
Abstract
Background
Remote facilitation is a synchronous distance education method where instructors facilitate a lesson, in real-time, in physically separate conditions. In this scoping review, we aimed to describe types of remote facilitation used in a healthcare simulation, the influences on learner outcomes, and related factors.
Methods
We accessed PubMed, EMBASE, CINAHL, ERIC, and Web of Science using our search strategies. Five reviewers performed the review using the Preferred Reporting Items for Systematic Reviews and Meta Analysis extension for Scoping Reviews (PRISMA-ScR) framework, and the Johanna Briggs Institute (JBI) guidelines.
Results
We included a total of 29 articles presenting 28 simulation studies. The most common tool was videoconferencing (n = 26, 89.7%). Knowledge improvement was the most frequently measured outcome. There was no significant difference in learning outcomes between the two teaching modes. There were differences in learners’ preferences and satisfaction with remote facilitators before and after COVID-19.
Conclusions
Our scoping review indicates that remote facilitation has been widely accepted in many healthcare professions using various types of simulation modalities. Remote facilitation can be used to overcome logistical problems of synchronous multi-location education, and to improve learner knowledge, skills, and confidence measured by instructor evaluation or self-assessment.
Similar content being viewed by others


Introduction
During the COVID-19 pandemic, much of healthcare education, including simulations-based trainings, rapidly transitioned to remote platforms rather than in-person classes [1, 2]. However, remote simulation or telesimulation is not a new concept. Telesimulation is a process by which telecommunication and telesimulation resources are used to provide education, training, and/or assessment to learners at an off-site location [3]. Remotely facilitated simulation-based training (RF-SBT) is a synchronous distance education method in which instructors facilitate lessons in real time under physically separate conditions [4]. RF-SBT can be conducted using a variety of techniques. For example, trainees may have access to both patient simulators (e.g., a manikin, a standardized patient) and instructors remotely. In another approach, the simulators are on-site, but the instructors control and facilitate the lesson remotely with or without on-site instructors. In the many years since virtual technology for education was introduced, RF-SBT was initially be conducted with a screen-based simulation and has evolved to an application using other methods. The unifying key characteristic of these simulations is remote facilitation.
Several studies have reported that remote facilitation is effective and applicable in healthcare simulation education [5,6,7,8,9,10]. However, the perception of remote facilitation and its effect on educational outcomes are unclear. Several studies have reported learner satisfaction with remote facilitation [11,12,13,14], whereas other participants have indicated difficulties using technology, discomfort, and communication barriers [4, 7, 8, 10]. Before COVID-19, remote facilitation was used for specific reasons, such as education in underdeveloped countries, rural or resource-limited areas, or military medical practice [15,16,17,18,19]. Today, remote education is frequently considered in various healthcare education contexts because remote educational experiences using telecommunications technology have become common during COVID-19 [2]. Debriefing is essential for learning in all simulations, including virtual simulation experiences [20]. The question now is how best to conduct debriefings and facilitation during remote simulations, as educational institutions increasingly use online and technology-enabled learning [11]. In a recent meta-analysis, approximately half of the virtual simulations, regardless of whether they were operated remotely or locally, did not have post-simulation debriefing sessions [21]. Thus, most studies did not examine the effectiveness of debriefing sessions on student learning.
With this scoping review, we aimed to describe the types of remote facilitation in a healthcare simulation, the influence on learner outcomes, and other related factors. To achieve this goal, we scrutinized the circumstances and types of simulation education using remote facilitation, outcomes observed in simulation-based education with remote facilitation, learners’ preferences, and factors related to the effect of remote facilitation on learning outcomes.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta Analysis extension for Scoping Reviews (PRISMA-ScR) framework [22] and the Johanna Briggs Institute (JBI) guidelines [23, 24].
Inclusion criteria
To be included in the review, articles were required to describe simulation education and report information on facilitation and learning outcomes. We included peer-reviewed articles if they were published before April 2021 and written in English. We only included studies on remote facilitation conducted synchronously with simulation or consecutively conducted as a debriefing session by a facilitator with greater expertise than learners. We included all simulation topics and techniques, such as mannequins, task trainers, standardized patients, simulated patients, virtual reality and others in simulation education research in order to encompass all element of remote simulation facilitation to the fullest extent possible.
Search strategy and screening
For this scoping review, we accessed PubMed, EMBASE, CINAHL, ERIC, and Web of Science using our search strategies (Supplementary material 1). We did not identify or include gray literature sources. We performed a systematic search of these databases from April 1 to May 13, 2021. The search strategies were developed by an experienced research librarian (MK) and further refined through reviewer discussions to identify relevant primary studies. The final search strategy for all databases is in Supplementary material 1. The final search outcome was deduplicated by the librarian (MK) following Bramer’s methods [25]. We included quantitative, qualitative, and mixed methods studies to understand the full scope of learning outcomes and the learners’ experiences. We excluded gray literature such as conference abstracts, editorials, interviews, lectures, letters, news, guidelines, methodology papers, and non-systematic reviews.
