
Abstract
Effective malaria control requires information on both the geographical distribution of malaria risk and the effectiveness of malaria interventions. The current standard for estimating malaria infection and impact indicators are household cluster surveys, but their complexity and expense preclude frequent and decentralized monitoring. This paper reviews the historical experience and current rationale for the use of schools and school children as a complementary, inexpensive framework for planning, monitoring and evaluating malaria control in Africa. Consideration is given to (i) the selection of schools; (ii) diagnosis of infection in schools; (iii) the representativeness of schools as a proxy of the communities they serve; and (iv) the increasing need to evaluate interventions delivered through schools. Finally, areas requiring further investigation are highlighted.
Similar content being viewed by others


Background
The burden of malaria in some areas of sub-Saharan Africa (SSA) has started to decline over recent years: analyses of hospital admission data provide evidence of declining morbidity and mortality in Kenya [1, 2], The Gambia [3], South Africa [4], Zanzibar [5], and Eritrea [6]. Such reductions have been variously attributed to the expanded distribution of insecticide-treated nets (ITNs), changing first-line treatments to artemisinin combination therapy (ACT) and increasing access to it, and the renewed use of indoor residual spraying (IRS). There are, however, fewer reports on the impact of these interventions on malaria transmission [5, 7]. This is partly due to the technical and ethical difficulties associated with quantifying transmission using vector-based indices, such as the entomological inoculation rate [8]. A more frequently used malariometric index is the Plasmodium falciparum parasite rate (Pf PR): the proportion of surveyed persons harbouring parasites in their peripheral blood. The Pf PR among children aged 2-10 years provides an indirect quantitative measure of transmission intensity across a range of malaria endemicities [9, 10]. Historically, the measurement of Pf PR had important roles during the first phase of the Global Malaria Elimination Programme (GMEP) and was subsequently used to monitor progress and verify interruption of transmission [11]. Moreover, contemporary maps of Pf PR can provide important information for national malaria control programmes by targeting interventions according to endemicity, thus cost-effectively targeting resources for malaria control [12, 13].
Currently, the most robust sampling framework for national malaria surveys are household cluster surveys, including: Demographic and Health Surveys [14], the Multiple Indicator Cluster Surveys [15], and Malaria Indicator Surveys (MIS) [16]. All of these surveys collect household-level information on malaria intervention coverage, patterns of anti-malarial use, and in selected MIS, on the prevalence of malaria infection and anaemia among pregnant women and children under five years of age. However, estimating Pf PR among these age groups is not optimal as pregnant women sequester infections [17] and infection prevalence in very young children is modified by a variety of factors including presence of maternal antibodies [18, 19]. More importantly, national cluster surveys are expensive, time-consuming, technically complicated to undertake, and sampling is typically powered to provide only national or in some instances, first-level administrative unit (e.g. State or Province) representative estimates of malaria risk and intervention coverage. Such limitations preclude frequent monitoring and evaluation, beyond the first administrative level, hindering decentralized planning and allocation of resources for targeted control. Increasing the frequency of monitoring risk enables prompt feedback of intervention effectiveness, helping control programmes to adapt and improve control strategies. Across much of SSA, routine collection of malaria information at district levels currently focuses on passive case detection data on suspected malaria cases compiled by health facilities. However, these data are almost universally incomplete [20], lack diagnostic precision [21], and are rarely used for planning purposes. Because of these shortcomings, alternative sampling methods for monitoring malaria risk and intervention coverage are being explored, including household lot quality assurance sampling [22, 23] and expanded programme of immunization (EPI) contact sampling [24, 25]. This article reviews the historical experience and current rationale for the use of schools and school children as a complementary, inexpensive framework for malaria planning, monitoring and evaluation.
The history of school malaria surveys
Conducting school malaria surveys is not a new approach in malariology. School surveys were a common feature of early approaches to malaria reconnaissance and control [26, 27] (Figure 1). During the 1920-40s, large-scale school parasite surveys were frequently conducted in the United States and used to track the decline of malaria in the country: between 1942-43, for example, blood films were collected from 104,613 school children in seventeen states, with only 201 were found to be infected [28]. In the interests of time, survey investigations involved the examination of splenomegaly, limiting the collection of blood smears to children with enlarged spleens and/or a random proportion of children without palpable spleens. Such a screening approach was for instance adopted in nationally representative school malaria surveys undertaken in Cuba, 1935-1942 [29] and El Salvador, 1938-1940 [30].

Historical recommendations for planning and conducting school malaria parasite surveys [26].
