
Abstract
Background
Rett syndrome (RTT) is an X-linked neurodevelopmental disease affecting predominantly females caused by MECP2 mutations. Although RTT is classically considered a monogenic disease, a stable proportion of patients, who do not exhibit MECP2 sequence variations, does exist. Here, we have attempted at uncovering genetic causes underlying the disorder in mutation-negative cases by whole genome analysis using array comparative genomic hybridization (CGH) and a bioinformatic approach.
Results
Using BAC and oligonucleotide array CGH, 39 patients from RTT Russian cohort (in total, 354 RTT patients), who did not bear intragenic MECP2 mutations, were studied. Among the individuals studied, 12 patients were those with classic RTT and 27 were those with atypical RTT. We have detected five 99.4 kb deletions in chromosome Xq28 affecting MECP2 associated with mild manifestations of classic RTT and five deletions encompassing MECP2 spanning 502.428 kb (three cases), 539.545 kb (one case) and 877.444 kb (one case) associated with mild atypical RTT. A case has demonstrated somatic mosaicism. Regardless of RTT type and deletion size, all the cases exhibited mild phenotypes.
Conclusions
Our data indicate for the first time that no fewer than 25% of RTT cases without detectable MECP2 mutations are caused by Xq28 microdeletions. Furthermore, Xq28 (MECP2) deletions are likely to cause mild subtypes of the disease, which can manifest as both classical and atypical RTT.
Similar content being viewed by others


Background
Rett syndrome (RTT // MIM 312750) is an X-linked neurodevelopmental disorder caused by MECP2 mutations that affects almost exclusively girls. Clinically, the disease presents with developmental regression accompanied by the loss of hand skills, mobility and speech. In addition, RTT is phenotypically characterized by stereotypic hand movements, respiratory abnormalities, scoliosis, growth deficits, hypotonia, microcephaly and seizures. Intragenic MECP2 mutations are the main cause of RTT. However, there does exist a proportion of RTT females (5-10%) without detectable MECP2 mutations [1–6]. To date, genetic causes in these RTT cases remain largely unknown.
Recently, it has been shown that Xq28 microdeletions can affect MECP2 leading to RTT-like phenotype [7, 8]. Since these submicroscopic genome variations were commonly detected in children with presumably idiopathic intellectual disability, autism, epilepsy and/or congenital anomalies [7], it is probable that submicroscopic Xq28 deletions are not rare and can be associated with RTT. In this context, one can suggest Xq28 deletions spanning the MECP2 gene to be a potential cause of the disease in affected females without mutations detectable by Sanger sequencing. Surprisingly, to the best our knowledge, there was no systematic whole genome analysis of MEPC2-mutation negative RTT patients. In the available literature, we have only found studies describing whole genome analysis of RTT females by array comparative genomic hybridization (CGH), which was performed for testing whether copy number variants (CNVs) are able to modulate the phenotype in mutation-positive RTT cases [9, 10]. Thus, we decided to share our data on the evaluation of MEPC2-mutation negative females from Russian RTT cohort addressed by BAC and oligonucleotide array CGH with bioinformatic analysis.
Results
In the present study, we have selected MECP2- mutation-negative patients from the Russian RTT cohort (354 RTT girls). The cohort includes 262 classic and 92 atypical RTT females according to revised diagnostic criteria [11], who have been previously found to bear a MECP2 mutation in 95.4% and 70.7% of cases, respectively [12–15]. The remaining RTT girls were classified as follows: classic RTT — 12 cases out of 262 patients (4.6%) and atypical RTT — 27 cases, among them 17 girls with “forme fruste”; 6 with a late regression; 4 girls with early-onset seizures. All the selected patients (n = 39) have been evaluated by BAC and oligonucleotide array CGH (Human BAC Array-System, Perkin Elmer and NimbleGen 135 K whole genome tiling array) using a specific bioinformatic protocol for data analysis. Five classic RTT cases and five atypical RTT cases were found to be associated with Xq28 deletions (Figure 1). The occurrence of Xq28 deletions in RTT females without MECP2 mutations detectable by Sanger sequencing was estimated at about 26%. These cases were all found to exhibit RTT-specific epigenetic phenomena (unusual replication pattern or type C undetectable in general population) observed at cytogenetic (cytological) level.

Flow chart illustrating the diagnostic workup for genetic evaluation in Russian RTT cohort.
Firstly, the deletions were detected in girls with atypical RTT by BAC array CGH. Oligonucleotide array CGH was then used to confirm the deletions and to narrow the breakpoints given according to hg19 assembly (Feb. 2009 Genome Reference Consortium GRCh37). Among them, three patients exhibited exactly the same (recurrent) deletions encompassing genomic loci in Xq28: arr Xq28(153,145,800-153,648,227)×1 (Additional file 1: Figure S1). The size of these three deletions was estimated as 502,428 bp. Another RTT patient has demonstrated an Xq28 deletion with the same distal breakpoint (arr Xq28(153,108,683-153,648,227)×1), the size of which is 539,545 bp (Additional file 2: Figure S2). The largest Xq28 deletion detected in this study spans 877,444 bp (arr Xq28(152,731,931-153,609,374)×1) and is featured by an unexpectedly mild RTT phenotype (Additional file 3: Figure S3). All the deletions detected in atypical RTT cases were found to encompass the MECP2 gene (Figure 2). Deletions were confirmed by fluorescence in situ hybridization (FISH). Molecular data (size and breakpoint locations) and clinical parameters (additional phenotypic features) of these deletions are summarized in Table 1.

