
Abstract
Background
Asynchronous e-learning has become the mainstream choice since the transformation of learning formats by the coronavirus disease-19 pandemic. This scoping review aimed to examine the technologies used in asynchronous e-learning for the continuing education of clinical nurses and their modes of delivery and effectiveness.
Methods
This scoping review covered the period between 2011 and 2023. Six databases were searched for relevant studies following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) protocol.
Results
Sixty articles met the inclusion criteria. There was a noticeable trend toward using diverse technology-enabled and enhanced training (TEET) options after 2017. The enabling technological approaches, such as interactive online modules (25 articles) and video modules (25 articles), are described in the articles. The most commonly used enhancing technologies were scenario-based learning (nine articles), resource access (eight articles), computer simulation or virtual reality (three articles), and gamification (three articles). Among the outcomes, knowledge acquisition was the most commonly examined outcome (41 articles).
Conclusions
Notably, many interactive TEET modules were used in asynchronous e-learning. There were few studies on gamification, computer simulation or virtual reality, and scenario-based learning (techniques to enhance intrinsic motivation further). However, the adoption of asynchronous e-learning with advanced TEET options is anticipated to increase in the future. Therefore, objective outcome measures are required to determine the effects of such learning methods on knowledge acquisition and behavioral changes.
Similar content being viewed by others


Background
E-learning enables learning regardless of the learner’s geographic location and time [1, 2]. In recent years, it has become the mainstream choice for continuing education for nurses, and changes in learning formats prompted by the coronavirus disease 2019 (COVID-19) pandemic have further increased the uptake of e-learning [3,4,5]. E-learning can be synchronous, connecting learners with instructors and other students in real-time, or asynchronous, allowing learners to study at a time and place of their choice [6]. The asynchronous type is a learner-directed method suitable for adult learning which enables learners to balance professional development with personal and professional obligations, particularly for nurses with irregular work schedules [7, 8]. However, because of the high level of independence among learners using e-learning, the lack of motivation for learning is considered a serious issue, and various types of asynchronous e-learning models have been developed to overcome this challenge.
The asynchronous e-learning models and designs reported in the literature range from slide-based models to types that include interactive elements [9]. Delivery methods also vary, with the most common methods categorized as (a) enhanced or supplemental, serving as an aide to face-to-face classroom learning and providing students with relative independence; (b) blended e-learning models, integrating face-to-face classroom and online learning; and (c) pure online or fully online models that provide students with maximum independence with no classroom or traditional face-to-face learning [10]. In recent years, novel e-learning methods, such as gamification and augmented or virtual reality (AR or VR), have been developed using information communication technology (ICT) and other technologies [1, 11, 12].
The term technology-enabled and enhanced training (TEET) reflects the various contributions of technology to education [13]. TEET includes both technology-enabled and technology-enhanced training. Technology-enhanced training can improve the effectiveness of interactive learning using videos, graphics, images, or simulations [14]. TEET continues to evolve as it is closely aligned with technological advancements [14]. However, very few studies have examined the effectiveness of e-learning using innovative technology in continuing education for nurses [1].
Button et al. [15] conducted a literature review to identify the technologies used for e-learning and ICT in nursing education and the problems the learners and educators face. The results revealed issues related to learners’ e-learning, information technology use, educators’ pedagogy, workload, and staff development for e-learning and related technologies. However, this study was a 10-year-old literature review covering the period between 2001 and 2012, which differs from the current ICT situation, although the low level of computer literacy is still an issue. In addition, the e-learning format was simple, such as a PowerPoint slide format or simple video. Furthermore, because the target audience included clinical nurses and students, the characteristics of continuing education for health personnel, such as motivation to learn and outcome evaluation, were unclear.
Ngenzi et al. [14] conducted a scoping review to identify available and effective TEET options to provide continuing professional development to health care providers in Rwanda, a low-income country with a limited and widely distributed health workforce. Technologies were categorized into modes of delivery and technological approaches. The technological approaches are divided into two subcategories: enabling technologies and enhancing technologies. They found several valid TEET options for both pure e-learning and blended learning modes and internet-based technologies. In this previous review, all studies using technological approaches also measured changes in the health personnel’s knowledge, skills, and behaviors, leading to increased knowledge acquisition, skills and self-efficacy, and leadership skills [14]. However, this previous study concerns e-learning and ICT-based education. Therefore, with the current development of various novel asynchronous e-learning methods, we considered that by categorizing asynchronous e-learning in continuing education for clinical nurses within the framework of TEET options used by Ngenzi et al. (2021) [14], we could identify effective TEET options and their delivery methods and educational effectiveness. This scoping review is anticipated to provide suggestions regarding the features that can be included in asynchronous e-learning, which is expected to accelerate in the future, and is foreseen to clarify the effects of asynchronous e-learning and learner motivation, which is an issue in asynchronous e-learning.
Purpose and research question
This study aimed to identify the features of asynchronous e-learning for the continuing education of clinical nurses. The following research questions were addressed:
-
(1)
What technologies are used (TEET options) and their delivery modes in asynchronous e-learning for clinical nursing education?
-
(2)
What are the effective outcomes and outcome measures adopted in clinical nursing education using asynchronous e-learning?
