
Abstract
Background
Maintenance of effect following treatment with galcanezumab compared to placebo in adult patients with episodic or chronic migraine was evaluated.
Methods
In 2 similarly designed studies of patients with episodic migraine (6 months) and 1 study of patients with chronic migraine (3 months), patients randomized in a 1:1:2 ratio received a subcutaneous injection of galcanezumab 120 mg/month (after an initial loading dose of 240 mg) or 240 mg/month or placebo. Maintenance of effect during the double-blind phase was evaluated based on a comparison of the percentages of galcanezumab- and placebo-treated patients with maintenance of 30, 50, 75, and 100% response (defined as ≥30, ≥50, ≥75, and 100% reduction from baseline in monthly migraine headache days [MHD]) at an individual patient level. Logistic regression analyses were used for between treatment comparisons.
Results
A total of 1773 adult patients with episodic migraine (n = 444 for galcanezumab 120 mg; n = 435 for galcanezumab 240 mg; n = 894 for placebo for 2 studies pooled) and 1113 patients with chronic migraine (n = 278 for galcanezumab 120 mg; n = 277 for galcanezumab 240 mg; n = 558 for placebo) were evaluated. In patients with episodic migraine, ≥50% response was maintained in 41.5 and 41.1% of galcanezumab-treated patients (120 mg and 240 mg, respectively) for ≥3 consecutive months (until patient’s endpoint) and 19.0 and 20.5%, respectively, for 6 consecutive months and was significantly greater than the 21.4 and 8.0% of placebo-treated patients at ≥3 and 6 months consecutively (P < 0.001). Approximately 6% of galcanezumab-treated patients maintained ≥75% response all 6 months versus 2% of placebo-treated patients. Few galcanezumab-treated patients maintained 100% response. In patients with chronic migraine, 29% of galcanezumab-treated patients maintained ≥30% response all 3 months compared to 16% of placebo patients while ≥50% response was maintained in 16.8 and 14.6% of galcanezumab-treated patients (120 mg and 240 mg) and was greater than placebo (6.3%; p < 0.001). Few patients maintained ≥75% response.
Conclusions
Treatment with galcanezumab 120 mg or 240 mg demonstrated statistically significant and clinically meaningful persistence of effect in patients with episodic migraine (≥3 and 6 consecutive months) and in patients with chronic migraine (for 3 months).
Study identification and trial registration
Study Identification: EVOLVE-1 (I5Q-MC-CGAG); EVOLVE-2 (I5Q-MC-CGAH); REGAIN (I5Q-MC-CGAI)
Trial Registration
ClinicalTrials.gov; NCT02614183 (EVOLVE-1); NCT02614196 (EVOLVE-2); NCT02614261 (REGAIN)
Similar content being viewed by others


Background
Galcanezumab is a humanized monoclonal antibody, indicated for the prevention of migraine, that binds to calcitonin gene-related peptide (CGRP) and prevents its biological activity without blocking the CGRP receptor [1]. The efficacy of galcanezumab was examined in 3 randomized, double-blind, placebo-controlled, Phase 3 studies of galcanezumab (120 and 240 mg/month) in patients with episodic (EVOLVE-1 and EVOLVE-2 6-month studies) or chronic (REGAIN 3-month study) migraine [2,3,4]. The mean monthly percentages of galcanezumab-treated patients with episodic migraine or chronic migraine that achieved ≥50% reduction in MHD was greater than the percentages of placebo-treated patients (60% versus 36% to 39% and 27% versus 15%, respectively) [2,3,4]. For patients with episodic migraine, galcanezumab-treated patients experienced approximately 4 fewer MHD/month (versus 2 with placebo) and patients with chronic migraine had approximately 5 fewer MHD/month (versus 3 with placebo) with a similar effect in both galcanezumab dose groups [2,3,4].
