positively correlated with the features of unfavorable outcomes, such as tumor size [124], proliferation index [124], high-risk GIST [125, 153] and therapy resistance [153], but was not associated with RFS [109], metastasis [124] and OS [105, 109, 124]. Besides, the expression level of PD-L1 on immune cells is related to worse DFS [154, 155]. In plasma, high expression of soluble PD-L1 (sPD-L1) is associated with PFS and poor prognosis [156,157,158,159].
PD1 is primarily expressed on GIST-infiltrated T cells [35] with low levels [104, 127]. PD1 has been reported to be present on 48.5% or 88% of GIST samples [98, 103], and such discrepancy may be associated with the samples they chose. The expression of PD1 in intratumoral T cells is higher than that in circulating T cells [35] and its expression shows no correlation with RFS or OS [109]. Same as sPD-L1, the high expression of soluble PD1 (sPD1) in plasma is associated with PFS and poor prognosis [156,157,158].
IDO
Indoleamine 2,3-dioxygenase (IDO), the rate-limiting enzyme of tryptophan metabolism in human, metabolizes tryptophan, an essential amino acid, into kynurenin, which changes the tumor microenvironment from immunogenic to tolerogenic [160]. IDO exerts immunosuppressive effects by directly inhibiting the CD8+ T cell activity and inducing Treg cell differentiation [161,162,163]. In addition, tryptophan metabolites are able to polarize antigen presenting cells (APCs) to exhibit an immunotolerant phenotype featured by secreting TGFβ or IL-10 [164]. In GIST, the constitutively activated KIT signaling upregulates IDO expression through the transcription factor ETS variant 4 (ETV4) [95]. The IDO expression level is high in GIST with 63%-89.8% of GISTs are IDO-positive [34, 124] and almost all of PD-L1+ GISTs are IDO+ GISTs [124]. Moreover, all PDGFRA-mutant GISTs express IDO but show no correlation with clinicopathological features [98]. In addition, CD4+ T cells are more abundantly infiltrated in PDGFRA-mutant GISTs with high IDO level [98], while in PD-L1+IDO+ GIST, higher infiltration level of Treg cells is found [124]. In KitV558Δ/+ GIST mice, IDO inhibitors may enhance the antitumor effect of imatinib [95] or anti-PD1 antibody [35] through activating CD8+ T cells and inducing apoptosis of Treg cells [95, 165], suggesting that the IDO-targeted immunotherapy would be of great value.
Tim-3/Gal-9 and other immune checkpoints
In GIST, T cell immunoglobulin and mucin-domain containing-3 (Tim-3) is mostly present in TILs [108] with low expression level [127]. Galectin-9 (Gal-9), the ligand of Tim-3, is expressed mainly in tumor cells [108]. Nearly all GIST samples with Tim-3+ NK-infiltration showed the Gal-9 expression [108], suggesting that their interactions are likely involved in the suppression of antitumor immunity, and therefore, blocking Tim-3/Gal-9 pathway may become a new strategy for GIST treatment [108]. The expression level of Tim-3 in GIST shows positive correlations with OS, PFS and density of CD8+ T cells [128], but a negative correlation with high risk GISTs [128]. Contrary to Tim-3, Gal-9 expression is positively correlated with high-risk GISTs [128], negatively correlated with the densities of CD8+ T cells and CD56+ NK cells [128], and displays no correlation with OS and PFS [128]. These conflicting findings suggest that Tim-3 and Gal-9 may have different mechanisms in terms of immune escape in GIST, which differ from those in epithelial tumors [128].
Lymphocyte activation gene-3 (LAG3) and V-type immunoglobulin (Ig) domain-containing suppressor of T-cell activation (VISTA) are mainly expressed on the surface of T cells. The expression of LAG3 in GIST is also low [127], but its expression in intratumoral T cells is significantly higher than that in circulating T cells [35]. The expression of VISTA in GIST is associated with improved outcomes [154, 155], which implies that VISTA has multifaceted roles in different cancers, and also highlights the complexity of VISTA as an immune checkpoint protein. In addition, inducible T cell costimulator (ICOS) and its ligand, B7H2 (ICOSL), are also present in GIST, and related to poor prognosis [166]. B7-H6, a novel immune checkpoint molecule, is able to elicit NK cells’ antitumor immune responses upon interacting with its receptor NKp30 on NK cells. Given B7-H6 is highly expressed in GIST [99, 134, 167], it will be a potential immunotherapy target.
CTA, MHC-I and MICA/B
Cancer testis antigens (CTAs) are a large class of tumor-associated antigens, when presented by MHC-I molecules expressed on the surface of APCs, they can be recognized by specific cytotoxic T lymphocytes and trigger the antitumor immunity. CTAs are expressed in various malignant tumors, whereas in normal tissues, CTAs are only present in germ cells of the testis and placenta; therefore, CTAs are considered to be ideal targets for the immunotherapy of various cancers [168]. It has been reported that 26.7%-40% of GIST patients show CTAs expression [168,169,170]. G antigen (GAGE) [171], melanoma-associated antigen (MAGE)-A1 [168, 169], MAGE-A3 [168, 169], MAGE-A4 [168, 169], MAGE-C1 [168, 169], MAGE-C2 (CT10) [171] and New York esophageal squamous cell carcinoma-1 (NY-ESO-1) [168, 169] are present in 12%, 9%-14.3%, 8%-14.3%, 13%-14.3%, 15%-25.8%, 10% and 12%-20.0% of GIST patients, respectively. Another two studies, however, have demonstrated that NY-ESO-1 was almost not expressed in GIST [172, 173]. The CTAs expression is associated with clinicopathological features of GIST with predicting values [168, 169, 171]. CTA+ GISTs have worse responses to imatinib and shorter RFS [168, 169]; while the MAGE-A3 and NY-ESO-1 levels correlate with tumor progression after imatinib treatment [168].
MHC molecules, also called human leukocyte antigens (HLAs), are mostly expressed on the surface of tumor cells and antigen-presenting cells. However, only 30% of GIST samples show a normal expression level of MHC-I molecules [97], and a majority of them have partial defects of HLA expression; 38% of GISTs show no HLA-A expression and 20% show no expressions of HLA-B and HLA-C [97]. These findings suggest that there are interactions between tumor cells and immune cells and those clones with low levels of MHC-I molecules are selected and survive [97]. Defective expression of MHC-I molecules led to decreased recognition of tumor cells by cytotoxic T lymphocytes and weakened the antitumor immune responses [97]. Although the MHC-I expression is lost in GIST, MHC class I chain-related protein A and B (MICA/B) are found in GIST, suggesting that NK cells may play a crucial role in the antitumor immune responses [174, 175].
Other immune-related genes
By releasing a variety of molecules, tumor cells are able to recruit different types of cells into tumor tissues, transform the tumor microenvironment and promote their growth and metastasis in return. The expression of inflammatory cytokines in GIST is very low, and the TNFα expression is basically negligible [100], suggesting an immunosuppressive microenvironment in GIST. As for chemokines, such as CCL2, CCL3 and CXCL1, their expressions in GISTs are relatively high [101] and CCL2 induces the infiltration of macrophages into tumor tissues and promotes tumor growth [101, 145]. CXCL2, which is mainly produced by M2 macrophages in metastatic GISTs, promotes migration, invasion and EMT of GIST cells in vitro and in vivo [117]. GIST cells facilitate p65 phosphorylation and nuclear translocation through lowering the expression of secreted protein acidic and rich in cysteine-like 1 (SPARCL1), and thereby increasing the release of cytokines and the infiltration of M2 macrophages [176]. In addition, GIST microenvironment contains large amounts of TGFβ1, which reduces the activity of immune effector cells [177] and promotes tumor metastasis. CC chemokine receptor type 8 (CCR8) is mainly present in Treg cells and negatively correlated with patients’ survival [178]. The ligand of CCR8, CCL1, enhances tumor immunosuppressive microenvironment via the recruitment of CCR8+ Treg cells [179]. Anti-CCR8 antibody is able to selectively eliminate the clonally expanding Treg cells within the tumor, but has no effect on tumor-infiltrating effector T cells or natural Treg cells [180,181,182,183,184,185], making it a potential treatment for GIST. In GIST cell lines, KIT exon 11 codon 557–558 deletion enhances the expression of C-X-C chemokine receptor 4 (CXCR4) [186]. Tumor cells harboring high expression of CXCR4 maybe attracted by CXCL12 secreted by hepatic cells, which partially explains the high prevalence of liver metastases of advanced GIST [186], and provides a new therapeutic target for GIST management.
Several immune-related gene sets have been constructed to evaluate the immune characteristics of GIST. Pantaleo et al. constructed the expanded IFNγ-induced immune signature (EIIS) [102] and T-cell-inflamed signature (TIS) in GIST [102], both of which are related to clinical benefit of ICIs treatment and considered as predictors of immunotherapy [187, 188]. EIIS is present in all GIST samples while TIS is highly expressed in GISTs, and they both are positively correlated with PD-L1 expression [102], suggesting that GIST may benefit from immunotherapy alone or in combination with TKIs [102]. Based on RNA-seq data, Petitprez et al. recently investigated the tumor microenvironment of 608 soft tissue sarcomas (STS) which includes 60 GISTs [189]. 25% of GIST patients belonged to sarcoma immune classes-E (SIC-E) group and such proportion was higher in GIST than in other sarcomas [189]. SIC-E subtype is characterized by strong expression of genes specific to cytotoxic lymphocytes, immune checkpoint molecules, the presence of TLSs, and may exhibit better response to PD1 blockade and longer survival [189]. In addition, Yi et al. established a prognostic model based on immunoscore [118, 119] and proved that the immunoscore is an independent prognostic factor for GIST [118, 119].
Immunological effects of imatinib in GIST
Imatinib inhibits the proliferation and survival of GIST tumor cells primarily through suppressing KIT signaling pathway. However, some GISTs without hallmark mutations of imatinib sensitivity also show long-term responses to imatinib [136, 175], implying that the off-target effects also mediate, at least in part, the therapeutic efficacy of imatinib. For example, a case report demonstrated that a GIST patient with low KIT expression had response to imatinib treatment [190], and 6 patients without typical target mutations of imatinib were still sensitive to imatinib therapy [175]. Imatinib could kill the tumors established from several imatinib-resistant cell lines in immunocompetent mice in vivo [175], and these effects were found to be mediated mainly by the NK cells infiltrated into the tumor [136, 175]. In addition, CD8+ T cells were also reported to mediate part of the off-target effects of imatinib [95]. Taken together, the success of imatinib in clinic should be partially credited to its impact on the innate and adaptive immunity by modifying the tumor immune microenvironment.
In general, the effects of imatinib on immune microenvironment of GIST are complex (Fig. 3A). On the one hand, imatinib brings meaningful immunologic benefit to GIST patients, such as augmentations of the infiltration and activity of CD8+ T cells, DC cells and NK cells, increases of IFNγ secretion, reductions in Treg cells infiltration [35, 95, 99, 113, 134, 136, 141, 169, 175, 191,192,193,194] and PD-L1 expression [35, 102], and thereby enhancing the antitumor immune responses. On the other hand, imatinib also induces immunosuppressive microenvironment. For instance, imatinib drives intratumoral macrophage M2 polarization [116], induces M1 macrophages to secrete anti-inflammatory cytokine IL-10 [97] and lowers MHC-I expression [99, 195]. Moreover, chronic imatinib therapy decreases the number of intratumoral CD8+ T cells and DC cells [191], and thus weakens the antitumor immune responses.

The immunomodulatory effects of imatinib in GIST. A The general immunological effects of imatinib in GIST. Short-term administration of imatinib enhanced the antitumor immune response via increasing the infiltration and activity of immune cells and the secretion of IFNγ. While, long-term usage of imatinib may weaken the antitumor immune response by enriching the M2 macrophages and decreasing the amounts of CD8+ T and DC cells, as well as the expression of MHC-I molecules. B Dissected immunological effects of imatinib on various types of cells within the GIST, including GIST cells, CD8+ T cells, γδ T cells, Treg cells, NK cells, Macrophages and DC cells. GIST: gastrointestinal stromal tumor; DC: dendritic cell; NK: natural killer cell; IFNγ: interferon gamma; PD-L1: programmed death-ligand 1; MHC-I: major histocompatibility complex class I; IDO: indoleamine 2,3-dioxygenase; Treg: regulatory T cells; MΦ: macrophages; γδ T cell: gamma delta T cell with T cell receptors (TCRs) composed of γ- and δ-chains
The effect of imatinib on T cells
T cells play an important role in mediating the antitumor effect of imatinib. When compared with untreated and imatinib-resistant GIST patients, imatinib-sensitive GIST patients have more CD3+ and CD8+ T cells [95] and less Treg cells infiltration [95, 99]. As presented in Fig. 3A, imatinib treatment significantly reduced the infiltration of Treg cells [99] and imatinib exerted its antitumor effect through enhancing the function of CD8+ T cells [35]. In addition to studies on human GIST, there are at least four research works have examined the effects of imatinib on T cell infiltration and function in the KitV558Δ/+ mouse GIST model. First, Balachandran et al. reported that imatinib altered the immune microenvironment of GIST by inhibiting the expression of IDO [95]. On the one hand, imatinib enhanced the infiltration and proliferation of CD8+ T cells in tumors, and thus augmented their antitumor immune responses which was diminished by CD8+ lymphodepletion [95], suggesting that the antitumor role of imatinib depends on CD8+ T lymphocytes. On the other hand, imatinib induced the apoptosis of Treg cells, leading to a lower infiltration level of Treg cells and higher CD8+ T/Treg cell ratio [95]. Second, Medina et al. showed that the antitumor effect of imatinib in GIST was partially mediated by DCs and effector CD8+ T cells [191]. Acute treatment of imatinib (1 week) increased the amount of DCs and effector CD8+ T cells in tumors as well as promoted the maturation of DCs. While chronic imatinib therapy decreased the infiltration of DCs and effector CD8+ T cells in tumors [191]. Third, Tieniber et al. demonstrated that imatinib reduced the infiltration of effector CD8+ T cells and increased that of naive T cells (Tn) in GIST, which were accompanied by alterations of chemokines secretion, CD8+ T cells recruitment and PI3K signaling within CD8+ T cells [196]. Interestingly, their findings about the effects of imatinib on immune cells infiltration from mouse GIST models were further validated in human GIST samples [196, 197]. Fourth, Etherington et al. reported that imatinib increased the γδ T cells count in GIST, and upregulated the secretion of IL17A through elevating the expression of RAR related orphan receptor C (RORC) [115]. In addition, the combined administration of imatinib and peginterferon α-2b (PegIFNα2b) induced the generation of IFNγ-producing CD8+ T cells [193], and the efficacy of imatinib could be enhanced by Treg cells suppression [141, 192].
The effect of imatinib on NK cells
The therapeutic effect of imatinib in GIST can also be achieved by activating NK cells through inhibiting the KIT signaling in DCs and thus promoting the cross-talk between DCs and NK cells, resulting in the secretion of IFNγ [113, 136, 175, 192, 194]. Imatinib increases the infiltration of NK cells in GIST [99] and augments their ability to secrete IFNγ [95, 113, 134, 175, 192, 193] which was positively correlated with PFS [134, 136] and was an independent predictor of long-term survival of GIST patients with imatinib therapy [136, 175]. In addition, imatinib can activate NK cells via decreasing the expression of IDO in GIST [95]. In clinical practice, imatinib combined with IL-2 stimulates circulating NK cells in GIST patients [135, 198] and increases the expression levels of HLA-DR, TNF-related apoptosis-inducing ligand (TRAIL) and CD56 in NK cells; the abundance of HLA-DR+ NK cells is reported to be associated with PFS and OS in GIST [135, 198].
The effect of imatinib on macrophages
The effect of imatinib on the immune response to GIST is not always beneficial. In GIST patients [97, 116] and KitV558Δ/+ mouse GIST model [116], imatinib, through activating CCAT enhancer binding protein β (C/EBPβ) [116], drives intratumoral macrophage M2 polarization and contributes to the development of immunosuppressive microenvironment, which might partially explain the survival of tumor cells during imatinib therapy. Imatinib also downregulates the expression level of MHC-II molecules in macrophages of GIST mice [116], which contributes to the tumor progression. In addition, it has been reported that imatinib lowered the CD40 expression in macrophages and GIST cells [199], decreased the binding of CD40 to its ligands CD40L and CD154, which were expressed on activated T-helper cells, and thus led to less CD8+ T cell activation [199]. In vitro study also showed that imatinib increased the secretion of IL-10, an anti-inflammatory cytokine, from M1 macrophages [97] and the generation of Treg cells [97]. Therefore, modulation of the polarization status of TAM may be a promising approach for the treatment of GIST in future [97].
The effect of imatinib on immune checkpoint and MHC molecules expression
In human GIST cell lines and KitV558Δ/+ mouse GIST model, imatinib downregulates the expressions of IFNγ-related genes and IFNγ-induced PD-L1 expression by inhibiting STAT1 signaling pathway [35, 102], thereby reducing immune escape and enhancing antitumor immune response. However, imatinib also increased the expression of PD-L1 in T cells within the tumor [35]. Imatinib, through inhibiting the transcription factor ETV4, reduced the IDO expression, leading to the activation of CD8+ T cells and apoptosis of Treg cells [95]. Simultaneous inhibition of KIT, IDO and PD1/PD-L1 in mice was able to enhance the antitumor effect of imatinib by augmenting the function of effector T cells [35].
The expression of MHC-I molecules in GIST is highly heterogeneous, which was further decreased by the weakened type I interferons (IFNs) signaling mediated by imatinib treatment [99, 195]. In patients receiving imatinib treatment, up to 30% of GISTs completely lose and about 40% of GISTs displayed localized loss of MHC-I expression [99]. Moreover, in KitV558Δ/+ GIST mice, Liu et al. reported that imatinib reduced the expression of MHC-I molecules by inhibiting type I IFNs production and signaling, attenuated tumor immunogenicity, decreased the infiltration of CD8+ T cells, and thus weakening the antitumor immune responses [195], which may partially explain the limited efficacy of immunotherapy for GIST patients having received prior imatinib therapy. Considering the role of type I IFNs played in affecting MHC-I expression and thus the antitumor immune responses, type I IFNs signaling has been widely exploited to improve the antitumor effect of imatinib [195]. IFNα is one of the members of type I IFNs family; in human GIST cell lines, IFNα alone is able to induce MHC-I expression, and such effect could be attenuated by imatinib [195]. In addition, the small-molecule agonist of type I IFNs has been shown to activate cGAS-STING (cyclic GMP-AMP synthase-stimulator of interferon genes) pathway and partially overcome the immunosuppressive effect caused by KIT signaling blockade, therefore enhancing the therapeutic efficacy of imatinib [195].
Immunotherapy
Tumor immunotherapy, which harnesses the immune system of the host to eliminate viable tumor cells, has developed rapidly in recent years and been considered as a promising approach for cancer therapy. Since there are large amounts of immune cells infiltrated in GIST and the antitumor effect of imatinib is partly dependent on the immune system, immune cells and molecules are believed to play important roles in the occurrence and progression of GIST. Therefore, therapies by targeting the immune microenvironment of GIST have been proposed to be exploited to reactivate the antitumor immunity of the host immune system and enhance the therapeutic efficacy of imatinib, which may become new strategies to solve the bottleneck of GIST management in future. So far, several immunotherapy approaches have been reported, which include cytokine therapy, ICIs, antibody treatment, antibody–drug conjugates (ADCs), vaccine therapy and adoptive cell therapy (ACT) (Fig. 4). All clinical trials associated with the immunotherapy of GIST are registered on https://clinicaltrials.gov/ and listed in Table 2, and selected results are detailed in the following parts of this review. It is undeniable that the exploration of GIST immunotherapy is still at an early stage with controversial and even unsatisfactory findings, which may due to the immunotherapy reagents used or the patients recruited, and more research studies on GIST immunotherapy are urgently required.