School surveys were also an important component of early, particularly colonial, malaria reconnaissance and monitoring in Africa. In his survey of malaria in Southern Rhodesia, Alves reports results of school surveys conducted between 1937 and 1948 [31], while in the seminal 1967 book Malaria in Tanzania by Clyde [32] many of the reports of parasite prevalence were based on surveys of school children. In Uganda, as part of the pre-eradication programme of the 1960s, the nationwide distribution of different Plasmodium species was mainly based on school surveys conducted in different ecological settings across the country [33]. In Kenya, a recent assembly of parasite prevalence data found that over 50% of surveys conducted between 1975 and 1989 were Ministry of Health surveys of school children, which previously were a routine activity of the Division of Vector Borne Diseases (Noor et al. in preparation). School surveys were also an important component of monitoring the impact of malaria control: for example, the impact on malaria and anaemia of IRS in the Taveta-Pare area of Kenya and Tanzania during 1954 and 1959 was evaluated, in part, through school surveys [34, 35]. Seemingly, however, school surveys fell out of favour, presumably due to financing constraints and a shift in the goals of control programmes from malaria elimination to morbidity control. More recently, school parasite surveys have been included in rapid assessments of malaria in urban SSA [36].
Advantages of school-based malaria surveillance
The practical advantages of sampling children at school are clear: identification and selection of individuals is simplified, compliance is high, and costs are reduced, since only a fraction of the population is examined. In addition, ministries of education are increasingly developing or upgrading national school databases using geographical information systems (GIS). This allows incorporation of information on schools location and enrolment into a single database, and the use of geo-statistical methods to model risks between schools and across unsampled schools.
There are additionally important epidemiological reasons for sampling children who attend school. Historically, malaria endemicity was defined on the basis of Pf PR among children aged 2-10 years and geographical reconnaissance of malaria was recommended in all areas prior to a control programme launching into an attack phase of the GMEP [11, 33, 34]. Recent mathematical models of malaria transmission dynamics indicate that EIR determines both the rate at which Pf PR rises during early childhood and the age at which maximum Pf PR is attained [9, 10]. Age-stratified studies in varying transmission settings reveal that Pf PR consistency has a convex relationship with age, with Pf PR rapidly rising in among young children, attaining a maximum within the 5-10 year old age class, and declines among adolescents and young adults, thereafter maintaining a relatively stable low value throughout adulthood (Figure 2). Such consistency in the relationship between Pf PR and age settings permits age-standardization of available Pf PR estimates to the two to 10 year age range on the basis of catalytic conversion models [9], although estimates are most precise when the majority of the sampled population are within this age range.

The relationship between age and Plasmodium falciparum parasite rate ( Pf PR) [Adapted from data provided in ref [9]]. Each line represents the age profile for population living in varying transmission settings: South and Central Somalia (Pf PR among 5-14 year olds (Pf PR5-14) = 24.6%) [74]; Kilifi, coastal Kenya (Pf PR5-14 = 37.5%) [75]; Navrongo, Ghana (Pf PR5-14 = 66.9%) [76] and Kilombero, Tanzania (PfPR5-14 = 83.7%) [77]. Shaded box indicates typical age range of Primary school children in Africa (5-14 years).
Monitoring intervention coverage
School-based surveys may potentially provide useful proximate estimates of the coverage of community-wide malaria interventions. Interviewing African school children by teachers is a well accepted and cost-effective approach for determining the prevalence of urinary schistosomiasis [37] and may potentially be used to monitor mosquito net coverage. Studies in Uganda show that schoolchildren reliably reported net ownership and the proportion of children protected in their households, hence providing a cheap and relatively fast method to estimate coverage at the community level [38, 39]. The additional work involved in administering questionnaires to the pupils did not appear to pose any problems to the teachers, and importantly, school children were able to differentiate between treated and untreated nets [38]; though this will become less relevant as the use of long-lasting insecticide nets (LLINs) increases. The questionnaire approach may also be extended to monitoring household IRS coverage. By contrast, school children are unlikely to provide coverage information on the quality of disease management and treatment practices among their younger siblings or their pregnant mothers or sisters, and household surveys remain most relevant here.
Selection of schools
The question as to how many schools to be included in malaria surveillance in a given area is similar to that faced by all large-scale surveys, and needs to be guided by both statistical and practical considerations. The appropriate sample size will depend on the expected Pf PR, the desired precision of Pf PR estimates, and the intrinsic variation of Pf PR between schools [40]. Practical constraints include availability of financial and human resources as well as accessible of schools.