To clarify the inclusion criteria and increase consistency among reviewers, all reviewers conducted pilot screening using 50 papers randomly selected from the search results. During the pilot screening, the reviewers narrowed the inclusion criteria and revised the data extraction form.
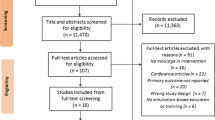
Four reviewers (BB, JL, YE, ES) working in pairs sequentially evaluated the titles, abstracts, and then the full texts of all articles. Each reviewer pair was responsible for half of the entire search results. The fifth author (JP) independently screened all findings. Thus, each paper was screened by three independent reviewers and decisions were made through the consensus of at least two reviewers. If the fifth reviewer determined that further discussion was necessary for an inclusion decision, all five reviewers reviewed and discussed the article to make a final decision (Fig. 1). Reviewers completed this process using the Colandr [26], a web-based evidence review platform.

The Preferred Reporting Items for Systematic Reviews and Meta Analysis extension for Scoping Reviews (PRISMA-ScR) flow diagram of this scoping review
Data extraction and synthesis
A data extraction chart was primarily developed by one reviewer (JP) and three reviewers (BB, JL, JP) independently charted the data, discussed the results, and updated the data-charting format through an iterative process. Appraisal of the included articles was completed by four reviewers in two scoring groups of two members each using the Joanna Briggs Critical Appraisal Tools [27, 28]. Each scoring group was assigned and scored half of the total number of manuscripts. Individual reviewers within a scoring group reconciled discrepancies within the scoring group through discussion. Recent developments in the subject matter include the difficulty of applying a rigorous research design; we did not exclude studies based on appraisal scores.
Due to the heterogeneity of study designs and interventions, we synthesized, summarized, and reported on the extracted data in a descriptive format. We initially summarized the characteristics of simulation and facilitation, and summarized logistical and organizational, demographic, and other educational characteristics of simulation and facilitation. Next, we synthesized essential qualitative data through discussions based on the research question and themes related to learner outcomes. Finally, we narratively described the essential qualitative data through reviewer discussions based on the research question.
Results
The initial systematic search of databases produced 5,198 records. After deduplication, the citation screening began with 2,809 articles and based on review titles and abstracts, we excluded 2,649 studies and downloaded 160 full-text manuscripts for further screening. After full-text screening, 54 articles were eligible for full-text review. Finally, we included 29 articles presenting 28 simulation studies in the scoping review (Fig. 1).
Study characteristics
Two articles [4, 5] were from one simulation study. All eligible studies were published after 2009, and eight studies described simulations during the COVID-19 pandemic (Table 1). There was one qualitative study [4]. Among others, seven articles used a mixed methods design, including a quantitative design as a major approach with qualitative data collection such as a focus group interview [14, 29], survey comments [7, 30,31,32], and audiovisual recorded comments [33]. Reviewers evaluated the quality of these mixed methods articles using a JBI checklist for quantitative designs if the primary technique was quantitative. Most articles showed a medium (0.5–0.7) quality of evidence based on the appraisal score (Table 1).
Target population
The number of learners varied by type of simulation and the duration of the curriculum, from 11 [29] in an avatar-based virtual continuing medical education (CME) workshop to 305 [5] in a statewide mandatory course offered year-round. The most common areas of professional expertise among learners were medical [6, 7, 10, 14, 17,18,19, 29, 33,34,35,36,37,38,39,40,41,42], nursing [11, 31, 43], multi-professional [4, 5, 13, 44], interprofessional [30, 32], and dental [45]. One study [46] reported on an educational intervention for research coordinators. The most common learner levels were students [5,6,7, 10, 11, 14, 17, 31,32,33, 37, 38, 41, 42], while other learners were professionals who had completed professional school or other higher education and had practical experience, such as medical specialists [18, 19, 29, 30, 35], medical residents [34, 39, 40], nursing staff [43, 44], research coordinators [46], or post-graduate students [4, 5, 13].