Immunotherapy strategies reported for GIST in literatures. The mostly studied immunotherapies for GIST are immune checkpoint inhibitors and cytokine therapies. Antibodies, antibody–drug conjugates, vaccines and adoptive cell therapies have also been widely evaluated in clinical or preclinical experiments in GIST. New emerging immunotherapy targets, such as WT1, CTA, CSPG4, LAG3, VISTA, Gal-9 and Tim-3, may also be exploited to develop antibody drugs or cell products to treat GIST in future. GIST: gastrointestinal stromal tumor; DC: dendritic cell; MHC-I: major histocompatibility complex class I; TCR: T cell receptors; CTLA-4: cytotoxic T-lymphocyte antigen 4; PD1: programmed cell death protein 1; PD-L1: programmed death-ligand 1; CIK: cytokine-induced killer cell; NKG2D: natural killer group 2 member D; MICA/B: MHC class I chain-related protein A and B; CAR-T: chimeric antigen receptor T; PHA: phytohemagglutinin; GPR20: G protein-coupled receptor 20; SSTR2: somatostatin receptor 2; VEGF: vascular endothelial growth factor; MΦ: macrophages; VISTA: V-type immunoglobulin (Ig) domain-containing suppressor of T-cell activation; Tim-3: T cell immunoglobulin and mucin-domain containing-3; LAG3: lymphocyte activation gene-3; CSPG4: chondroitin sulfate proteoglycan 4; Gal-9: Galectin-9; WT1: Wilms tumor protein 1; CTA: cancer testis antigen
Cytokine-based immunotherapy
Type I IFNs, which contain IFNα and IFNβ, are predominantly produced by macrophages, DC cells and neutrophils infiltrated in the tumor microenvironment [224]. Peginterferon α-2b (PegIFNα2b), a long-acting IFN formed by the combination of polyethylene glycol (PEG) and recombinant IFN-α-2b, has already been tested to treat GIST. Chen et al. administered 8 stage III/IV GIST patients with PegIFNα2b, and found that 4-week combination therapy induced a large amount of IFNγ and increased the infiltration of IFNγ producing CD4+ T, CD8+ T and NK cells [193, 225, 226]. After a median follow-up study of 3.6 years, they found that the overall response rate reached to 100%, and the combination therapy is superior to imatinib treatment alone [193]. To further unravel the underlying mechanisms, Zhang et al. treated the imatinib-resistant GIST cell lines with PegIFNα2b, and showed that the combination of PegIFNα2b and imatinib, but not the PegIFNα2b alone, significantly inhibited cell proliferation and induced cell apoptosis by downregulating p-mTOR (phosphorylated mammalian target of rapamycin) and BCL-2 (B-cell lymphoma-2) [227], suggesting that the combination therapy has synergistic and imatinib-resistance reversing effects [227]. Another research study reported by Pautier et al. showed that the efficacy of the combination of imatinib and IL-2 was better in GIST than renal cell carcinoma (RCC), based on 1 GIST patient [198].
Immune checkpoint inhibitors
Immune checkpoint inhibitors (ICIs) are the most common, effective and promising immunotherapy drugs, which include anti-PD1 antibodies (pembrolizumab, nivolumab and spartalizumab), anti-CTLA-4 antibody (ipilimumab) and anti-PD-L1 antibodies (avelumab and atezolizumab). Even though ICIs have not been approved for the treatment of GIST, many clinical trials are now ongoing to explore the efficacy of ICIs in GIST patients progressing at least to imatinib (Table 3). Unfortunately, most of those clinical trials, to a large extent, were unsuccessful; almost no clear synergy was found between TKIs and ICIs. However, we cannot conclude that ICIs are ineffective, since a small number of patients with advanced GIST have achieved stable disease (SD) or partial response (PR) from ICIs and combination therapies. There is no conclusive biomarker available for now to predict and select GIST patients who may benefit from ICI immunotherapy. Several points should be taken into account to improve the efficacy of ICIs in GIST in future. First, according to published results which will be detailed later, GIST patients with PDGFRA D842V mutation, KIT-WT genotype, TLS presence or high PD-L1 expression seemed to have more probabilities to benefit from ICIs and should be selected preferentially [153, 189]. Second, nearly all clinical trials with ICIs in GIST were conducted in patients with advanced disease, whose antitumor immunity maybe weakened or heavily suppressed by long-term imatinib and multiple lines of TKI therapy, and front-line use of ICIs should be welcomed and explored. Third, similar to other solid tumors, more reliable biomarkers should be developed to identify patients who are sensitive to ICIs and combination therapies to achieve precision immunotherapy.
PD1/PD-L1 inhibitors
As mentioned above, PD-L1 and PD1 are expressed on GIST cells and infiltrating T cells, respectively, and PD1/PD-L1 inhibitors may enhance the cytotoxicity of CD8+ T cells against GIST cells and thus improving patients’ prognosis. In in vitro co-culture experiments of GIST cells and CD8+ T cells, PD-L1 blockade activates CD8+ T cells, and inhibits the proliferation of GIST cells and promotes their apoptosis [153]. In KitV558Δ/+ mouse GIST model, anti-PD1 antibody or anti-PD-L1 antibody alone has no effect on GIST, but it can enhance the antitumor effect of imatinib through increasing the effector function of CD8+ T cells [35]. On the one hand, imatinib activates CD8+ T cells via inhibition of KIT signaling and reduction of IDO expression; on the other hand, PD1/PD-L1 blockade improves the killing activity of CD8+ T cells against GIST cells [35]. In clinic, a case report has shown durable responses following nivolumab treatment in a highly refractory metastatic KIT/PDGFRA-WT GIST patient [235]. Several clinical studies have investigated the therapeutic efficacy of PD1/PD-L1 inhibitors or their combinations with chemicals or antibodies in GIST [34, 238,239,240,241], but the results are unsatisfactory: most patients did not respond to these therapies and quite a few patients achieved PR or SD. In a phase 2 clinical trial, Toulmonde et al. reported that the 6-month non-progression rate of GIST patients treated with cyclophosphamide and pembrolizumab was only 11.1% [34, 232, 233]. Jiang et al. demonstrated that one GIST patient with pembrolizumab treatment achieved SD [239]. Kozak et al. evaluated the efficacy of the combination of avelumab and axitinib for unresectable/metastatic GIST but did not show their findings [240]. Curigliano et al. reported one GIST patient with combined treatment of anti-Tim-3 antibody and spartalizumab, showed progressive disease (PD) [241]. No effect was observed in two GIST patients with multisite metastases receiving pembrolizumab treatment in a retrospective study [238].
CTLA-4 inhibitors
CTLA-4, also known as CD152, is a transmembrane receptor on T cells. T cells lose their cytotoxicity when CTLA-4 was bound by its ligand B7, and CTLA-4 was recognized as a negative regulator of the antitumor immune response. In KitV558Δ/+ mouse GIST model, the combination of imatinib and CTLA-4 inhibitors enhanced the infiltration of CD8+ T cells evidently, strengthened the production of IFNγ markedly, and reduced the tumor size significantly [95]. What’s more, the therapeutic efficacy of the combination therapy group was superior to that of imatinib or CTLA-4 inhibitor alone group, suggesting that synergistic effects exist of these two drugs [95]. These exciting results encouraged researchers to evaluate the effect of CTLA-4 inhibitors in GIST. A phase Ib clinical trial has evaluated the efficacy of the combination of ipilimumab and dasatinib, a second-generation TKI, in 20 advanced refractory GIST patients [229], and showed that durable Choi responses were few and synergistic effect was not observed [229]. Another phase Ib clinical trial has evaluated the efficacy of the combination of imatinib and ipilimumab in 12 metastatic/unresectable GIST patients [230], and found that only 1 gastric GIST patient with KIT/PDGFRA-WT genotype benefited from such combination therapy whom showed PR [230]. The above two clinical trials indicate that ipilimumab is clinically safe, but it seems to fail to trigger strong antitumor immune responses in patients with advanced GIST.
Dual inhibition of PD1/PD-L1 and CTLA-4
Two phase II clinical trials have examined the efficacy of nivolumab with or without ipilimumab in advanced GIST population, but contrasting results were obtained [236, 237]. One of the clinical trials reported by Singh et al. showed that 10 out of 19 patients receiving nivolumab alone had SD; and among the 16 patients receiving the combined therapy of nivolumab and ipilimumab, 1 patient had CR and 4 patients had SD [237]. These results suggested that immunotherapy is safe and GIST patients can benefit from ICIs. The GIST patient who had CR had primary mutation on exon 11 and secondary mutation on exon 17 of KIT gene [237]. Moreover, among the GIST patients who have benefited from ICIs for more than 6 months, 5 had tumors originated from the small intestine [237], indicating that intestinal GIST patients may be more likely to benefit from ICIs. Nevertheless, the cohort study of Alliance A091401 showed objective responses in neither 9 GIST patients undergoing nivolumab alone nor another 9 GIST patients receiving the combined therapy [236]; the median PFS of patients in single-agent nivolumab group and combined treatment group were 1.5 and 2.9 months, respectively [236]. Besides, A phase I clinical trial, with 9 metastatic or unresectable advanced GIST patients receiving different ICIs (not specified), reported that 3 patients had SD [231] and 1 patient showed hyper-progressive disease [231].
Antibody-based immunotherapy
Monoclonal antibodies have been widely used for treating various types of tumors. Many research studies have evaluated the antitumor effects of antibodies against KIT [242,243,244] and CD40 [199] in mouse GIST models, and antibodies against PDGFRA [245], VEGF [246] and XmAb18087, an bispecific antibody targeting SSTR2 and CD3 simultaneously [217], in GIST patients. The findings obtained from the above studies will be systematically discussed below.
A series of research studies by Edris et al. [242, 243] showed that the anti-KIT monoclonal antibody, SR1, reduced the expression of KIT in tumor cells, strengthened the phagocytotic effect of macrophages and induced tumor cell death; its killing effect was not associated with imatinib sensitivity or resistance [242, 243]. These results suggested that anti-KIT monoclonal antibody has great potential for the treatment of GIST and might circumvent TKIs resistance, the bottleneck of the management of advanced GIST. However, CK6, another anti-KIT monoclonal antibody developed by Looy et al., failed to inhibit tumor growth in patient-derived xenograft (PDX) model, and had no synergistic antitumor effect with imatinib [244]. CD40, which is mainly expressed on the surface of APCs, is a member of the tumor necrosis factor receptor superfamily (TNFRSF) and also known as TNFRSF5. In KitV558Δ/+ mouse GIST model, anti-CD40 antibody activated tumor-associated macrophages (TAMs) to produce TNFα, and enhanced the antitumor activity of imatinib [199]. The effect of anti-CD40 antibody mainly depended on TAM, followed by CD8+ T cells, and was independent on CD4+ T and B cells [199].
In GIST, the expression of VEGF is associated with poor prognosis [246]. The anti-VEGF monoclonal antibody, bevacizumab, is effective in a variety of solid tumors. Blanke et al. evaluated the therapeutic effect of bevacizumab in patients with metastatic/unresectable GIST; however, due to the small number of GIST patients enrolled and the efficacy of bevacizumab was not satisfactory, the clinical trial was terminated without consolidated conclusions [246]. The efficacy of olaratumab, an anti-PDGFRA monoclonal antibody, has been examined in 31 patients with metastatic and/or unresectable GIST (but only 20 out of 31 patients were evaluable) in 2017 [245]; no CR and PR were observed and only 5 patients had SD [245]. Tidutamab, previously known as XmAb18087, is a bispecific antibody targeting somatostatin receptor 2 (SSTR2) and CD3 simultaneously, and the former is highly expressed in GIST [247]. There is an ongoing clinical trial (NCT03411915) investigating the therapeutic effect of tidutamab on patients with advanced GIST and neuroendocrine tumors [217].
Antibody–drug conjugates
Antibody–drug conjugates (ADC) are a kind of promising drugs in immunotherapy which chemically bond monoclonal antibodies and bioactive cytotoxic drugs. So far, two anti-KIT ADCs (LOP628-DM1 and NN2101-DM1) [248,249,250] and one anti-GPR20 ADC (DS-6157a) [251, 252] have been developed and tested in GIST. LOP628-emtansine (DM1) is sensitive in tumor cells with high KIT level, regardless of its mutational status, suggesting that this ADC may be used in the treatment of KIT-mutant and KIT-WT GIST [248,249,250], but the hypersensitivity reactions (HSRs) caused by LOP628-DM1 may constrain its usage in clinic [250]. Similarly, NN2101-DM1 was also found to inhibit the tumor growth in GIST both in vivo and in vitro, and exerted its effect regardless of KIT mutations [253]. As for DS-6157a, it is a conjugate of anti-GPR20 antibody and DNA topoisomerase I inhibitor exatecan derivative (DX-8951 derivative, DXd), which demonstrated strong cell killing activity against GIST in cell lines, cell line-derived xenograft (CDX) and PDX models [251, 252], and a phase I clinical trial examining the antitumor effect of DS-6157a in GIST patients is now ongoing [220].
Vaccine-based immunotherapy
Vaccine is a novel approach of tumor immunotherapy. As early as 2001, Shioyama et al. reported an inoperable GIST patient whose tumor size was reduced from 11 cm in diameter to 20 mm after receiving intratumoral injection of vaccine OK432 (5 KE) [254]. Ilixadencel, also known as Intuvax, is an allogeneic DC vaccine which primes antitumor immune responses after intratumoral injection. The therapeutic efficacy of ilixadencel has been evaluated in 6 unresectable or metastatic GIST patients, and 33% of patients had radiological tumor responses [255, 256], supporting the necessity of further investigations in future.
Adoptive cell therapy
Adoptive cell therapy (ACT) refers to collecting immune cells from patients, followed by cell expansion and genetic engineering in vitro, and then transfuses the modified cells back into the patients. Up to now, three research teams have explored the efficacy of ACT in GIST. The first one constructed chimeric antigen receptor T (CAR-T) cells targeting KIT in 2013 [257], and then demonstrated that such cells were able to produce IFNγ in vitro, lysed the cultured GIST cells and inhibit tumor growth in CDX model [257]. The second one stated, in 2019, that ACT and personalized vaccines can successfully treat recurrent GISTs [258]; eight refractory recurrent GIST patients were intravenously administrated with allogenous phytohemagglutinin (PHA)-activated T cells, personalized vaccines and low dose of interleukin-2, and 5 of them showed remissions, 1 had SD and 2 had PD after a 14-month follow-up study [258], suggesting that this therapy was safe and effective, at least for some GIST patients [258]. The third one got cytokine-induced killer cells (CIKs) from KIT/PDGFRA-WT GIST patients in 2022, and found that patient-derived CIKs killed autologous imatinib- and sunitinib-resistant tumor cells either directly or indirectly [259].
Other potential immunotherapy targets
In addition to the aforementioned immunotherapies, here are some other potential immunotherapy targets for GIST. Both M2 macrophages, one of the most abundant cells in the microenvironment of GIST [97, 101, 104] and Treg cells, which highly express CCR8 [97, 178], are involved in immune escape, therefore, they are considered as the targets for GIST immunotherapy. Moreover, LAG3 [35] and Tim-3 [35, 108] are present in tumor-infiltrating lymphocytes, suggesting that they may participate in immune escape of GIST and are the potential targets for immunotherapy. CTAs have been reported to be expressed in 26.7%-40% of GIST patients [168,169,170]; immune cells against these CTAs molecules will be established in the near future to treat GIST. In addition, Wilms tumor protein 1 (WT-1) [260] and chondroitin sulfate proteoglycan 4 (CSPG4) [261], which are overexpressed on GIST cells, are also regarded as new potential immunotherapy targets of GIST.
Research models for GIST
Basic and translational researches of GIST cannot be accomplished without appropriate experimental models, such as cells, animals and organoids, and the available models for GIST in literatures are illustrated in Fig. 5. The cell models mainly include primary cell culture [262] and immortalized cell lines; due to convenience and cost-effectiveness, cell lines are widely used in GIST studies, for example, GIST882, GIST-T1, GIST430, GIST48 and mouse S2 cells [116, 191, 199, 263, 264]. The major characteristics of GIST cell lines are described in Table 4. The reported animal models include the rat GIST model [265], chicken embryo model [266], lymph node metastasis mice [267], peritoneal dissemination mice [268], spleen-to-liver metastasis mice [176, 177, 269, 270], PDX and genetically engineered mouse models (GEMMs), with the latter two are the most widely used animal GIST models. The PDX model, which is established by implantation of tumor tissues [251, 271, 272] or primary cells derived from GIST patients [273,274,275] into immunodeficient mice, keeps most of the characteristics of primary GISTs at the histopathological, biological and genetic levels, but is not suitable for immune research. The GEMMs refer to mice that are modified by genetic engineering technology and develop GIST spontaneously with competent immune system. In view of the technical difficulties in construction and high cost during maintenance, only limited GEMMs for GIST have been successfully established, which are summarized in detail in Table 5. Tumor organoids are three-dimensional structures constructed by in vitro 3D culture of tumor tissues collected from patients; they not only maintain the morphological structure of tumors, but also keep the tumor gene expression and heterogeneity. As for the organoids for GIST, they are still in an initial stage; only Cao et al. [276] and Forsythe et al. [277] reported the establishment of GIST organoids and figured out that organoids may have the potential for the precise treatment of GIST.

Models for GIST research in literatures. Cell lines, CDX, PDX and genetically engineered mouse models are the most frequently used models. chicken embryo model and the duodenal reflux induced rat model have been reported for GIST but haven't been widely applied. Organoid models are emerging and hold brilliant future. CDX: cell line-derived xenograft; PDX: patient-derived xenograft
The immune microenvironment plays an important role in the pathogenesis and progression of GIST; however, most of the aforementioned experimental models for GIST lack in vivo immune microenvironment. Relatively speaking, the GEMMs better preserve the in vivo immune microenvironment, making them the best approach to examine the immuno-oncology of GIST and to develop drugs for GIST immunotherapy. So far, the established GEMMs mainly focus on mutations of KIT and BRAF, and mouse GIST models for other gene mutations are still underexplored. Moreover, most GIST mice driven by germline gene mutations develop tumors mainly in the cecum, which are not consistent with the conditions of human GISTs which almost originate from stomach and small intestine. Therefore, mouse GIST models that resemble human GIST conditions are urgently needed.
Conclusions and future perspectives
In summary, GISTs are predominantly populated by macrophages and T cells, and to a lesser extent, by NK and B cells, and the distribution of other immune cell subtypes are unclear up to now. The levels of intratumoral immune cells are associated with clinical outcomes and clinicopathological features of GIST patients, while their functions and underlying molecular mechanisms in the tumorigenesis, progression, metastasis and drug resistance of GIST require more attentions. The numbers of intratumoral immune cells are related to driver gene mutations, metastases and anatomical locations, and are modulated by various lines of targeted therapies, however nearly no research work have yet answered that how these factors reshaped the immune landscape of GIST exactly. The immune profiling analyses are mainly accomplished by immunohistochemistry (IHC), and rarely by flow cytometry or immunofluorescence, therefore, available conclusions need to be further confirmed and new immunotherapy targets need to be identified by more sophisticated techniques, such as multiplex immunohistochemistry and immunofluorescence (mIHC/mIF), which simultaneously evaluate the expression of multiple biomarkers within a single tissue slice [309], and single-cell multiomics which dissect the various intratumoral immune cell subtypes and identify the key regulators of antitumor immunity at high resolutions [310].
