
Abstract
Background
In global efforts to track mosquito infectivity and parasite elimination, controlled mosquito-feeding experiments can help in understanding the dynamics of parasite development in vectors. Anopheles stephensi is often accepted as the major urban malaria vector that transmits Plasmodium in Goa and elsewhere in South Asia. However, much needs to be learned about the interactions of Plasmodium vivax with An. stephensi. As a component of the US NIH International Center of Excellence for Malaria Research (ICEMR) for Malaria Evolution in South Asia (MESA), a series of membrane-feeding experiments with wild An. stephensi and P. vivax were carried out to better understand this vector-parasite interaction.
Methods
Wild An. stephensi larvae and pupae were collected from curing water in construction sites in the city of Ponda, Goa, India. The larvae and pupae were reared at the MESA ICEMR insectary within the National Institute of Malaria Research (NIMR) field unit in Goa until they emerged into adult mosquitoes. Blood for membrane-feeding experiments was obtained from malaria patients at the local Goa Medical College and Hospital who volunteered for the study. Parasites were counted by Miller reticule technique and correlation between gametocytaemia/parasitaemia and successful mosquito infection was studied.
Results
A weak but significant correlation was found between patient blood gametocytaemia/parasitaemia and mosquito oocyst load. No correlation was observed between gametocytaemia/parasitaemia and oocyst infection rates, and between gametocyte sex ratio and oocyst load. When it came to development of the parasite in the mosquito, a strong positive correlation was observed between oocyst midgut levels and sporozoite infection rates, and between oocyst levels and salivary gland sporozoite loads. Kinetic studies showed that sporozoites appeared in the salivary gland as early as day 7, post-infection.
Conclusions
This is the first study in India to carry out membrane-feeding experiments with wild An. stephensi and P. vivax. A wide range of mosquito infection loads and infection rates were observed, pointing to a strong interplay between parasite, vector and human factors. Most of the present observations are in agreement with feeding experiments conducted with P. vivax elsewhere in the world.
Similar content being viewed by others

Background
Plasmodium vivax poses a serious threat to half of the world’s population, including the whole of South Asia [1]. In 2015, an estimated 13.8 million cases were caused by P. vivax [2]. India, Pakistan and Ethiopia are estimated to contribute greater than 80% of P. vivax cases in the world [2]. Hypnozoites, the dormant liver forms that are unique to P. vivax and Plasmodium ovale, can spontaneously re-activate and lead to periodic clinical relapses [3]. Many of the asymptomatic P. vivax infections in endemic areas are caused by hypnozoites [4] and these sub-clinical infections are difficult to detect, and thus complicate control measures.
Until now, in the absence of a culture system for continuous development of P. vivax, most of the knowledge on P. vivax is based on experimental and natural human infections [4,5,6,7]. For example, unlike Plasmodium falciparum, which invades all stages of erythrocytes, P. vivax selectively invades reticulocytes [6, 8,9,10]. P. vivax sexual development takes place in vectors when they ingest mature, infective gametocytes circulating in the peripheral blood [6, 11]. Compared to P. falciparum, gametocytes are more commonly observed in P. vivax infections [12], and they appear in blood smears much earlier in an infection [13]. Although clinical studies have shown that blood from asymptomatic, sub-microscopic gametocyte infections can infect mosquitoes, the correlation between P. vivax gametocytaemia and mosquito infections have been variable, with studies showing positive [14, 15], weak [5, 16, 17] and poor correlation [18,19,20]. Studying gametocytes in human blood is further complicated by the fact that the conventional microscopic techniques used for counting gametocytaemia are not always accurate and could contribute to the over- or underestimation of parasites in patient blood smears [21,22,23,24]. Furthermore, in controlled mosquito infections, the correlation between midgut oocyst numbers and salivary gland sporozoite load in P. vivax infections is not well understood. Successful mosquito infection of Plasmodium could be influenced by a number of parasite, vector and human factors including the state of gametocyte maturation, proportion of male and female gametocytes, variation in parasite genetics and transmission-blocking antibodies [11, 25,26,27,28,29,30]. Additionally, mosquito factors such as age, genetic diversity and microbiota could potentially affect the P. vivax infection rate and oocyst load [26, 31,32,33]. Many of the above uncertainties in studying the complex life cycle of P. vivax may be overcome with controlled feeding experiments.
The standard membrane feeding assay (SMFA) and direct skin feeding are the two most commonly used techniques for controlled mosquito infections studies [34]. Although direct skin feeding is more sensitive [34], ethical considerations and practical constraints favour the use of SMFA at many endemic sites.
As a part of the US NIH International Centers of Excellence for Malaria Research (ICEMR) [35,36,37], the Malaria Evolution in South Asia (MESA) programme has set up a controlled mosquito-feeding laboratory at the MESA-National Institute of Malaria Research (NIMR) joint study site in Panaji, Goa, India. For mosquito-feeding experiments, P. vivax-infected blood was obtained from patients recruited at the nearby Goa Medical College and Hospital (GMC), the other MESA study site in Goa [38]. To better understand the dynamics of parasite development in mosquitoes in southwestern India, 30 laboratory-feeding experiments were conducted with wild An. stephensi [39, 40] and P. vivax-infected patient blood. This paper describes the importance of patient blood parasitaemia and gametocytaemia on successful mosquito infection, as measured by oocyst numbers and sporozoite load. The potential role of Indian mosquito immunity in controlling P. vivax sporozoite load is also described.
