
Abstract
Background
Elevated serum uric acid (SUA) is regarded as a risk factor for the development of cardiovascular diseases. Triglyceride-glucose (TyG) index, a novel surrogate for insulin resistance (IR), has been proven to be an independent predictor for adverse cardiac events. However, no study has specifically focused on the interaction between the two metabolic risk factors. Whether combining the TyG index and SUA could achieve more accurate prognostic prediction in patients undergoing coronary artery bypass grafting (CABG) remains unknown.
Methods
This was a multicenter, retrospective cohort study. A total of 1225 patients who underwent CABG were included in the final analysis. The patients were grouped based on the cut-off value of the TyG index and the sex-specific criteria of hyperuricemia (HUA). Cox regression analysis was conducted. The interaction between the TyG index and SUA was estimated using relative excess risk due to interaction (RERI), attributable proportion (AP), and synergy index (SI). The improvement of model performance yielded by the inclusion of the TyG index and SUA was examined by C-statistics, net reclassification improvement (NRI) and integrated discrimination improvement (IDI). The goodness-of-fit of models was evaluated using the Akaike information criterion (AIC), Bayesian information criterion (BIC) and χ2 likelihood ratio test.
Results
During follow-up, 263 patients developed major adverse cardiovascular events (MACE). The independent and joint associations of the TyG index and SUA with adverse events were significant. Patients with higher TyG index and HUA were at higher risk of MACE (Kaplan–Meier analysis: log-rank P < 0.001; Cox regression: HR = 4.10; 95% CI 2.80–6.00, P < 0.001). A significant synergistic interaction was found between the TyG index and SUA [RERI (95% CI): 1.83 (0.32–3.34), P = 0.017; AP (95% CI): 0.41 (0.17–0.66), P = 0.001; SI (95% CI): 2.13 (1.13–4.00), P = 0.019]. The addition of the TyG index and SUA yielded a significant improvement in prognostic prediction and model fit [change in C-statistic: 0.038, P < 0.001; continuous NRI (95% CI): 0.336 (0.201–0.471), P < 0.001; IDI (95% CI): 0.031 (0.019–0.044), P < 0.001; AIC: 3534.29; BIC: 3616.45; likelihood ratio test: P < 0.001).
Conclusions
The TyG index interacts synergistically with SUA to increase the risk of MACE in patients undergoing CABG, which emphasizes the need to use both measures concurrently when assessing cardiovascular risk.
Similar content being viewed by others

Background
Coronary heart disease (CHD) is the leading cause of death, constituting an increasing public health burden worldwide [1, 2]. Coronary artery bypass grafting (CABG) can effectively recover the myocardial blood supply of patients with CHD and is preferred for those with multivessel disease [3, 4]. Despite advances in surgical techniques, the long-term prognosis of patients after CABG remains poor due to the complex nature of coronary lesions [5, 6]. Therefore, it is crucial to identify reliable prognostic factors for patients who underwent CABG.
Previous studies have shown that patients with diabetes mellitus (DM) derive more benefit from CABG than those without DM [7,8,9], and as a result, patients selected for CABG tend to suffer from more metabolic risk factors. Insulin resistance (IR) and hyperuricemia (HUA) are both important metabolic risk factors. They promote each other through multiple mechanisms and ultimately promote the progression of atherosclerosis [10,11,12].
The triglyceride-glucose (TyG) index has recently been regarded as a reliable indicator of IR, which is more economical and convenient than traditional assessment methods and shows a high degree of consistency with the hyperinsulinemic-euglycemic clamp [13,14,15]. Among patients after revascularization, those with high levels of TyG index usually had poor prognosis [15,16,17]. Chen et al. found that the TyG index was an independent prognostic factor in diabetic patients after CABG [18].
Serum uric acid (SUA) homeostasis depends on its production, excretion and reabsorption [19]. Multiple factors can disrupt the homeostasis of SUA and lead to HUA. There is growing evidence that HUA is associated with higher risk of CHD morbidity and mortality [20,21,22].
However, the prognostic value of the TyG index and SUA in patients after CABG remains unclear so far. Moreover, no study has focused on the synergistic effect of the TyG index and SUA on the prediction of adverse cardiovascular events after CABG. In the present study, we sought to investigate the prognostic value of the TyG index and SUA in patients undergoing CABG and further evaluated the synergistic effect of the two indicators.