Data on current treatments for migraine prevention support that patients on recently approved and older treatments for migraine prevention do achieve a ≥ 50% level of response [5,6,7]. However, the important question of whether a ≥ 50% reduction in monthly MHD is maintained over time has not been sufficiently addressed for both episodic and chronic migraine [5, 8,9,10]. Further, can the additional responses of ≥30, ≥75, and 100% reduction in monthly MHD, also recognized to be clinically meaningful, be maintained [11,12,13]? For patients on a preventive treatment, this is a particularly important aspect since patients seek a medication with a consistent efficacy profile over time. Clinically, tachyphylaxis has been reported frequently by patients and physicians.
The current study evaluated data from the placebo-controlled EVOLVE-1 and EVOLVE-2 episodic migraine trials and the REGAIN chronic migraine trial and compared galcanezumab treatment to placebo in the maintenance of ≥30% (chronic only), ≥50, ≥75, and 100% (episodic only) response in the reduction of MHD from baseline.
Methods
Study design
Detailed descriptions of the study design for the 2 episodic migraine (6-month) and 1 chronic migraine (3-month) double-blind studies, have been reported separately (ClinicalTrials.gov NCT02614183, NCT02614196, and NCT02614261) [2,3,4]. Briefly, adult patients were randomized 1:1:2 and received subcutaneous injections of galcanezumab 120 mg/month (after a 240 mg initial loading dose) or 240 mg/month or placebo. Episodic migraine was defined as having between 4 and 14 MHD and at least 2 migraine attacks per month [2, 3, 14]. Chronic migraine was defined as having headache ≥15 days per month for ≥3 months and having features of migraine headache ≥8 days per month [4, 14]. The continuation or start of any additional migraine preventive treatments was not permitted; the exception for patients with chronic migraine was the use of topiramate or propranolol provided they entered trial on a stable dose. The ≥50, ≥75, and ≥ 100% response rates during the 6-month (episodic) or 3-month (chronic) study periods were key secondary objectives (adjusted for multiple testing) and response rates at each month (episodic and chronic studies) were secondary outcomes (not adjusted for multiple testing). The study protocols were reviewed and approved by the appropriate institutional review board for each of the study sites. The studies were conducted according to Good Clinical Practice and the Declaration of Helsinki guidelines. Patients provided written informed consent before undergoing study procedures. The trials are registered with ClinicalTrials.gov (NCT02614183, NCT02614196, and NCT02614261).
Statistical method
Data from the 2 episodic migraine trials combined and 1 chronic migraine trial were included in the analysis. In these trials, a 30, 50, 75, and 100% response rate at each month was defined as the percentage of patients meeting a defined threshold (≥30, ≥50, ≥75, and 100%) in the reduction of the number of monthly MHD during the double-blind treatment period. Only patients with both a baseline and ≥ 1 month of non-missing post-baseline MHD values were included in the analysis. The evaluation of maintenance of effect during the double-blind treatment period was a comparison of the percentages of galcanezumab- and placebo-treated patients with maintenance of ≥30, ≥50, ≥75, and 100% response at the individual patient level. In the episodic studies, maintenance of response was calculated for those with at least 3 months (until patient’s endpoint) and 6 consecutive months and 3 consecutive months for chronic migraine. A logistic regression analysis was used for between-treatment group comparisons. At each month, a cumulative 50% maintenance of response was also calculated and defined as patients with ≥50% response at a specific month (or before) and all subsequent months. For repeated binary data of monthly ≥50% response and cumulative ≥50% sustained response, a categorical, pseudolikelihood-based repeated measures model was implemented with SAS PROC GLIMMIX [15]. Two-sided p-values were calculated and compared with significance level of 0.05.