Simulation topics and modalities
Simulation topics for which remote facilitation was applied were very diverse. There were simulations for skills training [10, 13, 17, 18, 34, 35, 38, 39, 41, 44, 45], scenario-based simulations that included all or part of patient evaluation, diagnosis, and treatment [4,5,6,7, 11, 31, 37, 40, 42], In addition, there were simulations for interviewing patients or family members [29, 46], answering pages [33, 36], telehealth practice [31], medical records documentation [14], and interprofessional team training [30, 32]. Simulations focused on technical skills only [13, 17, 19, 34, 38, 39, 41, 47] (n = 8), non-technical skills (NTS), such as leadership, communication, teamwork, situation awareness and decision making, only [4,5,6, 10, 11, 30,31,32,33, 36, 40, 42, 46] (n = 13), and mixed (technical and non-technical) domains [7, 14, 18, 29, 35, 37, 44] (n = 8). Among NTS, communication was the most common domain.
With respect to the type of simulation modalities, simulations in the simulation center using only computer enhanced manikins [4,5,6, 10, 40, 42] or task trainers [17,18,19, 35, 38, 39, 41, 45] were common. One study, reported in two articles [4, 5], used a combination of mannequin simulators and simulated human patients. Simulations were primarily accomplished with learners participating in simulations in which equipment was installed in advance, such as a simulation center, captured on a camera, and observed synchronously by a facilitator in a remote location.
In some studies, simulated or standardized nurses were simulated via telephone [33, 36] or video [31, 32, 46]. Computer screen-based simulations, including virtual reality [11, 13, 14, 29, 30, 43], were used in many remotely facilitated simulations.
Facilitation
Before COVID-19, most studies connected learners and facilitators in a different location in the same building or on the same campus. However, under COVID-19, seven of eight studies connected participants across multiple locations (more than 3) in which participant connected from a different site [14, 40,41,42,43,44,45] (Table 2).
The most common tool for remote facilitation was videoconferencing ([3,4,5,6,7, 10, 11, 14, 17,18,19, 30,31,32, 34, 35, 38,39,40,41,42,43,44,45,46]) (n = 26, 89.7%). Two studies [33, 36] used a telephone for immediate feedback after simulated paging education. One study [29] employed the verbal and synchronous chat function in Second Life® (https://secondlife.com/) for within-event facilitation. There was one study using a specified web-based platform, Wizard of OZ Telemedicine Simulator [12], including synchronous text feedback [13]. Via the videoconferencing system, the facilitator could demonstrate the technical skills enhancing teaching and debriefing in nine studies [17,18,19, 35, 40,41,42, 44, 45] (Table 2).
Facilitators’ backgrounds varied depending on the subject matter of the simulation, but most facilitators were expert clinicians or educators. Eight studies [5, 6, 11, 13, 19, 33, 36, 42] indicated that the facilitators were trained or certified for the simulation, and three of them reported that the facilitators were trained for remote facilitation [5, 11, 42]. Remote facilitation was conducted during the simulation in 7 studies [19, 29, 30, 34, 35, 39, 41], post-simulation [7, 11, 31,32,33, 36, 37, 42] in 8, or both [4,5,6, 10, 13, 14, 17, 18, 38, 40, 43,44,45,46] in 17.
Learning outcomes of remotely facilitated simulations
Enhanced knowledge was the most commonly measured outcome. In most studies that compared facilitation methods, there were no significant differences in knowledge improvement between the on-site and remotely facilitated groups [5, 10, 11, 17, 34, 37]. Moreover, long term retention declined in both remotely and on-site facilitated groups [34]. One study using web-based immediate feedback improved knowledge in the remotely facilitated group more so than the group with no facilitation [13]. The pre- and post-studies [18, 30, 40, 44] for remote facilitation hint at improved knowledge as an outcome.
In the realm of technical skills, there were no significant differences in skills improvement between the on-site and remotely facilitated groups [17, 38]. In a simulation for focused assessment with sonography for trauma (FAST), the collective increase in knowledge was greater for the in-person group, whereas the improvement in FAST examination performance during the simulation was greater for the telementored group [38]. A remotely facilitated group improved their laparoscopic surgical technique more and reached a passing score more often than the self-practice group [19]. There was a statistically significant difference between on-site and remote facilitation in the change of clinical performance score to manage altered mental status to overdose, favoring on-site facilitation. In the same study, improvement in the management of dynamic hyperinflation with a mechanical ventilator revealed no difference between both types of facilitation [10]. In the pre- and post-studies, simulations with remote facilitation significantly enhanced in terms of writing medical records and summaries [14], in providing ultrasound-guided regional anesthesia [35], basic surgical skills (knot tying and suturing) [39], and neonatal resuscitation [44]. However, there was no change in the success rate of obtaining informed consent [46].
Other studies examined non-technical skills. When compared to on-site facilitation, remotely facilitated pediatric acute care teamwork training indicated no difference in performance between the groups [6]. In an interprofessional education (IPE) core competency simulation, there was statistically significant improvement in all scores when measured using pre-/post-testing [32].