Methods
Study population
The study was approved by the Ethics Review Committee of Shandong Provincial Hospital, The Second Hospital of Shandong University and Qilu Hospital of Shandong University and was carried out in compliance with the Helsinki Declaration. The patients provided verbal informed consent allowing the retrospective use of their anonymized data for health-related research, which was allowed by the Ethics Committee.
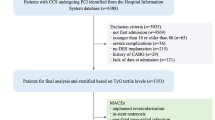
This multicenter retrospective cohort study included past-CABG patients from 3 tertiary public hospitals (Shandong Provincial Hospital, The Second Hospital of Shandong University and Qilu Hospital of Shandong University). From June 2014 to June 2018, 1665 consecutive patients who underwent CABG were screened. Among them, 270 were excluded due to concomitant surgery (valve surgery, surgical ablation or congenital heart surgery), 3 were excluded because of the history of CABG, 3 were excluded because of taking urate-lowering drugs, 11 were excluded because of suspected familial hypertriglyceridemia (triglyceride ≥ 5.65 mmol/L), and 13 were excluded due to missing data of SUA or data for TyG index calculation. A total of 1365 patients met all inclusion criteria and were followed up by telephone from July 2022 to November 2022. Finally, 1225 (89.7%) patients completed the telephone survey and were enrolled for the final analysis (Fig. 1).

Flow diagram of patient selection. CABG coronary artery bypass grafting, MACE major adverse cardiovascular events, MI myocardial infarction
Data collection
Data on demographic characteristics, medical history, personal history and medication usage were collected through the electronic medical records system. Venous blood samples were drawn after overnight fasting and the levels of fasting plasma glucose (FPG), SUA, serum creatinine (SCr), and lipid profile were measured. Hypertension was diagnosed when systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg, or if patients were on blood pressure-lowering therapies. Patients were classified as having diabetes mellitus (DM) if their casual blood glucose ≥ 11.1 mmol/L, or FPG ≥ 7.0 mmol/L, or if they were taking hypoglycemic drugs. Hyperlipidemia was defined based on ICD-10 code E78 with lipid-lowering drugs or total cholesterol (TC) ≥ 240 mg/dL [23]. The diagnosis of HUA was based on the sex-specific criteria: SUA level above 7 mg/dL in male and above 6 mg/dL in female [24]. Patients with a self-reported previous diagnosis of hypertension, DM, hyperlipidemia or HUA, which was confirmed by corresponding medical records, were also identified as having hypertension, DM, hyperlipidemia or HUA. Patients having 2-vessel or 3-vessel disease were classified as having multivessel disease and those with ≥ 50% stenosis occurring in the left main coronary artery were identified as containing the left main disease. Family history of coronary heart disease (FH-CHD) was defined as premature CHD in the immediate family (male < 55 or female < 65 years), which was determined by patient query. The eGFR was calculated using the following formula: eGFR (mL/min/1.73 m2) = 175 × SCr (mg/dL)−1.234 × age (year)−0.179 × 0.79 (if female) [25]. The TyG index was calculated based on fasting triglyceride (TG) and FPG: Ln [TG (mg/dL) × FPG (mg/dL)/2] [26].
Outcome
The first occurrence of a major adverse cardiovascular event (MACE), including all-cause death, non-fatal myocardial infarction (MI), non-fatal stroke or repeat coronary artery revascularization, was chosen as the primary endpoint in the present study. All-cause death was defined as death from cardiac or non-cardiac causes and only the death information during the follow-up was collected. Early in-hospital mortality was excluded from the analysis because of the known differences between early and late death hazard functions following CABG [27]. Non-fatal MI was confirmed using WHO criteria: typical symptoms plus electrocardiographic changes or elevated heart enzymes [28]. Repeat coronary artery revascularization included any ischemia-driven revascularization. We adopted the definition of ischemia-driven revascularization set by the EXCEL Trial [29]. All-cause death and cardiac death were analyzed as the secondary endpoints.
Statistical analysis
Statistical analysis was performed with SPSS version 25.0 (SPSS, Chicago, IL, United States) and R software version 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria). Differences were considered significant at P < 0.05. We initially performed receiver operating characteristic (ROC) curve analysis to determine the optimal cut-off value of the TyG index (the cut-off value of the TyG index for predicting MACE = 8.87). The baseline characteristics of the patients were described and compared based on the cut-off value of the TyG index and the presence or absence of HUA. Continuous variables were reported as mean ± standard deviation (SD) or median (interquartile range) and analyzed by the Student’s t-test or the Mann–Whitney U test, as appropriate. Number (percentage) and chi-square tests were used to describe and compare the categorical variables.