Results
Patient disposition
Data from the episodic migraine trials were from 1773 adult patients with episodic migraine treated with 120 mg galcanezumab (n = 444), 240 mg galcanezumab (n = 435), or placebo (n = 894). Data from the chronic migraine trial were from 1113 patients with chronic migraine treated with 120 mg galcanezumab (n = 278), 240 mg galcanezumab (n = 277), or placebo (n = 558). Baseline demographics and disease characteristics of the episodic and chronic migraine populations show that over 80% were female, over 74% were white, had a mean age of 40 years, and had migraine disease duration of 20 years. As permitted by protocol for the chronic migraine trial, concomitant use of topiramate or propranolol during the double-blind phase, across all treatment groups, occurred in 10.3 and 3.6% of patients, respectively. At baseline, the mean MHD/month was 9.1 for episodic migraine and 19.3 for chronic migraine. The mean baseline Migraine Disability Assessment score for patients treated with galcanezumab or placebo was 33.1 for episodic migraine and 65.8 (galcanezumab) and 68.7 (placebo) for chronic migraine and was reflective of severe (episodic) and very severe (chronic) migraine disability. The mean baseline Migraine-Specific Quality of Life Questionnaire Role Function-Restrictive subdomain score for patients treated with galcanezumab or placebo with episodic migraine was 51.1 and 52.1, respectively, and with chronic migraine was 39.1 and 38.4, respectively. Patients with chronic migraine had greater functional impairment than patients with episodic migraine (Table 1).
Proportions of patients with ≥50% response
The model-estimated proportions of patients with episodic migraine achieving ≥50% response were significantly greater for both galcanezumab dose groups compared to placebo starting at Month 1 (p < 0.001) and at each month after (p < 0.001), as well as overall across 6 months (p < 0.001) (Table 2). For patients with chronic migraine, the model-estimated proportions of patients achieving ≥50% response was significantly greater for both dose groups compared to placebo starting at Month 1 (p < 0.001) and at each month after (p ≤ 0.004), as well as overall across 3 months (p < 0.001) (Table 2). The absolute values for the proportions of patients with episodic or chronic migraine that achieved ≥50% response were very similar to the estimated values proportions and are shown in Additional file 1: Table S1.
Maintenance of response
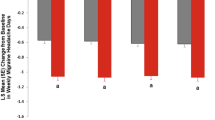
Significantly more patients with episodic migraine treated with galcanezumab in both dose groups (approximately 41%) maintained response of ≥50% fewer MHD for ≥3 consecutive months until patient’s endpoint compared to placebo (21%). Over Month 1 to Month 6, approximately 20% of galcanezumab-treated patients in both dose groups maintained a response of ≥50% fewer MHD that was significantly greater than placebo (8%) (Fig. 1).

Episodic migraine: proportions of patients with maintenance of ≥ 50% response for ≥ 3 consecutive months until patient’s endpoint and response from month 1 to month 6. a maintenance of ≥ 50% response for ≥ 3 consecutive months. b maintenance of ≥ 50% response from month 1 to month 6. Abbreviations: OR = odds ratio. *** = p < 0.001
In patients with chronic migraine, significantly more patients in both the 120 mg (17%) and 240 mg (15%) galcanezumab dose groups maintained a response of ≥50% fewer MHD for 3 consecutive months compared to placebo (6%) (Fig. 2). The difference between dose groups for either episodic or chronic migraine in the proportions of patients with maintenance of response was not significant.

Chronic migraine: proportions of patients with maintenance of ≥ 50% response for 3 consecutive months. Abbreviations: OR = odds ratio. *** = p < 0.001
The model-estimated proportions of patients with episodic migraine who maintained a response of ≥75 and 100% and those patients with chronic migraine who maintained a response of ≥30 and ≥ 75% are shown in (Table 3). The proportions of galcanezumab-treated patients with episodic migraine who maintained a response of ≥75% fewer MHD for 3 consecutive months until patient’s endpoint (19.7 and 21.3%) was significantly greater than placebo (8.5%; p < 0.001). While fewer, 6% of galcanezumab-treated patients maintained a response of ≥75% fewer MHD for all 6 months compared with 1.8% of placebo-treated patients. A small percentage of patients maintained 100% response for 3 consecutive months and very few maintained 100% response for all 6 months. The proportions of galcanezumab-treated patients with chronic migraine who maintained a response of ≥30% fewer MHD for all 3 months (29%) was significantly greater than placebo (16.4%; p < 0.001). The proportions of patients who maintained ≥75% fewer MHD for all 3 months was not different between the galcanezumab and placebo groups.