Methods
Wild An. stephensi larvae collection and maintenance
Wild An. stephensi larvae and pupae were collected from breeding habitats, the curing waters in construction sites, around Ponda city in the state of Goa, India. The mosquito larvae and pupae were collected using the dipping technique and were transferred, along with breeding water, to plastic containers. The containers were then brought to the MESA insectary at the NIMR Goa field station. In the insectary, third and fourth instar larvae were separated from the first and second instar larvae and were reared separately. Pupae collected from the field were kept in 500-ml plastic bowls containing 200 ml of tap water, and inside a closed cage for controlled emergence. The larvae were reared in plastic trays containing tap water under laboratory conditions at 27 ± 2 °C, 70 ± 5% relative humidity and 12 h light/12 h dark photoperiod cycling. A pinch of Cerelac® powder (Nestle) and fish food (1:1) mixture was given to the larvae once a day until pupal stage development was visible. Once formed, pupae were collected in fresh plastic bowls containing tap water, and then kept inside a closed cage for emergence of adults. The adult mosquitoes that emerged from these pupae were given 10% glucose soaked in a cotton pad. The species of emerged adult mosquitoes were identified using standard morphological keys.
Ethics and approvals
The human subjects protocol governing collection of malaria parasites at GMC was approved by the Institutional Ethics Committee of Goa Medical College and Hospital, the University of Washington Institutional Review Board and by the US NIH/NIAID Division of Microbiology and Infectious Disease (DMID). The MESA-ICEMR programme project was additionally approved by the Health Ministry Screening Committee (HMSC) of the Government of India and by the Government of Goa Public Health Department.
Blood collection from P. vivax patients
Plasmodium vivax patients confirmed by microscopy at GMC were briefed about the study by the project staff, and volunteers were recruited for the study. Prior to blood collection, informed consent was obtained from each patient. Approximately 6 ml of blood was drawn into an acid citrate dextrose vacutainer by venipuncture. Immediately after collection, the vacutainer was placed in a thermos flask maintained at 37 °C and was transported to the mosquito infection laboratory at NIMR-Goa.
Mosquito-feeding experiments
Six to seven days old, adult, female mosquitoes were used for all the experiments. Female mosquitoes were caught using an aspirator and were transferred to plastic cups covered with mesh netting secured by a rubber band and a cup lid. Approximately 125 mosquitoes were placed in each cup. These mosquitoes were starved for 16–18 h prior to blood feeding. The close proximity of the malaria patient pool at GMC helped in receiving the patient blood at NIMR-Goa within one-and-a-half hours from the time of blood draw. Within minutes of arrival at NIMR-Goa, 2 ml of infected blood was added to a 5-cm wide water-jacketed membrane feeder fitted to a circulating water bath maintained at 37 °C. The feeder was positioned in the centre of the plastic container holding the mosquitoes. The blood was maintained at 37 °C during the entire 90-min feeding time to avoid premature exflagellation. After feeding, unfed mosquitoes were separated from fully engorged ones using an aspirator. The plastic cup containing the fully fed mosquitoes were kept in Percival incubators at 27 °C ±2 and 80% ±2 relative humidity. A cotton pad soaked in 10% glucose solution feed was provided until the mosquitoes were dissected at various time points (see below).
Mosquito dissections and microscopy
For oocyst dissection on days 7/8 post blood feeding, five mosquitoes at a time were caught using a glass aspirator and were transferred to a test tube, which was then plugged with cotton. The test tube was placed in a −20 °C freezer for 2–3 min to immobilize the mosquitoes. Once the mosquitoes were knocked down, the test tube was placed on ice. Proboscis, wings and legs were first dissected to prevent accidental escape of infected mosquitoes. The dissected midgut was placed in a drop of 2% mercurochrome in PBS on a microscope slide with a coverslip, and examined for oocysts. The oocysts were counted using a phase contrast microscope at 5× and 10× (Carl Zeiss Axio Lab. A1). Salivary glands were dissected on different days post-infection, and were imaged at 40× magnification with a phase contrast microscope (Carl Zeiss Axio Lab. A1). Oocysts and sporozoites were counted independently by two project staff. The sporozoite load was calculated based on earlier studies [19, 41], and the gland index was recorded as: 1+ for (1–10 sporozoites), 2+ for (10–100 sporozoites), 3+ for (101–1000 sporozoites), 4+ for (>1000 sporozoites). In the present study, oocyst infection rate indicates the percentage of mosquitoes that contain one or more oocysts in a feeding experiment. Average oocyst load indicates the average number of oocysts in a population of mosquitoes in a feeding experiment. Sporozoite infection rate indicates the percentage of mosquitoes that contain one or more sporozoites in a feeding experiment.
Patient blood parasite counts
Thin and thick smears were prepared with the donor patient blood and were stained with a 10% Giemsa solution. Patient blood parasitaemia and gametocytaemia in thin smears were counted by two trained technicians. Counting was done by the Miller reticule technique [42], and for every smear, 100 fields were counted. The ratio of large reticule to small reticule was calculated by ImageJ software, and was 4:1. The reticule factor was 25.