The Kaplan–Meier method was used to generate cumulative event curves, which were stratified by the cut-off value of the TyG index and HUA, respectively. The survival difference between groups was assessed by the log-rank test. Three Cox proportional hazards regression models were built to evaluate the independent association of the TyG index and SUA with the primary endpoint. We adjusted for age and gender in Model 1. The variables with P < 0.05 in univariate analysis entered Model 2. Variables that showed a univariate relationship with adverse events or potentially associated with clinical outcome were controlled in the fully adjusted model (Model 3), including variables in Model 2 plus gender, body mass index (BMI), drinking, hyperlipidemia, duration of surgery, coronary artery bypass grafting (OPCABG), number of grafts, use of arterial grafts, antiplatelet drugs, statins, hypoglycemic drugs and urate-lowering drugs. First, the TyG index and SUA were included together in the models as continuous variables. To limit the influence of extreme observations, the two variables of interest were further standardized to z score, which indicates the effect size per SD increase. The two variables were also included in the models as categorical variables, based on the cut-off value of the TyG index and the sex-specific criteria of HUA. We performed a collinearity diagnosis, showing that the degree of collinearity among variables was acceptable [all variance inflation factors (VIF) < 5] [30].
To investigate the joint predictive value of the TyG index and SUA on MACE, we divided the patients into four groups: Group 1: TyG ≤ 8.87 and Non-HUA, Group 2: TyG > 8.87 and Non-HUA, Group 3: TyG ≤ 8.87 and HUA, and Group 4: TyG > 8.87 and HUA. Corresponding Kaplan–Meier curves were generated followed by the log-rank test. The joint predictive value was further analyzed via the fully adjusted Cox regression model. To test the interaction between the TyG index and SUA, we calculated relative excess risk due to interaction (RERI), attributable proportion (AP), and synergy index (SI), as previously documented [31,32,33]. The incremental predictive value yielded by the inclusion of the TyG index or SUA was examined using C-statistics, net reclassification improvement (NRI) and integrated discrimination improvement (IDI). The goodness-of-fit of models was evaluated using the Akaike information criterion (AIC) and Bayesian information criterion (BIC) and the χ2 likelihood ratio test was performed.
Results
Main characteristic of participants
The ROC curve analysis showed that the optimal cut-off value of the TyG index for predicting MACE was 8.87, based on the maximum value of the Youden Index (Additional file 1: Table S1). Table 1 reported the general characteristics of the study population grouped by the cut-off value of the TyG index. In total, the study cohort included 1225 patients and male patients accounted for 70.0% (n = 857). Patients whose TyG index above the cut-off value were younger, tend to be female, and showed higher levels of BMI, FPG, TC, TG, low-density lipoprotein cholesterol (LDL-C), SUA and a lower level of high-density lipoprotein cholesterol (HDL-C). In patients with high TyG index, there were more individuals who had multivessel disease, DM, hypertension and hyperlipidemia, and were treated with hypoglycemic drugs and fibrates. Meanwhile, more patients underwent OPCABG in the high TyG index group. Moreover, the incidence of MACE was higher in patients with the TyG index above the cut-off value (Table 1).
The participants were further grouped into HUA group and non-HUA group, as shown in Table 2. Compared to non-HUA individuals, those with HUA showed higher levels of TG, LDL-C and SUA and lower levels of HDL-C and eGFR. Compared with non-HUA patients, those with HUA tend to have more MACE (Table 2).
Respective predictive value of the TyG index and SUA for MACE
In our study cohort (median follow-up time: 69 months, interquartile range: 56–76 months), MACE occurred in 263 (21.5%) patients (median time from index CABG to event: 28 months, interquartile range: 12–50 months). The first occurrence of MACE included 82 (6.7%) all-cause death [53 died from cardiac causes and 29 died from other causes], 70 (5.7%) non-fatal MI, 66 (5.4%) non-fatal stroke and 45 (3.7%) repeat revascularization. Kaplan–Meier survival curves were drawn according to the cut-off value of the TyG index and HUA (Fig. 2). Cumulative rate of MACE was significantly higher in patients with the TyG index above the cut-off value (log-rank test, P < 0.001). Meanwhile, compared to patients without HUA, those with HUA exhibited a higher MACE risk (log-rank test, P < 0.001).