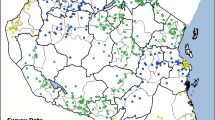
In traditional large-scale surveys, sampling units are typically selected on the basis of population proportionate sampling. Because there is need to define the geographical variation in Pf PR, a more spatially explicit sampling design may be required to capture spatial heterogeneities. Spatial sampling is an emerging area of scientific investigation [41, 42], for which almost no work exists for parasite epidemiology. However, advances in GIS coupled with increasing availability of spatially-referenced national school databases provide an important opportunity for constructing efficient spatial sampling designs. In Kenya, for example, there are over 17,727 government, day mixed schools, which can constitute the sampling frame and these have all been recently geo-located using hand-held global positioning systems [43]. Schools can serve as the primary sampling unit and children within selected schools as secondary sampling units. By way of example, Figure 3a presents a representative national sample of 416 schools (3% of total number of schools) representing 41,600 children. Schools were selected proportionate to the number of schools in each district. The total estimated financial cost of such a survey is US$ 424,808, or US$ 1,021 per school surveyed (Figure 3b). In each school, 10 boys and 10 girls (plus two reserve children per school) from each class are selected using random number tables. By comparison, the nationwide MIS conducted in Kenya in 2007 was based on a two stage-stage cluster sample of 6,854 households surveyed in 199 census enumeration areas (Figure 3c), randomly selected from all regions and urban areas of the country. The survey included 33,534 persons, including 6,842 children aged 0-4 years. The corresponding survey costs excluding training, piloting and technical costs are estimated to be US$ 649,930, or US$ 3,299 per cluster sampled (Figure 3d).

Developing a national school-based malaria information system in Kenya, 2009. (A) geographical location of the 416 sentinel schools in a national school malaria survey and all Government of Kenya (GoK) primary schools; and (B) the estimated personal, laboratory consumable, data management and logistics costs to implement a national school malaria survey in Kenya. (C) Geographical location of sampled 197 clusters in the 2007 Kenya Malaria Indicator Survey and all communities in Kenya; and (D) MIS costs, excluding training and piloting and technical support.
School surveys may be further simplified by the use of lot quality assurance sampling (LQAS) [44], which has the potential to classify geographical areas according to (i) specified categories of infection prevalence to target interventions [45] or (ii) establish whether a specified coverage target has been reached [46]. Although LQAS has been extensively used to monitor coverage of vaccination programmes [23], there are few documented applications in malaria monitoring and surveillance. Current applications include community LQAS surveys for the detection of epidemics in the Madagascan highlands [45] and large country LQAS surveys of malaria intervention coverage as part of the World Bank's Malaria Booster Project in Nigeria [47]. Whatever the sample design, the usefulness of national school surveys will crucially depend on a number of issues, including the accuracy of diagnosis and how representativeness schools are of the wider community, which are now considered.
Diagnosing infection in schools
The most common and widely used technique to detect Plasmodium sp. in circulating peripheral blood is microscopy. This method is, however, only as reliable as the quality of the blood slide preparation and equipment, skills of the microscopist and quality control [48, 49]. An alternative and increasingly used diagnostic method are rapid diagnostic tests (RDTs). A number of products are now commercially available, detecting different parasite protein products: P. falciparum-specific histadine-rich protein (HRP) or species-specific isotypes of lactate dehydrogenase [50]. When stored and used correctly RDTs can have an accuracy that exceeds 95% sensitivity and 90% specificity for detection of P. falciparum when compared to expert microscopy even at relatively low parasite densities [51]. The tests with the highest sensitivity are typically HRP-based test since Pf-HRP can persist for two weeks after parasite clearance. Although Pf-HRP-based tests are more likely to generate false positives, which has implications on their use for case-management [52], these tests are still valuable during community prevalence surveys which aim to estimate parasite exposure as a measure of transmission intensity. The ease with which RDTs can be used and the short time in which they provide a diagnosis means that they can readily be incorporated into routine school malaria surveys, with identified positives treated on site. Recent experience in Kenya shows that the use of RDTs in 65 schools, compared to validated microscopy results, has a sensitivity of 98.9% and a specificity of 84.9% (Brooker et al. unpublished). A more cost-effective approach to improve precision is to use RDTs for field-based diagnosis in areas of low malaria transmission, with microscopy of all RDT-positive samples and a corresponding random selection of RDT-negatives undertaken by quality assured microscopists unaware of the RDT results. This stepwise approach to diagnosis has parallels with the two-stage approach of spleen examination and blood samples adopted in the USA, Cuba and El Salvador in the 1930s [29, 30]. In areas of high transmission in Africa, the use of RDTs alone is advocated. Other diagnostic techniques are being explored to measure changes in infection exposure with time, notably serological measures of anti-malarial antibodies that persist for months or years after infection [53–56]. These approaches will become more valuable where school children may serve as sentinel surveillance to define malaria elimination progress in their communities.