Statistics
Statistical analysis was performed using the GraphPad Prism software. Pearson correlation was used to determine the significance of correlation between the counts of two independent slide readers. Linear regression was used to study the correlation between donor blood gametocytaemia and parasitaemia, and successful mosquito infections. The correlation between average oocyst load and sporozoite load was also evaluated using linear regression.
Results
Light microscopy
The parasitaemia and gametocytaemia counts (Fig. 1a, b) by two trained microscopists using the Miller reticule technique were significantly similar (parasitaemia-Pearson r 0.9685, p < 0.0001; gametocytaemia-Pearson r 0.9682, p < 0.0001). The average patient blood P. vivax parasitaemia (%) was 0.63 (Mean) ±0.38 (SD) and P. vivax gametocytaemia (%) was 0.19 (Mean) ±0.17 (SD), respectively. The number of female and male gametocytes were similar: The range and average of female gametocytes was 0.02–0.33% and 0.1 (Mean) ±0.08 (SD), respectively, and the range of male P. vivax gametocytes was 0–0.39%, and the average was 0.09 (Mean) ±0.09 (SD). The mean ratio of female to male P. vivax gametocytes was 1.31, and the range was 0–3.12. Parasite counts for each experiment from each of the two microscopists are given in Additional file 1. P. vivax gametocyte levels in patient blood were measured to study if it was the primary determinant of successful infection in mosquitoes. Linear regression analysis found a positive correlation between gametocytaemia and parasitaemia (R2 = 0.7686, p < 0.0001) (Fig. 1c). The average of the individual parasite counts of the two technicians were used for correlating gametocytaemia and parasitaemia to oocyst and sporozoite infection rates.

Assessment of co-relationship between gametocytaemia and parasitaemia in patient blood. a, b Graphs showing the direct comparison of individual values of parasitaemia and gametocytaemia counted by two microscopists to establish reproducibility and confidence in the data. c Linear regression to demonstrate the direct correlation between gametocytaemia and parasitaemia in patient blood
Gametocytaemia, parasitaemia and correlation with infection
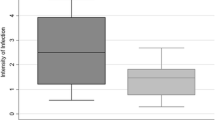
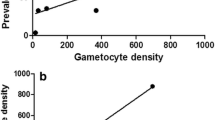
Thirty feeding experiments were conducted with P. vivax-infected patient blood and wild An. stephensi. Detailed information on the number of mosquitoes dissected, infection rates, oocyst range, average oocyst load, and salivary gland index are given in Table 1. Weak correlations were observed between patient blood P. vivax parasitaemia and oocyst number (R2 = 0.14, p = 0.04) and between patient blood gametocytaemia and oocyst number (R2 = 0.24, p = 0.006) (Fig. 2a, b). The oocyst infection rate based on 30 feeds had no correlation with parasitaemia (R2 = 5E − 05, p = 0.97) and gametocytaemia (R2 = 0.01, p = 0.58) (Fig. 2c, d).

Assessment of the role of gametocytaemia, parasitaemia and gametocyte sex ratio on mosquito infection. a, b Correlation between parasitaemia/gametocytaemia and oocyst number. c, d Correlation between parasitaemia/gametocytaemia and oocyst infection rate. e, f Correlation between parasitaemia/gametocytaemia and sporozoite infection rate. g Correlation between oocyst and sporozoite infection rate. h Correlation between female: male gametocyte ratio and average oocyst number
To calculate sporozoite infection rates, data from 23 of the 30 experiments, where at least ten mosquitoes were dissected for salivary gland infections, were included. Again, there was no correlation between sporozoite infection rate and patient blood parasitaemia (R2 = 0.004, p = 0.77) or patient blood gametocytaemia (R2 = 0.044, p = 0.33) (Fig. 2e, f). When oocyst and sporozoite infection rates were compared, a strong positive correlation (R2 = 0.84, p < 0.0001) was observed (Fig. 2g). The effect of sex ratio of female and male gametocytes on oocyst numbers was also compared, and no correlation was found (R2 = 0.0028, p = 0.78) (Fig. 2h). Interestingly, only five of the 30 patients had a female to male gametocyte sex ratio of >2, and in eight experiments where the average oocyst load was >20, the average sex ratio was 1.25. This indicates that higher oocyst load in wild An. stephensi in this region corresponds to a gametocyte sex ratio close to 1.
Correlation between P. vivax oocyst and P. vivax sporozoite load in An. stephensi
In the P. vivax patient blood-feeding experiments, a wide range of oocyst numbers were observed in mosquitoes, even between individuals of the same batch. In some midguts, the number of oocysts were greater than 200 (Fig. 3a, b). The sporozoites were graded by gland index which ranged from 1+ to 4+. When salivary glands were dissected on days 12/13, the midguts were also examined for the presence of oocysts. The oocyst load on day 12/13 was significantly lower than on day 7 and the majority of the oocysts were not healthy. Images of varying loads of sporozoites (4+ to 1+) and their corresponding midguts are shown in Fig. 3c–j. A majority of the mosquitoes with a gland index of 4+ had some melanized and unhealthy oocysts in their midgut (Fig. 3c, d). In mosquitoes with gland index of 3+ , midguts with varying levels of oocysts from zero (Fig. 3e, f) to heavily loaded melanized and unhealthy oocysts were observed. There were no oocysts present in most of the mosquitoes that had a gland index of 2+ and 1+ (Fig. 3g–j). In several mosquitoes, midguts with a heavy load of unhealthy and melanized oocysts had a gland index of 3+ (Fig. 3l, k). Data from 19 positive salivary gland infection experiments, where at least ten mosquitoes were dissected (Table 1), allowed a comparison between average oocyst load and the sporozoite load. In general, there was a positive correlation as shown by the increase in mosquitoes with gland index of 3+ (R2 = 0.29, p = 0.016) and 4+ (R2 = 0.38, p = 0.004) (Fig. 4). Sporozoite loads of 4+ were seen even when the average oocyst load was less than 10 (Fig. 4). When the average oocyst load was greater than 79, the number of mosquitoes with gland index of 4+ decreased (Fig. 4), indicating a possible role of vector immune system in controlling Plasmodium infection.