The microenvironments of GISTs are grossly immunosuppressive, which are mediated by the infiltration of M2 macrophages [34] and Treg cells [97], high-expression of IDO on GIST cells [124] and immunosuppressive receptors on NK cells [134], and deficient expression of MHC-I on APCs [97]. Though CD8+ T cells are enriched in GIST [127], the CD8+ T/Treg cell ratio is relative low [97], and might be further inhibited by PD-L1 on GIST cells [124], and by glucocorticoid-induced TNF receptor-related protein (GITR) and inducible T-cell costimulator (ICOS) on Treg cells [166]. Besides, NK cells were found to be CD69 negative, suggesting they are in a dysfunctional state. Taken together, several factors contribute to the development of immunosuppressive microenvironments [97], which might mediate the primary resistance to ICIs in GIST [34].
Imatinib exerts antitumor activity by its direct killing ability on the tumor cells and indirect off-target effects on immune cells. The immunological effects of imatinib in GIST are complex, analytical researches are still necessary to dissect the exact roles of imatinib in GIST immuno-oncology. In general, short-term usage of imatinib enhances the host antitumor immune responses by activating CD8+ T cells, DC cells and NK cells, and inhibiting Treg cells. While chronic administration of imatinib may contribute to the immunosuppressive microenvironment of GIST by inducing the M2 polarization of macrophages, the loss of MHC-I expression, and the decrease of the activity of CD8+ T cells, and all these changes maybe the reasons of low response rates to ICIs in heavily pretreated GIST patients.
Several clinical and pre-clinical trials have been conducted in GIST to examine the effects of immunotherapies, such as cytokines, ICIs, antibodies, ADCs, vaccines and ACTs. Some of the findings are promising, while the others are controversial and unsatisfactory, especially for ICIs, which include anti-PD1/PD-L1 and anti-CTLA-4 antibodies and are the most widely studied drugs in heavily pretreated GIST patients. The relative low expression of PD1/PD-L1 and the loss of MHC-I in GIST may partially explain the low responsiveness to ICIs, which suggests that other new emerging immunotherapy targets, such as M2 macrophages, Treg cells, LAG3, Tim-3, CTAs, WT-1 and CSPG4, deserve more attentions. Since a few GIST patients did benefit from ICIs, which are consistent with other solid tumors, reliable biomarkers should be developed, patients should be carefully selected, combination therapy and front-line immunotherapy should be warmly recommended and encouraged in future investigations [311].
The establishments of GIST cell lines, CDX/PDX models and GEMMs considerably facilitate the research and understanding of the pathogenesis, progression, metastasis and drug resistance, and noticeably accelerate the screening and development of novel therapeutic targets and drugs, which in turn improve the management and outcome of GIST patients. However, these reported models cannot fully recapitulate the features of human GIST, such as the morphology, gene expression pattern and heterogeneity, and preserve the immune microenvironment, which seriously hinder the immuno-oncology research and the development of immunotherapy drugs. GEMMs harbor competent immune microenvironment but develop tumors in the cecum, which are scarcely observed in human GISTs. GIST models that more resemble the human GISTs in anatomy, genotype, phenotype and drug resistance are urgently needed. In addition, vascularized and immunized organoids [312] may be other models with brilliant prospect for studying GIST in near future.
Fundings
This study was supported by grants from the Guangdong Provincial Key Laboratory of Digestive Cancer Research (2021B1212040006), the Guangdong-Hong Kong-Macau University Joint Laboratory of Digestive Cancer Research (2021LSYS003), the Shenzhen Key Laboratory of Chinese Medicine Active Substance Screening and Translational Research (ZDSYS20220606100801003), the Shenzhen-Hong Kong-Macau Technology Research Program (Type C) (SGDX20201103092601008), the Guangdong Basic and Applied Basic Research Foundation (2022A1515110194, 2021B1515120069, 2022A1515110156), the National Natural Science Foundation of China (U20A20379, 82220108013), the Shenzhen Fundamental Research Program (JCYJ20220530142203008, JCYJ20190809142807444), the Shenzhen Sustainable Project (KCXFZ20200201101059392), and the Sanming Project of Medicine in Shenzhen (SZSM201911010).
Availability of data and materials
Not applicable.
Abbreviations
- ACT:
-
Adoptive cell therapy
- ADCC:
-
Antibody-dependent cellular cytotoxicity
- ADCs:
-
Antibody–drug conjugates
- AFIP:
-
Armed Forces Institute of Pathology
- APCs:
-
Antigen presenting cells
- BCL-2:
-
B-cell lymphoma-2
- BIRC3:
-
Baculoviral IAP repeat-containing protein 3
- BRAF:
-
B-Raf proto-oncogene
- CAR-T:
-
Chimeric antigen receptor T
- CCL:
-
C–C motif chemokine ligand
- CCR:
-
C–C chemokine receptor
- CDC:
-
Complement-dependent cytotoxicity
- CDX:
-
Cell line-derived xenograft
- C/EBPβ:
-
CCAT enhancer binding protein β
- cGAS-STING:
-
Cyclic GMP-AMP synthase-stimulator of interferon genes
- CIKs:
-
Cytokine-induced killer cells
- CR:
-
Complete response
- CSPG4:
-
Chondroitin sulfate proteoglycan 4
- CTAs:
-
Cancer testis antigens
- CTLA-4:
-
Cytotoxic T-lymphocyte antigen 4
- CXCL:
-
C-X-C motif chemokine ligand
- CXCR:
-
C-X-C chemokine receptor
- DC:
-
Dendritic cell
- DFS:
-
Disease-free survival
- DKK4:
-
Dickkopf 4
- DM1:
-
Emtansine
- DXd:
-
DX-8951 derivative
- EC:
-
Extracellular domain
- EIIS:
-
Expanded IFNγ-induced immune signature
- ETV4:
-
ETS variant transcription factor 4
- FDA:
-
Food and Drug Administration
- GAGE:
-
G antigen
- Gal-9:
-
Galectin-9
- γδ T cell:
-
Gamma delta T cells with TCRs composed of γ- and δ-chains
- GEMMs:
-
Genetically engineered mouse models
- GIST:
-
Gastrointestinal stromal tumor
- GITR:
-
Glucocorticoid-induced TNF receptor-related protein
- GPR20:
-
G protein-coupled receptor 20
- HALP:
-
The combined index of hemoglobin, albumin, lymphocyte, and platelet
- HGF:
-
Hepatocyte growth factor
- HLAs:
-
Human leukocyte antigens
- HSRs:
-
Hypersensitivity reactions
- ICCs:
-
Interstitial cells of Cajal
- ICIs:
-
Immune checkpoint inhibitors
- ICOS:
-
Inducible T cell costimulator
- IDO:
-
Indoleamine 2,3-dioxygenase
- IFN:
-
Interferon
- Ig:
-
Immunoglobulin
- IHC:
-
Immunohistochemistry
- IL:
-
Interleukin
- JM:
-
Juxtamembrane domain
- LAG3:
-
Lymphocyte activation gene-3
- LMR:
-
Lymphocyte-to-monocyte ratio
- LWR:
-
Lymphocyte-to-white cell ratio
- MΦ:
-
Macrophages;
- M1:
-
M1 macrophages that are classically activated
- M2:
-
M2 macrophages that are alternatively activated
- MAGE:
-
Melanoma-associated antigen
- MDSCs:
-
Myeloid-derived suppressor cells
- MHC:
-
Major histocompatibility complex
- MICA/B:
-
MHC class I chain-related protein A and B
- mIHC/mIF:
-
Multiplex immunohistochemistry and immunofluorescence
- MLR:
-
Monocyte-to-lymphocyte ratio
- ML-CTC:
-
Macrophage-like circulating tumor cells
- MWR:
-
Monocyte-to-white cell ratio
- NAR:
-
Neutrophil-to-albumin ratio
- NCR1:
-
Natural cytotoxicity triggering receptor 1
- NF1:
-
Neurofibromatosis type 1
- NF-kB:
-
Nuclear factor kappa-light-chain-enhancer of activated B cells
- NK:
-
Natural killer cell
- NKG2D:
-
Natural killer group 2 member D
- NKp30:
-
Natural killer cell p30-related protein
- NKp46:
-
Natural killer cell p46-related protein
- NKT:
-
Natural killer T cells
- NLR:
-
Neutrophil-to-lymphocyte ratio
- NSCLC:
-
Non-small cell lung cancer
- NWR:
-
Neutrophil-to-white blood cell ratio
- NY-ESO-1:
-
New York esophageal squamous cell carcinoma-1
- OS:
-
Overall survival
- PBMC:
-
Peripheral blood mononuclear cell
- PD:
-
Progressive disease
- PD1:
-
Programmed cell death protein 1
- PDGFRA:
-
Platelet-derived growth factor receptor alpha
- PDX:
-
Patient-derived xenograft
- PD-L1:
-
Programmed death-ligand 1
- PEG:
-
Polyethylene glycol
- PegIFNα2b:
-
Peginterferon α-2b
- PFS:
-
Progression-free survival
- PHA:
-
Phytohemagglutinin
- PLR:
-
Platelet-to-lymphocyte ratio
- PNI:
-
Prognostic nutritional index
- PR:
-
Partial response
- PWR:
-
Platelet-to-white cell ratio
- p-mTOR:
-
Phosphorylated mammalian target of rapamycin (mTOR)
- RAS:
-
Rat sarcoma viral oncogene
- RCC:
-
Renal cell carcinoma
- RFS:
-
Recurrence-free survival
- RORC:
-
RAR related orphan receptor C
- ROS:
-
Reactive oxygen species
- SD:
-
Stable disease
- SDH:
-
Succinate dehydrogenase
- SIC-E:
-
Sarcoma immune classes-E
- SII:
-
Systemic immunoinflammatory index
- SPARCL1:
-
Secreted protein acidic and rich in cysteine-like 1
- SSTR2:
-
Somatostatin receptor 2
- STS:
-
Soft tissue sarcoma
- TAM:
-
Tumor-associated macrophage
- TCR:
-
T cell receptor
- TGFβ:
-
Transforming growth factor beta
- Th1:
-
T helper type 1 cell
- Th2:
-
T helper type 2 cell
- TILs:
-
Tumor-infiltrating lymphocytes
- Tim-3:
-
T cell immunoglobulin and mucin-domain containing-3
- TIS:
-
T-cell-inflamed signature
- TK:
-
Tyrosine kinase domain
- TKIs:
-
Tyrosine kinase inhibitors
- TLS:
-
Tertiary lymphoid structures
- TM:
-
Transmembrane domain
- Tn:
-
Naive T cells
- TNFα:
-
Tumor necrosis factor alpha
- TNFRSF:
-
Tumor necrosis factor receptor superfamily
- TRAF1:
-
Tumor necrosis factor receptor (TNFR) associated factor 1
- TRAIL:
-
TNF-related apoptosis-inducing ligand
- Treg:
-
Regulatory T cell
- VEGF:
-
Vascular endothelial growth factor
- VISTA:
-
V-type immunoglobulin (Ig) domain-containing suppressor of T-cell activation
- WT:
-
Wild type
- WT-1:
-
Wilms tumor protein 1
References
Campanella NC, Oliveira ATd, Scapulatempo-Neto C, Guimarães DP, Reis RM. Biomarkers and novel therapeutic targets in gastrointestinal stromal tumors (GISTs). Recent Pat Anticancer Drug Discov. 2013;8(3):288–97.
Søreide K, Sandvik OM, Søreide JA, Giljaca V, Jureckova A, Bulusu VR. Global epidemiology of gastrointestinal stromal tumours (GIST): A systematic review of population-based cohort studies. Cancer Epidemiol. 2015;40:39–46.
Casali PG, Blay JY, Abecassis N, Bajpai J, Bauer S, Biagini R, Bielack S, Bonvalot S, Boukovinas I, Bovee JVMG, Boye K, Brodowicz T, Buonadonna A, Álava ED, Tos APD, Muro XGD, Dufresne A, Eriksson M, Fedenko A, Ferraresi V, Ferrari A, Frezza AM, Gasperoni S, Gelderblom H, Gouin F, Grignani G, Haas R, Hassan AB, Hindi N, Hohenberger P, Joensuu H, Jones RL, Jungels C, Jutte P, Kasper B, Kawai A, Kopeckova K, Krákorová DA, Cesne AL, Grange FL, Legius E, Leithner A, Lopez-Pousa A, Martin-Broto J, Merimsky O, Messiou C, Miah AB, Mir O, Montemurro M, Morosi C, Palmerini E, Pantaleo MA, Piana R, Piperno-Neumann S, Reichardt P, Rutkowski P, Safwat AA, Sangalli C, Sbaraglia M, Scheipl S, Schöffski P, Sleijfer S, Strauss D, Strauss SJ, Hall KS, Trama A, Unk M, Sande MAJvd, Graaf WTAvd, Houdt WJv, Frebourg T, Gronchi A, Stacchiotti S, Committee EG, GENTURIS Ea. Gastrointestinal stromal tumours ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(1):20–33.
Zhang B, Zhu F, Li P, Zhu J. Artificial intelligence-assisted endoscopic ultrasound in the diagnosis of gastrointestinal stromal tumors: a meta-analysis. Surg Endosc. 2023;37(3):1649-57.
Poveda A, Muro XGD, López-Guerrero JA, Cubedo R, Martínez V, Romero I, Serrano C, Valverde C, Martín-Broto J. GEIS guidelines for gastrointestinal sarcomas (GIST). Cancer Treat Rev. 2017;55:107–19.
Zhang J, Chen K, Tang Y, Luan X, Zheng X, Lu X, Mao J, Hu L, Zhang S, Zhang X, Chen W. LncRNA-HOTAIR activates autophagy and promotes the imatinib resistance of gastrointestinal stromal tumor cells through a mechanism involving the miR-130a/ATG2B pathway. Cell Death Dis. 2021;12(4):367.
Kang N, Gu H, Ni Y, Wei X, Zheng S. Prognostic and clinicopathological significance of the Prognostic Nutritional Index in patients with gastrointestinal stromal tumours undergoing surgery: a meta-analysis. BMJ Open. 2022;12(12): e064577.
DeMatteo RP, Lewis JJ, Leung D, Mudan SS, Woodruff JM, Brennan MF. Two hundred gastrointestinal stromal tumors: recurrence patterns and prognostic factors for survival. Ann Surg. 2000;231(1):51–8.
Yu X, Liang X, Wen K. Clinical characteristics and prognosis of gastrointestinal stromal tumors with rare site metastasis (Review). Oncol Lett. 2022;24(6):453.
Cavnar MJ, Seier K, Curtin C, Balachandran VP, Coit DG, Yoon SS, Crago AM, Strong VE, Tap WD, Gönen M, Antonescu CR, Brennan MF, Singer S, DeMatteo RP. Outcome of 1000 Patients With Gastrointestinal Stromal Tumor (GIST) treated by surgery in the pre- and post-imatinib eras. Ann Surg. 2021;273(1):128–38.
Hirota S, Isozaki K, Moriyama Y, Hashimoto K, Nishida T, Ishiguro S, Kawano K, Hanada M, Kurata A, Takeda M, Tunio GM, Matsuzawa Y, Kanakura Y, Shinomura Y, Kitamura Y. Gain-of-function mutations of c-kit in human gastrointestinal stromal tumors. Science. 1998;279(5350):577–80.
Heinrich MC, Corless CL, Duensing A, McGreevey L, Chen C-J, Joseph N, Singer S, Griffith DJ, Haley A, Town A, Demetri GD, Fletcher CDM, Fletcher JA. PDGFRA activating mutations in gastrointestinal stromal tumors. Science. 2003;299(5607):708–10.
Dermawan JK, Rubin BP. Molecular pathogenesis of gastrointestinal stromal tumor: a paradigm for personalized medicine. Annu Rev Pathol. 2022;17:323–44.
Blay J-Y, Kang Y-K, Nishida T, Mehren Mv. Gastrointestinal stromal tumours. Nat Rev Dis Primers. 2021;7(1):22.
Brčić I, Argyropoulos A, Liegl-Atzwanger B. Update on molecular genetics of gastrointestinal stromal tumors. Diagnostics (Basel). 2021;11(2):194.
Doyle LA, Hornick JL. Gastrointestinal stromal tumours: from KIT to succinate dehydrogenase. Histopathology. 2014;64(1):53–67.
Nishida T, Yoshinaga S, Takahashi T, Naito Y. Recent progress and challenges in the diagnosis and treatment of gastrointestinal stromal tumors. Cancers (Basel). 2021;13(13):3158.
Klug LR, Khosroyani HM, Kent JD, Heinrich MC. New treatment strategies for advanced-stage gastrointestinal stromal tumours. Nat Rev Clin Oncol. 2022;19(5):328–41.
Zalupski M, Metch B, Balcerzak S, Fletcher WS, Chapman R, Bonnet JD, Weiss GR, Ryan J, Benjamin RS, Baker LH. Phase III comparison of doxorubicin and dacarbazine given by bolus versus infusion in patients with soft-tissue sarcomas: a Southwest oncology group study. J Natl Cancer Inst. 1991;83(13):926–32.
Ryan DP, Puchalski T, Supko JG, Harmon D, Maki R, Garcia-Carbonero R, Kuhlman C, Winkelman J, Merriam P, Quigley T, Jimeno J, Manola J, Demetri GD. A phase II and pharmacokinetic study of ecteinascidin 743 in patients with gastrointestinal stromal tumors. Oncologist. 2002;7(6):531–8.
Trent JC, Beach J, Burgess MA, Papadopolous N, Chen LL, Benjamin RS, Patel SR. A two-arm phase II study of temozolomide in patients with advanced gastrointestinal stromal tumors and other soft tissue sarcomas. Cancer. 2003;98(12):2693–9.
Merry E, Thway K, Jones RL, Huang PH. Predictive and prognostic transcriptomic biomarkers in soft tissue sarcomas. NPJ Precis Oncol. 2021;5(1):17.
Dematteo RP, Ballman KV, Antonescu CR, Maki RG, Pisters PWT, Demetri GD, Blackstein ME, Blanke CD, Mehren Mv, Brennan MF, Patel S, McCarter MD, Polikoff JA, Tan BR, Owzar K, Team ACoSOGAIAGS. Adjuvant imatinib mesylate after resection of localised, primary gastrointestinal stromal tumour: a randomised, double-blind, placebo-controlled trial. Lancet. 2009;373(9669):1097–104.
Patrikidou A, Chabaud S, Ray-Coquard I, Bui BN, Adenis A, Rios M, Bertucci F, Duffaud F, Chevreau C, Cupissol D, Domont J, Pérol D, Blay JY, Cesne AL, Group FS. Influence of imatinib interruption and rechallenge on the residual disease in patients with advanced GIST: results of the BFR14 prospective French sarcoma group randomised, phase III trial. Ann Oncol. 2013;24(4):1087–93.
Verweij J, Casali PG, Zalcberg J, LeCesne A, Reichardt P, Blay J-Y, Issels R, Oosterom Av, Hogendoorn PCW, Glabbeke MV, Bertulli R, Judson I. Progression-free survival in gastrointestinal stromal tumours with high-dose imatinib: randomised trial. Lancet. 2004;364(9440):1127–34.
Blanke CD, Rankin C, Demetri GD, Ryan CW, Mehren Mv, Benjamin RS, Raymond AK, Bramwell VHC, Baker LH, Maki RG, Tanaka M, Hecht JR, Heinrich MC, Fletcher CDM, Crowley JJ, Borden EC. Phase III randomized, intergroup trial assessing imatinib mesylate at two dose levels in patients with unresectable or metastatic gastrointestinal stromal tumors expressing the kit receptor tyrosine kinase: S0033. J Clin Oncol. 2008;26(4):626–32.