Some studies have employed self-assessment by learners for program evaluation. In a study that compared remote and on-site facilitation, learners in both groups reported feeling greater comfort and competence for the simulation tasks after the course and 6 months later, without any difference between the groups [34]. Confidence was improved without a statistically significant difference between groups with various facilitation types in a FAST simulation [38], mechanical ventilation training [10], and the virtual gaming simulation of mental health assessment [11].
In an international remote facilitation study, learners reported significant improvement in their comfort, familiarity, and knowledge when inserting an intraosseous needle after simulation training [18]. Similarly, students’ aggregate confidence score rose significantly after interactive remote basic surgical skills during COVID-19 [41]. In addition, 90% of learners of pediatric patient care simulations agreed with the statements “I am more comfortable with pediatrics after this session” and “Participating improved my pediatric knowledge/skills” [42].
Learners’ preferences and satisfaction
There were differences in learners’ preferences and satisfaction with remote facilitation before and after COVID-19. In studies conducted before COVID-19, either on-site facilitation was preferred [4, 5, 32] or there was no difference in the preference for type of facilitation [17, 37]. There were two studies that used the Debriefing Assessment for Simulation in Healthcare (DASH) for evaluation of debriefing, and DASH scores were significantly higher for the in-person facilitation group than the remote facilitation group [10, 38]. When comparing in-person, remote, and self-debriefing methods, in-person facilitation was most favored, followed by remote facilitation and finally self-debriefing [11].
There have been no studies comparing different types of facilitation under COVID-19. Student peer-teachers and neonatal nursing staff reported that they still preferred traditional face-to face instruction after a neonatal resuscitation training that connected the clinical skills center with students at home [44]. However, in a study that involved remote facilitation only, learners reported that remote facilitation achieved the intended learning objectives [46], was helpful for practice [36], and learner satisfaction levels were either acceptable [14] or high [45]. Furthermore, learners were likely to recommend remotely facilitated training to others with a high net promoter score [43]. Residents reported that remote facilitation seemed like a good educational tool [39] and could be a reasonable substitute for simulation with in-person facilitation [40].
Barriers to, and enabling factors of, remote facilitation
Technical issues are among the most common barriers, such as low-speed internet in rural areas [17] or developing countries [19], and an unreliable internet connection, e.g., freezing, lost sound, or calls getting dropped [5, 10, 29, 31, 35, 40, 43, 44]. Moreover, audio-visual (AV) device operation issues— which interrupt learner engagement—have been reported, such as noise pollution from side conversations, echoes, and microphone feedback [40], as well as technical problems with AV devices in remote locations [32]. A few recent studies recommend checking for technical problems and providing an introduction to the connection modality or software in a pre-briefing session [41, 42]. In one study, the number of technical issues was greatest in the first session and declined over subsequent sessions [29]. In team simulations such as with IPE, it was difficult to gauge when the appropriate time was to speak using distance technology [32]. Headphones and high-definition cameras were utilized to overcome these technical constraints [44].
With respect to enabling factors of facilitation, a “time out (pause and reflect)” strategy and debriefing scripts were used to improve remote facilitation [42, 46]. A simulation coordinator, technician, assistant, or on-site expert helped with setup and troubleshoot any problem during remote facilitation [11, 36]. The facilitator and participants alike received training or orientation on remote technology [4, 5, 11, 30]. Modification via rehearsal or a pilot study prior to the actual simulation was helpful for remote facilitation [10, 11, 40].
Discussion
In general, remote facilitation has been applied to diverse types of healthcare simulation trainings. The most common method of synchronous connection is through videoconferencing software or applications. Remote facilitation in simulation education consistently improves knowledge, skills, and confidence, measured either by instructor evaluation or self-assessment, and there was no significant difference from on-site facilitation or self-debriefing. Before COVID-19, students reported that they preferred on-site facilitation to remote facilitation, but after COVID-19, students became satisfied with remote facilitation and considered it a reasonable substitute for simulation with in-person learning. The barriers identified the most frequently were those related to communications technology, where prior orientation or training for remote technology could improve remote facilitation.
Remote or distance simulation with synchronous facilitation has been around for over a decade [48,49,50], connecting learners who are separated from their instructors, via communications technology, using various simulation modalities including human patient simulators, SPs, and task trainers. Given the long history of use, terminology or nomenclature requires definitions. Standardized terminology and reporting standards can clarify the understanding of outcomes, align methodology for research, and aid in the replication of educational curricula in numerous settings. In our scoping review, we found multiple terms and nomenclature referring to similar and dissimilar activities. The terms telesimulation [3, 17,18,19, 37, 40, 42,43,44, 46], telementoring [34, 39], and telepresent training [10, 38] were all used to describe similar and dissimilar simulation activities using audiovisual communications technology as a platform to connect instructors and learners in separate locations.