-
(3)
What are the benefits and issues related to asynchronous e-learning?
Definition of terms
Asynchronous e-learning
A type of e-learning that does not have a human facilitator and allows self-directed learning at a time and place of the learner’s choice.
Synchronous e-learning
A type of e-learning wherein a human facilitator is present, and the learning takes place in real time at a fixed time. Learners are often able to interact with the instructor and other learners.
Methods
A scoping review was selected as this study’s methodology. A scoping review provides an overview (mapping) of a broad body of literature, allowing for a comprehensive survey of current research and identification of areas where research has not yet been conducted (research gaps) [16, 17]. The scoping review methodology was conceptualized by Arksey and O'Malley [18] in 2005 and was subsequently developed by Levac et al. (2010) [19] and the Joanna Briggs Institute [20]. In 2018, Tricco et al. published guidelines for reporting scoping reviews as an extension of the PRISMA statement (i.e., Preferred Reporting Items for Systematic Reviews and Meta-Analysis) [17] (PRISMA-ScR: PRISMA extension for Scoping Reviews). The present review was conducted following the PRISMA-ScR protocol. The review framework consisted of 5 steps: (1) defining the research question; (2) identifying relevant studies; (3) selecting the studies; (4) charting the data; and (5) collecting, summarizing, and reporting the results.
Identifying relevant studies
The lead author (RK) and our university librarian devised the search strategy. The period covered was between 2011 and 2021. The following indexing databases were searched: PubMed, CINAHL, Cochrane Library, ERIC, Embase, and Ichu-shi Web. The inclusion criteria were intervention studies and practice reports on asynchronous e-learning in clinical nursing education written in English or Japanese. Notably, the same educational system training program provides post-graduate education for nurses and midwives in Japan. Therefore, midwives were included in the target population. The exclusion criteria were as follows: studies with no description of whether the e-learning method was synchronous or asynchronous or of the TEET option used, conference proceedings, and studies that included nursing students. The search terms used are listed in Table 1. The target population was clinical nurses and midwives; however, we decided to include cases in which nurses were part of the health care team. Therefore, the search terms were not limited to nurses but also included health personnel. With the expert help of our librarian, we checked each database for the inclusion of nurses in the subterms of health care professionals. In addition, many studies did not specify whether the type of e-learning was synchronous or asynchronous; therefore, we searched extensively for terms relating to e-learning. The Patient, Concept, Context (hereafter, “PCC”) framework shown in Table 1 was used as follows; Patient: Health personnel, Concept: Asynchronous e-learning and TEET, and Context: Clinical setting. The search string was created by connecting search terms related to each PCC category with OR and combining them with AND. The search formula used in PubMed was as follows:
-
((“e-learning”[Title/Abstract] OR “electronic learning”[Title/Abstract] OR “web based learning”[Title/Abstract] OR “online-learning”[Title/Abstract] OR “ICT”[Title/Abstract] OR “distance learn*”[Title/Abstract] OR “computer assisted instruction”[MeSH Terms] OR “internet based learning”[Title/Abstract] OR “technology enhanced learning"[Title/Abstract]) AND (“health personnel”[MeSH Terms] OR “health professional*”[Title/Abstract] OR “nurse”[Title] OR “nurses”[Title] OR “midwi*”[Title]) AND (“education, continuing”[MeSH Terms]).
We searched each database with the librarian, checking each subword so that the other databases would follow the same search formula.
The search was conducted on February 18, 2022, with a follow-up search on June 12, 2023, to add new literature. The Rayyan software was used to manage the search results.
Selection of studies
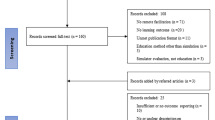
An overview of the article selection process is presented in the PRISMA-ScR flow diagram (Fig. 1). In total, 1428 articles were selected, and after removing duplicate references using automation tools, 1344 articles were selected for screening. In the first stage, two researchers (RK and MM) independently and manually screened the titles, abstracts, and inclusion or exclusion criteria. The authors were blinded to each other’s judgment. They classified the studies using Rayyan as included, excluded, or undecided, and the authors discussed the articles classified as “conflicting” and “undecided.” The screening process yielded 294 studies, of which 283 were eligible for full-text review. After excluding 11 that were unavailable, a second screening was conducted similarly. Consequently, studies that did not include nurses in the target population (n = 77), did not focus on asynchronous e-learning (n = 23), or had different objectives (n = 123) were excluded, and 60 reports were finally selected (Table 2).

PRISMA-ScR flow diagram of the article selection process. * Total number of records identified across all databases/registers, and number of records identified from each database searched. **Number of records excluded by manually
Charting the data
Data were extracted from the 60 articles, and data were charted for the following items: author, publication year, country, target population, study design aims, type of e-learning, outcomes, measurement tool of outcomes, benefits or effects related to e-learning technology, and issues or needs related to e-learning technology. The e-learning modes of delivery and technologies used were classified into modes of delivery and technological approaches (i.e., TEET) using the classification of Ngenzi et al. (2021) [14]. The quality of the articles was not examined as this step was not part of the study’s objective.