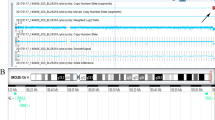
Schematic overview of detected Xq28 deletions depicted using UCSC Genome Browser (Human Feb. 2009 (GRCh37/hg19) Assembly) (see also Table 1 for details).
Secondly, oligonucleotide array CGH has indentified another five deletions in nearly classic RTT patients. All these deletions have the same breakpoints (same size) (Table 1, Additional file 4: Figure S4): about 99.4 kb (arr Xq28(153,213,483-153,312,854) ×1). One case was found to be associated with mosaic deletion (Table 1), which was confirmed by FISH through studying 100 metaphase plates and 1000 interphase nuclei (unfortunately, other tissues were not available for analysis due to parents’ lack of further cooperation). According to molecular analysis, two MECP2 exons were affected (Figure 2, Additional file 4: Figure S4). However, taking into account the probe distribution on the NimbleGen 135 K whole genome tiling array, complete MECP2 deletion on one chromosome X homologue cannot be excluded. It is intriguing to note that further molecular cytogenetic confirmation analysis demonstrated a discrepancy between array CGH and FISH, which mainly concerned the mosaic case hallmarked by an apparent difference between proportions of cells affected by MECP2 deletion (Figure 3). Apart from Xq28 deletions, other CNVs were also detected. These were losses within 3p13, 3q27.1, 11p13, 15q11.2, Xp22.13 and gains within 1q21, 11p14.3, 15q14, 22q11.21. We recognize that their intrinsic pathogenic value can be appreciable and requires to be addressed by further bioinformatics and molecular analyses (more detailed data will be presented elsewhere).

FISH demonstrating mosaic MECP2 deletion. (A) interphase FISH: two signals correspond to two MECP2 copies in a nucleus without deletion and a single signal is observed in a nucleus lacking one MECP2 copy; (B) percentages of abnormal cells detected by array CGH and FISH.
An attempt at correlation between genotype and phenotype in reported cases and cases with MECP2 mutations has shown that Xq28 (MECP2) microdeletions are likely to cause specific subtypes of RTT, which are clinically milder than the phenotype resulted from intragenic MECP2 sequence variations. Deletions were featured by late regression age, intact ability to walk, mild dyspraxia of hand movements, and microcephaly absence. Although some cases fulfil both canonical and more recent diagnostic criteria for classic RTT [11, 16], we did observe that almost all the RTT symptoms (addressed by a scale developed specifically for the evaluation of RTT symptoms severity [8, 14, 15]) in cases of Xq28 deletions are comparably milder than those caused by intragenic MECP2 mutations. Additional clinical signs featuring this RTT subtype are low birth weight in ~2/3 of cases, malformations (vascular dorsal skin hemangiomatosis, verrucous patches resembling incontinentia pigmenti phenotype, cerebellar vermis hypoplasia, polycystic kidney disease, patent foramen ovale) and facial dysmorphisms.
Discussion
RTT is a common monogenic cause of neurodevelopmental abnormalities in females [1–6]. Although it has been repeatedly noted that the phenotype of affected girls depends on the presence or absence of MECP2 mutation, the latter have not been ever considered as an exclusive criterion for RTT [11, 16, 17]. Apparently, non-striking phenotypic differences between a significant proportion of mutation-positive and mutation-negative cases [17] indicate that the same genetic defect causes the disease in mutation-negative cases. Currently, there have been reported several genomic abnormalities (i.e. 14q12 microdeletions) associated with RTT [5–7, 18, 19]. However, these genomic rearrangements are unlikely to cover all the mutation-negative RTT cases. Here, we report on the commonest cause of RTT in cases without detectable MECP2 mutations. To our knowledge, this is the first systematic report describing Xq28 genomic abnormities (Xq28 deletions affecting MECP2) in RTT.
Large intragenic MECP2 deletions have been consistently reported in the available literature [20–24]. Moreover, a RTT case was associated with a deletion detected by FISH [20]. Nevertheless, the existence of Xq28 deletions causing RTT has long remained a matter of conjecture. It seems that the high mutation detection rate and clinical heterogeneity in mutation-negative cases has resulted in the lack of studies dedicated to whole genome analysis among RTT females without detectable MECP2 mutations. On the other hand, MECP2 loss modulates RTT phenotypes in mice [25, 26] suggesting that similar genomic abnormality might cause RTT in humans. Xq28 (MECP2) deletions found in RTT girls has confirmed this expectation. Furthermore, studying functional consequences of MECP2 mutations [27–29] evidences that MECP2 loss has functional implications in females.