The simulation modalities varied within these and included human patient simulators, simple manikins, SPs, task trainers, actors, and video recordings. The term virtual, while used as a generally accepted reference to computer-based simulation [13, 29, 51], has also been applied to non-computer based, remote, or distance simulation [30, 39, 40]. Recognizing the need for organization and definitions, in 2020, the Society for Simulation in Healthcare published an addendum to the Healthcare Simulation Dictionary, 2nd edition [52] to include language for conducting simulations at a distance.
In recognizing that definitions specifically for virtual simulation have been variably reported, Cant et al. [53] proposed a common nomenclature to describe the modalities of computer-based simulation, specifying 3 categorical descriptions to include the level of fidelity, the presence of immersion or interactivity, and the form of the patient, whether a simulated patient or a computer-generated avatar. This proposal was limited to computer-based simulation and did not address instructor facilitation during interactive simulations. We suggest that a similarly expanded framework be considered to describe remote facilitation. This framework could include (1) a description of facilitation timing (synchronous or asynchronous); (2) a method for connecting learners and instructors (e.g., videoconferencing, telephone, computer-based); (3) a simulation modality and its location with respect to the participants (e.g., a human-patient simulator, simple manikin, task trainer, SP, actor, computer-based); and finally (4) a method of facilitation, feedback, and/or debriefing (e.g., via chat, verbally, or through visual feedback or demonstration, facilitated video discussion, computer-based via avatars, etc.).
A touted advantage of computer-based simulation is the ability to provide asynchronous guidance and feedback. There were not enough strictly computer-based simulations included in this scoping review [11, 13, 29] to allow comparison of computer-based to other simulation modalities, since our search specified synchronous facilitation activities. Given the increased experience with computer-based simulation and the expected expansion of distance learning, we anticipate growth in this area. More studies comparing computer-based simulation to other methods of remote simulation are needed. Computer-based simulation does not necessarily require active synchronous facilitation, nor does it mean that learners and instructors must be physically separated, although they may be.
Learner outcomes at Kirkpatrick levels 1 (reactions) and/or 2 (knowledge and skill acquisition) were noted in all reports. Level 2 was observed in 27, and level 1 in 25 reports. Level 3 and 4 outcomes were mentioned in 2 studies. Learners readily accepted and mentioned positive attitudes regarding remote facilitation, and knowledge outcomes improved uniformly using pre-/post-intervention assessments. Most studies did not make direct comparisons between remote and on-site in-person scenario facilitation and/or debriefing. The six studies that included comparisons showed no difference in knowledge outcomes or latency of knowledge decay. Kirkpatrick level 2 outcomes, regarding technical skills acquisition with remote facilitation, were demonstrably positive in reports on ultrasound and laparoscopic skills. However, direct comparisons were not uniformly equivalent, with some cases exhibiting better learning outcomes through on-site facilitation. These limited findings suggest that remote facilitation, when employed using optimum techniques, may yield equivalent knowledge outcomes, warranting further study of outcomes and determination of best practices with respect to remote facilitation instructional techniques, including immediate versus delayed individualized feedback, group debriefing formats, scenario facilitation approaches, and the selection of learning objectives (e.g., technical skills and/or knowledge).
Remote facilitation was conducted prior to COVID-19 in 21 reports and in 8 since COVID-19 restrictions in many healthcare education programs resulted in the transition of varying proportions of traditional curricula to distance and remote learning strategies. Prior to COVID-19, learners preferred on-site facilitation and scored on-site debriefers more highly than remote debriefers. More positive learner and facilitator level 1 reactions, including preferences, equivalency, and net promotor scores for remote facilitation in reports of learner experiences, were reported following the onset of the COVID-19 pandemic The positive reactions toward remote facilitation in the COVID era, while not directly compared to remote facilitation outcomes in the pre-COVID era, imply that deepening one’s familiarity with remote educational experiences and the adaptation of personal self-learning strategies may contribute to acceptance and effectiveness of novel approaches to distance learning, including remote facilitation of simulation-based healthcare education. On the other hand, in one survey administered to any profession involved in healthcare simulation in 2021, 67% of respondents considered the involvement of learners in distance simulation to be more challenging than in-person simulation. In particular, 52% of respondents believed that distance simulation made it more difficult to achieve learning objectives, but 40% thought they were similar to individual simulations [54]. To succeed in remote facilitated simulation education, both learners and instructors should be prepared and trained in techniques for this new trend of education.