Collating, summarizing, and analyzing data
A table summarizing the articles’ characteristics and findings was prepared, and a list of articles was compiled. An overview of the studies was conducted by systematically counting the geographic distribution of the articles, year of publication, TEET options, outcomes, and content analysis of the studies to identify the benefits, effects, and challenges related to e-learning technologies. The results were shared among the researchers, and the classification and results of content analysis were discussed to ensure consensus on the perceptions. Content analysis was conducted using the conventional content analysis method by Hsieh and Shannon (2005) [78]. The article’s content was read and summarized in the first stage according to semantic units (primary codes). In the second stage, primary codes were grouped and converted into secondary codes in light of the research objectives and analysis categories. In the third step, the codes were grouped into subcategories by comparing them from the viewpoint of similarity and difference. As for the fourth step, the codes were categorized based on the relationships among the subcategories.
Results
Characteristics of selected studies
Between 2011 and 2023, 11 studies were published in 2020, 10 in 2017, and seven in 2015; 39 of the 60 studies were published in 2017 or later (Fig. 2). Data on country of publication are shown in Fig. 3. The most common continents of publication were Asia (25 articles: China, three [27, 32, 40]; Japan, 11 [29, 34, 56, 61, 63, 64, 68, 70, 71, 75, 76]; South Korea, six [26, 30, 44, 47, 65, 69]; Singapore, two [12, 67]; Turkey, one [38]; Israel, one [66]]; Iran, one [25]), followed by North America (21 articles: US, 18 [11, 21, 24, 31, 39, 43, 46, 48,49,50, 52, 54, 55, 58, 60, 62, 72, 73]; Canada, three [9, 23, 57]), Europe (eight articles: UK, two [35, 45]; Spain, one [36]; Italy, one [59]; Switzerland, one [74]; Netherlands, one [77]; Sweden, one [37]; Finland, one [51]) and Australia (six articles [22, 28, 33, 41, 42, 53]). Of the 60 studies, three were systematic review articles (Table 3) [9, 12, 41], while the remaining 57 were intervention studies. The study population in the 37 articles included only nurses, two included only midwives [34, 63], and 21 included health personnel, such as physicians and therapists. The total number of healthcare professionals included in the intervention studies examined in this study was 26,273. Of the study designs, the most common was pretest–posttest (n = 34), followed by quasi-experimental design (n = 8) and randomized controlled trial (n = 8), and systematic review (n = 3).

Year of publication

Country of publication
Technologies used (TEET options)
Table 4 shows the classifications of technological approaches based on the two categories mentioned by Ngenzi et al. (2021) [14]. The most commonly used technologies among enabling technologies were interactive online modules (25 articles) [11, 21,22,23,24, 28, 29, 31, 33, 35, 37, 42, 43, 45, 48,49,50, 53, 54, 56, 57, 62, 65, 66, 72] and videos (25 articles) [11, 24, 26, 30,31,32, 34, 35, 38, 42, 44, 50, 52, 57, 61, 65, 68, 70,71,72,73,74,75,76,77]. The next most commonly used technologies were slides or PowerPoint (11 articles) [11, 34, 39, 46, 47, 58, 59, 63, 69, 73, 77] and online discussions (seven articles) [11, 26, 28, 31, 54, 57, 72]. The most commonly used enhancing technology category was scenario-based learning (nine articles) [31, 32, 42, 51, 53, 54, 59, 62, 76], followed by resource access (eight articles) [24, 26, 28, 33, 35, 53, 59, 60] and narrated PowerPoint (eight articles) [23, 27, 46, 57, 60, 64, 71, 75], computer simulation or virtual reality (three articles) [31, 49, 62], and gamification (three articles) [11, 50, 67]. Five studies used multiple enhancing technology options [31, 53, 59, 60, 62]. Overall, there was a marked trend toward using various TEET options after 2017.
Modes of delivery
According to Ngenzi et al. (2021) [14], delivery modes can be classified into three categories: face-to-face or on-campus delivery, blended delivery, and pure online delivery. Blended delivery is “a mode of study that encompasses both online and face-to-face learning”, and pure online delivery “encompasses online learning.” Of the 57 studies, 46 used purely online learning, and 11 used blended learning [37, 43, 44, 48, 51, 54, 63, 66, 68, 70, 77].
Outcomes
As shown in Table 4, all of the included papers reported some outcomes. Knowledge acquisition was the most frequently reported outcome (41 articles), followed by behavior (14 articles) [11, 24, 32, 33, 35, 39, 42, 45, 47, 49, 52, 59, 64, 76], attitude (12 articles) [11, 30, 32, 35, 40, 44, 45, 49, 52, 53, 59, 66], satisfaction (nine articles) [22, 24, 30, 34, 36, 38, 57, 59, 71], and skills (nine articles) [43, 50, 61, 62, 67, 68, 70, 72, 77].
The studies did not use a common method for assessing the outcomes. The following scales and tools were used in the studies: the knowledge, confidence, and attitudes scale [53]; self-efficacy toward helping scale [45]; professional comfort and capability instrument [55]; sexual healthcare practice scale [26]; attitudes regarding the use of restraints scale [44]; and other existing scales as well as independently developed tests, scales, and questionnaires such as comprehension, awareness, and confidence [28, 29, 33, 34, 47,48,49, 63, 65, 69, 72]. Attitude and behavioral outcome items were previously the main assessment items, but recent years have shown a trend toward assessing skills. In addition, among the enhancing technologies that have been used since 2017, those using computer simulation or virtual reality, scenario-based learning, and gamification were effective in improving knowledge acquisition and actual behavior-related outcomes such as skills, behavior, performance, and attitude [11, 49, 50, 53, 62, 67].