Kaplan–Meier survival curves according to the TyG index and HUA. TyG index triglyceride-glucose index, HUA hyperuricemia, MACE major adverse cardiovascular events
Univariate Cox regression analysis showed that the TyG index and SUA were significantly associated with MACE (Additional file 1: Table S2). The predictive value of the TyG index and SUA remained significant after adjusting for other cardiovascular risk factors (Table 3). Compared to patients with low levels of TyG index and SUA, the risk of MACE was 2.18 times higher for individuals with a high TyG index and 1.84 times higher for individuals with HUA.
Joint influences of the TyG index and SUA on incident MACE risk
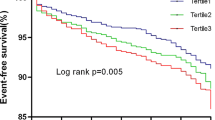
Patients were divided into four groups according to the cut-off value of the TyG index and the sex-specific criteria of HUA. Kaplan–Meier analysis was performed to compare the risk of MACE among the four groups (Fig. 3). Results showed that the risk of incident MACE was highest in patients with TyG index > 8.87 and HUA, and the cumulative rate of MACE was significantly lower in individuals with TyG index below the cut-off value and without HUA (log-rank test, P < 0.001).

Kaplan–Meier survival curves across TyG index and HUA groups. TyG index triglyceride-glucose index, HUA hyperuricemia, MACE major adverse cardiovascular events
The combined influences of the TyG index and SUA on MACE were further verified by Cox regression analysis. The highest risk of MACE was found among patients with TyG index > 8.87 and HUA (HR = 4.46; 95% CI 3.13–6.33, P < 0.001). The result remained significant in multivariable-adjusted analysis. The adjusted HR for MACE was 4.10 (95% CI 2.80–6.00) in patients with TyG index above the cut-off value and HUA, compared to individuals in Group 1 (Table 4). Other statistically significant variables included age, left ventricle ejection fraction (LVEF), left main disease, smoking, hypertension and TC (Additional file 1: Table S3).
We then investigated the joint impacts of the TyG index and SUA on all-cause death and cardiac death. The highest and statistically significant risk was observed among patients in Group 4 [HR (95% CI) of all-cause death: 5.10 (2.66–9.79), P < 0.001; HR (95% CI) of cardiac death: 6.07 (2.66–13.85), P < 0.001)] (Additional file 1: Table S4).
Sensitivity analysis was performed after exclusion of patients with renal insufficiency or individuals receiving lipid-lowering or hypoglycemic treatment at admission, which showed that our results were robust (Additional file 1: Table S5).
Subgroup analysis
Subgroup analysis was performed based on age, gender, BMI, DM, hypertension and hyperlipidemia. Figure 4 showed the combined association of the TyG index and SUA with MACE among subgroups. Generally, patients who had both high TyG index and HUA were more significantly associated with adverse cardiovascular outcomes, no matter in which subgroup (Fig. 4).

Subgroup analysis. TyG index triglyceride-glucose index, HUA hyperuricemia, BMI body mass index, DM diabetes mellitus
Interaction between the TyG index and SUA
The interaction analysis showed that the combined effect of the TyG index and HUA was significantly greater than the sum of their individual effects and the risk of MACE increased by 41% attributed to the interaction (Table 5). This synergistic interaction seemed to be more prominent in patients without DM and obesity (Additional file 1: Table S6).
The incremental predictive value of the TyG index and SUA
According to the C-statistic, continuous NRI and IDI, the addition of either the TyG index or SUA to the baseline model yielded a moderate but significant improvement in outcome prediction. We further added both the TyG index and SUA together to the baseline model, which achieved the greatest improvement of the model performance and showed a reduction of both false positives and false negatives [event NRI (95% CI): 0.141 (0.021–0.260), P = 0.021; non-event NRI (95% CI): 0.195 (0.134–0.257), P < 0.001] (Table 6).
Assessment of model goodness-of-fit
As shown in Table 7, the addition of either the TyG index or SUA to the baseline model improved model fit significantly. The model that included both the TyG index and SUA was the best-fit model, with the lowest AIC and BIC values and the likelihood ratio test was significant (Table 7).
Discussion
Based on our analysis, we have the following main findings: (1) Both the TyG index and SUA were independent prognostic factors for post-CABG patients. (2) Patients who had concurrent high TyG index and HUA had the greatest risk of MACE compared to those with neither risk factor elevated. (3) The TyG index and SUA synergistically increased the risk of incident MACE in patients after CABG.
Several studies have investigated the relationship between IR and adverse cardiovascular events after revascularization [34,35,36]. In this regard, the TyG index exhibited great potential as a cardiovascular risk predictor [15,16,17, 37, 38]. In the present study, we confirmed again that the TyG index was independently associated with MACE in patients who underwent CABG, consistent with previous findings in patients with DM [18, 39].