Representativeness of schools
An important determinant of the representativeness of schools of the communities they serve is the level and equity of school enrollment. Current commitment of national governments and donors to achieving universal primary school participation [57], means that school enrollment rates are increasing. This has been most pronounced in SSA where since 2000 there has been a 52% increase in pupil enrollment [58]. Across the continent, however, there remains substantial variation in enrollment levels, and this will impact on the representativeness of schools. School enrollment in East Africa is characterized by high enrollment and primary completion rates [59]: for example, in Tanzania in 2007, net primary enrolment was 98% and primary completion rate 85% [60]. Evidence suggests that in such settings the majority of non-enrolled school age children have at least one sibling attending school, and that neither socio-economic status nor maternal education is associated with higher enrolment [59, 61]. By contrast, in Central and West Africa, where both enrollment and completion rates are low, there are large differentials in enrollment by socio-economic and health status: for example, in Burkina Faso, only 18% from the poorest households enter grade 1 compared to 70% from the richest household [59]; and in Ghana, adolescent non-enrolled boys were more heavily infected with helminth infections and more likely to be anaemic than enrolled adolescent boys [62]. Such wealth differentials in enrollment have obvious implications for the schools representativeness of schools for the community at large where enrollment, infection and intervention use are affected by poverty. Representativeness will also depend on the types of schools sampled. In certain settings, boarding schools, single sex schools (such as Koranic schools), or non-government (private and parochial) schools may predominate; for example, parochial schools in Demographic Republic of Congo; and Koranic schools in Senegal. In such settings, it may be appropriate include non-government schools in the sampling frame. Representativeness of school surveys is likely to be greatest in those malaria endemic countries with the highest enrollment and completion rates, namely eastern and southern African countries (Figure 4). This will, in turn, help improve the coverage of Africa-wide empirical data to develop mapped extents of P. falciparum transmission intensity [63].

Representativeness of school children for malaria surveillance in Africa. (a) enrollment and (b) completion rates by country. Countries shaded grey indicate an absence of malaria transmission: Algeria, Egypt, Lesotho, Libya, Morocco, Tunisia and Western Sahara. Net enrollment ratio is the ratio of children of official school age who are enrolled in school to the population of the corresponding official school age. Primary completion rate is the percentage of students completing the last year of primary school. It is calculated by taking the total number of students in the last grade of primary school, minus the number of repeaters in that grade, divided by the total number of children of official graduation age. Data source: World Development Indicators [60]. (c) Geographical distribution of malaria survey data (n = 5307) currently included in the Malaria Atlas Project http://www.map.ox.ac.uk[63].
Finally, the representativeness of Pf PR data collected through school surveys may depend on size of the catchment area of schools. If, for example, a school's catchment area is large, it may include villages with varying malaria ecologies; if the catchment area is small, then the derived Pf PR is likely to be more representative of the immediate community. Little is known about the size and structure of school catchment areas in Africa, and this merits further investigation. It is known, however, that there is only a minor influence of household distance to schools on enrollment [64].
Combing surveillance and intervention in schools
There is increasing recognition that universal mosquito net coverage is one of the most effective malaria prevention tools, such that LLINs should be distributed freely or should be highly subsidized and used by all community members, including school children [65]. In addition, school children themselves are increasingly becoming the targets of malaria control [66]. As the intensity of malaria transmission declines, it is suggested that clinical immunity will be acquired more slowly, with disease burdens shifting into older age groups, including school children [67, 68]. This epidemiological transition is occurring at a time when more children than ever before are attending school. Consequently, there is growing interest in identifying malaria interventions that can be delivered through the existing school system [69], and control strategies for malaria in schools need to be formulated in relation to epidemiological patterns of infection and disease, as well as intervention cost-effectiveness. Monitoring and evaluation of school-based interventions will be essential to determine impacts of interventions on levels of infection, disease and school absenteeism. As such, schools become vehicles for surveillance of infection risks in the communities they serve and targets for intervention delivery. This too has a historical precedent: in Kenya, for example, during the 1970s and 1980s schools were used as a means to rapidly and routinely estimate infection risks across the country using technicians from regional offices of the Ministry of Health's Division of Vector Borne Diseases [70]. On completing these surveys staff provided chloroquine treatment for all infected children. Elsewhere in Africa, historical school-based delivery of malaria chemoprophylaxis was associated with significant reductions in malaria-related morbidity and mortality, and improvements in educational outcomes [71–73].
Future directions
The routine surveillance of malaria infection is uncommon in any national malaria strategy in Africa and it is notable that countries in southern Africa have identified elimination as an achievable immediate target without any mapped reconnaissance of malaria risk. It is argued that surveys of school attending children provide a rapid, cheap and sustainable platform to assemble information on malaria risk among communities, and that in time, children attending school will increasingly become the focus of intervention as the epidemiology of malaria risk changes. This is not a new approach but its significance has re-emerged during a renewed international interest in malaria control and elimination. The use of schools as sentinels does however require further validation and optimization. Notable areas of investigation that require attention include studies on the representativeness of schools and how this varies in relation to levels of school enrolment as well as malaria endemicity; the potential sampling and diagnostic biases introduced when transmission intensity declines and all new infections become clinical events resulting in absenteeism; and the validity of children's reporting on intervention, especially mosquito net, use among household members. However, it is likely that as pupil enrollment continues to expand schools will increasingly provide a representative sample of community events. Furthermore, the technical capacity to conduct school malaria surveys already exists in most SSA countries, and engaging the health and education sectors in malaria control promotes inter-sectoral collaboration at national levels.