Casali PG, Zalcberg J, Cesne AL, Reichardt P, Blay J-Y, Lindner LH, Judson IR, Schöffski P, Leyvraz S, Italiano A, Grünwald V, Pousa AL, Kotasek D, Sleijfer S, Kerst JM, Rutkowski P, Fumagalli E, Hogendoorn P, Litière S, Marreaud S, Graaf Wvd, Gronchi A, Verweij J, Group EOfRaToCSTaBS, Group IS, Group AGT. Ten-year progression-free and overall survival in patients with unresectable or metastatic GI stromal tumors: long-term analysis of the European organisation for research and treatment of cancer, Italian sarcoma group, and Australasian gastrointestinal trials group intergroup phase III randomized trial on Imatinib at two dose levels. J Clin Oncol. 2017;35(15):1713–20.
Demetri GD, Mehren MV, Blanke CD, Abbeele ADVd, Eisenberg B, Roberts PJ, Heinrich MC, Tuveson DA, Singer S, Janicek M, Fletcher JA, Silverman SG, Silberman SL, Capdeville R, Kiese B, Peng B, Dimitrijevic S, Druker BJ, Corless C, Fletcher CDM, Joensuu H. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med. 2002;47(7):472–80.
Demetri GD, Oosterom ATv, Garrett CR, Blackstein ME, Shah MH, Verweij J, McArthur G, Judson IR, Heinrich MC, Morgan JA, Desai J, Fletcher CD, George S, Bello CL, Huang X, Baum CM, Casali PG. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006;368(9544):1329–38.
Demetri GD, Reichardt P, Kang Y-K, Blay J-Y, Rutkowski P, Gelderblom H, Hohenberger P, Leahy M, Mehren Mv, Joensuu H, Badalamenti G, Blackstein M, Cesne AL, Schöffski P, Maki RG, Bauer S, Nguyen BB, Xu J, Nishida T, Chung J, Kappeler C, Kuss I, Laurent D, Casali PG, investigators Gs. Efficacy and safety of regorafenib for advanced gastrointestinal stromal tumours after failure of imatinib and sunitinib (GRID): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2013;381(9863):295–302.
Blay J-Y, Serrano C, Heinrich MC, Zalcberg J, Bauer S, Gelderblom H, Schöffski P, Jones RL, Attia S, D’Amato G, Chi P, Reichardt P, Meade J, Shi K, Ruiz-Soto R, George S. Mehren Mv. Ripretinib in patients with advanced gastrointestinal stromal tumours (INVICTUS): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2020;21(7):923–34.
Mehren MV, Heinrich MC, Shi H, Iannazzo S, Mankoski R, Dimitrijević S, Hoehn G, Chiroli S, George S. Clinical efficacy comparison of avapritinib with other tyrosine kinase inhibitors in gastrointestinal stromal tumors with PDGFRA D842V mutation: a retrospective analysis of clinical trial and real-world data. BMC Cancer. 2021;21(1):291.
Proudman D, Miller A, Nellesen D, Gomes A, Mankoski R, Norregaard C, Sullivan E. Financial implications of avapritinib for treatment of unresectable gastrointestinal stromal tumors in patients with a PDGFRA exon 18 variant or after 3 previous therapies in a hypothetical US health plan. JAMA Netw Open. 2020;3(11): e2025866.
Toulmonde M, Penel N, Adam J, Chevreau C, Blay J-Y, Cesne AL, Bompas E, Piperno-Neumann S, Cousin S, Grellety T, Ryckewaert T, Bessede A, Ghiringhelli F, Pulido M, Italiano A. Use of PD-1 targeting, macrophage infiltration, and IDO pathway activation in sarcomas: a phase 2 clinical trial. JAMA Oncol. 2018;4(1):93–7.
Seifert AM, Zeng S, Zhang JQ, Kim TS, Cohen NA, Beckman MJ, Medina BD, Maltbaek JH, Loo JK, Crawley MH, Rossi F, Besmer P, Antonescu CR, DeMatteo RP. PD-1/PD-L1 blockade enhances T-cell activity and antitumor efficacy of imatinib in gastrointestinal stromal tumors. Clin Cancer Res. 2017;23(2):454–65.
Erin N, Grahovac J, Brozovic A, Efferth T. Tumor microenvironment and epithelial mesenchymal transition as targets to overcome tumor multidrug resistance. Drug Resist Updat. 2020;53: 100715.
Hanahan D. Hallmarks of cancer: new dimensions. Cancer Discov. 2022;12(1):31–46.
Cananzi FCM, Minerva EM, Samà L, Ruspi L, Sicoli F, Conti L, Romario UF, Quagliuolo VL. Preoperative monocyte-to-lymphocyte ratio predicts recurrence in gastrointestinal stromal tumors. J Surg Oncol. 2019;119(1):12–20.
Racz JM, Cleghorn MC, Jimenez MC, Atenafu EG, Jackson TD, Okrainec A, Raghavan LV, Quereshy FA. Predictive ability of blood neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios in gastrointestinal stromal tumors. Ann Surg Oncol. 2015;22(7):2343–50.
Supsamutchai C, Wilasrusmee C, Hiranyatheb P, Jirasiritham J, Rakchob T, Choikrua P. A cohort study of prognostic factors associated with recurrence or metastasis of gastrointestinal stromal tumor (GIST) of stomach. Ann Med Surg (Lond). 2018;35:1–5.
Mo D-C, Liu X, Lv Y-J, Qin Y-Q, Xie G-S. Is monocyte-to-lymphocyte ratio the best systematic inflammatory biomarker for the prognosis of gastrointestinal stromal tumors? J Surg Oncol. 2019;119(7):1024–5.
Perez DR, Baser RE, Cavnar MJ, Balachandran VP, Antonescu CR, Tap WD, Strong VE, Brennan MF, Coit DG, Singer S, Dematteo RP. Blood neutrophil-to-lymphocyte ratio is prognostic in gastrointestinal stromal tumor. Ann Surg Oncol. 2013;20(2):593–9.
Jin X, Feng L, Li F, Yang C, Wang N. Relation between blood neutrophil-to-lymphocyte ratio and prognostic of patients with gastrointestinal stromal tumor and its clinical significance (in Chinese). Chin J Bases Clin General Surg. 2013;20(8):910–4.
Atila K, Arslan NC, Derici S, Canda AE, Sagol O, Oztop I, Bora S. Neutrophil-to-lymphocyte ratio: could it be used in the clinic as prognostic marker for gastrointestinal stromal tumor? Hepatogastroenterology. 2014;61(134):1649–53.
Kargın S, Çakır M, Gündeş E, Yavuz Y, Esen HH, İyisoy MS, Kökbudak N, Küçükkartallar T. Relationship of preoperative neutrophil lymphocyte ratio with prognosis in gastrointestinal stromal tumors. Ulus Cerrahi Derg. 2015;31(2):61–4.
Goh BKP, Chok A-Y, Allen JC Jr, Quek R, Teo MCC, Chow PKH, Chung AYF, Ong H-S, Wong W-K. Blood neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios are independent prognostic factors for surgically resected gastrointestinal stromal tumors. Surgery. 2016;159(4):1146–56.
Stotz M, Liegl-Atzwanger B, Posch F, Mrsic E, Thalhammer M, Stojakovic T, Bezan A, Pichler M, Gerger A, Szkandera J. Blood-based biomarkers are associated with disease recurrence and survival in gastrointestinal stroma tumor patients after surgical resection. PLoS ONE. 2016;11(7): e0159448.
Jiang C, Hu W-M, Liao F-X, Yang Q, Chen P, Rong Y-M, Guo G-F, Yin C-X, Zhang B, He W-Z, Xia L-P. Elevated preoperative neutrophil-to-lymphocyte ratio is associated with poor prognosis in gastrointestinal stromal tumor patients. Onco Targets Ther. 2016;9:877–83.
Feng F, Tian Y, Liu S, Zheng G, Liu Z, Xu G, Guo M, Lian X, Fan D, Zhang H. Combination of PLR, MLR, MWR, and tumor size could significantly increase the prognostic value for gastrointestinal stromal tumors. Medicine (Baltimore). 2016;95(14): e3248.
Yin X, Tang S, Yin Y, Shen C, Zhang B, Chen Z. Associations of preoperative platelet-to-lymphocyte ratio and derived neutrophil-to-lymphocyte ratio with the prognosis of gastrointestinal stromal tumor (in Chinese). J Sichuan Univ (Med Sci Edi). 2017;48(2):239–43.
Xue A, Gao X, Fang Y, Shu P, Ling J, Shen K, Sun Y, Qin J, Qin X, Hou Y. Incorporation of NLR into NIH stratification system increases predictive accuracy for surgically resected gastrointestinal stromal tumors. Acta Biochim Biophys Sin (Shanghai). 2017;49(2):179–85.
Luo X, Zhou L. Prognostic significance of neutrophil to lymphocyte ratio in patients with gastrointestinal stromal tumors: A meta-analysis. Clin Chim Acta. 2018;2018(477):7–12.
Hu G, Li W, Shao G, Zhang X. Predictive effect of preoperative platelet-lymphocyte ratio on prognosis of patients with gastric stromal tumor (in Chinese). Cancer Res Prev Treat. 2018;45(7):479–82.
Rutkowski P, Teterycz P, Klimczak A, Bylina E, Szamotulska K, Lugowska I. Blood neutrophil-to-lymphocyte ratio is associated with prognosis in advanced gastrointestinal stromal tumors treated with imatinib. Tumori. 2018;104(6):415–22.
Liu Q, Ma J, Zhou L. The preoperative platelet-to-lymphocyte ratio predicts clinical outcomes in patients with gastrointestinal stromal tumors: a meta-analysis. Int J Clin Exp Med. 2018;11(4):3051–9.
Zhang Q, Xu L. Prognostic significance of preoperative neutrophil to lymphocyte ratio in patients with gastrointestinal stromal tumors: a meta-analysis (in Chinese). Chin J Immunol. 2019;35(1):84–7.
Yilmaz A, Mirili C, Bilici M, Tekin SB. A novel predictor in patients with gastrointestinal stromal tumors: Systemic immune-inflammation index (SII). J BUON. 2019;24(5):2127–35.
Sun J, Mei Y, Zhu Q, Shou C, Tjhoi WEH, Yang W, Yu H, Zhang Q, Liu X, Yu J. Relationship of prognostic nutritional index with prognosis of gastrointestinal stromal tumors. J Cancer. 2019;10(12):2679–86.
Sobczuk P, Teterycz P, Lugowska I, Klimczak A, Bylina E, Czarnecka AM, Kosela-Paterczyk H, Osuch C, Streb J, Rutkowski P. Prognostic value of the pretreatment neutrophil-to-lymphocyte ratio in patients with advanced gastrointestinal stromal tumors treated with sunitinib after imatinib failure. Oncol Lett. 2019;18(3):3373–80.
Yang J, Gu Y, Huang X, Xu J, Zhang Y, Yang X, Tian H, Zhan W. Prognostic impact of preoperative neutrophil-lymphocyte ratio for surgically resected gastrointestinal stromal tumors. Medicine (Baltimore). 2019;98(16): e15319.
Shi W-K, Zhang X-H, Zhang J, Yu M, Yuan Y-J, Xiong W, Zhang C-H, He Y-L, Wei Z-W. Predictive ability of prognostic nutritional index in surgically resected gastrointestinal stromal tumors: a propensity score matching analysis. Jpn J Clin Oncol. 2019;49(9):823–31.
Sun H, Sun Y. Predictive value of neutrophil lymphocyte ratio and plasma fibrinogen in the prognosis of patients with gastrointestinal stromal tumors (in Chinese). J Clin Surg. 2020;28(10):951–4.
Wei Z, Huang W, Yang D, Yuan Y, He Y, Zhang C. The prognostic roles of platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio in gastrointestinal stromal tumours: a meta-analysis. Transl Cancer Res. 2020;9(9):5128–38.
Catal O, Ozer B, Sit M, Ozer SP. The role of lymphocyte-monocyte ratio and platelet to lymphocyte ratio in predicting risk groups in gastrointestinal stromal tumors. Exp Biomed Res. 2020;3(4):255–61.
Lin Y, Wang M, Jia J, Wan W, Wang T, Yang W, Li C, Chen X, Cao H, Zhang P, Tao K. Development and validation of a prognostic nomogram to predict recurrence in high-risk gastrointestinal stromal tumour: a retrospective analysis of two independent cohorts. EBioMedicine. 2020;2020(60): 103016.
Li R, Sun Z, Song S, He X, Shi X, Li Z, Song J. NARFIB: a novel prognostic score based on the neutrophil-to-albumin ratio and fibrinogen can predict the prognosis of gastrointestinal stromal tumors. Cancer Manag Res. 2020;12:11183–90.
Chang W, Yang W, Zeng X, Li C, Xiong Z, Wang T, Zhang R, Tao K, Zhang P. Elevated preoperative platelet-to-lymphocyte ratio predicts poor prognosis of patients with primary gastrointestinal stromal tumor. BMC Gastroenterol. 2020;20:124.
Guo Y, Liu J, Zhang W, Xiao S, Zheng G, Liu S, Guo M, Zhang H, Feng F. Prognostic value of fibrinogen and lymphocyte count in intermediate and high risk gastrointestinal stromal tumors. Cancer Manag Res. 2020;12:8149–57.
Yan L, Cao Y, Deng S, Gu J, Mao F, Xue Y, Li H, Liu X. The Value of Preoperative Blood Neutrophil-Lymphocyte, White Blood Cell-Lymphocyte, Monocyte-Lymphocyte, and Platelet-Lymphocyte Ratios in Predicting the Malignant Potential of Gastrointestinal Stromal Tumor: A Retrospective Study. Res Sq. Preprint published 5 April 2021. https://doi.org/10.21203/rs.3.rs-386992/v1.
Li S, Chen D, Li S, Zhao Z, Yang H, Wang D, Zhang Z, Fu W. Novel prognostic nomogram for recurrence-free survival of patients with primary gastrointestinal stromal tumors after surgical resection: combination of prognostic nutritional index and basic variables. Front Oncol. 2021;10: 581855.
Lu Z, Li R, Cao X, Liu C, Sun Z, Shi X, Shao W, Zheng Y, Song J. Assessment of systemic inflammation and nutritional indicators in predicting recurrence-free survival after surgical resection of gastrointestinal stromal tumors. Front Oncol. 2021;11: 710191.
Zhao Z, Yin X-N, Wang J, Chen X, Cai Z-L, Zhang B. Prognostic significance of hemoglobin, albumin, lymphocyte, platelet in gastrointestinal stromal tumors: A propensity matched retrospective cohort study. World J Gastroenterol. 2022;28(27):3476–87.
Li Z, Zhang D, Mo C, Zhu P, Fan X, Tang T. The prognostic significance of prognostic nutritional index in gastrointestinal stromal tumors: a systematic review and meta-analysis. Medicine (Baltimore). 2022;101(47): e32067.
Yang W, Shou C, Yu J, Wang X, Zhang Q, Yu H, Lin X. Elevated preoperative controlling nutritional status (CONUT) scores as a predictor of postoperative recurrence in gastrointestinal stromal tumors. J Surg Oncol. 2022;126(7):1191–8.
Ding PA, Wu J, Wu H, Sun C, Guo H, Lowe S, Yang P, Tian Y, Liu Y, Meng L, Zhao Q. Inflammation and nutritional status indicators as prognostic indicators for patients with locally advanced gastrointestinal stromal tumors treated with neoadjuvant imatinib. BMC Gastroenterol. 2023;23(1):23.
Gay LJ, Felding-Habermann B. Contribution of platelets to tumour metastasis. Nat Rev Cancer. 2011;11(2):123–34.
Haemmerle M, Stone RL, Menter DG, Afshar-Kharghan V, Sood AK. The platelet lifeline to cancer: challenges and opportunities. Cancer Cell. 2018;33(6):965–83.
Labelle M, Begum S, Hynes RO. Platelets guide the formation of early metastatic niches. Proc Natl Acad Sci U S A. 2014;111(30):E3053–61.
Kolaczkowska E, Kubes P. Neutrophil recruitment and function in health and inflammation. Nat Rev Immunol. 2013;13(3):159–75.
Tan KW, Chong SZ, Wong FHS, Evrard M, Tan SML, Keeble J, Kemeny DM, Ng LG, Abastado J-P, Angeli V. Neutrophils contribute to inflammatory lymphangiogenesis by increasing VEGF-A bioavailability and secreting VEGF-D. Blood. 2013;122(22):3666–77.
Shojaei F, Singh M, Thompson JD, Ferrara N. Role of Bv8 in neutrophil-dependent angiogenesis in a transgenic model of cancer progression. Proc Natl Acad Sci U S A. 2008;105(7):2640–5.
Bausch D, Pausch T, Krauss T, Hopt UT, Fernandez-del-Castillo C, Warshaw AL, Thayer SP, Keck T. Neutrophil granulocyte derived MMP-9 is a VEGF independent functional component of the angiogenic switch in pancreatic ductal adenocarcinoma. Angiogenesis. 2011;14(3):235–43.
Shamamian P, Schwartz JD, Pocock BJ, Monea S, Whiting D, Marcus SG, Mignatti P. Activation of progelatinase A (MMP-2) by neutrophil elastase, cathepsin G, and proteinase-3: a role for inflammatory cells in tumor invasion and angiogenesis. J Cell Physiol. 2001;189(2):197–206.
McCourt M, Wang JH, Sookhai S, Redmond HP. Activated human neutrophils release hepatocyte growth factor/scatter factor. Eur J Surg Oncol. 2001;27(4):396–403.
Jabłońska E, Kiluk M, Markiewicz W, Piotrowski L, Grabowska Z, Jabłoński J. TNF-alpha, IL-6 and their soluble receptor serum levels and secretion by neutrophils in cancer patients. Arch Immunol Ther Exp (Warsz). 2001;49(1):63–9.
Schaider H, Oka M, Bogenrieder T, Nesbit M, Satyamoorthy K, Berking C, Matsushima K, Herlyn M. Differential response of primary and metastatic melanomas to neutrophils attracted by IL-8. Int J Cancer. 2003;103(3):335–43.
Spiegel A, Brooks MW, Houshyar S, Reinhardt F, Ardolino M, Fessler E, Chen MB, Krall JA, DeCock J, Zervantonakis IK, Iannello A, Iwamoto Y, Cortez-Retamozo V, Kamm RD, Pittet MJ, Raulet DH, Weinberg RA. Neutrophils suppress intraluminal NK cell-mediated tumor cell clearance and enhance extravasation of disseminated carcinoma cells. Cancer Discov. 2016;6(6):630–49.
Zhang X, Xu W. Neutrophils diminish T-cell immunity to foster gastric cancer progression: the role of GM-CSF/PD-L1/PD-1 signalling pathway. Gut. 2017;66(11):1878–80.
Coffelt SB, Wellenstein MD, Visser KEd. Neutrophils in cancer: neutral no more. Nat Rev Cancer. 2016;16(7):431–46.
Terzić J, Grivennikov S, Eliad Karin MK. Inflammation and colon cancer. Gastroenterology. 2010;138(6):2101–14.
Lee KH, Kim EY, Yun JS, Park YL, Do S-I, Chae SW, Park CH. The prognostic and predictive value of tumor-infiltrating lymphocytes and hematologic parameters in patients with breast cancer. Medicine (Baltimore). 2020;18(1):938.
Kitayama J, Yasuda K, Kawai K, Sunami E, Nagawa H. Circulating lymphocyte is an important determinant of the effectiveness of preoperative radiotherapy in advanced rectal cancer. BMC Cancer. 2011;11:64.