Whether the SUA is an independent risk factor for adverse cardiovascular events is still controversial [40]. Studies in animal models have proposed potential mechanisms leading to cardiovascular events in response to HUA [41, 42]. Several epidemiological studies have also revealed the association between SUA and cardiovascular risk [43,44,45]. However, no independent predictive value of SUA was found in a Mendelian randomization study [46]. In our present study, we found that SUA was associated with MACE in patients after CABG, which was independent of traditional cardiovascular risk factors.
To the best of our knowledge, the current study provided the first proof of the synergistic effect between the TyG index and SUA in increasing the risk of MACE. We use the additive model to perform interaction analysis, which is suitable for biological and etiological investigations [47, 48]. Despite the precise mechanism of synergistic interaction remaining unclear, some previous studies provided valuable mechanistic insights. IR could reduce UA excretion and enhance UA reabsorption [10, 49]. Meanwhile, HUA could adversely interfere with glucose uptake in skeletal muscle and induce oxidative changes in adipocytes, and lead to IR [50,51,52]. They promote each other and ultimately promote the progression of atherosclerosis through inflammation, oxidative stress, endothelial dysfunction and renin–angiotensin–aldosterone system activation [53,54,55,56]. Moreover, CATAMERI Study also provided evidence of interaction between IR and SUA in promoting vascular damage [57].
The ability of the TyG index to improve model performance was found in previous studies [58, 59], but the usefulness of the TyG index in the improvement of risk prediction after CABG was uncertain. In our current data analysis, NRI was used to measure the clinically meaningful improvement in risk classification, and IDI was used to represent the improvement in risk discrimination. The present study discovered the incremental predictive value of the TyG index and SUA in post-CABG patients for the first time. Further analysis revealed that combining the two factors could yield the greatest improvement in risk classification and discrimination and model fit. The TyG index and SUA could be used together for post-CABG risk forecasting and stratification. In addition, improvement was seen in the C-statistics after adding the TyG index and SUA, which was often very difficult to achieve in models with strong predictive power. In the current study, non-inclusion of several variables that were already known to determine post-CABG outcome made the base model weak. This made it easier to improve the C-statistics.
To rule out the influence of lipid-lowering or hypoglycemic treatment on the calculation of the TyG index, data were reanalyzed after excluding patients taking lipid-lowering or hypoglycemic drugs. We further excluded individuals with renal insufficiency, which can substantially influence the SUA level. We also explored the joint association of the TyG index and SUA with MACE among different subgroups. The results did not change significantly in sensitivity analysis and subgroup analysis, indicating that the predictive value of the TyG index and SUA for MACE was applicable to almost all populations.
This study has several limitations. First, although this is a multicenter cohort study, the retrospective design and its inherent limitations cannot be avoided. Second, several variables associated with post-CABG adverse events were not included in the regression model, such as admission type, clinical syndrome, pre-operative co-morbidity and pre-operative risk. In addition, although multiple variables associated with the progression of atherosclerosis were adjusted, we did not adjust for several variables affecting graft failure and further driving the occurrence of repeat revascularization. Therefore, no statement can be made whether the association of the TyG index and SUA with MACE was independent of these risk factors. Third, repeat revascularization was difficult to assess though it was explicitly defined and confirmed by carefully reviewing the corresponding medical records. Fourth, the HbA1c levels were not measured and data for the Society of Thoracic Surgeons (STS) risk score and Syntax score calculation were not available in most patients. Finally, our study population had a low rate of therapeutic intervention for uric acid and diabetes, which limited the generalization of results to other populations. Further prospective studies among populations with a higher therapeutic intervention rate could address the limitations of this study and confirm our findings.