Oocyst and sporozoite infection in wild An. stephensi. Range of oocysts seen in a single feeding experiment (>200 oocysts: a; 0–10 oocysts: b). The midgut and gland indices of mosquitoes dissected on day 12/13 (c 4+, e 3+, g 2+, i 1+). The corresponding midguts of 4+, 3+, 2+, and 1+ mosquitoes are shown in d, f, h, and j. Midgut with heavily melanized and unhealthy oocysts, and corresponding gland with 3+ sporozoite load are shown in l and k, respectively. Melanized oocysts appear deformed, and contain dark pigments

Correlation between oocyst and sporozoite load. a A stacked column comparing the average oocyst load (horizontal axis) to the sporozoite load (vertical axis) is shown. Sporozoite gland index are denoted by 1+ (blue), 2+ (orange), 3+ (grey), and 4+ (yellow). The number of positive mosquitoes are shown inside the coloured bars. b, c Linear regression to study correlation between average oocyst load and percentage of mosquitoes (out of total dissected) that had gland index of 3+ and 4+, respectively. Oocyst numbers were obtained on days 7/8 post feeding
Kinetics of P. vivax sporozoites development at different time points post blood feeding in wild An. stephensi
The presence of P. vivax sporozoites in salivary glands was examined at different time points post-infection with patient blood. The first appearance of sporozoites was on day 7, and the sporozoite load in positive mosquitoes (two out of 17 dissected) were quite low (1+). The positivity of gland infection increased on day 8, and by day 12/13, the majority of oocyst had ruptured and salivary gland invasion was almost complete. Few mosquitoes were alive in the 4th week post blood feeding, and sporozoites were observed in 15 out of the 17 mosquitoes that were dissected. One mosquito survived up to day 30, and was also positive for salivary gland infection (Table 2).
Discussion
Controlled laboratory-feeding experiments can help in understanding the development kinetics of Plasmodium in its vector [5, 6, 43]. Mosquito-feeding experiments were carried out using wild An. stephensi mosquitoes that emerged from field-caught larvae. In contrast, to date, most of the P. vivax infection experiments published earlier were done with colonized Anopheles mosquitoes [11, 14, 19, 41, 44,45,46,47,48]. When field mosquitoes are colonized, they generally undergo genetic drift, lose rare alleles, and show a decrease in heterozygosity and an increase in inbreeding that may not fully represent the biological interactions with parasite that happen in the wild [43, 49,50,51]. A recent report suggested that, by the 21st generation, colonized Anopheles darlingi underwent low to moderate differentiation from the original wild mosquito population [50]. Although collecting wild larvae requires additional human resources, is tedious, and collections are limited by seasonal availability, infection experiments with wild mosquitoes provide a solid baseline simulation of Plasmodium-Anopheles interactions in the wild. In the future, experiments with high passage colonized An. stephensi maintained in the MESA NIMR Goa insectary will be compared with the wild population for their susceptibility to P. vivax infections.
In many places, it is not common to have patient blood with P. vivax and vector laboratories in close proximity. The MESA-ICEMR mosquito infection laboratory at NIMR is located within 5 km of GMC, the study site where P. vivax patients are recruited and enrolled [38]. The close proximity of the two study sites facilitates easy transport of blood and enables feeding of mosquitoes to within one-and-a-half hours from the time of blood collection. The short duration between blood collection and mosquito feeding minimizes the loss in infectivity of the blood sample due to environmental factors, such as drop in temperature and change in blood pH [26, 52]. A recent study found that blood samples fed to mosquitoes at 8 h were significantly less infective than samples fed at 4 h post blood collection [26]. Furthermore, from the point of collection through mosquito feeding, the blood was always maintained at 37 °C to prevent premature exflagellation and any accompanying loss in mosquito infectivity.