Cézé N, Thibault G, Goujon G, Viguier J, Watier H, Dorval E, Lecomte T. Pre-treatment lymphopenia as a prognostic biomarker in colorectal cancer patients receiving chemotherapy. Cancer Chemother Pharmacol. 2011;68(5):1305–13.
Herlea V, Rosulescu A, Iorgescu A, Dima SO, Dumitrascu T, Brasoveanu V, Stroescu C, Vasilescu C, Popescu I. The immune response in gastrointestinal stromal tumors. J Cancer Res Immunooncol. 2020;6(3):1000125.
Balachandran VP, Cavnar MJ, Zeng S, Bamboat ZM, Ocuin LM, Obaid H, Sorenson EC, Popow R, Ariyan C, Rossi F, Besmer P, Guo T, Antonescu CR, Taguchi T, Yuan J, Wolchok JD, Allison JP, DeMatteo RP. Imatinib potentiates antitumor T cell responses in gastrointestinal stromal tumor through the inhibition of Ido. Nat Med. 2011;17(9):1094–100.
Rosulescu A, Costache M, Dumitru A, Sajin M. Expression of PD-L1 and immune cells in gastrointestinal stromal tumors. Arch Balkan Med Union. 2021;56(3):284–90.
Dongen Mv, Savage NDL, Jordanova ES, Bruijn IHB-d, Walburg KV, Ottenhoff THM, Hogendoorn PCW, Burg SHvd, Gelderblom H, Hall Tv. Anti-inflammatory M2 type macrophages characterize metastasized and tyrosine kinase inhibitor-treated gastrointestinal stromal tumors. Int J Cancer. 2010;127(4):899–909.
Sun X, Sun J, Yuan W, Gao X, Fu M, Xue A, Li H, Shu P, Fang Y, Hou Y, Shen K, Sun Y, Qin J, Qin X. Immune cell infiltration and the expression of PD-1 and PD-L1 in primary PDGFRA-mutant gastrointestinal stromal tumors. J Gastrointest Surg. 2020;25(8):2091–100.
Rusakiewicz S, Semeraro M, Sarabi M, Desbois M, Locher C, Mendez R, Vimond N, Concha A, Garrido F, Isambert N, Chaigneau L, Brun-Ly VL, Dubreuil P, Cremer I, Caignard A, Poirier-Colame V, Chaba K, Flament C, Halama N, Jager D, Eggermont A, Bonvalot S, Commo Fe, Terrier P, Opolon P, Emile J-F, Coindre J-M, Kroemer G, Chaput N, Cesne AL, Blay J-Y, Zitvogel L. Immune infiltrates are prognostic factors in localized gastrointestinal stromal tumors. Cancer Res. 2013;73(12):3499–510.
Cameron S, Haller F, Dudas J, Moriconi F, Gunawan B, Armbrust T, Langer C, Fuzesi L, Ramadori G. Immune cells in primary gastrointestinal stromal tumors. Eur J Gastroenterol Hepatol. 2008;20(4):327–34.
Cameron S, Gieselmann M, Blaschke M, Ramadori G, Füzesi L. Immune cells in primary and metastatic gastrointestinal stromal tumors (GIST). Int J Clin Exp Pathol. 2014;7(7):3563–79.
Pantaleo MA, Tarantino G, Agostinelli C, Urbini M, Nannini M, Saponara M, Castelli C, Stacchiotti S, Fumagalli E, Gatto L, Santini D, Leo AD, Marafioti T, Akarca A, Sabattini E, Pession A, Ardizzoni A, Indio V, Astolfi A. Immune microenvironment profiling of gastrointestinal stromal tumors (GIST) shows gene expression patterns associated to immune checkpoint inhibitors response. Oncoimmunology. 2019;8(9): e1617588.
Sun X, Shu P, Fang Y, Yuan W, Zhang Q, Sun J, Fu M, Xue A, Gao X, Shen K, Hou Y, Sun Y, Qin J, Qin X. Clinical and prognostic significance of tumor-infiltrating CD8+ T cells and PD-L1 expression in primary gastrointestinal stromal tumors. Front Oncol. 2021;11: 789915.
Gasparotto D, Sbaraglia M, Rossi S, Baldazzi D, Brenca M, Mondello A, Nardi F, Racanelli D, Cacciatore M, Tos APD, Maestro R. Tumor genotype, location, and malignant potential shape the immunogenicity of primary untreated gastrointestinal stromal tumors. JCI Insight. 2020;5(22): e142560.
Herlea V, Roșulescu A, Calotă VC, Croitoru V, Mustafa ES, Vasilescu C, Alexandrescu S, Dumitrașcu T, Popescu I, Dima SO, Sajin M. Combined positive score for programmed death ligand-1 expression and inflammatory microenvironment in gastrointestinal stromal tumors. Medicina (Kaunas). 2022;58(2):174.
Esmail RSEN, Nada YW, Kamal A, ElSayed H, El-Anwer NM. Immunohistochemical characterization of immune cell infiltrate in gastrointestinal stromal tumor and its prognostic correlation. Egypt J Pathol. 2020;40(2):229–36.
Dancsok AR, Gao D, Lee AF, Steigen SE, Blay J-Y, Thomas DM, Maki RG, Nielsen TO, Demicco EG. Tumor-associated macrophages and macrophage-related immune checkpoint expression in sarcomas. Oncoimmunology. 2020;9(1):1747340.
Komita H, Koido S, Hayashi K, Kan S, Ito M, Kamata Y, Suzuki M, Homma S. Expression of immune checkpoint molecules of T cell immunoglobulin and mucin protein 3/galectin-9 for NK cell suppression in human gastrointestinal stromal tumors. Oncol Rep. 2015;34(4):2099–105.
Wei Z, Wu J, Huang W, Li J, Lu X, Yuan Y, Xiong W, Zhang X, Wang W, He Y, Zhang C. Immune-infiltration based signature as a novel prognostic biomarker in gastrointestinal stromal tumour. EBioMedicine. 2020;57: 102850.
Tan Y, Garcia-Buitrago MT, Trent JC, Rosenberg AE. The immune system and gastrointestinal stromal tumor: a wealth of opportunities. Curr Opin Oncol. 2015;27(4):338–42.
Bai C, Xu Y, Qiu C. A New Monoclonal Antibody that Blocks KIT Dimerisation and Inhibits Gastrointestinal Stromal Tumour Growth. Res Sq. Preprint published 05 August 2020. https://doi.org/10.21203/rs.3.rs-48780/v1.
Vitiello GA, Bowler TG, Liu M, Medina BD, Zhang JQ, Param NJ, Loo JK, Goldfeder RL, Chibon F, Rossi F, Zeng S, DeMatteo RP. Differential immune profiles distinguish the mutational subtypes of gastrointestinal stromal tumor. J Clin Invest. 2019;129(5):1863–77.
Tan Y, Trent J, Wilky B, Kerr D, Rosenberg A. Current status of immunotherapy for gastrointestinal stromal tumor. Cancer Gene Ther. 2017;24(3):130–3.
Arshad J, Costa PA, Barreto-Coelho P, Valdes BN, Trent JC. Immunotherapy strategies for gastrointestinal stromal tumor. Cancers (Basel). 2021;13:3525.
Etherington M, Hanna A, Liu M, Medina B, Do K, Levin L, Rossi F, DeMatteo R. Imatinib activates gamma delta T (ydT) cells in Gastrointestinal Stromal Tumor (GIST). J Am Coll Surg. 2020;231(4S1):S268–9.
Cavnar MJ, Zeng S, Kim TS, Sorenson EC, Ocuin LM, Balachandran VP, Seifert AM, Greer JB, Popow R, Crawley MH, Cohen NA, Green BL, Rossi F, Besmer P, Antonescu CR, DeMatteo RP. KIT oncogene inhibition drives intratumoral macrophage M2 polarization. J Exp Med. 2013;210(13):2873–86.
Cai H, Chen Y, Chen X, Sun W, Li Y. Tumor-associated macrophages mediate gastrointestinal stromal tumor cell metastasis through CXCL2/CXCR2. Cell Immunol. 2023;384: 104642.
Yi M, Zhao R, Wan Q, Wu X, Zhuang W, Wu C, Xia L, Chen Y, Zhou Y, Chen Z. Development of a Novel Immune-Based Prognostic Nomogram for Localized Primary Gastrointestinal Stromal Tumors after complete surgery. SSRN. Preprint published 05 October 2020. https://doi.org/10.2139/ssrn.3692429.
Yi M, Zhao R, Wan Q, Wu X, Zhuang W, Yang H, Wu C, Xia L, Chen Y, Zhou Y. Tumor-infiltrating immune cells signature predicts recurrence free survival after complete resection of localized primary gastrointestinal stromal tumors. medRxiv. Preprint published 29 February 2020. https://doi.org/10.1101/2020.02.28.20025908.
Guo X, Li Y, Wan B, Lv Y, Wang X, Liu G, Wang P. ETV1 inhibition depressed M2 polarization of tumor-associated macrophage and cell process in gastrointestinal stromal tumor via down-regulating PDE3A. J Clin Biochem Nutr. 2023;72:1–8.
Li H, Meng QH, Noh H, Somaiah N, Torres KE, Xia X, Batth IS, Joseph CP, Mulder ZA, Wang R, Li S. Abstract 1107: Cell-surface vimentin-positive macrophages like CTCs as novel biomarkers of metastatic gastrointestinal stromal tumors. Cancer Res. 2018;78(13_Suppl):1107.
Li H, Meng QH, Noh H, Somaiah N, Torres KE, Xia X, Batth IS, Joseph CP, Liu M, Wang R, Li S. Cell-surface vimentin-positive macrophage-like circulating tumor cells as a novel biomarker of metastatic gastrointestinal stromal tumors. Oncoimmunology. 2018;7(5): e1420450.
D’Angelo SP, Shoushtari AN, Agaram NP, Kuk D, Qin L-X, Carvajal RD, Dickson MA, Gounder M, Keohan ML, Schwartz GK, Tap WD. Prevalence of tumor-infiltrating lymphocytes and PD-L1 expression in the soft tissue sarcoma microenvironment. Hum Pathol. 2014;46(3):357–65.
Blakely AM, Matoso A, Patil PA, Taliano R, Machan JT, Miner TJ, Lombardo KA, Resnick MB, Wang L-J. Role of immune microenvironment in gastrointestinal stromal tumours. Histopathology. 2018;72(3):405–13.
Tian G, Xu W, Sun Y, Wang J, Ke Q, Yuan M, Wang J-J, Zhuang C, Gong Q. BDNF expression in GISTs predicts poor prognosis when associated with PD-L1 positive tumor-infiltrating lymphocytes. Oncoimmunology. 2021;1020:03956.
Tumeh PC, Harview CL, Yearley JH, Shintaku IP, Taylor EJM, Robert L, Chmielowski B, Spasic M, Henry G, Ciobanu V, West AN, Carmona M, Kivork C, Seja E, Cherry G, Gutierrez A, Grogan TR, Mateus C, Tomasic G, Glaspy JA, Emerson RO, Robins H, Pierce RH, Elashoff DA, Robert C, Ribas A. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature. 2014;515(7528):568–71.
Klaver Y, Rijnders M, Oostvogels A, Wijers R, Smid M, Grünhagen D, Verhoef C, Sleijfer S, Lamers C, Debets R. Differential quantities of immune checkpoint-expressing CD8 T cells in soft tissue sarcoma subtypes. J Immunother Cancer. 2020;8(2): e000271.
Zhuang C, Ni B, Zhang Z-Z, Zhao W-Y, Tu L, Ma X-L, Yang L-X, Cao H, Wang M. Low distribution of TIM-3+ cytotoxic tumor-infiltrating lymphocytes predicts poor outcomes in gastrointestinal stromal tumors. J Immunol Res. 2021;2021:6647292.
Wang M, Ni B, Zhuang C, Zhao W-Y, Tu L, Ma X-L, Yang L-X, Zhang Z-G, Cao H. Aberrant accumulation of Dickkopf 4 promotes tumor progression via forming the immune suppressive microenvironment in gastrointestinal stromal tumor. Cancer Med. 2019;8(11):5352–66.
Tanaka A, Sakaguchi S. Regulatory T cells in cancer immunotherapy. Cell Res. 2017;27(1):109–18.
Jordanova ES, Gorter A, Ayachi O, Prins F, Durrant LG, Kenter GG, Burg SHvd, Fleuren GJ. Human leukocyte antigen class I, MHC class I chain-related molecule A, and CD8+/regulatory T-cell ratio: which variable determines survival of cervical cancer patients? Clin Cancer Res. 2008;14(7):2028–35.
Desbois M, Rusakiewicz S, Locher C, Zitvogel L, Chaput N. Natural killer cells in non-hematopoietic malignancies. Front Immunol. 2012;3:395.
Rusakiewicz S, Perier A, Semeraro M, Pitt JM, Strandmann EPv, Reiners KS, Aspeslagh S, Pipéroglou C, Vély F, Ivagnes A, Jegou S, Halama N, Chaigneau L, Validire P, Christidis C, Perniceni T, Landi B, Berger A, Isambert N, Domont J, Bonvalot S, Terrier P, Adam J, Coindre J-M, Emile J-F, Poirier-Colame V, Chaba K, Rocha B, Caignard A, Toubert A, Enot D, Koch J, Marabelle A, Lambert M, Caillat-Zucman S, Leyvraz S, Auclair C, Vivier E, Eggermont A, Borg C, Blay JY, Cesne AL, Mir O, Zitvogel L. NKp30 isoforms and NKp30 ligands are predictive biomarkers of response to imatinib mesylate in metastatic GIST patients. Oncoimmunology. 2017;6(1):e1137418.
Delahaye NF, Rusakiewicz S, Martins I, Ménard Cd, Roux S, Lyonnet L, Paul P, Sarabi M, Chaput N, Semeraro M, Minard-Colin Vr, Poirier-Colame V, Chaba K, Flament C, Baud VR, Authier Hln, Kerdine-Römer S, Pallardy M, Cremer I, Peaudecerf L, Rocha Bnd, Valteau-Couanet D, Gutierrez JC, Nunès JA, Commo FDR, Bonvalot S, Ibrahim N, Terrier P, Opolon P, Bottino C, Moretta A, Tavernier J, Rihet P, Coindre J-M, Blay J-Y, Isambert N, Emile J-FO, Vivier E, Lecesne A, Kroemer G, Zitvogel L. Alternatively spliced NKp30 isoforms affect the prognosis of gastrointestinal stromal tumors. Nat Med. 2011;17(6):700–7.
Chaput N, Flament C, Locher C, Desbois M, Rey A, Rusakiewicz S, Poirier-Colame V, Pautier P, Cesne AL, Soria J-C, Paci A, Rosenzwajg M, Klatzmann D, Eggermont A, Robert C, Zitvogel L. Phase I clinical trial combining imatinib mesylate and IL-2: HLA-DR + NK cell levels correlate with disease outcome. Oncoimmunology. 2013;2(2): e23080.
Ménard C, Blay J-Y, Borg C, Michiels S, Ghiringhelli F, Robert C, Nonn C, Chaput N, Taïeb J, Delahaye NF, Flament C, Emile J-F, Cesne AL, Zitvogel L. Natural killer cell IFN-gamma levels predict long-term survival with imatinib mesylate therapy in gastrointestinal stromal tumor-bearing patients. Cancer Res. 2009;69(8):3563–9.
Aboud M, Kingsmore S, Segal S. Role of natural killer cells in controlling local tumor formation and metastatic manifestation of different 3LL Lewis lung carcinoma cell clones. Nat Immun. 1993;12(1):17–24.
Fend L, Rusakiewicz S, Adam J, Bastien B, Caignard A, Messaoudene M, Iribarren C, Cremer I, Marabelle A, Borg C, Semeraro M, Barraud L, Limacher J-M, Eggermont A, Kroemer G, Zitvogel L. Prognostic impact of the expression of NCR1 and NCR3 NK cell receptors and PD-L1 on advanced non-small cell lung cancer. Oncoimmunology. 2016;6(1): e1163456.
Zitvogel L, Rusakiewicz S, Routy B, Ayyoub M, Kroemer G. Immunological off-target effects of imatinib. Nat Rev Clin Oncol. 2016;13(7):431–46.
Ivagnès A, Messaoudene M, Stoll G, Routy B, Fluckiger A, Yamazaki T, Iribarren K, Duong CPM, Fend L, Caignard A, Cremer I, LeCesne A, Adam J, Honoré C, Mir O, Chaigneau L, Berger A, Validire P, Christidis C, Brun-Ly VL, Smyth MJ, Mariette X, Salomon BL, Kroemer G, Rusakiewicz S, Zitvogel L. TNFR2/BIRC3-TRAF1 signaling pathway as a novel NK cell immune checkpoint in cancer. Oncoimmunology. 2018;7(12): e1386826.
Ghiringhelli F, Ménard C, Terme M, Flament C, Taieb J, Chaput N, Puig PE, Novault S, Escudier B, Vivier E, Lecesne A, Robert C, Blay J-Y, Bernard J, Caillat-Zucman S, Freitas A, Tursz T, Wagner-Ballon O, Capron C, Vainchencker W, Martin F, Zitvogel L. CD4+CD25+ regulatory T cells inhibit natural killer cell functions in a transforming growth factor-beta-dependent manner. J Exp Med. 2005;202(8):1075–85.
Garaud S, Dieu-Nosjean M-C, Willard-Gallo K. T follicular helper and B cell crosstalk in tertiary lymphoid structures and cancer immunotherapy. Nat Commun. 2022;13(1):2259.
Lin Q, Tao P, Wang J, Ma L, Jiang Q, Li J, Zhang G, Liu J, Zhang Y, Hou Y, Lu W, Xue R, Tong H. Tumor-associated tertiary lymphoid structure predicts postoperative outcomes in patients with primary gastrointestinal stromal tumors. Oncoimmunology. 2020;9(1):1747339.
Westrich JA, Vermeer DW, Colbert PL, Spanos WC, Pyeon D. The multifarious roles of the chemokine CXCL14 in cancer progression and immune responses. Mol Carcinog. 2020;59(7):794–806.
Mu J, Sun P, Ma Z, Sun P. BRD4 promotes tumor progression and NF-κB/CCL2-dependent tumor-associated macrophage recruitment in GIST. Cell Death Dis. 2019;10(12):935.
Lasota J, Dansonka-Mieszkowska A, Sobin LH, Miettinen M. A great majority of GISTs with PDGFRA mutations represent gastric tumors of low or no malignant potential. Lab Invest. 2004;84(7):874–83.
Wozniak A, Rutkowski P, Schöffski P, Ray-Coquard I, Hostein I, Schildhaus H-U, Cesne AL, Bylina E, Limon J, Blay J-Y, Siedlecki JA, Wardelmann E, Sciot R, Coindre J-M, Debiec-Rychter M. Tumor genotype is an independent prognostic factor in primary gastrointestinal stromal tumors of gastric origin: a european multicenter analysis based on ConticaGIST. Clin Cancer Res. 2014;20(23):6105–5116.
Rossi S, Gasparotto D, Miceli R, Toffolatti L, Gallina G, Scaramel E, Marzotto A, Boscato E, Messerini L, Bearzi I, Mazzoleni G, Capella C, Arrigoni G, Sonzogni A, Sidoni A, Mariani L, Amore P, Gronchi A, Casali PG, Maestro R, Tos APD. KIT, PDGFRA, and BRAF mutational spectrum impacts on the natural history of imatinib-naive localized GIST: a population-based study. Am J Surg Pathol. 2015;39(7):922–30.
Indio V, Ravegnini G, Astolfi A, Urbini M, Saponara M, Leo AD, Gruppioni E, Tarantino G, Angelini S, Pession A, Pantaleo MA, Nannini M. Gene expression profiling of PDGFRA mutant GIST reveals immune signatures as a specific fingerprint of D842V exon 18 mutation. Front Immunol. 2020;11:851.