References
Okiro EA, Hay SI, Gikandi PW, Sharif SK, Noor AM, Peshu N, Marsh K, Snow RW: The decline in paediatric malaria admissions on the coast of Kenya. Malar J. 2007, 6: 151-10.1186/1475-2875-6-151.
O'Meara WP, Bejon P, Mwangi TW, Okiro EA, Peshu N, Snow RW, Newton CR, Marsh K: Effect of a fall in malaria transmission on morbidity and mortality in Kilifi, Kenya. Lancet. 2008, 372: 1555-1562. 10.1016/S0140-6736(08)61655-4.
Ceesay SJ, Casals-Pascual C, Erskine J, Anya SE, Duah NO, Fulford AJ, Sesay SS, Abubakar I, Dunyo S, Sey O, Palmer A, Fofana M, Corrah T, Bojang KA, Whittle HC, Greenwood BM, Conway DJ: Changes in malaria indices between 1999 and 2007 in The Gambia: a retrospective analysis. Lancet. 2008, 372: 1545-1554. 10.1016/S0140-6736(08)61654-2.
Barnes KI, Durrheim DN, Little F, Jackson A, Mehta U, Allen E, Dlamini SS, Tsoka J, Bredenkamp B, Mthembu DJ, White NJ, Sharp BL: Effect of artemether-lumefantrine policy and improved vector control on malaria burden in KwaZulu-Natal, South Africa. PLoS Med. 2005, 2: e330-10.1371/journal.pmed.0020330.
Bhattarai A, Ali AS, Kachur SP, Martensson A, Abbas AK, Khatib R, Al-Mafazy AW, Ramsan M, Rotllant G, Gerstenmaier JF, Molteni F, Abdulla S, Montgomery SM, Kaneko A, Bjorkman A: Impact of artemisinin-based combination therapy and insecticide-treated nets on malaria burden in Zanzibar. PLoS Med. 2007, 4: e309-10.1371/journal.pmed.0040309.
Nyarango PM, Gebremeskel T, Mebrahtu G, Mufunda J, Abdulmumini U, Ogbamariam A, Kosia A, Gebremichael A, Gunawardena D, Ghebrat Y, Okbaldet Y: A steep decline of malaria morbidity and mortality trends in Eritrea between 2000 and the effect of combination of control methods. Malar J. 2006, 5: 33-10.1186/1475-2875-5-33.
Sharp BL, Kleinschmidt I, Streat E, Maharaj R, Barnes KI, Durrheim DN, Ridl FC, Morris N, Seocharan I, Kunene S, JJ LAG, Mthembu JD, Maartens F, Martin CL, Barreto A: Seven years of regional malaria control collaboration--Mozambique, South Africa, and Swaziland. Am J Trop Med Hyg. 2007, 76: 42-47.
Drakeley C, Schellenberg D, Kihonda J, Sousa CA, Arez AP, Lopes D, Lines J, Mshinda H, Lengeler C, Armstrong Schellenberg J, Tanner M, Alonso P: An estimation of the entomological inoculation rate for Ifakara: a semi-urban area in a region of intense malaria transmission in Tanzania. Trop Med Int Health. 2003, 8: 767-774. 10.1046/j.1365-3156.2003.01100.x.
Smith DL, Guerra CA, Snow RW, Hay SI: Standardizing estimates of the Plasmodium falciparum parasite rate. Malar J. 2007, 6: 131-10.1186/1475-2875-6-131.
Smith DL, McKenzie FE, Snow RW, Hay SI: Revisiting the basic reproductive number for malaria and its implications for malaria control. PLoS Biol. 2007, 5: e42-10.1371/journal.pbio.0050042.
Hay SI, Smith DL, Snow RW: Measuring malaria endemicity from intense to interrupted transmission. Lancet Infect Dis. 2008, 8: 369-378. 10.1016/S1473-3099(08)70069-0.
Hay SI, Snow RW: The malaria Atlas Project: developing global maps of malaria risk. PLoS Med. 2006, 3: e473-10.1371/journal.pmed.0030473.
Snow RW, Marsh K, Le Sueur D: The need for maps of transmission intensity to guide malaria control in Africa. Parasitology Today. 1996, 12: 455-457. 10.1016/S0169-4758(96)30032-X.