Studying the correlation between the parasite load in the patient blood sample and the corresponding mosquito infections may help better understand the dynamics of parasite development in its vector in specific geographic locations. Correlations made between gametocyte density and mosquito infection based on thick smears are not always reliable, as up to 80% of gametocytes may be lost during the staining procedure [21], and the density of white blood cells (WBCs), to which gametocyte counts are related, is difficult to ascertain [22, 23]. In this study, two expert microscopists counted the parasites in 100 fields each by the Miller counting technique, and their counts were significantly similar, thereby giving greater confidence in the correlation analysis. Positive correlation was observed between gametocytaemia and parasitaemia in P. vivax patient smears. The correlation between gametocyte density and mosquito infection is often considered weak [7,8,9,10]. In the studies presented here, there was weak correlation between gametocytaemia/parasitaemia to oocyst numbers and no correlation to oocyst infection rate. Also, the ratio of female to male gametocytes did not affect mosquito infections. It appears that the number of mature/infective gametocytes in the blood sample is more important in determining the oocyst load than the absolute number of gametocytes. Furthermore, since the study was conducted in a malaria-endemic area, the transmission blocking immunity in the host serum [28,29,30] may also help determine the oocyst numbers. In experiments where the average mosquito oocyst load was greater than 20, the proportion of male gametocytes in patient blood was closer to 50%. This indicates that for good infectivity in this transmission setting, equal proportion of male and female gametocytes are required. In natural infections of P. falciparum [53,54,55] and in P. vivax [14], ratios of three or four female gametocytes to a male gametocyte is common, although there are variations depending on clones [56], treatment [57, 58] and the course of infection [59, 60]. The high proportion of male gametocytes in this geographical location may be an adaptation of the parasite to counter host’s transmission blocking immune mechanisms that may affect the production of male gametes [61]. Also, in P. falciparum, it has been suggested that gametocyte density may affect gametocyte sex ratios, with low density favouring greater proportion of male gametocytes and increased transmission [62].
Sub-microscopic gametocyte infections are less common with P. vivax than with P. falciparum [12] and, as reported earlier [6], gametocytes were seen in all of the patient samples. In agreement with earlier studies [19, 63], at one level, development of parasites from oocytes to sporozoites appeared very efficient in mosquitoes. There was a strong positive correlation between the percentage of mosquitoes positive for oocysts and per cent sporozoite positivity. However, the correlation between oocyst numbers in individual mosquitoes and sporozoite load was not linear. When the average oocyst load ranged between 0 and 66, a positive correlation with the sporozoite load was observed, as indicated by the increase in mosquitoes with gland indices of 3+ and 4+. While P. vivax studies of this type in An. stephensi are not known, an earlier study reported a linear correlation between oocyst and sporozoite load in Anopheles dirus and Anopheles minimus infected with P. vivax [47]. In the present study, however, when the average oocyst load was greater than 79, there was a decrease in the number of mosquitoes with a gland index of 4+. On day 12, some salivary glands were dissected in parallel with the midguts of the same mosquitoes and examined for oocyst health and load. In several cases, mosquitoes with numerous melanized and unhealthy oocysts failed to have a heavy sporozoite load (4+). This suggests that when the oocyst load is sufficiently high, enhanced melanization is activated in the mosquito, providing protection from tissue damage that would be caused by rupturing oocysts and continuously invading sporozoites. In contrast, an earlier study based on P. vivax infections in colonized An. dirus and An. minimus suggests that once oocysts are formed, the mosquito does not impose a ‘carrying capacity’ on the developing oocysts [47]. Here, in wild An. stephensi, the presence of melanized and unhealthy oocysts in the midgut strongly suggest a potential role of the mosquito’s immune system in controlling infection.
As seen in earlier studies [19, 41], in most feeding experiments, there was high variability in the oocyst load within individual mosquitoes of the same batch: Some were completely protected (zero oocysts) and some allowed large oocyst loads (>200). The genetic diversity of the wild mosquito population could be a critical factor that determines P. vivax infection load. Anopheles gambiae, the African malaria vector has been shown to exist in M and S forms based on its larval habitat and this adaptive divergence may influence the vector capacity and concomitant malaria epidemiology [64]. Future research on understanding the underlying traits that confer protection to Plasmodium infections in the wild would be of value.
Conclusions
Goa is an endemic area for P. vivax and An. stephensi is the major malaria vector in this region. This study describes the findings of 30 feeding experiments carried out with wild An. stephensi and natural isolates of P. vivax. The present results point to important variations in wild An. stephensi to resist P. vivax infections. Additional, controlled infection studies will help further mimic, define, and understand the natural interactions of the parasite and the vector in the wild in South Asia.
Abbreviations
- GMC:
-
Goa Medical College and Hospital
- MESA:
-
Malaria Evolution in South Asia
- ICEMR:
-
International Center of Excellence for Malaria Research
- NIMR:
-
National Institute of Malaria Research
- NIAID:
-
National Institute of Allergy and Infectious Diseases
- NIH:
-
US National Institutes of Health
- SMFA:
-
standard membrane feeding assay
- WBC:
-
white blood cell
- UW:
-
University of Washington
- DMID:
-
Division of Microbiology and Infectious Disease
References
Guerra CA, Howes RE, Patil AP, Gething PW, Van Boeckel TP, Temperley WH, et al. The international limits and population at risk of Plasmodium vivax transmission in 2009. PLoS Negl Trop Dis. 2010;4:e774.
Howes RE, Battle KE, Mendis KN, Smith DL, Cibulskis RE, Baird JK, et al. Global epidemiology of Plasmodium vivax. Am J Trop Med Hyg. 2016;95:15–34.
Hulden L, Hulden L, Heliovaara K. Natural relapses in vivax malaria induced by Anopheles mosquitoes. Malar J. 2008;7:64.
Anstey NM, Douglas NM, Poespoprodjo JR, Price RN. Plasmodium vivax: clinical spectrum, risk factors and pathogenesis. Adv Parasitol. 2012;80:151–201.