Benefits of asynchronous e-learning
The benefits of asynchronous e-learning were as follows: cost-effective [25, 30, 32, 39, 47, 57, 70], time-saving and efficient [9, 25, 32, 47, 52, 68, 69, 75, 76], immediate feedback [11, 47, 68], self-paced learning [9, 11, 25, 47, 53, 57, 70, 76], flexibility [50, 70, 72, 75], ease of participation despite location and time limitations [26, 32, 50, 52, 53, 57, 63, 72], ease of participation [30, 35, 51,52,53, 57, 68], and repeated learning [53].
In addition, the following description of the benefits of the onboard features was provided: the simulation of interactive materials allows for a proxy experience on the screen. The proxy experience enhances self-efficacy, provides motivation, and leads to continued motivation to learn [29]. No one dropped out because the interactive materials kept them engaged [29]; the variety of interactive, multimedia, and hands-on elements helped maintain the nurses' curiosity and interest [43]; fun quiz formats could be used [26]; and innovative and interactive features retained the participants' interest [35]. Regarding motivation, the authors stated that adding incentives increased extrinsic motivation [11], and the connection of learning content to clinical experience increased intrinsic motivation [71]. Creating an active learning experience that promotes a sense of accomplishment among learners to increase motivation is necessary [30].
Issues related to asynchronous e-learning
The challenges related to asynchronous e-learning were as follows: the need for communication between learners and educators [57, 58]; lack of real-time feedback [71]; the influence of module and evaluation design on learning effectiveness [58]; possible failure to complete the entire module by some participants [58]; lack of time to study lengthy content [26, 51, 62]; lack of computer skills [33, 37, 51]; internet connection problems [9, 33]; lack of follow-up to prevent dropping out [56]; and lack of incentives to stay motivated [26]. Consequently, the need to provide opportunities to observe actual situations [71] has been highlighted, as asynchronous e-learning was considered insufficient for improving confidence [47] and practical skills [22, 71].
The onboard features in gamification present some risks; for instance, in situations involving differences or discontinuities in spatial position and timing of movements between practice with web-based game scenarios and real-life scenarios, game users might negatively modify their performance, and an inappropriate transfer of skills may occur. Moreover, a negative transfer may occur when game users find that the skills they see in the game differ from those needed in real life [67]. It was also stated that research designs to measure the educational effectiveness of e-learning are insufficient because there is a lack of good-quality RCTs to compare the effects of purely digital education [12]. In particular, few studies have measured outcomes on the impact of gamification, and those that have identified educational or clinical outcomes have low power and little clear evidence [67].
Discussion
Interactive modules and videos are the most frequently used enabling technologies under TEET. In contrast to face-to-face learning or synchronous e-learning, asynchronous e-learning lacks the feeling of being taught directly in real-time. As learners can engage with e-learning modules at their own pace, this may affect their motivation levels. Cheng [79] explored the relationship between intrinsic and extrinsic motivation in nurses’ e-learning. Interaction was one of the most essential factors in the e-learning environment. Based on the Technology Acceptance Model and flow theory, three types of interaction factors (i.e., learner-system interaction, instructor-learner interaction, and learner-learner interaction) that lead to nurses’ acceptance of e-learning systems were studied. The results revealed that instructor–learner interaction was the most crucial antecedent factor impacting nurses’ extrinsic motivation. Notably, learner-learner interaction greatly influences nurses’ intrinsic motivation, suggesting it can promote their learning persistence [79].
The guiding framework for developing asynchronous e-learning modules for healthcare professionals by Sinclair et al. (2017) [80] provides 10 guidelines for creating engaging and effective asynchronous e-learning programs. It states that because many purported e-learning programs have limited interactivity, developing and delivering engaging and pedagogically sound e-learning programs must be based on evidence-based instructional design principles. Interactive elements are required to provide learning guidance, content, and feedback [80]. Therefore, considering the three types of interactions (learner–system, instructor–learner, and learner–learner), using interactivity at the necessary stages can help maintain learners’ motivation.
Video module was the most frequently used enabling technology among the TEET options. Videos and other images can promote a person-centered approach in health professional education and motivate learners by using text, videos, and audio files to introduce them to the “person” under their care. This indicates that by relating to the patient or person who needs nursing care, learners experience a sense of connection and are motivated despite the individualistic asynchronous e-learning method. This method would help learners view their learning as a meaningful engagement with real people [32, 80]. Personal stories are powerful and effective methods for adult learners to retain information [81]. Videos are an effective means of learning because they provide a realistic sense of a particular place or scenario.