Demographic and Health Surveys. [http://www.measuredhs.com]
UNICEF: Monitoring the situation of children and women. Multiple indicator cluster survey manual. 2006, New York: United Nations Children's Fund
Roll Back Malaria Monitoring and Evaluation Reference Group WHO, United Nations Children's Fund, MEASURE DHS, MEASURE Evaluation, and U.S. Centers for Disease Control and Prevention: Malaria indicator survey: basic documentation for survey design and implementation/Roll Back Malaria Monitoring and Evaluation Reference Group. 2005, Calverton, Maryland: MEASURE Evaluation
Brabin BJ: An analysis of malaria in pregnancy in Africa. Bulletin of the World Health Organization. 1983, 61: 1005-1016.
Covell G: Congenital malaria. Tropical Diseases Bulletin. 1950, 47: 1147-1167.
Hviid L, Staalsoe T: Malaria immunity in infants: a special case of a general phenomenon. Trends in Parasitology. 2004, 20: 66-72. 10.1016/j.pt.2003.11.009.
Gething PW, Noor AM, Gikandi PW, Hay SI, Nixon MS, Snow RW, Atkinson PM: Developing geostatistical space-time models to predict outpatient treatment burdens from incomplete national data. Geogr Anal. 2008, 40: 167-188. 10.1111/j.1538-4632.2008.00718.x.
Reyburn H, Mbatia R, Drakeley C, Carneiro I, Mwakasungula E, Mwerinde O, Saganda K, Shao J, Kitua A, Olomi R, Greenwood BM, Whitty CJ: Overdiagnosis of malaria in patients with severe febrile illness in Tanzania: a prospective study. British Medical Journal. 2004, 329: 1212-10.1136/bmj.38251.658229.55.
Gerstl S, Cohuet S, Edoh K, Brasher C, Lesage A, Guthmann JP, Checchi F: Community coverage of an antimalarial combination of artesunate and amodiaquine in Makamba Province, Burundi, nine months after its introduction. Malar J. 2007, 6: 94-10.1186/1475-2875-6-94.
Robertson SE, Valadez JJ: Global review of health care surveys using lot quality assurance sampling (LQAS), 1984-2004. Soc Sci Med. 2006, 63: 1648-1660. 10.1016/j.socscimed.2006.04.011.
Bennett S, Woods T, Liyanage WM, Smith DL: A simplified general method for cluster-sample surveys of health in developing countries. World Health Stat Q. 1991, 44: 98-106.
Turner AG, Magnani RJ, Shuaib M: A not quite as quick but much cleaner alternative to the Expanded Programme on Immunization (EPI) Cluster Survey design. Int J Epidemiol. 1996, 25: 198-203. 10.1093/ije/25.1.198.
Boyd MF, Putnam P, Christophers R: Surveys: epidemiologic and entomologic. Malariology A comprehensive survey of all aspects of this group of diseases from a global standpoint. Edited by: Boyd MF. 1949, Philadelphia and London: W.B. Saunders, 831-873.
Russell PF, West LS, Manwell RD: Malaria surveys. Practical Malariology. 1946, Philadelphia and London: W.B. Saunders, 378-403.
Faust EC: Malaria incidence in North America. Malariology A comprehensive survey of all aspects of this group of diseases from a global standpoint. Edited by: Boyd MF. 1949, Philadelphia and London: W.B. Saunders, 749-763.
Carr HP, Hill RB: A malaria survey of Cuba. American Journal of Tropical Medicine & Hygiene. 1942, s1-22: 587-607.
Sutter VA, Zuniga H: A malaria survey of El Salvador, Central America. Ameican Journal of Tropical Medicine and Hygiene. 1942, 22: 387-398.
Alves W: Malaria parasite rates in Southern Rhodesia: May-September 1956. Bulletin of the World Health Organization. 1958, 19: 69-74.
Clyde DF: Malaria in Tanzania. 1967, London: Oxford University Press
Onori E: Distribution of Plasmodium ovale in the eastern, western and northern regions of Uganda. Bulletin of the World Health Organization. 1967, 37: 665-668.
Draper CC: Effect of malaria control on haemoglobin levels. British Medical Journal. 1960, 1 (5184): 1480-1842.
Draper CC, Smith A: Malaria in the Pare area of Tanganyika. Part II. Effects of three years' spraying of huts with dieldrin. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1960, 54: 342-357.
Wang SJ, Lengeler C, Smith TA, Vounatsou P, Cisse G, Diallo DA, Akogbeto M, Mtasiwa D, Teklehaimanot A, Tanner M: Rapid urban malaria appraisal (RUMA) in sub-Saharan Africa. Malar J. 2005, 4: 40-
Lengeler C, Utzinger J, Tanner M: Questionnaires for rapid screening of schistosomiasis in sub-Saharan Africa. Bull World Health Organ. 2002, 80: 235-242.