Characterization of patients with episodic migraine with ≥50% response at month 1
Among the 50.9 and 47.2% of galcanezumab 120 mg- and 240 mg-treated patients with episodic migraine who met ≥50% response at Month 1, the average reduction in MHD over the remaining 5 months of the double-blind phase was 66.6 and 71.5%. Of the 23.8% of placebo-treated patients with ≥50% response at Month 1, the average reduction in MHD was 63.2%. Further, among only those with ≥50% response at Month 1, 85.4 and 92.4% of patients in the 2 galcanezumab dose groups and 80.7% in the placebo group averaged at least a 40% response over the remaining 5 months. Moreover, 80.8 and 85.4% of patients in the 2 galcanezumab groups respectively and 71.1% of patients in the placebo group averaged at least ≥50% response over the remaining 5 months.
Cumulative and onset of maintenance of response
The cumulative maintenance of response is defined as individual patients who met ≥50% response starting at a given month (or before) and then all the months subsequent. The proportions of patients with episodic migraine in the galcanezumab 120 mg and 240 mg groups achieving cumulative maintenance of ≥50% response was superior to placebo at every month of the 6-month double-blind phase (p < 0.001) (Fig. 3). For example, 31% of patients with episodic migraine treated with galcanezumab 120 mg reached ≥50% at or before Month 3 and maintained that response in the subsequent months (Month 4 to Month 6). The difference between the galcanezumab dose groups for cumulative maintenance of response was not significant.

Cumulative maintained ≥ 50% response: percentages of patients with episodic migraine who reached ≥ 50% response at or before each month and all subsequent months
The onset of ≥50% maintenance of response and the percentage of patients with episodic or chronic migraine who reached ≥50% response at the specific month (but not before) and then maintained that response in the subsequent months of treatment is shown in Table 4. To illustrate the onset for patients with episodic migraine, 19, 6, and 6% of patients treated with galcanezumab 120 mg reached ≥50% response at Months 1, 2, and 3, respectively, and maintained that response in the subsequent months of treatment (Months 2 to 6, Months 3 to 6, and Month 4 to 6, respectively). Across the 6-month double-blind phase, onset of maintenance of response occurred for approximately 4 to 21% of galcanezumab-treated patients with highest rate occurring in Month 1. In all but one time point, the proportions of patients were greater in the galcanezumab treatment groups than the placebo group at each month. The exception was at 6 months where the proportions of patients were similar between the galcanezumab 120 mg (10.6%) and placebo (10.9%) groups.
In patients with chronic migraine, the proportions of patients treated with galcanezumab 120 mg or 240 mg achieving cumulative maintenance of ≥50% response was superior to placebo at every month of the 3-month double-blind phase (p < 0.001). At Month 3 or before, approximately 30% of patients in the galcanezumab treatment groups achieved and maintained ≥50% response (Fig. 4). The difference between the galcanezumab dose groups for cumulative maintenance of response was not significant. To illustrate the onset of the maintenance of ≥50% response for patients with chronic migraine (Table 4), 15, 5, and 11% of patients treated with galcanezumab 120 mg reached ≥50% response at Month 1, 2, and 3, respectively.

Cumulative maintained ≥ 50% response: percentages of patients with chronic migraine who reached ≥ 50% response at or before each month and all subsequent months
Safety and tolerability
The most commonly reported treatment-emergent adverse events (TEAE) were injection site-related pain, reaction, erythema, pruritus, and swelling. Discontinuation due to an injection site-related TEAE was low (< 0.5% across all 3 trials). There were no significant differences between galcanezumab and placebo in changes in vital signs and blood pressure. The safety profile between the 120 mg and 240 mg doses were similar [2,3,4].