This study contains a systematic, detailed review of the literature available for remote facilitation. We chose the scoping review method to derive a broader range of results and criteria since there was a lack of predefined criteria for remote facilitation and related learning outcomes. Gray literature, including editorials, interviews, news, non-systematic reviews, and non-peer reviewed literature were excluded due to lack of robust source verification and/or sufficient detail regarding simulation techniques or facilitation methods to meet the evaluation criteria of this scoping review. However, the publications of simulation studies reported using diverse study types resulted in a significant heterogeneity of studies, posing a challenge for data comparison. Finally, many simulation education studies did not adequately report the types and methods of facilitation for inclusion in this scoping review. For future research, the development of standardized reporting guidelines for simulation education and facilitation is essential [55].
The COVID-19 pandemic persisted and lasted longer than expected, and simulation centers have gradually transformed to meet the circumstances of the COVID-19 pandemic. In our search, we targeted studies released before April 2021, and the COVID-19 pandemic continues so far. In this context, more studies on remote facilitation may have been published after our search. Because we wanted to investigate the nature of remote facilitation and set the scope for it (versus a response technology in a particular situation such as COVID-19), it was enough to investigate the research of the above period.
This study offers insight into remote facilitation in healthcare simulations. Our scoping review indicates that remote facilitation has been widely accepted across many healthcare professions and various kinds of simulation modalities. Remote facilitation has been used to overcome logistical problems in terms of synchronous, multi-location education, as well as to improve knowledge, skills, and confidence measured by instructor evaluation or self-assessment. As learners have grown more accustomed to remote facilitation amidst COVID-19 and their preference for it has increased, new education through high-quality remote facilitation can be considered and adapted in a changing educational context.
Data availability
The code of database search during this study are included in the supplementary material.
References
Said JT, Schwartz AW. Remote Medical Education: adapting Kern’s Curriculum Design to Tele-teaching. Med Sci Educ. 2021;31:805–12.
Rose S. Medical Student Education in the time of COVID-19. JAMA. 2020;323:2131–2.
McCoy CE, Sayegh J, Alrabah R, Yarris LM. Telesimulation: an innovative tool for health professions education. AEM Educ Train. 2017;1:132–6.
Duch Christensen M, Oestergaard D, Dieckmann P, Watterson L. Learners’ perceptions during Simulation-Based training: an interview study comparing Remote Versus locally facilitated Simulation-Based training. Simul Healthc. 2018;13:306–15.
Christensen MD, Rieger K, Tan S, Dieckmann P, Østergaard D, Watterson LM. Remotely Versus locally facilitated Simulation-based training in management of the deteriorating patient by newly graduated Health Professionals: a controlled trial. Simul Healthc. 2015;10:352–9.
Ohta K, Kurosawa H, Shiima Y, Ikeyama T, Scott J, Hayes S, et al. The effectiveness of Remote Facilitation in Simulation-Based Pediatric Resuscitation Training for Medical Students. Pediatr Emerg Care. 2017;33:564–9.
Hayden EM, Navedo DD, Gordon JA. Web-conferenced simulation sessions: a satisfaction survey of clinical simulation encounters via remote supervision. Telemed J E Health. 2012;18:525–9.
Ahmed R, King Gardner A, Atkinson SS, Gable B. Teledebriefing: connecting learners to faculty members. Clin Teach. 2014;11:270–3.
Ahmed RA, Atkinson SS, Gable B, Yee J, Gardner AK. Coaching from the Sidelines: examining the impact of Teledebriefing in Simulation-Based training. Simul Healthc. 2016;11:334–9.
Ciullo A, Yee J, Frey JA, Gothard MD, Benner A, Hammond J, et al. Telepresent mechanical ventilation training versus traditional instruction: a simulation-based pilot study. BMJ STEL. 2018;5:bmjstel–2017.
Verkuyl M, Atack L, McCulloch T, Liu L, Betts L, Lapum JL, et al. Comparison of debriefing methods after a virtual Simulation: an experiment. Clin Simul Nurs. 2018;19:1–7.
Katz A, Basis F, Shtub A. Using Wizard of Oz technology for telemedicine. Health Syst. 2015;4:224–35.
Katz A, Tepper R, Shtub A. Simulation training: evaluating the instructor’s contribution to a wizard of oz simulator in obstetrics and gynecology ultrasound training. JMIR Med Educ. 2017;3:e8.
Kasai H, Shikino K, Saito G, Tsukamoto T, Takahashi Y, Kuriyama A, et al. Alternative approaches for clinical clerkship during the COVID-19 pandemic: online simulated clinical practice for inpatients and outpatients-A mixed method. BMC Med Educ. 2021;21:149.