Ndyomugyenyi R, Kroeger A: Using schoolchildren's reports of bed net use monitored by schoolteachers as a proxy of community coverage in malaria endemic areas of Uganda. Trop Med Int Health. 2007, 12: 230-237.
Kilian A, Byamukama W: Surveillance of mosquito net coverage using primary school based data collection in the districts of Kaborole, Kamwenge and Kyenjojo, 2000-2004. Gesellschaft fur Technishe Zusammenarbeit (GTZ) and District Health Services Kabarole District. Final report. 2005
Jovani R, Tella JL: Parasitic prevalence and sample size: misconceptions and solutions. Trends in Parasitology. 2006, 22: 214-218.
Kumar N: Spatial Sampling Design for a Demographic and Health Survey. Population Research and Policy Review. 2007, 26: 581-599.
Stevens DL, Olsen AR: Spatially balanced sampling of natural resources. Journal of of the American Statistical Association. 2004, 99: 262-278.
Ministry of Education: Inception Report. Consultancy on development of a GIS database of learning Institutions (School mapping exercise). 2008, Nairobi: Oakar Services Ltd
Lemeshow S, Taber S: Lot quality assurance sampling: single- and double-sampling plans. World Health Stat Q. 1991, 44: 115-132.
Rabarijaona L, Rakotomanana F, Ranaivo L, Raharimalala L, Modiano D, Boisier P, De Giorgi F, Raveloson N, Jambou R: Validity of Lot Quality Assurance Sampling to optimize falciparum malaria surveys in low-transmission areas. Trans R Soc Trop Med Hyg. 2001, 95: 267-269.
Lanata CF, Stroh G, Black RE, Gonzales H: An evaluation of lot quality assurance sampling to monitor and improve immunization coverage. Int J Epidemiol. 1990, 19: 1086-1090.
Hedt BL, Olives C, Pagano M, Valadez JJ: Large country-Lot Quality Assurance Sampling: a new method for rapid monitoring and evaluation of health, nutrition and population programs at sub-national levels. Health, Nutrition and Population Discussion Paper. 2008, Washington D.C.: World Bank
O'Meara WP, McKenzie FE, Magill AJ, Forney JR, Permpanich B, Lucas C, Gasser RA, Wongsrichanalai C: Sources of variability in determining malaria parasite density by microscopy. Am J Trop Med Hyg. 2005, 73: 593-598.
Drakeley C, Reyburn H: Out with the old, in with the new: the utility of rapid diagnostic tests for malaria diagnosis in Africa. Trans R Soc Trop Med Hyg. 2009, 103: 333-337.
Murray CK, Gasser RA, Magill AJ, Miller RS: Update on rapid diagnostic testing for malaria. Clin Microbiol Rev. 2008, 21: 97-110.
WHO: Malaria rapid diagnostic test performance: results of WHO product testing of malaria RDTs: round 1. 2009, Geneva: World Health Organization
Bell DR, Wilson DW, Martin LB: False-positive results of a Plasmodium falciparum histidine-rich protein 2-detecting malaria rapid diagnostic test due to high sensitivity in a community with fluctuating low parasite density. Am J Trop Med Hyg. 2005, 73: 199-203.
Drakeley CJ, Corran PH, Coleman PG, Tongren JE, McDonald SL, Carneiro I, Malima R, Lusingu J, Manjurano A, Nkya WM, Lemnge MM, Cox J, Reyburn H, Riley EM: Estimating medium- and long-term trends in malaria transmission by using serological markers of malaria exposure. Proc Natl Acad Sci USA. 2005, 102: 5108-5113.
Druilhe P, Pradier O, Marc JP, Miltgen F, Mazier D, Parent G: Levels of antibodies to Plasmodium falciparum sporozoite surface antigens reflect malaria transmission rates and are persistent in the absence of reinfection. Infect Immun. 1986, 53: 393-397.
Ramasamy R, Nagendran K, Ramasamy MS: Antibodies to epitopes on merozoite and sporozoite surface antigens as serologic markers of malaria transmission: studies at a site in the dry zone of Sri Lanka. Am J Trop Med Hyg. 1994, 50: 537-547.
Corran P, Coleman P, Riley E, Drakeley C: Serology: a robust indicator of malaria transmission intensity?. Trends Parasitol. 2007, 23: 575-582.
Fast Track Initiative: Quality Education for All Children: Meeting the Challenge. Book Quality Education for All Children: Meeting the Challenge. 2007, Washington DC: World Bank
Fast Track Initiative: Education for All. Fast Track Initiative. 2008 Annual Report. 2008, Washington DC: World Bank
Filmer D, Pritchett L: The effect of household wealth on educational attainment: evidence from 35 countries. Population and Development Review. 1999, 25: 85-120.