Regarding technological enhancement, there was no significant increase in innovations aimed at enhancing internal motivation, but scenario-based learning and gamification are likely to develop further [82]. Innovative e-learning is also being developed to integrate technologies such as virtual reality, virtual patient simulation, and virtual hands-on training to provide activities beyond the linear presentation of information in an e-learning format [1, 12]. These novel e-learning programs are expected to be adopted in clinical education and e-learning in future nursing studies. Using such innovative e-learning methods is expected to benefit knowledge acquisition and the ability of learners to connect what is learned with clinical practice, behavioral change, clinical judgment, and clinical reasoning levels.
The results of the present scoping review also revealed that, in recent years, many studies using video technology and simulation had evaluated skills as outcomes. In the past, the educational effects of e-learning on the continuing professional development of health personnel had focused mainly on learner satisfaction and knowledge acquisition, as the impact on practical behavior change has been considered difficult to assess [80]. There is limited research on evaluating more advanced aspects of education, such as behavioral change and the application of learning in clinical practice [80]. Therefore, there is a need for evaluation metrics or indicators aimed at behavioral change and skill development from innovative e-learning modules [83].
In addition, e-learning and evaluation metrics for TEET options and delivery methods should consider factors that facilitate and inhibit e-learning. Regmi and Jones [10] conducted a systematic review to identify and integrate the facilitating and inhibiting factors influencing e-learning in health sciences education. Their conceptual framework included three broad factors: “design and delivery,” “learning outcomes,” and “policy context” [10]. Because the authors found a clear link between the delivery mechanism of e-learning and the potential learning outcomes, developing asynchronous e-learning modules in light of these three factors can help increase external motivation among nurses.
Our scoping review had some limitations. The TEET modules used for e-learning were not standardized, so we judged based on the text descriptions, which may have caused a selection bias. We may also have missed some functions not detailed in the text. As gray literature was not searched, it is possible that some studies were missed. To grasp a wide range of data on asynchronous e-learning in this scoping review, we included pure online and blended learning. While we extracted content related to asynchronous e-learning in terms of benefits and challenges, the results were likely influenced by the effect of blended learning.
Considering that limiting the scope of this study to nurses would eliminate a wide range of asynchronous e-learning methods, we also expanded the scope to health personnel. However, nurses accounted for a large proportion of the health personnel. As more and more research on asynchronous e-learning is expected to be conducted in the future, subsequent reviews may focus on only nurses to determine the results of the review strategy.
Conclusions
Using data from the 60 articles on asynchronous e-learning, we categorized the technological approaches, modes of delivery, and outcomes. The most commonly used TEET options were interactive online modules and videos. The popularity of other advanced TEET options, such as computer simulations and gamification, is expected to increase in the future. Furthermore, outcome measures need to be continuously developed, considering that e-learning continues to evolve. Three types of interactions, namely, learner–system, instructor–learner, and learner–learner, are important for asynchronous e-learning. Therefore, using interactive features at necessary stages can help promote motivation among the learners.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- TEET:
-
Technology-enabled and enhanced training
- PRISMA-ScR:
-
Preferred Reporting Items for Systematic Reviews, and Meta-Analysis extension for Scoping Reviews
- ICT:
-
Information communication technology
References
Dahlke S, Hunter KF, Amoudu O. Innovation in education with acute care nurses. J Contin Educ Nurs. 2020;51:420–4.
Govranos M, Newton JM. Exploring ward nurses’ perceptions of continuing education in clinical settings. Nurse Educ Today. 2014;34:655–60.
Seymour-Walsh AE, Bell A, Weber A, Smith T. Adapting to a new reality: COVID-19 coronavirus and online education in the health professions. Rural Remote Health. 2020;20:6000.
Hamilton LS, Grant D, Kaufman JH, Diliberti MK, Schwartz HL, Hunter GP, et al. COVID-19 and the state of K–12 Schools: results and technical documentation from the Spring 2020 American educator panels COVID-19 surveys. https://www.rand.org/pubs/research_reports/RRA168-1.html. Accessed 30 Jan 2023.
Bacher-Hicks A, Goodman J, Mulhern C. Inequality in household adaptation to schooling shocks: Covid-induced online learning engagement in real time. J Public Econ. 2021;193:104345.
Lawn S, Zhi X, Morello A. An integrative review of e-learning in the delivery of self-management support training for health professionals. BMC Med Educ. 2017;17:183.
Sinclair P, Carstairs M, Shanahan B, Schoch M. The development of a medication calculation competency and quality use of renal medicine e-learning program. Ren Soc Australas J. 2014;10:58–60.
Xing W, Ao L, Xiao H, Cheng L, Liang Y, Wang J. Nurses’ attitudes toward, and needs for online learning: differences between rural and urban hospitals in Shanghai, East China. Int J Environ Res Public Health. 2018;15:1495.
Rouleau G, Gagnon MP, Côté J, Payne-Gagnon J, Hudson E, Dubois CA, et al. Effects of e-learning in a continuing education context on nursing care: systematic review of systematic qualitative, quantitative, and mixed-studies reviews. J Med Internet Res. 2019;21:e15118.
Regmi K, Jones L. A systematic review of the factors - enablers and barriers - affecting e-learning in health sciences education. BMC Med Educ. 2020;20:91.
ONeill K, Robb M, Kennedy R, Bhattacharya A, Dominici NR, Murphy A. Mobile technology, just-in-time learning and gamification: innovative strategies for a CAUTI Education Program. Online J Nurs Inform. 2018;22(2). https://www.himss.org/resources/mobile-technology-just-time-learning-and-gamification-innovative-strategies-cauti. Accessed 5 Jul 2023.