Discussion
Treatment with galcanezumab 120 mg or 240 mg demonstrated statistically significant and clinically meaningful maintenance of effect in patients with episodic migraine (≥3 consecutive months until patient’s endpoint and 6 consecutive months) or chronic migraine (3 months). Starting at Month 1, about 20% of galcanezumab-treated patients (either dose group) with episodic migraine had a sustained response of ≥50% reduction of MHD over 6 months; about 41% of patients maintained ≥50% response over ≥3 months. Among only the galcanezumab-treated patients who had a ≥ 50% reduction of MHD in Month 1, an average reduction of MHD of ≥40 and ≥ 50%, was achieved by 89 and 83% of patients, respectively, in the remaining 5 months of treatment suggesting minimal loss of efficacy among Month 1 responders. In galcanezumab-treated patients with chronic migraine, about 15% showed a ≥ 50% reduction of MHD over 3 consecutive months. Sustained efficacy was also observed in the placebo groups of patients with episodic and with chronic migraine; however, the placebo response was always significantly inferior to galcanezumab treatment. For example, galcanezumab-treated patients with episodic migraine were well over 2 times more likely than placebo-treated patients to achieve a sustained ≥50% response at 6 months and overall. Similarly, galcanezumab-treated patients with chronic migraine were twice as likely than placebo-treated patients to achieve a sustained ≥50% response at 3 months and overall. Several studies have shown the importance of expectation for the size of the placebo response and so a relatively high placebo response, typical for controlled treatment studies in migraine, was not an unexpected observation in our analysis [16,17,18]. The placebo response rate is likely a result of intensive patient care within the setting of a study. Regardless, the importance of this analysis is based on the fact that responders do not develop tachyphylaxis, for example, by up-regulation of other mediators of neurovascular inflammation.
Studies with monoclonal antibodies have shown sustained levels of 50% as well as 75 and 100% response in patients with episodic or chronic migraine [10]. Based on pre-specified analyses for our study, about 41% of galcanezuamb-treated patients with episodic migraine maintained ≥50% response for ≥3 consecutive months until patient’s endpoint and is a clinically relevant finding. In the additional post-hoc analysis of assessing the cumulative and onset of maintenance of ≥50% response, most patients reach ≥50% response and all subsequent months starting at Month 1, with approximately similar percentages of patients reaching ≥50% response and all subsequent months starting at Month 2, 3, 4, 5, and 6. These findings were generally consistent in the chronic migraine study although the percentages of patients with maintenance of response were generally lower given the higher baseline number of MHD. The 50% responder rate has been used as a secondary end-point in other trials, for example, with topiramate and botulinum toxin, in episodic and chronic migraine [5, 7, 19]. Comparison of those results to our data are difficult because only the 50% responder rate at the end of the double-blind period or at the end of cycle with botulinum toxin without any monthly and maintenance of response analysis was published.
Early and sustained response to preventive treatment is of special relevance. There is some evidence that improvement with preventive treatment at 3 months might be a predictor of persistent remission [20]. In addition, there is emerging evidence that more severely affected patients with a history of medication overuse, a high frequency of migraine attacks, and previously ineffective preventive treatments require long-term preventive treatment to maintain a reduced attack frequency, even after withdrawal of the preventive medication [21,22,23].
The maintenance of effect in patients with episodic or chronic migraine were similar between the galcanezumab 120 mg and 240 mg dose. This finding is consistent with previous reports in which there were no meaningful differences in efficacy measures between the galcanezumab doses and as such, the recommended dose is 120 mg after an initial loading dose of galcanezumab 240 mg (given as two 120 mg injections) [2,3,4].
One of the limitations of this paper is that the response rate was defined based on the primary efficacy measure, reduction in the number of MHD only. Additional analyses could be conducted in further publications to assess the response rate based on other efficacy measures, such as days of acute medication use, and measures of function and disability.
Conclusions
Treatment with galcanezumab 120 mg or 240 mg demonstrated statistically significant and clinically meaningful maintenance of effect in patients with episodic migraine (at least 3 and 6 consecutive months) and in patients with chronic migraine (for 3 months).