World Bank: World Development Indicators (WDI) 2009. 2009, Washington D.C.: World Bank
Montresor A, Ramsan M, Chwaya HM, Ameir H, Foum A, Albonico M, Gyorkos TW, Savioli L: School enrollment in Zanzibar linked to children's age and helminth infections. Trop Med Int Health. 2001, 6: 227-231.
Fentiman A, Hall A, Bundy DAP: Health and cultural factors associated with enrolment in basic education: a study in rural Ghana. Social Science and Medicine. 2001, 52: 429-439.
Hay SI, Guerra CA, Gething PW, Patil AP, Tatem AJ, Noor AM, Kabaria CW, Manh BH, Elyazar IR, Brooker S, Smith DL, Moyeed RA, Snow RW: A world malaria map: Plasmodium falciparum endemicity in 2007. PLoS Med. 2009, 6: e1000048-
Filmer D: If You Build It, Will They Come? School Availability and School Enrollment in 21 Poor Countries. World Bank Policy Research Working Paper No. 3340. Book If You Build It, Will They Come? School Availability and School Enrollment in 21 Poor Countries. World Bank Policy Research Working Paper No. 3340. 2004, Washington D.C: World Bank
Killeen GF, Smith TA, Ferguson HM, Mshinda H, Abdulla S, Lengeler C, Kachur SP: Preventing childhood malaria in Africa by protecting adults from mosquitoes with insecticide-treated nets. PLoS Medicine. 2007, 4: e229-
Brooker S, Clarke S, Snow RW, Bundy DA: Malaria in African schoolchildren: options for control. Trans R Soc Trop Med Hyg. 2008, 102: 304-305.
Snow RW, Marsh K: The consequences of reducing transmission of Plasmodium falciparum in Africa. Adv Parasitol. 2002, 52: 235-264.
Okiro EA, Al-Taiar A, Reyburn H, Idro R, Berkley JA, Snow RW: Age patterns of severe paediatric malaria and their relationship to Plasmodium falciparum transmission intensity. Malar J. 2009, 8: 4-
Brooker S: Malaria Control in Schools. A toolkit on effective education sector responses to malaria. 2009, Washington D.C.: The World Bank
Omumbo J, Snow RW: Plasmodium falciparum parasite prevalence in East Africa: a review. East African Medical Journal. 2004, 81: 649-656.
Clyde DF: Drug prophylaxis of malaria amongst premunized school children. East African Medical Journal. 1959, 36: 12-25.
Colbourne MJ: The effect of malaria suppression in a group of Accra school children. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1955, 49: 35-369.
Geerligs PD, Brabin BJ, Eggelte TA: Analysis of the effects of malaria chemoprophylaxis in children on haematological responses, morbidity and mortality. Bull World Health Organ. 2003, 81: 205-216.
Noor AM, Moloney G, Borle M, Fegan GW, Shewchuk T, Snow RW: The use of mosquito nets and the prevalence of Plasmodium falciparum infection in rural South Central Somalia. PLoS ONE. 2008, 3: e2081-
Mwangi TW, Ross A, Snow RW, Marsh K: Case definitions of clinical malaria under different transmission conditions in Kilifi District, Kenya. J Infect Dis. 2005, 191: 1932-1939.
Koram KA, Owusu-Agyei S, Fryauff DJ, Anto F, Atuguba F, Hodgson A, Hoffman SL, Nkrumah FK: Seasonal profiles of malaria infection, anaemia, and bednet use among age groups and communities in northern Ghana. Tropical Medicine and International Health. 2003, 8 (9): 793-802.
Smith T, Charlwood JD, Kihonda J, Mwankusye S, Billingsley P, Meuwissen J, Lyimo E, Takken W, Teuscher T, Tanner M: Absence of seasonal variation in malaria parasitaemia in an area of intense seasonal transmission. Acta Tropica. 1993, 54: 55-72.
Acknowledgements
SB is supported by a Research Career Development Fellowship from the Wellcome Trust (#081673), CWG is supported by a Commonwealth Scholarship, AMN is supported by the Wellcome Trust as a Research Training Fellow (#081829) and RWS is a Wellcome Trust Principal Research Fellow (#079080). This paper is published with the permission of the director of KEMRI. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors also thank Dave Smith and Simon Hay for constructive comments on an earlier draft.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
SB and RWS conceived the idea for the paper, and SB developed the initial draft paper. JK and AMN contributed to the survey design issues, and CWG contributed to the issues surrounding the representativeness of schools. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Brooker, S., Kolaczinski, J.H., Gitonga, C.W. et al. The use of schools for malaria surveillance and programme evaluation in Africa. Malar J 8, 231 (2009). https://doi.org/10.1186/1475-2875-8-231
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2875-8-231