Bharti AR, Chuquiyauri R, Brouwer KC, Stancil J, Lin J, Llanos-Cuentas A, et al. Experimental infection of the neotropical malaria vector Anopheles darlingi by human patient-derived Plasmodium vivax in the Peruvian Amazon. Am J Trop Med Hyg. 2006;75:610–6.
Bousema T, Drakeley C. Epidemiology and infectivity of Plasmodium falciparum and Plasmodium vivax gametocytes in relation to malaria control and elimination. Clin Microbiol Rev. 2011;24:377–410.
Singh R, Singh DP, Savargaonkar D, Singh OP, Bhatt RM, Valecha N. Evaluation of SYBR green I based visual loop-mediated isothermal amplification (LAMP) assay for genus and species-specific diagnosis of malaria in P. vivax and P. falciparum endemic regions. J Vector Borne Dis. 2017;54:54–60.
Malleret B, Li A, Zhang R, Tan KS, Suwanarusk R, Claser C, et al. Plasmodium vivax: restricted tropism and rapid remodeling of CD71-positive reticulocytes. Blood. 2015;125:1314–24.
Mayor A, Alano P. Bone marrow reticulocytes: a Plasmodium vivax affair? Blood. 2015;25:1203–5.
Moreno-Perez DA, Ruiz JA, Patarroyo MA. Reticulocytes: Plasmodium vivax target cells. Biol Cell. 2013;105:251–60.
Vallejo AF, Garcia J, Amado-Garavito AB, Arevalo-Herrera M, Herrera S. Plasmodium vivax gametocyte infectivity in sub-microscopic infections. Malar J. 2016;15:48.
McKenzie FE, Wongsrichanalai C, Magill AJ, Forney JR, Permpanich B, Lucas C, et al. Gametocytemia in Plasmodium vivax and Plasmodium falciparum infections. J Parasitol. 2006;92:1281–5.
McKenzie FE, Jeffery GM, Collins WE. Gametocytemia and fever in human malaria infections. J Parasitol. 2007;93:627–33.
Zhu G, Xia H, Zhou H, Li J, Lu F, Liu Y, et al. Susceptibility of Anopheles sinensis to Plasmodium vivax in malarial outbreak areas of central China. Parasit Vectors. 2013;6:176.
Rios-Velasquez CM, Martins-Campos KM, Simoes RC, Izzo T, dos Santos EV, Pessoa FA, et al. Experimental Plasmodium vivax infection of key Anopheles species from the Brazilian Amazon. Malar J. 2013;12:460.
Gamage-Mendis AC, Rajakaruna J, Carter R, Mendis KN. Infectious reservoir of Plasmodium vivax and Plasmodium falciparum malaria in an endemic region of Sri Lanka. Am J Trop Med Hyg. 1991;45:479–87.
Graves PM, Burkot TR, Carter R, Cattani JA, Lagog M, Parker J, et al. Measurement of malarial infectivity of human populations to mosquitoes in the Madang area, Papua, New Guinea. Parasitology. 1988;96(Pt 2):251–63.
Coleman RE, Kumpitak C, Ponlawat A, Maneechai N, Phunkitchar V, Rachapaew N, et al. Infectivity of asymptomatic Plasmodium-infected human populations to Anopheles dirus mosquitoes in western Thailand. J Med Entomol. 2004;41:201–8.
Solarte Y, Manzano MR, Rocha L, Hurtado H, James MA, Arevalo-Herrera M, et al. Plasmodium vivax sporozoite production in Anopheles albimanus mosquitoes for vaccine clinical trials. Am J Trop Med Hyg. 2011;84:28–34.
Sattabongkot J, Maneechai N, Rosenberg R. Plasmodium vivax: gametocyte infectivity of naturally infected Thai adults. Parasitology. 1991;102:27–31.
Dowling MA, Shute GT. A comparative study of thick and thin blood films in the diagnosis of scanty malaria parasitaemia. Bull World Health Organ. 1966;34:249–67.
McKenzie FE, Prudhomme WA, Magill AJ, Forney JR, Permpanich B, Lucas C, et al. White blood cell counts and malaria. J Infect Dis. 2005;192:323–30.
McKenzie FE, Bossert WH. An integrated model of Plasmodium falciparum dynamics. J Theor Biol. 2005;232:411–26.
Lim C, Pereira L, Shardul P, Mascarenhas A, Maki J, Rixon J, et al. Improved light microscopy counting method for accurately counting Plasmodium parasitemia and reticulocytemia. Am J Hematol. 2016;91:852–5.
Lensen A, Bril A, van de Vegte M, van Gemert GJ, Eling W, Sauerwein R. Plasmodium falciparum: infectivity of cultured, synchronized gametocytes to mosquitoes. Exp Parasitol. 1999;91:101–3.
Vallejo AF, Rubiano K, Amado A, Krystosik AR, Herrera S, Arevalo-Herrera M. Optimization of a membrane feeding assay for Plasmodium vivax infection in Anopheles albimanus. PLoS Negl Trop Dis. 2016;10:e0004807.
da Silva AN, Santos CC, Lacerda RN, Machado RL, Povoa MM. Susceptibility of Anopheles aquasalis and An. darlingi to Plasmodium vivax VK210 and VK247. Mem Inst Oswaldo Cruz. 2006;101:547–50.