Indio V, Astolfi A, Tarantino G, Urbini M, Patterson J, Nannini M, Saponara M, Gatto L, Santini D, Valle IFd, Castellani G, Remondini D, Fiorentino M, Mehren Mv, Brandi G, Biasco G, Heinrich MC, Pantaleo MA. Integrated molecular characterization of Gastrointestinal Stromal Tumors (GIST) harboring the rare D842V mutation in PDGFRA gene. Int J Mol Sci. 2018;19(3):732.
Indio V, Astolf A, Urbini M, Nannini M, Pantaleo MA. Genetics and treatment of gastrointestinal stromal tumors with immune checkpoint inhibitors: what do we know? Pharmacogenomics. 2020;21(4):231–4.
Bertucci F, Finetti P, Mamessier E, Pantaleo MA, Astolfi A, Ostrowski J, Birnbaum D. PDL1 expression is an independent prognostic factor in localized GIST. Oncoimmunology. 2015;4(5): e1002729.
Zhao R, Song Y, Wang Y, Huang Y, Li Z, Cui Y, Yi M, Xia L, Zhuang W, Wu X, Zhou Y. PD-1/PD-L1 blockade rescue exhausted CD8+ T cells in gastrointestinal stromal tumours via the PI3K/Akt/mTOR signalling pathway. Cell Prolif. 2019;52(3): e12571.
Hacking S, Wu D, Lee L, Vitkovski T, Nasim M. Nature and significance of stromal differentiation, PD-L1, and VISTA in GIST. Pathol Res Pract. 2022;229: 153703.
Hacking S, Wu D, Lee L, Vitkovski T, Chavarria H, Nasim M. Nature and Significance of Stromal Differentiation, PD-L1, and VISTA in GIST: Shifting Current Paradigms. Res Sq. Preprint published 02 March 2021. https://doi.org/10.21203/rs.3.rs-286338/v1.
Fanale D, Incorvaia L, Badalamenti G, Luca ID, Algeri L, Bonasera A, Corsini LR, Brando C, Russo A, Iovanna JL, Bazan V. Prognostic role of plasma PD-1, PD-L1, pan-BTN3As and BTN3A1 in patients affected by metastatic gastrointestinal stromal tumors: can immune checkpoints act as a sentinel for short-term survival? Cancers (Basel). 2021;13(9):2118.
Brando C, Fanale D, Incorvaia L, Algeri L, Barraco N, Corsini LR, Cucinella A, Dimino A, Filorizzo C, Fiorino A, Galvano A, Madonia G, Magrin L, Pedone E, Ricciardi MR, Sciacchitano R, Scalia R, Badalamenti G, Bazan V, Russo A. Correlation between circulating immune checkpoints and KIT mutations in metastatic gastrointestinal stromal tumors. Qeios. Preprint published 10 January 2022. https://doi.org/10.32388/0E2ZME.
Brando C, Fanale D, Incorvaia L, Algeri L, Barraco N, Corsini LR, Cucinella A, Dimino A, Filorizzo C, Fiorino A, Madonia G, Magrin L, Pedone E, Ricciardi MR, Sciacchitano R, Scalia R, Badalamenti G, Bazan V, Russo A. 32P Can circulating immune checkpoints and KIT exon 11 mutations be prognostic factors in metastatic gastrointestinal stromal tumors? Annals of Oncology. 2021;32(7_Suppl):1386.
Brinch CM, Hogdall E, Junker N, Moeller HJ, Sandfeld-Paulsen B, Heer PD, Penninga L, Rossen PB, Krarup-Hansen A, Aggerholm-Pedersen N. The prognostic value of plasma programmed death protein-1 (PD-1) and Programmed Death-Ligand 1 (PD-L1) in patients with gastrointestinal stromal tumor. Cancers (Basel). 2022;14(23):5753.
Munn DH, Mellor AL. Indoleamine 2,3-dioxygenase and tumor-induced tolerance. J Clin Invest. 2007;117(5):1147–54.
Schafer CC, Wang Y, Hough KP, Sawant A, Grant SC, Thannickal VJ, Zmijewski J, Ponnazhagan S, Deshane JS. Indoleamine 2,3-dioxygenase regulates anti-tumor immunity in lung cancer by metabolic reprogramming of immune cells in the tumor microenvironment. Oncotarget. 2016;7(46):75407–24.
Mezrich JD, Fechner JH, Zhang X, Johnson BP, Burlingham WJ, Bradfield CA. An interaction between kynurenine and the aryl hydrocarbon receptor can generate regulatory T cells. J Immunol. 2010;185(6):3190–8.
Munn DH, Mellor AL. IDO in the tumor microenvironment: inflammation, counter-regulation, and tolerance. Trends Immunol. 2016;37(3):193–207.
Ravishankar B, Liu H, Shinde R, Chandler P, Baban B, Tanaka M, Munn DH, Mellor AL, Karlsson MCI, McGaha TL. Tolerance to apoptotic cells is regulated by indoleamine 2,3-dioxygenase. Proc Natl Acad Sci U S A. 2012;109(10):3909–14.
Sharma MD, Baban B, Chandler P, Hou D-Y, Singh N, Yagita H, Azuma M, Blazar BR, Mellor AL, Munn DH. Plasmacytoid dendritic cells from mouse tumor-draining lymph nodes directly activate mature Tregs via indoleamine 2,3-dioxygenase. J Clin Invest. 2007;117(9):2570–82.
Dufresne A, Lesluyes T, Ménétrier-Caux C, Brahmi M, Darbo E, Toulmonde M, Italiano A, Mir O, Cesne AL, Guellec SL, Valentin T, Chevreau C, Bonvalot S, Robin YM, Coindre J-M, Caux C, Blay JY, Chibon F. Specific immune landscapes and immune checkpoint expressions in histotypes and molecular subtypes of sarcoma. Oncoimmunology. 2020;9(1):1792036.
Wu M-R, Zhang T, DeMars LR, Sentman CL. B7H6-specific chimeric antigen receptors lead to tumor elimination and host antitumor immunity. Gene Ther. 2015;22(8):675–84.
Perez D, Hauswirth F, Jäger D, Metzger U, Samartzis EP, Went P, Jungbluth A. Protein expression of cancer testis antigens predicts tumor recurrence and treatment response to imatinib in gastrointestinal stromal tumors. Int J Cancer. 2011;128(12):2947–52.
Perez D, Herrmann T, Jungbluth AA, Samartzis P, Spagnoli G, Demartines N, Clavien P-A, Marino S, Seifert B, Jaeger D. Cancer testis antigen expression in gastrointestinal stromal tumors: new markers for early recurrence. Int J Cancer. 2008;123(7):1551–5.
Ayyoub M, Taub RN, Keohan M-L, Hesdorffer M, Metthez G, Memeo L, Mansukhani M, Hibshoosh H, Hesdorffer CS, Valmori D. The frequent expression of cancer/testis antigens provides opportunities for immunotherapeutic targeting of sarcoma. Cancer Immun. 2004;4:7.
Ghadban T, Perez DR, Vashist YK, Bockhorn M, Koenig AM, Gammal ATE, Izbicki JR, Metzger U, Hauswirth F, Frosina D, Jungbluth AA. Expression of cancer testis antigens CT10 (MAGE-C2) and GAGE in gastrointestinal stromal tumors. Eur J Surg Oncol. 2014;40(10):1307–12.
Endo M, Graaff MAd, Ingram DR, Lim S, Lev DC, Bruijn IHB-d, Somaiah N, Bovée JVMG, Lazar AJ, Nielsen TO. NY-ESO-1 (CTAG1B) expression in mesenchymal tumors. Mod Pathol. 2015;28(4):587–95.
Lai J, Rosenberg AZ, Miettinen MM, Lee C-CR. NY-ESO-1 expression in sarcomas: A diagnostic marker and immunotherapy target. OncoImmunology. 2012;1(8):1409–10.
Ghiringhelli F, Ménard C, Martin F, Zitvogel L. The role of regulatory T cells in the control of natural killer cells: relevance during tumor progression. Immunol Rev. 2006;214:229–38.
Borg C, Terme M, Taïeb J, Ménard C, Flament C, Robert C, Maruyama K, Wakasugi H, Angevin E, Thielemans K, Cesne AL, Chung-Scott V, Lazar V, Tchou I, Crépineau F, Lemoine F, Bernard J, Fletcher JA, Turhan A, Blay J-Y, Spatz A, Emile J-F, Heinrich MC, Mécheri S, Tursz T, Zitvogel L. Novel mode of action of c-kit tyrosine kinase inhibitors leading to NK cell–dependent antitumor effects. J Clin Invest. 2004;114(3):379–88.
Shen C, Han L, Liu B, Zhang G, Cai Z, Yin X, Yin Y, Chen Z, Zhang B. The KDM6A-SPARCL1 axis blocks metastasis and regulates the tumour microenvironment of gastrointestinal stromal tumours by inhibiting the nuclear translocation of p65. Br J Cancer. 2022;126(10):1457–69.
Yoon H, Tang C-M, Banerjee S, Delgado AL, Yebra M, Davis J, Sicklick JK. TGF-β1-mediated transition of resident fibroblasts to cancer-associated fibroblasts promotes cancer metastasis in gastrointestinal stromal tumor. Oncogenesis. 2021;10(2):13.
Li H-L, Wang L-H, Hu Y-L, Feng Y, Li X-H, Liu Y-F, Li P, Mao Q-S, Xue W-J. Clinical and prognostic significance of CC chemokine receptor type 8 protein expression in gastrointestinal stromal tumors. World J Gastroenterol. 2020;26(31):4656–68.
Simone MD, Arrigoni A, Rossetti G, Gruarin P, Ranzani V, Politano C, Bonnal RJP, Provasi E, Sarnicola ML, Panzeri I, Moro M, Crosti M, Mazzara S, Vaira V, Bosari S, Palleschi A, Santambrogio L, Bovo G, Zucchini N, Totis M, Gianotti L, Cesana G, Perego RA, Maroni N, Ceretti AP, Opocher E, Francesco RD, Geginat J, Stunnenberg HG, Abrignani S, Pagani M. Transcriptional landscape of human tissue lymphocytes unveils uniqueness of tumor-infiltrating T regulatory cells. Immunity. 2016;45(5):1135–47.
Kidani Y, Nogami W, Yasumizu Y, Kawashima A, Tanaka A, Sonoda Y, Tona Y, Nashiki K, Matsumoto R, Hagiwara M, Osaki M, Dohi K, Kanazawa T, Ueyama A, Yoshikawa M, Yoshida T, Matsumoto M, Hojo K, Shinonome S, Yoshida H, Hirata M, Haruna M, Nakamura Y, Motooka D, Okuzaki D, Sugiyama Y, Kinoshita M, Okuno T, Kato T, Hatano K, Uemura M, Imamura R, Yokoi K, Tanemura A, Shintani Y, Kimura T, Nonomura N, Wada H, Mori M, Doki Y, Ohkura N, Sakaguchi S. CCR8-targeted specific depletion of clonally expanded Treg cells in tumor tissues evokes potent tumor immunity with long-lasting memory. Proc Natl Acad Sci U S A. 2022;119(7): e2114282119.
Villarreal DO, L’Huillier A, Armington S, Mottershead C, Filippova EV, Coder BD, Petit RG, Princiotta MF. Targeting CCR8 induces protective antitumor immunity and enhances vaccine-induced responses in colon cancer. Cancer Res. 2018;78(18):5340–8.
Damme HV, Dombrecht B, Kiss M, Roose H, Allen E, Overmeire EV, Kancheva D, Martens L, Murgaski A, Bardet PMR, Blancke G, Jans M, Bolli E, Martins MS, Elkrim Y, Dooley J, Boon L, Schwarze JK, Tacke F, Movahedi K, Vandamme N, Neyns B, Ocak S, Scheyltjens I, Vereecke L, Nana FA, Merchiers P, Laoui D, Ginderachter JAV. Therapeutic depletion of CCR8+ tumor-infiltrating regulatory T cells elicits antitumor immunity and synergizes with anti-PD-1 therapy. J Immunother Cancer. 2021;9(2): e001749.
Campbell JR, McDonald BR, Mesko PB, Siemers NO, Singh PB, Selby M, Sproul TW, Korman AJ, Vlach LM, Houser J, Sambanthamoorthy S, Lu K, Hatcher SV, Lohre J, Jain R, Lan RY. Fc-optimized anti-CCR8 antibody depletes regulatory T cells in human tumor models. Cancer Res. 2021;81(11):2983–94.
Wang T, Zhou Q, Zeng H, Zhang H, Liu Z, Shao J, Wang Z, Xiong Y, Wang J, Bai Q, Xia Y, Wang Y, Liu L, Zhu Y, Xu L, Dai B, Guo J, Chang Y, Wang X, Xu J. CCR8 blockade primes anti-tumor immunity through intratumoral regulatory T cells destabilization in muscle-invasive bladder cancer. Cancer Immunol Immunother. 2020;69(9):1855–67.
Haruna M, Ueyama A, Yamamoto Y, Hirata M, Goto K, Yoshida H, Higuchi N, Yoshida T, Kidani Y, Nakamura Y, Nagira M, Kawashima A, Iwahori K, Shintani Y, Ohkura N, Wada H. The impact of CCR8+ regulatory T cells on cytotoxic T cell function in human lung cancer. Sci Rep. 2022;12(1):5377.
Wang H-C, Li T-Y, Chao Y-J, Hou Y-C, Hsueh Y-S, Hsu K-H, Shan Y-S. KIT Exon 11 Codons 557–558 deletion mutation promotes liver metastasis through the CXCL12/CXCR4 axis in gastrointestinal stromal tumors. Clin Cancer Res. 2016;22(14):3477–87.
Ayers M, Lunceford J, Nebozhyn M, Murphy E, Loboda A, Kaufman DR, Albright A, Cheng JD, Kang SP, Shankaran V, Piha-Paul SA, Yearley J, Seiwert TY, Ribas A, McClanahan TK. IFN-γ–related mRNA profile predicts clinical response to PD-1 blockade. J Clin Invest. 2017;127(8):2930–40.
Danaher P, Warren S, Lu R, Samayoa J, Sullivan A, Pekker I, Wallden B, Marincola FM, Cesano A. Pan-cancer adaptive immune resistance as defined by the Tumor Inflammation Signature (TIS): results from The Cancer Genome Atlas (TCGA). J Immunother Cancer. 2018;6(1):63.
Petitprez F, Reyniès AD, Keung EZ, Chen TWW, Sun C-M, Calderaro J, Jeng Y-M, Hsiao L-P, Lacroix L, Bougoüin A, Moreira M, Lacroix G, Natario I, Adam J, Lucchesi C, Laizet YH, Toulmonde M, Burgess MA, Bolejack V, Reinke D, Wani KM, Wang W-L, Lazar AJ, Roland CL, Wargo JA, Italiano A, Sautès-Fridman C, Tawbi HA, Fridman WH. B cells are associated with survival and immunotherapy response in sarcoma. Nature. 2020;577(7791):556–60.
Bauer S, Corless CL, Heinrich MC, Dirsch O, Antoch G, Kanja J, Seeber S, Schütte J. Response to imatinib mesylate of a gastrointestinal stromal tumor with very low expression of KIT. Cancer Chemother Pharmacol. 2003;51(3):261–5.
Medina BD, Liu M, Vitiello GA, Seifert AM, Zeng S, Bowler T, Zhang JQ, Cavnar MJ, Loo JK, Param NJ, Maltbaek JH, Rossi F, Balachandran V, DeMatteo RP. Oncogenic kinase inhibition limits Batf3-dependent dendritic cell development and antitumor immunity. J Exp Med. 2019;216(6):1359–76.
Zitvogel L, Ghiringhelli F, Terme M, Borg C, Chaput N, Lecesne CM, Fletcher J, Heinrich MC, Tursz T, Taieb J. A novel mode of antitumor activity for imatinib mesylate: Consequences for the design of surrogate markers of efficacy and combination therapies. J Clin Oncol. 2005;23(16_suppl):2516.
Chen LL, Chen X, Choi H, Sang H, Chen LC, Zhang H, Gouw L, Andtbacka RH, Chan BK, Rodesch CK, Jimenez A, Cano P, Jones KA, Oyedeji CO, Martins T, Hill HR, Schumacher J, Willmore C, Scaife CL, Ward JH, Morton K, Randall RL, Lazar AJ, Patel S, Trent JC, Frazier ML, Lin P, Jensen P, Benjamin RS. Exploiting antitumor immunity to overcome relapse and improve remission duration. Cancer Immunol Immunother. 2012;61(7):1113–24.
Borg C, Jalil A, Laderach D, Maruyama K, Wakasugi H, Charrier S, Ryffel B, Cambi A, Figdor C, Vainchenker W, Galy A, Caignard A, Zitvogel L. NK cell activation by dendritic cells (DCs) requires the formation of a synapse leading to IL-12 polarization in DCs. Blood. 2004;104(10):3267–75.
Liu M, Etherington MS, Hanna A, Medina BD, Vitiello GA, Bowler TG, Param NJ, Levin L, Rossi F, DeMatteo RP. Oncogenic KIT modulates type I IFN-mediated antitumor immunity in GIST. Cancer Immunol Res. 2021;9(5):542–53.
Tieniber AD, Hanna AN, Medina BD, Vitiello GA, Etherington MS, Liu M, Do KJ, Rossi F, DeMatteo RP. Tyrosine kinase inhibition alters intratumoral CD8+ T-cell subtype composition and activity. Cancer Immunol Res. 2022;10(10):1210–23.
Tieniber A, Hanna A, Medina B, Do K, Levin L, Rossi F, DeMatteo R. Abstract P050: Oncogenic kinase therapy restricts CD8 T cell differentiation and clonal expansion. Cancer Immunol Res. 2022;10(1 Suppl):P050.
Pautier P, Locher C, Robert C, Deroussent A, Flament C, Cesne AL, Rey A, Bahleda R, Ribrag V, Soria J-C, Vassal G, Eggermont A, Zitvogel L, Chaput N, Paci A. Phase I clinical trial combining imatinib mesylate and IL-2 in refractory cancer patients: IL-2 interferes with the pharmacokinetics of imatinib mesylate. Oncoimmunology. 2013;2(2): e23079.
Zhang JQ, Zeng S, Vitiello GA, Seifert AM, Medina BD, Beckman MJ, Loo JK, Santamaria-Barria J, Maltbaek JH, Param NJ, Moral JA, Zhao JN, Balachandran V, Rossi F, Antonescu CR, DeMatteo RP. Macrophages and CD8+ T cells mediate the antitumor efficacy of combined CD40 ligation and imatinib therapy in gastrointestinal stromal tumors. Cancer Immunol Res. 2018;6(4):434–47.
ClinicalTrials.gov. Vaccine Therapy and Sargramostim in Treating Patients With Sarcoma or Brain Tumor. https://clinicaltrials.gov/ct2/show/NCT00069940 (2022, accessed 07 Oct 2022).
clinicaltrials.gov. Imatinib Mesylate With or Without Bevacizumab in Treating Patients With Metastatic or Unresectable Gastrointestinal Stromal Tumor (S0502). https://clinicaltrials.gov/ct2/show/NCT00324987 (2022, accessed 01 Oct 2022).
ClinicalTrials.gov. A Phase 1 Study of Mixed Bacteria Vaccine (MBV) in Patients With Tumors Expressing NY-ESO-1 Antigen. https://clinicaltrials.gov/ct2/show/NCT00623831 (2022, accessed 07 Oct 2022).