Conclusion
In conclusion, the results emerging from our study revealed the prognostic value of the TyG index and SUA in patients who underwent CABG. Furthermore, our data provided novel information on the synergistic interaction between the TyG index and SUA. The combination of the TyG index and SUA could be proposed as a useful prognostic indicator in post-CABG patients.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SUA:
-
Serum uric acid
- TyG index:
-
Triglyceride-glucose index
- IR:
-
Insulin resistance
- CABG:
-
Coronary artery bypass grafting
- HUA:
-
Hyperuricemia
- RERI:
-
Relative excess risk due to interaction
- AP:
-
Attributable proportion
- SI:
-
Synergy index
- NRI:
-
Net reclassification improvement
- IDI:
-
Integrated discrimination improvement
- MACE:
-
Major adverse cardiovascular events
- CHD:
-
Coronary heart disease
- DM:
-
Diabetes mellitus
- FPG:
-
Fasting plasma glucose
- SCr:
-
Serum creatinine
- TC:
-
Total cholesterol
- FH-CHD:
-
Family history of coronary heart disease
- TG:
-
Triglyceride
- MI:
-
Myocardial infarction
- ROC curve:
-
Receiver operating characteristic curve
- SD:
-
Standard deviation
- BMI:
-
Body mass index
- LVEF:
-
Left ventricular ejection fraction
- OPCABG:
-
Off-pump coronary artery bypass grafting
- HDL-C:
-
High-density lipoprotein cholesterol
- LDL-C:
-
Low-density lipoprotein cholesterol
- VIF:
-
Variance inflation factors
References
Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics-2020 update: a report from the American Heart Association. Circulation. 2020;141(9):e139–596.
Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, Abbasi-Kangevari M, Abbastabar H, Abd-Allah F, Abdelalim A, Abdollahi M. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–22.
Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165.
Mohr FW, Morice MC, Kappetein AP, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet. 2013;381(9867):629–38.
Raja SG, Benedetto U, Chudasama D, Daley S, Husain M, Amrani M. Long-term follow-up of off-pump and on-pump coronary artery bypass grafting. Innovations. 2014;9(2):122–9 (discussion 129).
Shahian DM, O’Brien SM, et al. Predictors of long-term survival after coronary artery bypass grafting surgery: results from the society of thoracic surgeons adult cardiac surgery database (the ASCERT study). Circulation. 2012;125(12):1491–500.
Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367(25):2375–84.
Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360(10):961–72.
Tam DY, Dharma C, Rocha R, et al. Long-term survival after surgical or percutaneous revascularization in patients with diabetes and multivessel coronary disease. J Am Coll Cardiol. 2020;76(10):1153–64.
Miao Z, Yan S, Wang J, et al. Insulin resistance acts as an independent risk factor exacerbating high-purine diet induced renal injury and knee joint gouty lesions. Inflamm Res. 2009;58(10):659–68.
Doshi M, Takiue Y, Saito H, Hosoyamada M. The increased protein level of URAT1 was observed in obesity/metabolic syndrome model mice. Nucleosides Nucleotides Nucleic Acids. 2011;30(12):1290–4.
Leyva F, Wingrove CS, Godsland IF, Stevenson JC. The glycolytic pathway to coronary heart disease: a hypothesis. Metabolism. 1998;47(6):657–62.
Abbasi F, Reaven GM. Comparison of two methods using plasma triglyceride concentration as a surrogate estimate of insulin action in nondiabetic subjects: triglycerides × glucose versus triglyceride/high-density lipoprotein cholesterol. Metabolism. 2011;60(12):1673–6.
Simental-Mendía LE, Rodríguez-Morán M, Guerrero-Romero F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008;6(4):299–304.
Vasques AC, Novaes FS, de Oliveira MS, et al. TyG index performs better than HOMA in a Brazilian population: a hyperglycemic clamp validated study. Diabetes Res Clin Pract. 2011;93(3):e98–100.
Luo E, Wang D, Yan G, et al. High triglyceride-glucose index is associated with poor prognosis in patients with acute ST-elevation myocardial infarction after percutaneous coronary intervention. Cardiovasc Diabetol. 2019;18(1):150.
Ma X, Dong L, Shao Q, et al. Triglyceride glucose index for predicting cardiovascular outcomes after percutaneous coronary intervention in patients with type 2 diabetes mellitus and acute coronary syndrome. Cardiovasc Diabetol. 2020;19(1):31.
Chen L, Ding XH, Fan KJ, et al. Association between triglyceride-glucose index and 2-year adverse cardiovascular and cerebrovascular events in patients with type 2 diabetes mellitus who underwent off-pump coronary artery bypass grafting. Diabetes Metab Syndr Obes. 2022;15:439–50.
Maesaka JK, Fishbane S. Regulation of renal urate excretion: a critical review. Am J Kidney Dis. 1998;32(6):917–33.
Li M, Hu X, Fan Y, et al. Hyperuricemia and the risk for coronary heart disease morbidity and mortality a systematic review and dose-response meta-analysis. Sci Rep. 2016;6:19520.
Zuo T, Liu X, Jiang L, Mao S, Yin X, Guo L. Hyperuricemia and coronary heart disease mortality: a meta-analysis of prospective cohort studies. BMC Cardiovasc Disord. 2016;16(1):207.