Gamage-Mendis AC, Rajakaruna J, Carter R, Mendis KN. Transmission blocking immunity to human Plasmodium vivax malaria in an endemic population in Kataragama, Sri Lanka. Parasite Immunol. 1992;14:385–96.
Ramsey JM, Salinas E, Rodriguez MH. Acquired transmission-blocking immunity to Plasmodium vivax in a population of southern coastal Mexico. Am J Trop Med Hyg. 1996;54:458–63.
Arevalo-Herrera M, Solarte Y, Zamora F, Mendez F, Yasnot MF, Rocha L, et al. Plasmodium vivax: transmission-blocking immunity in a malaria-endemic area of Colombia. Am J Trop Med Hyg. 2005;73:38–43.
Blandin SA, Wang-Sattler R, Lamacchia M, Gagneur J, Lycett G, Ning Y, et al. Dissecting the genetic basis of resistance to malaria parasites in Anopheles gambiae. Science. 2009;326:147–50.
Blanford S, Chan BH, Jenkins N, Sim D, Turner RJ, Read AF, et al. Fungal pathogen reduces potential for malaria transmission. Science. 2005;308:1638–41.
Scholte EJ, Knols BG, Takken W. Infection of the malaria mosquito Anopheles gambiae with the entomopathogenic fungus Metarhizium anisopliae reduces blood feeding and fecundity. J Invertebr Pathol. 2006;91:43–9.
Bousema T, Dinglasan RR, Morlais I, Gouagna LC, van Warmerdam T, Awono-Ambene PH, et al. Mosquito feeding assays to determine the infectiousness of naturally infected Plasmodium falciparum gametocyte carriers. PLoS ONE. 2012;7:e42821.
Kumar A, Chery L, Biswas C, Dubhashi N, Dutta P, Dua VK, et al. Malaria in South Asia: prevalence and control. Acta Trop. 2012;121:246–55.
Narayanasamy K, Chery L, Basu A, Duraisingh MT, Escalante A, Fowble J, et al. Malaria evolution in South Asia: knowledge for control and elimination. Acta Trop. 2012;121:256–66.
Rao MR. Foreword: international centers of excellence for malaria research. Am J Trop Med Hyg. 2015;93:1–4.
Chery L, Maki JN, Mascarenhas A, Walke JT, Gawas P, Almeida A, et al. Demographic and clinical profiles of Plasmodium falciparum and Plasmodium vivax patients at a tertiary care centre in southwestern India. Malar J. 2016;15:569.
Kumar A, Hosmani R, Jadhav S, de Sousa T, Mohanty A, Naik M, et al. Anopheles subpictus carry human malaria parasites in an urban area of Western India and may facilitate perennial malaria transmission. Malar J. 2016;15:124.
Thomas S, Ravishankaran S, Justin NA, Asokan A, Mathai MT, Valecha N, et al. Resting and feeding preferences of Anopheles stephensi in an urban setting, perennial for malaria. Malar J. 2017;16:111.
Joshi D, Choochote W, Park MH, Kim JY, Kim TS, Suwonkerd W, et al. The susceptibility of Anopheles lesteri to infection with Korean strain of Plasmodium vivax. Malar J. 2009;8:42.
Riley RS, Ben-Ezra JM, Goel R, Tidwell A. Reticulocytes and reticulocyte enumeration. J Clin Lab Anal. 2001;15:267–94.
Aguilar R, Dong Y, Warr E, Dimopoulos G. Anopheles infection responses; laboratory models versus field malaria transmission systems. Acta Trop. 2005;95:285–91.
Basseri HR, Doosti S, Akbarzadeh K, Nateghpour M, Whitten MM, Ladoni H. Competency of Anopheles stephensi mysorensis strain for Plasmodium vivax and the role of inhibitory carbohydrates to block its sporogonic cycle. Malar J. 2008;7:131.
Thongsahuan S, Baimai V, Junkum A, Saeung A, Min GS, Joshi D, et al. Susceptibility of Anopheles campestris-like and Anopheles barbirostris species complexes to Plasmodium falciparum and Plasmodium vivax in Thailand. Mem Inst Oswaldo Cruz. 2011;106:105–12.
Moreno M, Tong C, Guzman M, Chuquiyauri R, Llanos-Cuentas A, Rodriguez H, et al. Infection of laboratory-colonized Anopheles darlingi mosquitoes by Plasmodium vivax. Am J Trop Med Hyg. 2014;90:612–6.
Zollner GE, Ponsa N, Garman GW, Poudel S, Bell JA, Sattabongkot J, et al. Population dynamics of sporogony for Plasmodium vivax parasites from western Thailand developing within three species of colonized Anopheles mosquitoes. Malar J. 2006;5:68.
Zhang C, Shi G, Cheng P, Wang H, Liu H, Liu L, et al. A reassessment of the artificial infection of three predominant mosquito species with Plasmodium vivax in Shandong Province, China. J Vector Borne Dis. 2016;53:208–14.
Sattler PW, Hilburn LR, Davey RB, George JE, Rojas Avalos JB. Genetic similarity and variability between natural populations and laboratory colonies of North American Boophilus (Acari: Ixodidae). J Parasitol. 1986;72:95–100.