Martinengo L, Yeo NJY, Markandran KD, Olsson M, Kyaw BM, Car LT. Digital health professions education on chronic wound management: A systematic review. Int J Nurs Stud. 2020;104:103512.
Scott RE, Maurice M. The spectrum of needed e-Health capacity building - towards a conceptual framework for e-Health ‘training.’ Global Telehealth. 2014;206:70–7.
Ngenzi JL, Scott RE, Mars M. Information and communication technology to enhance continuing professional development (CPD) and continuing medical education (CME) for Rwanda: a scoping review of reviews. BMC Med Educ. 2021;21:245.
Button D, Harrington A, Belan I. E-learning & information communication technology (ICT) in nursing education: A review of the literature. Nurse Educ Today. 2014;34:1311–23.
Peters MD, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–26. https://doi.org/10.11124/JBIES-20-00167.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467–73.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):69–78.
Peters MDJ, Godfrey C, McInerney P, Baldini Soares C, Khalil H, Parker D. Scoping reviews In: Aromataris E. Munn Z, eds. Joanna Briggs Institute Reviewer’s Manual. Adelaide, Australia: Joanna Briggs Inst: 2020.https://reviewersmanual. Joannabriggs.org/. Accessed 30 Jan 2023.
Dennison HA. Creating a computer-assisted learning module for the non-expert nephrology nurse. Nephrol Nurs J. 2011;38:41–52.
Sherriff K, Burston S, Wallis M. Effectiveness of a computer based medication calculation education and testing programme for nurses. Nurs Educ Today. 2012;32:46–51.
Spiva L, Johnson K, Robertson B, Barrett DT, Jarrell NM, Hunter D, et al. The effectiveness of nurses’ ability to interpret basic electrocardiogram strips accurately using different learning modalities. J Contin Educ Nurs. 2012;43:81–9.
Gordon JS, Mahabee-Gittens EM, Andrews JA, Christiansen SM, Byron DJ. A randomized clinical trial of a web-based tobacco cessation education program. Pediatrics. 2013;131:e455–62.
Alipour S, Jannat F, Hosseini L. Teaching breast cancer screening via text messages as part of continuing education for working nurses: A case-control study. Asian Pac Cancer Prev. 2014;15(14):5607–9.
Kim JH, Shin JS. Effects of an online problem-based learning program on sexual health care competencies among oncology nurses: a pilot study. J Contin Educ Nurs. 2014;45:393–401.
Liu W-I, Chu K-C, Chen S-C. The development and preliminary effectiveness of a nursing case management e-learning program. Comput Inform Nurs. 2014;32(7):343–52.
McCrow J, Sullivan KA, Beattie ER. Delirium knowledge and recognition: a randomized controlled trial of a web-based educational intervention for acute care nurses. Nurs Educ Today. 2014;34:912–7.
Yoshikawa Y. Comparative study of the e-learning materials evaluation in newcomer nursing education: Comparative to interactive teaching materials and video teaching materials. Int Nurs Care Res. 2014;13:81–90.
De Gagne JC, Park S, So A, Wu B, Palmer MH, McConnell ES. A urinary incontinence continuing education online course for community health nurses in South Korea. J Contin Educ Nurs. 2015;46:171–8.
Delaney MM, Friedman MI, Dolansky MA, Fitzpatrick JJ. Impact of a sepsis educational program on nurse competence. J Contin Educ Nurs. 2015;46:179–86.
Hsu TC, Chiang-Hanisko L, Lee-Hsieh J, Lee GY, Turton MA, Tseng YJ. Effectiveness of an online caring curriculum in enhancing nurses’ caring behavior. J Contin Educ Nurs. 2015;46(9):416–24.
Johnson M, Kelly L, Siric K, Tran DT, Overs B. Improving falls risk screening and prevention using an e-learning approach. J Nurs Manag. 2015;23:910–9.
Kato C, Katoka Y, Igarashi Y, Hiruta A. Evaluation of an e-learning program of continuing midwifery education on postpartum hemorrhage. J Jpn Acad Midwif. 2015;29:77–86.
Murphy J, Worswick L, Pulman A, Ford G, Jeffery J. Translating research into practice: evaluation of an e-learning resource for health care professionals to provide nutrition advice and support for cancer survivors. Nurse Educ Today. 2015;35:271–6.
Sarabia-Cobo CM, Torres-Manrique B, Ortego-Mate MC, Salvadores-Fuentes P, Sáenz-Jalón M. Continuing education in patient safety: Massive open online courses as a new training tool. J Contin Educ Nurs. 2015;46(10):439–45.
Berggren E, Orrevall Y, Olin AÖ, Strang P, Szulkin R, Törnkvist L. Evaluation of a continuing educational intervention for primary health care professionals about nutritional care of patients at home. J Nutr Health Aging. 2016;20:428–38.
Okuroğlu GK, Alpar ŞE. Development of a web-based diabetes education program for health care professionals. J Contin Educ Nurs. 2016;47:464–71.
Perrego K. Improving staff knowledge of perioperative regulated-waste management. AORN J. 2017;105:85–91.