ClinicalTrials.gov. Study of Imatinib and Peginterferon α-2b in Gastrointestinal Stromal Tumor (GIST) Patients. https://clinicaltrials.gov/ct2/show/NCT00585221 (2022, accessed 06 Oct 2022).
clinicaltrials.gov. A Study of Olaratumab (IMC-3G3) in Previously Treated Participants With Unresectable and/or Metastatic Gastrointestinal Stromal Tumors. https://clinicaltrials.gov/ct2/show/NCT01316263 (2022, accessed 01 Oct 2022).
ClinicalTrials.gov. Ipilimumab and Imatinib Mesylate in Advanced Cancer, https://clinicaltrials.gov/ct2/show/record/NCT01738139 (2022, accessed 22 Sept 2022).
ClinicalTrials.gov. Dasatinib and Ipilimumab in Treating Patients With Gastrointestinal Stromal Tumors or Other Sarcomas That Cannot Be Removed by Surgery or Are Metastatic. https://clinicaltrials.gov/ct2/show/NCT01643278 (2022, accessed 03 Oct 2022).
ClinicalTrials.gov. A Combination Clinical Study of PLX3397 and Pembrolizumab To Treat Advanced Melanoma and Other Solid Tumors. https://clinicaltrials.gov/ct2/show/NCT02452424 (2022, accessed 25 Sept 2022).
ClinicalTrials.gov. Combination of MK3475 and Metronomic Cyclophosphamide in Patients With Advanced Sarcomas : Multicentre Phase II Trial (PEMBROSARC). https://clinicaltrials.gov/ct2/show/NCT02406781 (2022, accessed 25 Sept 2022).
ClinicalTrials.gov. Axitinib and Pembrolizumab in Subjects With Advanced Alveolar Soft Part Sarcoma and Other Soft Tissue Sarcomas. https://clinicaltrials.gov/ct2/show/NCT02636725 (2022, accessed 25 Sept 2022).
ClinicalTrials.gov. Nivolumab With or Without Ipilimumab in Treating Patients With Metastatic Sarcoma That Cannot Be Removed by Surgery. https://clinicaltrials.gov/ct2/show/NCT02500797 (2022, accessed 07 Oct 2022).
ClinicalTrials.gov. A Study to Evaluate the Safety of Intuvax Administered Intra-tumorally in Patients With Gastrointestinal Stromal Tumors (GIST). https://clinicaltrials.gov/ct2/show/record/NCT02686944 (2022, accessed 22 Sept 2022).
ClinicalTrials.gov. Nivolumab With or Without Ipilimumab in Treating Patients With Gastrointestinal Stromal Tumor That Is Metastatic or Cannot Be Removed by Surgery. https://clinicaltrials.gov/ct2/show/NCT02880020 (2022, accessed 25 Sept 2022).
ClinicalTrials.gov. Nivolumab and Ipilimumab in Treating Patients With Rare Tumors. https://clinicaltrials.gov/ct2/show/study/NCT02834013 (2022, accessed 22 Sept 2022).
ClinicalTrials.gov. Immunomodulating Nutrients in Perioperative Patients With Gastric Cancer. https://clinicaltrials.gov/ct2/show/NCT03123432 (2022, accessed 07 Oct 2022).
ClinicalTrials.gov. Epacadostat and Pembrolizumab in Patients With GIST. https://clinicaltrials.gov/ct2/show/NCT03291054 (2022, accessed 22 Sept 2022).
ClinicalTrials.gov. A Phase I/II Study of Regorafenib Plus Avelumab in Solid Tumors (REGOMUNE). https://clinicaltrials.gov/ct2/show/NCT03475953 (2022, accessed 01 Oct 2022).
ClinicalTrials.gov. A Study of XmAb®18087 in Subjects With NET and GIST. https://clinicaltrials.gov/ct2/show/study/NCT03411915 (2022, accessed 22 Sept 2022).
ClinicalTrials.gov. PDR001 Plus Imatinib for Metastatic or Unresectable GIST. https://clinicaltrials.gov/ct2/show/NCT03609424 (2022, accessed 22 Sept 2022).
ClinicalTrials.gov. Phase Ib Study of TNO155 in Combination With Spartalizumab or Ribociclib in Selected Malignancies. https://clinicaltrials.gov/ct2/show/NCT04000529 (2022, accessed 01 Oct 2022).
ClinicalTrials.gov. DS-6157a in Participants With Advanced Gastrointestinal Stromal Tumor (GIST). https://clinicaltrials.gov/ct2/show/results/NCT04276415 (2022, accessed 25 Sept 2022).
ClinicalTrials.gov. A Study of Avelumab In Combination With Axitinib in Patients With Unresectable/Metastatic Gastrointestinal Stromal Tumor After Failure of Standard Therapy (AXAGIST). https://clinicaltrials.gov/ct2/show/NCT04258956 (2022, accessed 01 Oct 2022).
ClinicalTrials.gov. DNX-2440 for Resectable Colorectal Liver Metastasis. https://clinicaltrials.gov/ct2/show/NCT04714983 (2022, accessed 07 Oct 2022.
ClinicalTrials.gov. A Prospective, Randomized, Multicenter, Comparative Study of the Efficacy of Imatinib Resumption Combined With Atezolizumab Versus Imatinib Resumption Alone in Patients With Unresectable Advanced Gastrointestinal Stromal Tumors (GIST) After Failure of Standard Treatments (ATEZOGIST). https://clinicaltrials.gov/ct2/show/NCT05152472 (2022, accessed 07 Oct 2022).
Ivashkiv LB, Donlin LT. Regulation of type I interferon responses. Nat Rev Immunol. 2014;14(1):36–49.
Chen LL, Chen X, Gouw LG, Andtbacka RI, Jones KA, Randall JHW, Trent JC, Patel S, Benjamin RS. Combination of targeted therapy (imatinib) with immunotherapy (peginterferon α-2b) to overcome drug resistance and tumor stem cells in gastrointestinal stromal tumors (GIST). J Clin Oncol. 2010;28(15_suppl):10035.
Chen LL, Gouw L, Sabripour M, Hwu W-J, Benjamin RS. Combining targeted therapy with immunotherapy (interferon-α). Rational, efficacy in gastrointestinal stromal tumor model and implications in other malignancies. Oncoimmunology. 2012;1(5):773–6.
Zhang L, Huang J, Pi Z, Yu M. Inhibition effect of Peg-IFNα-2b and Imatinib alone or combination on imatinib-resistant gastrointestinal stromal tumors cell lines. Int J Clin Exp Pathol. 2015;8(9):11340–7.
Shoushtari AN, D’Angelo SP, Keohan ML, Dickson MA, Gounder MM, Erinjeri AKAP, Bluth MJ, Ustoyev Y, Condy MM, Streicher H, Takebe N, DeMatteo RP, Schwartz GK, Tap WD, Carvajal RD. Combined KIT and CTLA-4 blockade in patients with refractory GIST and other advanced sarcomas. J Clin Oncol. 2014;32(15):10521.
D’Angelo SP, Shoushtari AN, Keohan ML, Dickson MA, Gounder MM, Chi P, Loo JK, Gaffney L, Schneider L, Patel Z, Erinjeri JP, Bluth MJ, Sjoberg A, Streicher H, Takebe N, Qin L-X, Antonescu C, DeMatteo RP, Carvajal RD, Tap WD. Combined KIT and CTLA-4 blockade in patients with refractory GIST and other advanced sarcomas: a phase Ib study of Dasatinib plus Ipilimumab. Clin Cancer Res. 2017;23(12):2972–80.
Reilley MJ, Bailey A, Subbiah V, Janku F, Naing A, Falchook G, Karp D, Piha-Paul S, Tsimberidou A, Fu S, Lim J, Bean S, Bass A, Montez S, Vence L, Sharma P, Allison J, Meric-Bernstam F, Hong DS. Phase I clinical trial of combination imatinib and ipilimumab in patients with advanced malignancies. J Immunother Cancer. 2017;5:35.
Groisberg R, Hong DS, Behrang A, Hess K, Janku F, Piha-Paul S, Naing A, Fu S, Benjamin R, Patel S, Somaiah N, Conley A, Meric-Bernstam F, Subbiah V. Characteristics and outcomes of patients with advanced sarcoma enrolled in early phase immunotherapy trials. J Immunother Cancer. 2017;5(1):100.
Toulmonde M, Penel N, Adam J, Chevreau C, Blay J-Y, Cesne AL, Bompas E, Piperno-Neumann S, Cousin S, Ryckewaert T, Bessede A, Ghiringhelli F, Grellety T, Pulido M, Italiano A. Combination of pembrolizumab and metronomic cyclophosphamide in patients with advanced sarcomas and GIST: A French sarcoma group phase II trial. J Clin Oncol. 2017;35(15_suppl):11053.
Toulmonde M, Penel N, Adam J, Chevreau C, Blay J-Y, Cesne AL, Bompas E, Piperno-neumann S, Cousin S, Ryckewaert T, Bessede A, Ghiringhelli F, Pulido M, Italiano A. Combination of pembrolizumab and metronomic cyclophosphamide in patients with advanced sarcomas: a french sarcoma group study (Abstract). Cancer Res. 2017;77(13_Supplement):LB-190.
Al-Share B, Alloghbi A, Hallak MNA, Uddin H, Azmi A, Mohammad RM, Kim SH, Shields AF, Philip PA. Gastrointestinal stromal tumor: a review of current and emerging therapies. Cancer Metastasis Rev. 2021;40(2):625–41.
Schroeder BA, Kohli K, O’Malley RB, Kim TS, Jones RL, Pierce RH, Pollack SM. Durable tumor regression in highly refractory metastatic KIT/PDGFRA wild-type GIST following treatment with nivolumab. Oncoimmunology. 2020;9(1):1710064.
Chen JL, Mahoney MR, George S, Antonescu CR, Liebner DA, Tine BAV, Milhem MM, Tap WD, Streicher H, Schwartz GK, D’Angelo SP. A multicenter phase II study of nivolumab +/- ipilimumab for patients with metastatic sarcoma (Alliance A091401): Results of expansion cohorts. J Clin Oncol. 2020;38(15_suppl):11511.
Singh AS, Hecht JR, Rosen L, Wainberg ZA, Wang X, Douek M, Hagopian A, Andes R, Sauer L, Brackert SR, Chow W, DeMatteo R, Eilber FC, Glaspy JA, Chmielowski B. A randomized phase II study of nivolumab monotherapy or nivolumab combined with ipilimumab in patients with advanced gastrointestinal stromal tumors. Clin Cancer Res. 2022;28(1):84–94.
Reddy R, Velagapudi RM, Chitikela SD, Barwad A, Shrivastava S, Dhamija E, Shamim SA, Tripathy S, Pandey R, Rastogi S. Indian experience with immunotherapy in sarcoma and gastrointestinal stromal tumors: a retrospective study. Future Sci OA. 2022;8(5):FSO795.
Jiang C, Cai X, Zhang H, Xia X, Zhang B, Xia L. Activity and immune correlates of a programmed death-1 blockade antibody in the treatment of refractory solid tumors. J Cancer. 2018;9(1):205–12.
Kozak K, Pantaleo MA, Fumagalli E, Nannini M, Bylina E, Poleszczuk J, Klimczak A, Casali PG, Rutkowski P. 1667TiP A phase II, single arm study of avelumab in combination with axitinib in patients with unresectable/metastatic gastrointestinal stromal tumor after failure of standard therapy - AXAGIST. Ann Oncol. 2020;31(Suppl 4):S990.
Curigliano G, Gelderblom H, Mach N, Doi T, Tai D, Forde PM, Sarantopoulos J, Bedard PL, Lin C-C, Hodi FS, Wilgenhof S, Santoro A, Sabatos-Peyton CA, Longmire TA, Xyrafas A, Sun H, Gutzwiller S, Manenti L, Naing A. Phase I/Ib clinical trial of Sabatolimab, an Anti-TIM-3 antibody, alone and in combination with Spartalizumab, an Anti-PD-1 antibody advanced solid tumors. Clin Cancer Res. 2021;27(13):3620–9.
Edris B, Willingham SB, Weiskopf K, Volkmer AK, Volkmer J-P, Mühlenberg T, Montgomery KD, Contreras-Trujillo H, Czechowicz A, Fletcher JA, West RB, Weissman IL, Rijn Mvd. Anti-KIT monoclonal antibody inhibits imatinib-resistant gastrointestinal stromal tumor growth. Proc Natl Acad Sci U S A. 2013;110(9):3501–6.
Edris B, Willingham S, Weiskopf K, Volkmer AK, Volkmer J-P, Mühlenberg T, Weissman IL, Rijn Mvd. Use of a KIT-specific monoclonal antibody to bypass imatinib resistance in gastrointestinal stromal tumors. Oncoimmunology. 2013;2(6):e24452.
Looy TV, Wozniak A, Floris G, Li H, Wellens J, Vanleeuw U, Sciot R, Debiec-Rychter M, Schöffski P. Therapeutic efficacy assessment of CK6, a monoclonal KIT antibody, in a panel of gastrointestinal stromal tumor xenograft models. Transl Oncol. 2015;8(2):112–8.
Wagner AJ, Kindler H, Gelderblom H, Schöffski P, Bauer S, Hohenberger P, Kopp H-G, Lopez-Martin JA, Peeters M, Reichardt P, Qin A, Nippgen J, Ilaria RL, Rutkowski P. A phase II study of a human anti-PDGFRα monoclonal antibody (olaratumab, IMC-3G3) in previously treated patients with metastatic gastrointestinal stromal tumors. Ann Oncol. 2017;28(3):541–6.
Blanke CD, Rankin C, Corless C, Eary JF, Mulder K, Okuno SH, George S, Heinrich M. S0502: a SWOG phase III randomized study of imatinib, with or without bevacizumab, in patients with untreated metastatic or unresectable gastrointestinal stromal tumors. Oncologist. 2015;20(12):1353–4.
Zhao W-y, Zhuang C, Xu J, Wang M, Zhang Z, Tu L, Wang C, Ling T, Cao H, Zhang Z. Somatostatin receptors in gastrointestinal stromal tumors: new prognostic biomarker and potential therapeutic strategy. Am J Transl Res. 2014;6(6):831–40.
Format C, Abrams TJ, Niu X, Embry M, Kline J, Patawaran M, Fanton C, Ison-Dugenny M, Schneider T, Miller K, Wang Z, Ghoddusi M, Cohen S, Hong EE, Lees E, Schleyer S. Development of a novel antibody-drug conjugate for the treatment of c-Kit expressing solid tumors and AML [abstract]. Cancer Res. 2015;75(15 Suppl):1695.
Abrams T, Connor A, Fanton C, Cohen SB, Huber T, Miller K, Hong EE, Niu X, Kline J, Ison-Dugenny M, Harris S, Walker D, Krauser K, Galimi F, Wang Z, Ghoddusi M, Mansfield K, Lee-Hoeflich ST, Holash J, Pryer N, Kluwe W, Ettenberg SA, Sellers WR, Lees E, Kwon P, Abraham JA, Schleyer SC. Preclinical antitumor activity of a novel anti-c-KIT antibody-drug conjugate against mutant and wild-type c-KIT-positive solid tumors. Clin Cancer Res. 2018;24(17):4297–308.
L’Italien L, Orozco O, Abrams T, Cantagallo L, Connor A, Desai J, Ebersbach H, Gelderblom H, Hoffmaster K, Lees E, Maacke H, Schleyer S, Skegro D, Lee-Hoeflich ST. Mechanistic insights of an immunological adverse event induced by an Anti-KIT antibody drug conjugate and mitigation strategies. Clin Cancer Res. 2018;24(14):3465–74.
Iida K, Ahmed AHA, Nagatsuma AK, Shibutani T, Yasuda S, Kitamura M, Hattori C, Abe M, Hasegawa J, Iguchi T, Karibe T, Nakada T, Inaki K, Kamei R, Abe Y, Nomura T, Andersen JL, Santagata S, Hemming ML, George S, Doi T, Ochiai A, Demetri GD, Agatsuma T. Identification and therapeutic targeting of GPR20, selectively expressed in gastrointestinal stromal tumors, with DS-6157a, a first-in-class antibody-drug conjugate. Cancer Discov. 2021;11(6):1508–23.
Iida K, Abdelhamid AH, Nagatsuma AK, Shibutani T, Yasuda S, Kitamura M, Hattori C, Abe M, Hasegawa J, Iguchi T, Karibe T, Nakada T, Inaki K, Kamei R, Abe Y, Andersen JL, Santagata S, Hemming ML, George S, Doi T, Ochiai A, Demetri GD, Agatsuma T. Abstract 5181: Therapeutic targeting of GPR20, selectively expressed in gastrointestinal stromal tumor (GIST), with DS-6157a, an antibody-drug conjugate (ADC). Cancer Res. 2020;80(16):5181.
Kim J-O, Kim K-H, Baek EJ, Park B, So MK, Ko BJ, Ko H-J, Park SG. A novel anti-c-Kit antibody-drug conjugate to treat wild-type and activating-mutant c-Kit-positive tumors. Mol Oncol. 2022;16(6):1290–308.
Shioyama Y, Yakeishi Y, Watanabe T, Nakamura K, Kunitake N, Kimura M, Sasaki M, Honda H, Terashima H, Masuda K. Long-term control for a retroperitoneal metastasis of malignant gastrointestinal stromal tumor after chemoradiotherapy and immunotherapy. Acta Oncol. 2001;40(1):102–4.
Fröbom R, Berglund E, Berglund D, Nilsson I-L, Åhlén J, Sivers Kv, Linder-Stragliotto C, Suenaert P, Karlsson-Parra A, Bränström R. Phase I trial evaluating safety and efficacy of intratumorally administered inflammatory allogeneic dendritic cells (ilixadencel) in advanced gastrointestinal stromal tumors. Cancer Immunol Immunother. 2020;69(11):2393–401.
Karlsson-Parra A, Fröbom R, Berglund E, Berglund D, Nilsson I-L, Linder-Stragliotto C, Suenaert P, Branstrom R. Phase I trial evaluating safety and efficacy of intratumorally administered allogeneic monocyte-derived cells (ilixadencel) in advanced gastrointestinal stromal tumors. J Clin Oncol. 2020;38(5_suppl):15.
Katz SC, Burga RA, Naheed S, Licata LA, Thorn M, Doreen Osgood CTN, Joseph Espat N, Fletcher JA, Junghans RP. Anti-KIT designer T cells for the treatment of gastrointestinal stromal tumor. J Transl Med. 2013;11(1):46.
Tavartkiladze AA, Khutsishvili R, Revazishvili P, Maisuradze M, Tavartkiladze L, Tavartkiladze G. Treatment of refractory recurrent gastrointestinal stromal tumors with adoptive cellular immunotherapy (TILs) and personalized vaccine. Ann Oncol. 2019;30(11):13.
Fiorino E, Merlini A, D’Ambrosio L, Cerviere I, Berrino E, Marchiò C, Giraudo L, Basiricò M, Massa A, Donini C, Leuci V, Rotolo R, Galvagno F, Vitali L, Proment A, Ferrone S, Pisacane A, Pignochino Y, Aglietta M, Grignani G, Mesiano G, Sangiolo D. Integrated Antitumor Activities of Cellular Immunotherapy with CIK Lymphocytes and Interferons against KIT/PDGFRA Wild Type GIST. Int J Mol Sci. 2022;23:10368.
Kang G-H, Kim K-M, Noh J-H, Sohn T-S, Kim S, Park C-K, Lee C-S, Kang D-Y. WT-1 expression in gastrointestinal stromal tumours. Pathology. 2010;42(1):54–7.
Nonneville AD, Finetti P, Picard M, Monneur A, Pantaleo MA, Astolfi A, Ostrowski J, Birnbaum D, Mamessier E, Bertucci F. CSPG4 expression in GIST is associated with better prognosis and strong cytotoxic immune response. Cancers (Basel). 2022;14(5):1306.