Kim SY, Guevara JP, Kim KM, Choi HK, Heitjan DF, Albert DA. Hyperuricemia and coronary heart disease: a systematic review and meta-analysis. Arthritis Care Res (Hoboken). 2010;62(2):170–80.
Hong S, Han K, Park CY. The triglyceride glucose index is a simple and low-cost marker associated with atherosclerotic cardiovascular disease: a population-based study. BMC Med. 2020;18(1):361.
Liu H, Zhang XM, Wang YL, Liu BC. Prevalence of hyperuricemia among Chinese adults: a national cross-sectional survey using multistage, stratified sampling. J Nephrol. 2014;27(6):653–8.
Ma YC, Zuo L, Chen JH, et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006;17(10):2937–44.
Guerrero-Romero F, Simental-Mendía LE, González-Ortiz M, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–51.
Lobato RL, White WD, Mathew JP, Newman MF, Smith PK, McCants CB, Alexander JH, Podgoreanu MV. Thrombomodulin gene variants are associated with increased mortality after coronary artery bypass surgery in replicated analyses. Circulation. 2011;124(11 Suppl):S143-148.
Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007;115(17):2344–51.
Stone GW, Sabik JF, Serruys PW, Simonton CA, Généreux P, Puskas J, Kandzari DE, Morice MC, Lembo N, Brown WM 3rd, et al. Everolimus-eluting stents or bypass surgery for left main coronary artery disease. N Engl J Med. 2016;375(23):2223–35.
Kim JH. Multicollinearity and misleading statistical results. Korean J Anesthesiol. 2019;72(6):558–69.
Foraita R. A conditional synergy index to assess biological interaction. Eur J Epidemiol. 2009;24(9):485–94.
Knol MJ, VanderWeele TJ. Recommendations for presenting analyses of effect modification and interaction. Int J Epidemiol. 2012;41(2):514–20.
VanderWeele TJ, TchetgenTchetgen EJ. Attributing effects to interactions. Epidemiology. 2014;25(5):711–22.
Nishimura M, Tokoro T, Nishida M, et al. Association of insulin resistance with de novo coronary stenosis after percutaneous coronary artery intervention in hemodialysis patients. Nephron Clin Pract. 2008;109(1):c9-17.
Uetani T, Amano T, Harada K, et al. Impact of insulin resistance on post-procedural myocardial injury and clinical outcomes in patients who underwent elective coronary interventions with drug-eluting stents. JACC Cardiovasc Interv. 2012;5(11):1159–67.
Tie HT, Shi R, Li ZH, Zhang M, Zhang C, Wu QC. Risk of major adverse cardiovascular events in patients with metabolic syndrome after revascularization: a meta-analysis of eighteen cohorts with 18,457 patients. Metabolism. 2015;64(10):1224–34.
Li Y, He S, Wu Z, et al. The predictive value of the triglyceride-glucose index for cardiovascular events in patients with coronary chronic total occlusion. Cardiovasc Diabetol. 2022;21(1):149.
Zou S, Xu Y. Association of the triglyceride-glucose index and major adverse cardiac and cerebrovascular events in female patients undergoing percutaneous coronary intervention with drug-eluting stents: a retrospective study. Diabetes Res Clin Pract. 2021;181: 109073.
Zhang H, Chong H, Li Z, et al. Triglyceride-glucose index in the prediction of major adverse cardiovascular events in patients with type 2 diabetes mellitus after coronary artery bypass surgery: a retrospective cohort study. Front Endocrinol. 2022;13:1015747.
Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk. N Engl J Med. 2008;359(17):1811–21.
Mazzali M, Hughes J, Kim YG, et al. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension. 2001;38(5):1101–6.
Nakagawa T, Hu H, Zharikov S, et al. A causal role for uric acid in fructose-induced metabolic syndrome. Am J Physiol Renal Physiol. 2006;290(3):F625–31.
Niskanen LK, Laaksonen DE, Nyyssönen K, et al. Uric acid level as a risk factor for cardiovascular and all-cause mortality in middle-aged men: a prospective cohort study. Arch Intern Med. 2004;164(14):1546–51.
Alderman MH, Cohen H, Madhavan S, Kivlighn S. Serum uric acid and cardiovascular events in successfully treated hypertensive patients. Hypertension. 1999;34(1):144–50.