Sarna L, Bialous SA, Zou XN, Wang W, Hong J, Wells M, et al. Evaluation of a web-based educational programme on changes in frequency of nurses’ interventions to help smokers quit and reduce second-hand smoke exposure in China. J Adv Nurs. 2016;72:118–26.
Sinclair PM, Kable A, Levett-Jones T, Booth D. The effectiveness of Internet-based e-learning on clinician behaviour and patient outcomes: A systematic review. Int J Nurs Stud. 2016;57:70–81.
Bond SE, Crowther SP, Adhikari S, Chubaty AJ, Yu P, Borchard JP, et al. Design and implementation of a novel web-based e-learning tool for education of health professionals on the antibiotic vancomycin. J Med Internet Res. 2017;19:1–13.
Glover KR, Stahl BR, Murray C, LeClair M, Gallucci S, King MA, et al. A simulation-based blended curriculum for short peripheral intravenous catheter insertion: an industry-practice collaboration. J Contin Educ Nurs. 2017;48:397–406.
Kong EH, Song E, Evans LK. Effects of a multicomponent restraint reduction program for Korean nursing home staff. J Nurs Scholarsh. 2017;49:325–35.
Manning JC, Carter T, Latif A, Horsley A, Cooper J, Armstrong M, et al. ‘Our Care through Our Eyes’. Impact of a co-produced digital educational programme on nurses’ knowledge, confidence and attitudes in providing care for children and young people who have self-harmed: A mixed-methods study in the UK. BMJ Open. 2017;7:e014750.
Micheel CM, Anderson IA, Lee P, Chen SC, Justiss K, Giuse NB, et al. Internet-based assessment of oncology health care professional learning style and optimization of materials for web-based learning: Controlled trial with concealed allocation. J Med Internet Res. 2017;19:1–14.
Shin JY, Issenberg SB, Roh YS. The effects of neurologic assessment e-learning in nurses. Nurse Educ Today. 2017;57:60–4.
Smith JM, Van Aman MN, Schneiderhahn ME, Edelman R, Ercole PM. Assessment of delirium in intensive care unit patients: educational strategies. J Contin Educ Nurs. 2017;48:239–44.
Trudeau KJ, Hildebrand C, Garg P, Chiauzzi E, Zacharoff KL. A randomized controlled trial of the effects of online pain management education on primary care providers. Pain Med. 2017;18:680–92.
Williams K, Abd-Hamid NH, Perkhounkova Y. Transitioning communication education to an interactive online module format. J Contin Educ Nurs. 2017;48:320–8.
Ylönen M, Viljamaa J, Isoaho H, Junttila K, Leino-Kilpi H, Suhonen R. Internet-based learning programme to increase nurses’ knowledge level about venous leg ulcer care in home health care. J Clin Nurs. 2017;26(21–22):3646–57.
Goodman HA, Pacheco CL, Loescher LJ. an online intervention to enhance nurse practitioners’ skin cancer knowledge, attitudes, and counseling behaviors: a pilot study. J Dermatol Nurs Assoc. 2018;10:20–8.
Meredith P, Yeates H, Greaves A, Taylor M, Slattery M, Charters M, et al. Preparing mental health professionals for new directions in mental health practice: Evaluating the sensory approaches e-learning training package. Int J Ment Health Nurs. 2018;27:106–15.
Abel SE, Hall M, Swartz MJ, Madigan EA. Empowerment of front-line leaders in an online learning, certificate programme. J Nurs Manag. 2020;28:359–67.
Gullatte MM, Allen CS, Botheroyd E, Hess RG Jr, Higgins M, Meneghetti J, et al. Improving end-of-life communications using technology-assisted continuing education with interprofessional teams. J Nurs Prof Dev. 2019;35:25–31.
Kaneko T, Morita N, Ito M, Sekiya D. Examination of the impact of the educational web program to improve emotional coping with emotional labor among nurses. J Jpn Acad Nurs Sci. 2019;39:45–53.
Lineker SC, Fleet LJ, Bell MJ, Sweezie R, Curran V, Brock G, et al. Getting a grip on arthritis online: responses of rural/remote primary care providers to a web-based continuing medical education programme. Can J Rural Med. 2019;24:52–60.
Schilinski S, Hellier SD, Cline TW. Evaluation of an electronically delivered learning module intended for continuing education of practicing registered nurses: a pretest-posttest longitudinal study. J Contin Educ Nurs. 2019;50:331–6.
Colaceci S, Zambri F, D’amore C, De Angelis A, Rasi F, Pucciarelli G, et al. Long-term effectiveness of an e-learning program in improving health care professionals’ attitudes and practices on breastfeeding: A 1-year follow-up study. Breastfeed Med. 2020;15:254–60.
Harvey A, Zhang Y, Phillips S, Suarez R, Dekle L, Villalobos A, et al. Initial outcomes of an online continuing education series focused on post-treatment cancer survivorship care. J Cancer Educ. 2020;35:144–50.
Horiguchi T, Asada Y, Tasaki K, Inagaki M. Investigation of educational methods using e-learning teaching materials to improve nurses’ skills in promoting team-based diabetes medical care. J Jpn Acad Nurs Sci. 2020;40:579–86.