Zhang D, He C, Guo Y, Li J, Li B, Zhao Y, Yu L, Chang Z, Pei H, Yang M, Li N, Zhang Q, He Y, Pan Y, Zhao ZJ, Zhang C, Chen Y. Efficacy of SCF drug conjugate targeting c-KIT in gastrointestinal stromal tumor. BMC Med. 2022;20(1):257.
Zeng S, Seifert AM, Zhang JQ, Cavnar MJ, Kim TS, Balachandran VP, Santamaria-Barria JA, Cohen NA, Beckman MJ, Medina BD, Rossi F, Crawley MH, Loo JK, Maltbaek JH, Besmer P, Antonescu CR, DeMatteo RP. Wnt/β-catenin signaling contributes to tumor malignancy and is targetable in gastrointestinal stromal tumor. Mol Cancer Ther. 2017;16(9):1954–66.
Zeng S, Seifert AM, Zhang JQ, Kim TS, Bowler TG, Cavnar MJ, Medina BD, Vitiello GA, Rossi F, Loo JK, Param NJ, DeMatteo RP. ETV4 collaborates with Wnt/β-catenin signaling to alter cell cycle activity and promote tumor aggressiveness in gastrointestinal stromal tumor. Oncotarget. 2017;8(69):114195–209.
Mukaisho K-I, Miwa K, Totsuka Y, Shimomura A, Sugihara H, Wakabayashi K, Hattori T. Induction of gastric GIST in rat and establishment of GIST cell line. Cancer Lett. 2006;231(2):295–303.
Guérin A, Martire D, Trenquier E, Lesluyes T, Sagnol S, Pratlong M, Lefebvre E, Chibon F, Barbara PdS, Faure S. LIX1 regulates YAP activity and controls gastrointestinal cancer cell plasticity. J Cell Mol Med. 2020;24(16):9244–54.
Sakurama K, Naomoto Y, Ohara T, Watanabe N, Takaoka M, Nagatsuka H, Tomono Y, Tanida T, Noma K, Tanabe S, Fujiwara Y, Motoki T, Shirakawa Y, Yamatsuji T, Hirota S, Taguchi T, Tanaka N. Establishment of a lymph node metastasis model from subcutaneous tumors of gastrointestinal stromal tumor model cells. Oncol Rep. 2009;21(2):407–11.
Sasaki M, Tanaka M, Ichikawa H, Suzuki T, Nishie H, Ozeki K, Shimura T, Kubota E, Tanida S, Kataoka H. 5-aminolaevulinic acid (5-ALA) accumulates in GIST-T1 cells and photodynamic diagnosis using 5-ALA identifies gastrointestinal stromal tumors (GISTs) in xenograft tumor models. PLoS ONE. 2021;16(4): e0249650.
Shen C, Yin Y, Chen H, Wang R, Yin X, Cai Z, Zhang B, Chen Z, Zhou Z. Secreted protein acidic and rich in cysteine-like 1 suppresses metastasis in gastric stromal tumors. BMC Gastroenterol. 2018;18(1):105.
Yoon H, Tang C-M, Banerjee S, Yebra M, Noh S, Burgoyne AM, Torre JDL, Siena MD, Liu M, Klug LR, Choi YY, Hosseini M, Delgado AL, Wang Z, French RP, Lowy A, DeMatteo RP, Heinrich MC, Molinolo AA, Gutkind JS, Harismendy O, Sicklick JK. Cancer-associated fibroblast secretion of PDGFC promotes gastrointestinal stromal tumor growth and metastasis. Oncogene. 2021;40(11):1957–73.
Flavahan WA, Drier Y, Johnstone SE, Hemming ML, Tarjan DR, Hegazi E, Shareef SJ, Javed NM, Raut CP, Eschle BK, Gokhale PC, Hornick JL, Sicinska ET, Demetri GD, Bernstein BE. Altered chromosomal topology drives oncogenic programs in SDH-deficient GISTs. Nature. 2019;575(7781):229–33.
Hemming ML, Benson MR, Loycano MA, Anderson JA, Andersen JL, Taddei ML, Krivtsov AV, Aubrey BJ, Cutler JA, Hatton C, Sicinska E, Armstrong SA. MOZ and Menin-MLL complexes are complementary regulators of chromatin association and transcriptional output in gastrointestinal stromal tumor. Cancer Discov. 2022;12(7):804–1823.
Smith BD, Kaufman MD, Lu W-P, Gupta A, Leary CB, Wise SC, Rutkoski TJ, Ahn YM, Al-Ani G, Bulfer SL, Caldwell TM, Chun L, Ensinger CL, Hood MM, McKinley A, Patt WC, Ruiz-Soto R, Su Y, Telikepalli H, Town A, Turner BA, Vogeti L, Vogeti S, Yates K, Janku F, Razak ARA, Rosen O, Heinrich MC, Flynn DL. Ripretinib (DCC-2618) is a switch control kinase inhibitor of a broad spectrum of oncogenic and drug-resistant KIT and PDGFRA variants. Cancer Cell. 2019;35(5):738–51.
Lin W-H, Wu S-Y, Yeh T-K, Chen C-T, Song J-S, Shiao H-Y, Kuo C-C, Hsu T, Lu C-T, Wang P-C, Wu T-S, Peng Y-H, Lin H-Y, Chen C-P, Weng Y-L, Kung F-C, Wu M-H, Su Y-C, Huang K-W, Chou L-H, Hsueh C-C, Yen K-J, Kuo P-C, Huang C-L, Chen L-T, Shih C, Tsai H-J, Jiaang W-T. Identification of a multitargeted tyrosine kinase inhibitor for the treatment of gastrointestinal stromal tumors and acute myeloid leukemia. J Med Chem. 2019;62(24):11135–50.
Lu X, Pang Y, Cao H, Liu X, Tu L, Shen Y, Jia X, Lee J-C, Wang Y. Integrated screens identify CDK1 as a therapeutic target in advanced gastrointestinal stromal tumors. Cancer Res. 2021;81(9):2481–94.
Cao Y, Zhang X, Chen Q, Rao X, Qiu E, Wu G, Lin Y, Zeng Z, Zheng B, Li Z, Cai Z, Wang H, Han S. Patient-derived organoid facilitating personalized medicine in gastrointestinal stromal tumor with liver metastasis: a case report. Front Oncol. 2022;12: 920762.
Forsythe SD, Sivakumar H, Erali RA, Wajih N, Li W, Shen P, Levine EA, Miller KE, Skardal A, Votanopoulos KI. Patient-specific sarcoma organoids for personalized translational research: unification of the operating room with rare cancer research and clinical implications. Ann Surg Oncol. 2022;29(12):7354–67.
Nishida T, Hirota S, Taniguchi M, Hashimoto K, Isozaki K, Nakamura H, Kanakura Y, Tanaka T, Takabayashi A, Matsuda H, Kitamura Y. Familial gastrointestinal stromal tumours with germline mutation of the KIT gene. Nat Genet. 1998;19(4):323–4.
Nakahara M, Isozaki K, Hirota S, Miyagawa J, Hase-Sawada N, Taniguchi M, Nishida T, Kanayama S, Kitamura Y, Shinomura Y, Matsuzawa Y. A novel gain-of-function mutation of c-kit gene in gastrointestinal stromal tumors. Gastroenterology. 1998;115(5):1090–5.
Tuveson DA, Willis NA, Jacks T, Griffin JD, Singer S, Fletcher CD, Fletcher JA, Demetri GD. STI571 inactivation of the gastrointestinal stromal tumor c-KIT oncoprotein: biological and clinical implications. Oncogene. 2001;20(36):5054–8.
Taguchi T, Sonobe H, Toyonaga S-i, Yamasaki I, Shuin T, Takano A, Araki K, Akimaru K, Yuri K. Conventional and molecular cytogenetic characterization of a new human cell line, GIST-T1, established from gastrointestinal stromal tumor. Lab Invest. 2002;82(5):663–5.
Duensing A, Medeiros F, McConarty B, Joseph NE, Panigrahy D, Singer S, Fletcher CDM, Demetri GD, Fletcher JA. Mechanisms of oncogenic KIT signal transduction in primary gastrointestinal stromal tumors (GISTs). Oncogene. 2004;23(22):3999–4006.
Bauer S, Hubert C, Heinrich MC, Cohen P, Bertagnolli M, Fletcher GDD. KIT hyperactivation in imatinib-resistant GIST: Implications for salvage therapies. J Clin Oncol. 2005;23(16_suppl):9034.
Bauer S, Yu LK, Demetri GD, Fletcher JA. Heat shock protein 90 inhibition in imatinib-resistant gastrointestinal stromal tumor. Cancer Res. 2006;66(18):9153–61.
Prenen H, Stefan C, Landuyt B, Vermaelen P, Debiec-Rychter M, Bollen M, Stroobants S, Bruijn Ed, Mortelmans L, Sciot R, Schöffski P, Oosterom Av. Imatinib mesylate inhibits glucose uptake in gastrointestinal stromal tumor cells by downregulation of the glucose transporters recruitment to the plasma membrane. Am J Biochem Biotechnol. 2005;1(2):95–102.
Prenen H, Guetens G, Boeck Gd, Debiec-Rychter M, Manley P, Schoffski P, Oosterom ATv, Bruijn Ed. Cellular uptake of the tyrosine kinase inhibitors imatinib and AMN107 in gastrointestinal stromal tumor cell lines. Pharmacology. 2006;77(1):11–6.
Rossi S, Ou W, Tang D, Bhattacharya N, Tos APD, Fletcher JA, Loda M. Gastrointestinal stromal tumours overexpress fatty acid synthase. J Pathol. 2006;209(3):369–75.
Zhu B, Liao G, Liu S, Huang B, Wu S, Zhou J, Gu H, Zhu H. Characteristics and establishment of cell lines from human gastrointestinal stromal tumors. J Cent South Univ (Med Sci). 2010;35(11):1138–44.
Floris G, Debiec-Rychter M, Wozniak A, Stefan C, Normant E, Faa G, Machiels K, Vanleeuw U, Sciot R, Schöffski P. The heat shock protein 90 inhibitor IPI-504 induces KIT degradation, tumor shrinkage, and cell proliferation arrest in xenograft models of gastrointestinal stromal tumors. Mol Cancer Ther. 2011;10(10):1897–908.
Floris G, Sciot R, Wozniak A, Looy TV, Wellens J, Faa G, Normant E, Debiec-Rychter M, Schöffski P. The Novel HSP90 inhibitor, IPI-493, is highly effective in human gastrostrointestinal stromal tumor xenografts carrying heterogeneous KIT mutations. Clin Cancer Res. 2011;17(17):5604–14.
Simon S, Grabellus F, Ferrera L, Galietta L, Schwindenhammer B, Mühlenberg T, Taeger G, Eilers G, Treckmann J, Breitenbuecher F, Schuler M, Taguchi T, Fletcher JA, Bauer S. DOG1 regulates growth and IGFBP5 in gastrointestinal stromal tumors. Cancer Res. 2013;73(12):3661–70.
Sun X-C, Yan J-Y, Chen X-L, Huang Y-P, Shen X, Ye X-H. Depletion of telomerase RNA inhibits growth of gastrointestinal tumors transplanted in mice. World J Gastroenterol. 2013;19(15):2340–7.
Fukuda K, Saikawa Y, Sako H, Yoshimura Y, Takahashi T, Wada N, Kawakubo H, Takeuchi H, Ohmori T, Kitagawa Y. Establishment and characterization of novel cell lines and xenografts from patients with gastrointestinal stromal tumors. Oncol Rep. 2013;30(1):71–8.
Kim TS, Cavnar MJ, Cohen NA, Sorenson EC, Greer JB, Seifert AM, Crawley MH, Green BL, Popow R, Pillarsetty N, Veach DR, Ku AT, Rossi F, Besmer P, Antonescu CR, Zeng S, Dematteo RP. Increased KIT inhibition enhances therapeutic efficacy in gastrointestinal stromal tumor. Clin Cancer Res. 2014;20(9):2350–62.
Serrano C, Mariño-Enríquez A, Tao DL, Ketzer J, Eilers G, Zhu M, Yu C, Mannan AM, Rubin BP, Demetri GD, Raut CP, Presnell A, McKinley A, Heinrich MC, Czaplinski JT, Sicinska E, Bauer S, George S, Fletcher JA. Complementary activity of tyrosine kinase inhibitors against secondary kit mutations in imatinib-resistant gastrointestinal stromal tumours. Br J Cancer. 2019;120(6):612–20.
Cohen NA, Zeng S, Seifert AM, Kim TS, Sorenson EC, Greer JB, Beckman MJ, Santamaria-Barria JA, Crawley MH, Green BL, Rossi F, Besmer P, Antonescu CR, DeMatteo RP. Pharmacological inhibition of KIT activates MET signaling in gastrointestinal stromal tumors. Cancer Res. 2015;75(10):2061–70.
Li B, Wang A, Liu J, Qi Z, Liu X, Yu K, Wu H, Chen C, Hu C, Wang W, Wu J, Hu Z, Ye L, Zou F, Liu F, Wang B, Wang L, Ren T, Zhang S, Bai M, Zhang S, Liu J, Liu Q. Discovery of N-((1-(4-(3-(3-((6,7-Dimethoxyquinolin-3-yl)oxy)phenyl)ureido)-2-(trifluoromethyl)phenyl)piperidin-4-yl)methyl)propionamide (CHMFL-KIT-8140) as a highly potent type II inhibitor capable of inhibiting the T670I “Gatekeeper” mutant of cKIT kinase. J Med Chem. 2016;59(18):8456–72.
Tu Y, Zuo R, Ni N, Eilers G, Wu D, Pei Y, Nie Z, Wu Y, Wu Y, Ou W-B. Activated tyrosine kinases in gastrointestinal stromal tumor with loss of KIT oncoprotein expression. Cell Cycle. 2018;17(23):2577–92.
Sommer G, Agosti V, Ehlers I, Rossi F, Corbacioglu S, Farkas J, Moore M, Manova K, Antonescu CR, Besmer P. Gastrointestinal stromal tumors in a mouse model by targeted mutation of the Kit receptor tyrosine kinase. Proc Natl Acad Sci U S A. 2003;100(11):6706–11.
Rubin BP, Antonescu CR, Scott-Browne JP, Comstock ML, Gu Y, Tanas MR, Ware CB, Woodell J. A knock-in mouse model of gastrointestinal stromal tumor harboring kit K641E. Cancer Res. 2005;65(15):6631–9.
Nakai N, Ishikawa T, Nishitani A, Liu N-N, Shincho M, Hao H, Isozaki K, Kanda T, Nishida T, Fujimoto J, Hirota S. A mouse model of a human multiple GIST family with KIT-Asp820Tyr mutation generated by a knock-in strategy. J Pathol. 2008;214(3):302–11.
Bosbach B, Deshpande S, Rossi F, Shieh J-H, Sommer G, Stanchina Ed, Veach DR, Scandura JM, Manova-Todorova K, Moore MAS, Antonescu CR, Besmer P. Imatinib resistance and microcytic erythrocytosis in a KitV558Δ;T669I/+ gatekeeper-mutant mouse model of gastrointestinal stromal tumor. Proc Natl Acad Sci U S A. 2012;109(34):E2276-83.
Pelczar P, Zibat A, Dop WAv, Heijmans J, Bleckmann A, Gruber W, Nitzki F, Uhmann A, Guijarro MV, Hernando E, Dittmann K, Wienands J, Dressel R, Wojnowski L, Binder C, Taguchi T, Beissbarth T, Hogendoorn PCW, Antonescu CR, Rubin BP, Schulz-Schaeffer W, Aberger F, Brink GRvd, Hahn H. Inactivation of Patched1 in mice leads to development of gastrointestinal stromal-like tumors that express Pdgfrα but not kit. Gastroenterology. 2013;144(1):134–44.
Ran L, Sirota I, Cao Z, Murphy D, Chen Y, Shukla S, Xie Y, Kaufmann MC, Gao D, Zhu S, Rossi F, Wongvipat J, Taguchi T, Tap WD, Mellinghoff IK, Besmer P, Antonescu CR, Chen Y, Chi P. Combined inhibition of MAP kinase and KIT signaling synergistically destabilizes ETV1 and suppresses GIST tumor growth. Cancer Discov. 2015;5(3):304–15.
Bosbach B, Rossi F, Yozgat Y, Loo J, Zhang JQ, Berrozpe G, Warpinski K, Ehlers I, Veach D, Kwok A, Manova K, Antonescu CR, DeMatteo RP, Besmer P. Direct engagement of the PI3K pathway by mutant KIT dominates oncogenic signaling in gastrointestinal stromal tumor. Proc Natl Acad Sci U S A. 2017;114(40):E8448–57.
Ran L, Murphy D, Sher J, Cao Z, Wang S, Walczak E, Guan Y, Xie Y, Shukla S, Zhan Y, Antonescu CR, Chen Y, Chi P. ETV1-positive cells give rise to BRAFV600E -mutant gastrointestinal stromal tumors. Cancer Res. 2017;77(14):3758–65.
Kondo J, Huh WJ, Franklin JL, Heinrich MC, Rubin BP, Coffey RJ. A smooth muscle-derived, BRAF-driven mouse model of gastrointestinal stromal tumor (GIST): evidence for an alternative GIST cell-of-origin. J Pathol. 2020;252(4):441–50.
Zhang JQ, Bosbach B, Loo JK, Vitiello GA, Zeng S, Seifert AM, Medina BD, Param NJ, Maltbaek JH, Rossi F, Antonescu CR, Besmer P, DeMatteo RP. The V654A second-site KIT mutation increases tumor oncogenesis and STAT activation in a mouse model of gastrointestinal stromal tumor. Oncogene. 2020;39(49):7153–65.
Tan WCC, Nerurkar SN, Cai HY, Ng HHM, Wu D, Wee YTF, Lim JCT, Yeong J, Lim TKH. Overview of multiplex immunohistochemistry/immunofluorescence techniques in the era of cancer immunotherapy. Cancer Commun (Lond). 2020;40(4):135–53.
Wang G, Sun J, Zhang J, Zhu Q, Lu J, Gao S, Wang F, Yin Q, Wan Y, Li Q. Single-cell transcriptional profiling uncovers the association between EOMES+CD8+ T cells and acquired EGFR-TKI resistance. Drug Resist Updat. 2023;66: 100910.
Dugage MR, Jones RL, Trent J, Champiat Sp, Dumont S. Beyond the driver mutation: immunotherapies in gastrointestinal stromal tumors. Front Immunol. 2021;12:715727.
Song S, Li B, Carvalho MR, Wang H, Mao D, Wei J, Chen W, Weng Z, Chen Y, Deng C, Reis RL, Oliveira JM, He Y, Yan L, Zhang C. Complex in vitro 3D models of digestive system tumors to advance precision medicine and drug testing: Progress, challenges, and trends. Pharmacol Ther. 2022;239: 108276.
Author information
Authors and Affiliations
Contributions
B.L., H.C. and S.Y. collected relevant literatures, drafted the contents, wrote and edited the manuscript. B.L. and H.C. designed and prepared figures and tables. F.C., L.X., Y.L., M.L., C.Z., F.S., X.Z., reviewed and critically revised this manuscript. C.Z., Y.H., L.Z. and C.D. conceptualized this work and guided the preparation of this manuscript. All authors have read and approved the content of the manuscript before the final submission.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, B., Chen, H., Yang, S. et al. Advances in immunology and immunotherapy for mesenchymal gastrointestinal cancers. Mol Cancer 22, 71 (2023). https://doi.org/10.1186/s12943-023-01770-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12943-023-01770-6