Lainhart W, Bickersmith SA, Moreno M, Rios CT, Vinetz JM, Conn JE. Changes in genetic diversity from field to laboratory during colonization of Anopheles darlingi Root (Diptera: Culicidae). Am J Trop Med Hyg. 2015;93:998–1001.
Norris DE, Shurtleff AC, Toure YT, Lanzaro GC. Microsatellite DNA polymorphism and heterozygosity among field and laboratory populations of Anopheles gambiae ss (Diptera: Culicidae). J Med Entomol. 2001;38:336–40.
Billker O, Shaw MK, Margos G, Sinden RE. The roles of temperature, pH and mosquito factors as triggers of male and female gametogenesis of Plasmodium berghei in vitro. Parasitology. 1997;115:1–7.
Kar PK, Dua VK, Gupta NC, Gupta A, Dash AP. Plasmodium falciparum gametocytaemia with chloroquine chemotherapy in persistent malaria in an endemic area of India. Indian J Med Res. 2009;129:299–304.
Robert V, Read AF, Essong J, Tchuinkam T, Mulder B, Verhave JP, et al. Effect of gametocyte sex ratio on infectivity of Plasmodium falciparum to Anopheles gambiae. Trans R Soc Trop Med Hyg. 1996;90:621–4.
Robert V, Sokhna CS, Rogier C, Ariey F, Trape JF. Sex ratio of Plasmodium falciparum gametocytes in inhabitants of Dielmo, Senegal. Parasitology. 2003;127:1–8.
Burkot TR, Williams JL, Schneider I. Infectivity to mosquitoes of Plasmodium falciparum clones grown in vitro from the same isolate. Trans R Soc Trop Med Hyg. 1984;78:339–41.
Sowunmi A, Balogun T, Gbotosho GO, Happi CT, Adedeji AA, Fehintola FA. Activities of amodiaquine, artesunate, and artesunate-amodiaquine against asexual- and sexual-stage parasites in falciparum malaria in children. Antimicrob Agents Chemother. 2007;51:1694–9.
Talman AM, Paul RE, Sokhna CS, Domarle O, Ariey F, Trape JF, et al. Influence of chemotherapy on the Plasmodium gametocyte sex ratio of mice and humans. Am J Trop Med Hyg. 2004;71:739–44.
Paul RE, Brey PT, Robert V. Plasmodium sex determination and transmission to mosquitoes. Trends Parasitol. 2002;18:32–8.
Paul RE, Coulson TN, Raibaud A, Brey PT. Sex determination in malaria parasites. Science. 2000;287:128–31.
Reece SE, Ramiro RS, Nussey DH. Plastic parasites: sophisticated strategies for survival and reproduction? Evol Appl. 2009;2:11–23.
Mitri C, Thiery I, Bourgouin C, Paul RE. Density-dependent impact of the human malaria parasite Plasmodium falciparum gametocyte sex ratio on mosquito infection rates. Proc Biol Sci. 2009;276:3721–6.
Gamage-Mendis AC, Rajakaruna J, Weerasinghe S, Mendis C, Carter R, Mendis KN. Infectivity of Plasmodium vivax and P. falciparum to Anopheles tessellatus; relationship between oocyst and sporozoite development. Trans R Soc Trop Med Hyg. 1993;87:3–6.
White BJ, Lawniczak MK, Cheng C, Coulibaly MB, Wilson MD, Sagnon N, et al. Adaptive divergence between incipient species of Anopheles gambiae increases resistance to Plasmodium. Proc Natl Acad Sci USA. 2011;108:244–9.
Authors’ contributions
PBN, AKM, NV, AK, and PKR designed the study. LC, SKM, AK, NV, and PKR administered the study. PBN, AKM, SB, SV, SBH, MD, JW, and AM carried out the experiments. PBN, AKM, AK, and PKR analyzed the data. PBN, AKM, LC, NV, AK, and PKR wrote and edited the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors thank all participating malaria patients at the Goa Medical College and Hospital who volunteered for this study, and Dr. Sachin Shinde, Special Secretary (Health) and Administrator (GMC), for his support. The authors are most grateful for the administrative and scientific guidance provided by the MESA-ICEMR Scientific Advisory Group, including the Government of India representatives Dr. Rashmi Arora, Dr. Shiv Lal and Dr. P Joshi and US NIH Programme Officer Dr. Malla Rao. This manuscript was approved by the publication committee of NIMR and bears Approval No. 022/2017.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article.
Ethics approval and consent to participate
The human subjects protocol and consent forms for enrollment of Plasmodium positive individuals presenting to Goa Medical College and Hospital were approved by the institutional review boards of the Division of Microbiology and Infectious Diseases at the US National Institute of Allergy and Infectious Diseases (DMID 11-0074), GMC (no number assigned), and the University of Washington (42271).
Funding
This work was supported by the US NIAID MESA-ICEMR Program Project U19 AI089688 (Programme Director, Pradipsinh K Rathod of the University of Washington, Seattle, WA, USA), and by the Government of India [The National Institute of Malaria Research (NIMR) and the Indian Council of Medical Research (ICMR)].
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Balabaskaran Nina, P., Mohanty, A.K., Ballav, S. et al. Dynamics of Plasmodium vivax sporogony in wild Anopheles stephensi in a malaria-endemic region of Western India. Malar J 16, 284 (2017). https://doi.org/10.1186/s12936-017-1931-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-017-1931-8