Howard MS, Embree JL. Educational intervention improves communication abilities of nurses encountering workplace incivility. J Contin Educ Nurs. 2020;51:138–44.
Akemi I. Development and assessment of a training program for improving midwives’ knowledge and perceptions of family role acquisition in the perinatal period. J Jpn Acad Midwif. 2020;34:61–8.
Kurotaki A. The effect of an educational program on improving the ability of hospital nursing administrators to accept supporting nurses. J Japan Soc Disaster Nurs. 2020;22:15–27.
Mun MY, Hwang SY. Development and evaluation of a web-based learning course for clinical nurses: anticancer chemotherapy and nursing. Korean J Adult Nurs. 2020;32:364–73.
Shchory MP, Goldstein LH, Arcavi L, Shihmanter R, Berkovitch M, Levy A. The effect of an intervention program on the knowledge and attitudes among medical staff regarding adverse drug reaction reporting. Pharmacoepidemiol Drug Saf. 2020;29:1246–53.
Yeo CL, Ho SKY, Tagamolila VC, Arunachalam S, Bharadwaj SS, Poon WB, et al. Use of web-based game in neonatal resuscitation - is it effective? BMC Med Educ. 2020;20:170.
Yoshida M, Miura Y, Yabunaka K, Sato N, Matsumoto M, Yamada M, et al. Efficacy of an education program for nurses that concerns the use of point-of-care ultrasound to monitor for aspiration and pharyngeal post-swallow residue: A prospective, descriptive study. Nurse Educ Pract. 2020;44:102749.
Lim H, Yi Y. Effects of a web-based education program for nurses using medical malpractice cases: A randomized controlled trial. Nurse Educ Today. 2021;104:104997.
Matsumoto M, Tamai N, Miura Y, Okawa Y, Yoshida M, Igawa Y, et al. Evaluation of a point-of-care ultrasound educational program for nurse educators. J Contin Educ Nurs. 2021;52:375–81.
Ota Y. Development and operation of an e-learning program for nurses to support attachment formation between mother and child in the early postpartum period. Matern Health. 2021;62:168–78.
Williams KN, Coleman CK, Perkhounkova Y, Beachy T, Hein M, Shaw CA, et al. Moving online: A pilot clinical trial of the changing talk online communication education for nursing home staff. Gerontologist. 2021;61:1338–45.
Evelyn AE, Kittelson S, Mandernach MW, Black V, Duckworth L, Wilkie DJ. Nursing education for the acute care nurse on pain mechanisms of sickle cell disease. J Contin Educ Nurs. 2022;53:137–44.
Fang J, Chen S, Yang L, Liao K, Lin C, Fujimori M, et al. Improving transitional care through online communication skills training. Aging Clin Exp Res. 2022;34:3063–71.
Nakamura S, Takeuchi S, Hoshino T, Okubo N, Horiuchi S. Effects of web-based learning for nurses on their care for pregnant women with hiesho (sensitivity of hands or feet to cold): A randomized controlled trial. Jpn J Nurs Sci. 2022;19(4):1–10.
Suzuki M, Yoshimura H, Omuro S, Sawaki K, Naito T, Inagaki K, et al. Effectiveness of a dementia nursing practice skills development program for nurses in acute care hospitals. Jpn J Geriatr. 2022;59(1):67–78.
Bos–van den Hoek DW, Smets EMA, Ali R, Baas-Thijssen MCM, Bomhof-Roordink H, Helsper CW, et al. A blended learning for general practitioners and nurses on skills to support shared decision-making with patients about palliative cancer treatment: A one-group pre-posttest study. Patient Educ Couns. 2023;112:107712.
Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–88.
Cheng YM. Exploring the roles of interaction and flow in explaining nurses’ e-learning acceptance. Nurse Educ Today. 2013;33:73–80.
Sinclair PM, Levett-Jones T, Morris A, Carter B, Bennett PN, Kable A. High engagement, high quality: A guiding framework for developing empirically informed asynchronous e-learning programs for health professional educators. Nurs Health Sci. 2017;19:126–37.
Prusak L, Groh K, Denning S, Brown JS. Storytelling in Organizations: Why Storytelling is Transforming 21st Century Organizations and Management. Place: Routledge; 2016. p. 1–208.
Bezovski Z, Poorani S. The evolution of e-learning and new trends. Inf Knowl Manag. 2016;6:50–7.
Webb TL, Joseph J, Yardley L, Michie S. Using the internet to promote health behavior change: a systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J Med Internet Res. 2010;12:e4.
Acknowledgements
Not applicable.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
RK conceived and designed the study; RK and MM collected the data, analyzed and interpreted it; RK drafted the article; EB, MM, and NH revised it critically to form important intellectual content; RK, MM, EB, and NH re-checked and approved the final article for submission; RK, MM, EB, and NH agreed to be accountable for all aspects of this review.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
An ethics statement is not applicable because this study is based exclusively on published literature.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kimura, R., Matsunaga, M., Barroga, E. et al. Asynchronous e-learning with technology-enabled and enhanced training for continuing education of nurses: a scoping review. BMC Med Educ 23, 505 (2023). https://doi.org/10.1186/s12909-023-04477-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-023-04477-w