Rojas-Muñoz E, Cabrera ME, Lin C, Sánchez-Tamayo N, Andersen D, Popescu V, et al. Telementoring in Leg Fasciotomies via Mixed-Reality: clinical evaluation of the STAR platform. Mil Med. 2020;185(Suppl 1):513–20.
Nurhan Abbud JB. A systematic review of telementoring in modern surgical education: modalities available and their effectiveness.
Jewer J, Parsons MH, Dunne C, Smith A, Dubrowski A. Evaluation of a Mobile Telesimulation Unit to train rural and remote practitioners on high-acuity low-occurrence procedures: pilot randomized controlled trial. J Med Internet Res. 2019;21:e14587.
Mikrogianakis A, Kam A, Silver S, Bakanisi B, Henao O, Okrainec A, et al. Telesimulation: an innovative and effective tool for teaching novel intraosseous insertion techniques in developing countries. Acad Emerg Med. 2011;18:420–7.
Okrainec A, Henao O, Azzie G. Telesimulation: an effective method for teaching the fundamentals of laparoscopic surgery in resource-restricted countries. Surg Endosc. 2010;24:417–22.
Fung JTC, Zhang W, Yeung MN, Pang MTH, Lam VSF, Chan BKY, et al. Evaluation of students’ perceived clinical competence and learning needs following an online virtual simulation education programme with debriefing during the COVID-19 pandemic. Nurs Open. 2021;8:3045–54.
Shin H, Rim D, Kim H, Park S, Shon S. Educational characteristics of virtual simulation in nursing: an integrative review. Clin Simul Nurs. 2019;37:18–28.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467–73.
Peters M, Godfrey C, McInerney P, Munn Z, Trico A, Khalil H. Chapter 11: scoping reviews. In: Aromataris E, Munn Z, editors. JBI manual for evidence synthesis. JBI; 2020.
Peters MDJ, Godfrey CM, Khalil H, McInerney P, Parker D, Soares CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13:141–6.
Bramer WM, Giustini D, de Jonge GB, Holland L, Bekhuis T. De-duplication of database search results for systematic reviews in EndNote. J Med Libr Assoc. 2016;104:240–3.
Cheng SH, Augustin C, Bethel A, Gill D, Anzaroot S, Brun J, et al. Using machine learning to advance synthesis and use of conservation and environmental evidence. Conserv Biol. 2018;32:762–4.
critical-appraisal-tools. - Critical Appraisal Tools | Joanna Briggs Institute. https://jbi.global/critical-appraisal-tools. Accessed 9 Jan 2022.
Munn Z, Moola S, Riitano D, Lisy K. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int J Health Policy Manag. 2014;3:123–8.
Shershneva M, Kim J-H, Kear C, Heyden R, Heyden N, Lee J, et al. Motivational interviewing workshop in a virtual world: learning as avatars. Fam Med. 2014;46:251–8.
So M, Dziuban EJ, Franks JL, Cobham-Owens K, Schonfeld DJ, Gardner AH, et al. Extending the reach of pediatric emergency preparedness: a virtual tabletop exercise targeting children’s needs. Public Health Rep. 2019;134:344–53.
Phillips TA, Munn AC, George TP. Assessing the impact of telehealth objective structured clinical examinations in graduate nursing education. Nurse Educ. 2020;45:169–72.
Wen A, Wong L, Ma C, Arndt R, Katz AR, Richardson K, et al. An interprofessional team simulation exercise about a complex geriatric patient. Gerontol Geriatr Educ. 2019;40:16–29.
Cetrone E, Mutter K, Pedersen K, Shah N, Martindale J. A paging training program for a fourth-year internship readiness course. MedEdPORTAL. 2020;16:11021.
Altieri MS, Carmichael H, Jones E, Robinson T, Pryor A, Madani A. Educational value of telementoring for a simulation-based fundamental use of surgical energy™ (FUSE) curriculum: a randomized controlled trial in surgical trainees. Surg Endosc. 2020;34:3650–5.
Burckett-St Laurent DA, Cunningham MS, Abbas S, Chan VW, Okrainec A, Niazi AU. Teaching ultrasound-guided regional anesthesia remotely: a feasibility study. Acta Anaesthesiol Scand. 2016;60:995–1002.
Heidemann LA, Kempner S, Walford E, Chippendale R, Fitzgerald JT, Morgan HK. Internal medicine paging curriculum to improve physician-nurse interprofessional communication: a single center pilot study. J Interprof Care. 2020;:1–4.
McCoy CE, Sayegh J, Rahman A, Landgorf M, Anderson C, Lotfipour S. Prospective randomized crossover study of telesimulation versus standard simulation for teaching medical students the management of critically ill patients. AEM Educ Train. 2017;1:287–92.