Abbreviations
- CGRP:
-
Calcitonin gene-related peptide
- MHD:
-
Migraine headache days
References
Benschop RJ, Collins EC, Darling RJ, Allan BW, Leung D, Conner EM et al (2014) Development of a novel antibody to calcitonin gene-related peptide for the treatment of osteoarthritis-related pain. Osteoarthr Cartil 22:578–585
Stauffer VL, Dodick DW, Zhang Q, Carter JN, Ailani J, Conley RR (2018) Evaluation of galcanezumab for the prevention of episodic migraine: the EVOLVE-1 randomized clinical trial. JAMA Neurology 75:1080–1088
Skljarevski V, Matharu M, Millen BA, Ossipov MH, Kim BK, Yang JY (2018) Efficacy and safety of galcanezumab for the prevention of episodic migraine: results of the EVOLVE-2 phase 3 randomized controlled clinical trial. Cephalalgia 38:1442–1454
Detke HC, Goadsby PJ, Wang S, Friedman DI, Selzler KJ, Aurora SK (2018) Galcanezumab in chronic migraine: the randomized, double-blind, placebo-controlled REGAIN study. Neurology [Epub ahead of print, November 16]
Diener HC, Bussone G, Van Oene JC, Lahaye M, Schwalen S, Goadsby PJ, TOPMAT-MIG-201(TOP-CHROME) study group (2007) Topiramate reduces headache days in chronic migraine: a randomized, double-blind, placebo-controlled study. Cephalalgia 27:814–823
Tepper S, Ashina M, Reuter U, Brandes JL, Doležil D, Silberstein S et al (2017) Safety and efficacy of erenumab for preventive treatment of chronic migraine: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol 16:425–434
Dodick DW, Ashina M, Brandes JL, Kudrow D, Lanteri-Minet M, Osipova V et al (2018) ARISE: a phase 3 randomized trial of erenumab for episodic migraine. Cephalalgia 38:1026–1037
Brandes JL, Saper JR, Diamond M, Couch JR, Lewis DW, Schmitt J et al (2004) Topiramate for migraine prevention a randomized controlled trial. JAMA 291:965–973
Dodick DW, Turkel CC, DeGryse RE, Aurora SK, Silberstein SD, Lipton RB et al (2010) OnabotulinumtoxinA for treatment of chronic migraine: pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 50:921–936
Halker Singh RB, Aycardi E, Bigal ME, Loupe PS, McDonald M et al (2018) Sustained reductions in migraine days, moderate-to-severe headache days and days with acute medication use for HFEM and CM patients taking fremanezumab: post-hoc analyses from phase 2 trials. Cephalalgia:333102418772585 [Epub ahead of print]
Tfelt-Hansen P, Pascual J, Ramadan N, Dahlöf C, D'Amico D, Diener HC et al (2012) Guidelines for controlled trials of drugs in migraine: third edition. A guide for investigators. Cephalalgia 32:6–38
Silberstein S, Tfelt-Hansen P, Dodick DW, Limmroth V, Lipton RB, Pascual J et al (2008) Guidelines for controlled trials of prophylactic treatment of chronic migraine in adults. Cephalalgia 28:484–495
Tassorelli C, Diener HC, Dodick DW, Silberstein SD, Lipton RB, Ashina M et al (2018) Guidelines of the international headache society for controlled trials of preventive treatment of chronic migraine in adults. Cephalalgia 38:815–832
[ICHD-3] Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013;33:629-808.
SAS Institute Inc (2017) SAS/STAT® 14.3 User’s Guide. SAS Institute Inc, Cary
Diener HC, Schorn CF, Bingel U, Dodick DW (2008) The importance of placebo in headache research. Cephalalgia 28(10):1003–1011
Diener HC (2010) Placebo effects in treating migraine and other headaches. Curr Opin Investig Drugs 11(7):735–739
Meissner K, Fässler M, Rücker G, Kleijnen J, Hróbjartsson A, Schneider A et al (2013) Differential effectiveness of placebo treatments: a systematic review of migraine prophylaxis. JAMA Intern Med 173:1941–1951
Silberstein SD, Dodick DW, Aurora SK, Diener HC, DeGryse RE, Lipton RB et al (2015) Percent of patients with chronic migraine who responded per onabotulinumtoxinA treatment cycle: PREEMPT. J Neurol Neurosurg Psychiatry 86:996–1001
Bhoi SK, Kalita J, Misra UK (2013) Is 6 months of migraine prophylaxis adequate? Neurol Res 35:1009–1014
Wöber C, Wöber-Bingöl C, Koch G, Wessely P (1991) Long-term results of migraine prophylaxis with flunarizine and beta-blockers. Cephalalgia 11(6):251–256
Pascual J, El Berdei Y, Gómez-Sánchez JC (2007) How many migraine patients need prolonged (>1 year) preventive treatment? Experience with topiramate. J Headache Pain 8(2):90–93
Silva-Néto RP, Almeida KJ, Bernardino SN (2014) Analysis of the duration of migraine prophylaxis. J Neurol Sci 337(1–2):38–41
Acknowledgements
Medical writing support was provided by Millie Hollandbeck and editorial support by Stephanie Bruns (Synchrogenix) which was funded by Eli Lilly and Company, Indianapolis, Indiana, USA. The authors thank Mallikarjuna Rettiganti, PhD (Eli Lilly and Company) for additional statistical review.