Fang J, Alderman MH. Serum uric acid and cardiovascular mortality the NHANES I epidemiologic follow-up study, 1971–1992. National health and nutrition examination survey. JAMA. 2000;283(18):2404–10.
Kleber ME, Delgado G, Grammer TB, et al. Uric acid and cardiovascular events: a Mendelian randomization study. J Am Soc Nephrol. 2015;26(11):2831–8.
Rothman KJ, Greenland S, Walker AM. Concepts of interaction. Am J Epidemiol. 1980;112(4):467–70.
de Mutsert R, Jager KJ, Zoccali C, Dekker FW. The effect of joint exposures: examining the presence of interaction. Kidney Int. 2009;75(7):677–81.
Quiñones Galvan A, Natali A, Baldi S, et al. Effect of insulin on uric acid excretion in humans. Am J Physiol. 1995;268(1 Pt 1):E1-5.
Cook S, Hugli O, Egli M, et al. Clustering of cardiovascular risk factors mimicking the human metabolic syndrome X in eNOS null mice. Swiss Med Wkly. 2003;133(25–26):360–3.
Sautin YY, Nakagawa T, Zharikov S, Johnson RJ. Adverse effects of the classic antioxidant uric acid in adipocytes: NADPH oxidase-mediated oxidative/nitrosative stress. Am J Physiol Cell Physiol. 2007;293(2):C584–96.
Furukawa S, Fujita T, Shimabukuro M, et al. Increased oxidative stress in obesity and its impact on metabolic syndrome. J Clin Invest. 2004;114(12):1752–61.
Kang DH, Park SK, Lee IK, Johnson RJ. Uric acid-induced C-reactive protein expression: implication on cell proliferation and nitric oxide production of human vascular cells. J Am Soc Nephrol. 2005;16(12):3553–62.
Rao GN, Corson MA, Berk BC. Uric acid stimulates vascular smooth muscle cell proliferation by increasing platelet-derived growth factor A-chain expression. J Biol Chem. 1991;266(13):8604–8.
Beverly JK, Budoff MJ. Atherosclerosis: pathophysiology of insulin resistance, hyperglycemia, hyperlipidemia, and inflammation. J Diabetes. 2020;12(2):102–4.
Bornfeldt KE, Tabas I. Insulin resistance, hyperglycemia, and atherosclerosis. Cell Metab. 2011;14(5):575–85.
Cassano V, Crescibene D, Hribal ML, et al. Uric acid and vascular damage in essential hypertension: role of insulin resistance. Nutrients. 2020;12(9):2509.
Zhu Y, Liu K, Chen M, et al. Triglyceride-glucose index is associated with in-stent restenosis in patients with acute coronary syndrome after percutaneous coronary intervention with drug-eluting stents. Cardiovasc Diabetol. 2021;20(1):137.
Jiao Y, Su Y, Shen J, et al. Evaluation of the long-term prognostic ability of triglyceride-glucose index for elderly acute coronary syndrome patients: a cohort study. Cardiovasc Diabetol. 2022;21(1):3.
Acknowledgements
Not applicable.
Funding
This work was supported by the grants of the National Natural Science Foundation of China (No. 81970366), the National Key Research and Development Program of China (No. 2021YFF0501403) and the Key Research and Development Plan of Shandong Province (No. 2021SFGC0503).
Author information
Authors and Affiliations
Contributions
ZW, CC, CZ and JY conceived and designed this study. XS, JW, DG and SC were responsible for the data collection and management. ZW, YZ, XL and LL contributed to analysis and interpretation of data. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Review Committee of Shandong Provincial Hospital, The Second Hospital of Shandong University and Qilu Hospital of Shandong University. As this was a retrospective cohort study and the follow-up was performed by phone, the ethics committee permitted verbal consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
ROC curve analysis determined optimal cut-off value of the TyG index for predicting MACE. Table S2. Univariate Cox regression analysis for MACE. Table S3. HR for variables in the multivariate Cox regression analysis. Table S4. Joint association of TyG index and SUA with all-cause death and cardiac death. Table S5. Sensitivity analysis for the joint association of the TyG index and SUA with MACE. Table S6. Synergistic interaction between the TyG index and SUA in patients with and without DM/obesity.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, Z., Cheng, C., Sun, X. et al. The synergistic effect of the triglyceride-glucose index and serum uric acid on the prediction of major adverse cardiovascular events after coronary artery bypass grafting: a multicenter retrospective cohort study. Cardiovasc Diabetol 22, 103 (2023). https://doi.org/10.1186/s12933-023-01838-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12933-023-01838-z