Poland S, Frey JA, Khobrani A, Ondrejka JE, Ruhlin MU, George RL, et al. Telepresent focused Assessment with Sonography for Trauma Examination Training Versus Traditional Training for Medical students: a Simulation-Based pilot study. J Ultrasound Med. 2018;37:1985–92.
Trujillo Loli Y, D’Carlo Trejo Huamán M, Campos Medina S. Telementoring of in-home real-time laparoscopy using whatsapp messenger: an innovative teaching tool during the COVID-19 pandemic. A cohort study. Ann Med Surg (Lond). 2021;62:481–4.
Patel SM, Miller CR, Schiavi A, Toy S, Schwengel DA. The sim must go on: adapting resident education to the COVID-19 pandemic using telesimulation. Adv Simul (Lond). 2020;5:26.
Quaranto BR, Lamb M, Traversone J, Hu J, Lukan J, Cooper C, et al. Development of an interactive Remote Basic Surgical Skills Mini-Curriculum for Medical Students during the COVID-19 pandemic. Surg Innov. 2021;28:220–5.
Yang T, Buck S, Evans L, Auerbach M. A telesimulation elective to provide medical students with pediatric patient care experiences during the COVID pandemic. Pediatr Emerg Care. 2021;37:119–22.
Montgomery EE, Thomas A, Abulebda K, Sanseau E, Pearson K, Chipman M, et al. Development and implementation of a pediatric telesimulation intervention for nurses in community emergency departments. J Emerg Nurs. 2021;47:818–823e1.
Mileder LP, Bereiter M, Wegscheider T. Telesimulation as a modality for neonatal resuscitation training. Med Educ Online. 2021;26:1892017.
Tan SHX, Ansari A, Ali NMI, Yap AU. Simulation design and students’ satisfaction with home-based simulation learning in oral health therapy. J Dent Educ. 2021;85:847–55.
LaMarra D, French J, Bailey C, Sisko MT, Coughlin-Wells K, Agus MSD, et al. A novel framework using remote telesimulation with standardized parents to improve research staff preparedness for informed consent in pediatric critical care research. Pediatr Crit Care Med. 2020;21:e1042–51.
Tan AL, Trauma Coordinators and Trauma Service Representatives, Nadkarni N, Wong TH. The price of personal mobility: burden of injury and mortality from personal mobility devices in Singapore - a nationwide cohort study. BMC Public Health. 2019;19:880.
Berg BW, Alverson D, Mccarty T, Sinclair N, Hudson D, Vincent DS. Standardized patient interviewing with remote interactive technologies. J Telemed Telecare. 2007;13 3suppl:14–7.
Berg BW, Wong L, Vincent DS. Teaching nursing skills at a distance using a remotely controlled human patient simulator. J Telemed Telecare. 2007;13 3suppl:17–9.
Berg BW, Beamis EK, Murray WB, Boedeker BH. Remote videolaryngoscopy skills training for pre-hospital personnel. Stud Health Technol Inform. 2009;142:31–3.
Verkuyl M, Lapum JL, Hughes M, McCulloch T, Liu L, Mastrilli P, et al. Virtual Gaming Simulation: exploring Self-Debriefing, virtual debriefing, and In-person debriefing. Clin Simul Nurs. 2018;20:7–14.
Lioce L. In:, editors. Healthcare Simulation Dictionary. 2nd ed. Agency for Healthcare Research and Quality; 2020.
Cant R, Cooper S, Sussex R, Bogossian F. What’s in a name? Clarifying the nomenclature of virtual simulation. Clin Simul Nurs. 2019;27:26–30.
Buléon C, Caton J, Park YS, Eller S, Buyck M, Kardong-Edgren S, et al. The state of distance healthcare simulation during the COVID-19 pandemic: results of an international survey. Adv Simul (Lond). 2022;7:10.
Cheng A, Kessler D, Mackinnon R, Chang TP, Nadkarni VM, Hunt EA, et al. Reporting guidelines for health care simulation research: extensions to the CONSORT and STROBE statements. Simul Healthc. 2016;11:238–48.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
JP, BW, and JL conceived the study. MK carried out the search and deduplication. JP, BW, JL, ES, and YE reviewed and appraised articles. BW and JL provided expertise in healthcare simulation. BW, JL, and JP extracted data and synthesized results from articles. JP and KH prepared the original draft of the manuscript. BW, JL, and JP reviewed and edited the draft manuscripts. All authors were involved in revising the manuscript and agreed to the final content.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was not required for this systematic review.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Park, J.O., Lee-Jayaram, J., Sato, E. et al. A scoping review of remote facilitation during simulation-based healthcare education. BMC Med Educ 23, 592 (2023). https://doi.org/10.1186/s12909-023-04551-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12909-023-04551-3