Funding
This study was funded by Eli Lilly and Company, Indianapolis, Indiana, USA.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to proprietary reasons but are available from the corresponding author on reasonable request.
Prior data disclosures
Data were presented in part at the American Headache Society 60th Annual Meeting, June 28–July 1, 2018, San Francisco, CA, USA; the 17th Biennial Migraine Trust International Symposium, September 6–9, 2018, London, England, UK; and the 12th European Headache Federation, September 28–30, 2018, Florence, Italy.
Author information
Authors and Affiliations
Contributions
SF, QZ, VLS, SKA, and MJAL participated in the conception, design and acquisition. QZ performed all statistics and analyses of the data and SF, QZ, VLS, SKA, and MJAL participated in the interpretation of the data. SF, QZ, VLS, and MJAL were major contributors for the drafting of the manuscript and revision for intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocols were reviewed and approved by the appropriate institutional review board for each of the study sites. The studies were conducted according to Good Clinical Practice and the Declaration of Helsinki guidelines. Patients provided written informed consent before undergoing study procedures.
Consent for publication
Not applicable.
Competing interests
Stefanie Förderreuther, MD Steffi.Foerderreuther@med.uni-muenchen.de
Ludwig-Maximilians-University of Munich, Department of Neurology
Speaker’s Bureau: Novartis, Sanofi
Consultation: Sanofi
Honoraria: Allergan, Hormosan Pharma, AstraZeneca
Advisory Boards: Novartis, Eli Lilly
Qi Zhang, PhD qi.zhang@sanofi.com
Employee of Sanofi, Bridgewater, NJ, USA
Former employee of Eli Lilly and Company, and/or one of its subsidiaries, Indianapolis, IN, USA
Virginia L. Stauffer, PharmD vstauffer@lilly.com
Employee of Eli Lilly and Company, and/or one of its subsidiaries, Indianapolis, IN, USA
Sheena K. Aurora, MD sheena.aurora@lilly.com
Employee of Eli Lilly and Company, and/or one of its subsidiaries, Indianapolis, IN, USA
Miguel JA Láinez, MD, PhD miguel.lainez@sen.es
Hospital Clínico Universitario, Universidad Católica de Valencia, Spain
Research Grants: Allergan, Amgen, ATI, Bayer, Boehringer, electroCore, Eli Lilly, Medtronic, Novartis, Otsuka, Roche, Teva and UCB
Consultation: Allergan, Amgen, ATI, Bayer, Boehringer, electroCore, Eli Lilly, Medtronic, Novartis, Otsuka, Roche, Teva and UCB
Honoraria: Allergan, Amgen, ATI, Bayer, Boehringer, electroCore, Eli Lilly, Medtronic, Novartis, Otsuka, Roche, Teva and UCB
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Table S1. Absolute proportion of patients with episodic and chronic migraine with ≥50% response. (DOCX 48 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Förderreuther, S., Zhang, Q., Stauffer, V.L. et al. Preventive effects of galcanezumab in adult patients with episodic or chronic migraine are persistent: data from the phase 3, randomized, double-blind, placebo-controlled EVOLVE-1, EVOLVE-2, and REGAIN studies. J Headache Pain 19, 121 (2018). https://doi.org/10.1186/s10194-018-0951-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-018-0951-2