As detected by array CGH and FISH, one deletion causing classic RTT was mosaic. Somatic mosaicism for a structural chromosome abnormality or CNVs is common in genomic disorders or single-gene disease [30, 31]. It is also detected in cohorts of individuals with autistic spectrum disorders (in its widest sense) including girls suffering from RTT [12, 18, 32–35]. This makes it attractive to analyze molecular and clinical aspects of Xq28 (MECP2) deletions in the light of increasing interest in biomedical studies of autism, especially considering the positive experience in modelling neurodevelopmental abnormalities according to data on RTT pathogenesis [36, 37]. To explain differences between cell proportions uncovered by array CGH and FISH (Figure 3), one can compare molecular cytogenetic techniques in context of detecting somatic mosaicism [38–40]. In this instance, we have concluded that FISH results are more accurate. Similarly, FISH questioned in some detail the size of the recurrent deletion causing classic RTT. Since oligonucleotide probes cover a part of MECP2 sequence whereas the deletion was detectable by FISH with a probe for MECP2, we have speculated that genomic loss within Xq28 is a bit larger than shown by the array CGH. Likewise, sequence variations specifically generating Xq28 subchromosomal rearrangements are co-localized with the breakpoints outside of MECP2 loci [41, 42]. So far, it appears to be also valid for reported deletions. To determine the intrinsic nature and causes of Xq28 (MECP2) deletions leading to classic RTT, further studies are indisputably required.
The specific replication patterns in RTT or type C (observed in about 90% of affected children in contrast to unaffected females [12, 43]) have been detected in females with Xq28 microdeletions. The type C replication pattern represents a disturbance in the sequence of replication in an inactive chromosome X apparently caused by MECP2 mutations [12, 15]. These data allowed speculations that RTT in mutation-negative females is likely to be associated with genetic defects affecting the MECP2 gene [15]. Array CGH analysis of RTT girls, highlighting Xq28 (MECP2) deletion as a new cause of the disease, confirms this assumption.
Although RTT phenotype is characterized by recognizable patterns of malformation and distinct neurodevelopmental abnormalities, there does exist a clinical variability among females suffering from this severe disorder [3–6, 11, 14, 16, 17]. Xq28 deletions causing atypical RTT have shown to exhibit additional phenotypic features (Table 1). This can be easily explained, because all deletions have spanned significantly larger regions than the MECP2 locus, involving other Xq28 genes, as well (Figure 2). Conversely, Xq28 losses (MECP2 plus some additional genes) should naturally lead to the presence of phenotypic manifestations usually unseen in RTT. Interestingly, RTT females with large Xq28 deletions have demonstrated less severe disease manifestations as compared to their counterparts with intragenic MECP2 mutations of known functional consequences. This is likely to result from X chromosome inactivation skewing probably arisen from selective disadvantages of cells with an active deleted chromosome X. In the same way, MECP2 deletions causing classic RTT are likely to lead to less severe RTT manifestations through the skewed X chromosome inactivation patterns. Thus, epigenetic phenotype modulators determine the outcome of subchromosomal deletions involving MECP2. This has led us to the conclusion that, regardless of specific phenotypic appearance, the Xq28 deletion phenotype is not different enough from RTT due to intragenic MECP2 mutations to define it as an independent clinical entity or a microdeletion syndrome. Summarizing the clinical data on girls found to demonstrate Xq28 (MECP2) microdeletions, we have concluded that these genomic rearrangements cause at least two distinct RTT subtypes. The first subtype is caused by deletions spanning from 0.5 to 1 Mb and is characterized by less severe RTT manifestations as well as additional clinical signs. The second subtype is caused by deletions spanning about 100 kb leading to a loss of MECP2 per se and is simply a less severe classic RTT. Finally, both types can be arbitrarily designated as microdeletion RTT subtype.
To this end, it is to mention that submicroscopic genomic variations and CNVs are likely to be among the commonest causes of congenital malformations, idiopathic intellectual disability, autism, epilepsy, neuropsychiatric disorders [18, 36, 44]. Seemingly, these genome variations are likely to be important elements of pathogenetic cascades in complex disease mediating genetic-environmental interactions [45]. The present study evidences that submicroscopic deletions or CNVs cause single-gene disorders in an appreciable proportion of cases.
Conclusions
Using two array CGH platforms (BAC and oligonucleotide array CGH) and FISH, the existence of Xq28 deletions causing RTT was shown. To date, such genomic deletions were not actually recognized as a cause of RTT, a disease considered to be almost exclusively monogenic. We show that Xq28 (MECP2) deletions are common in RTT girls without detectable MECP2 sequence variations by Sanger sequencing affecting no fewer than 25% of mutation-negative females. Therefore, the efficiency of molecular diagnosis can be significantly increased through applying whole genome scan to mutation-negative RTT cases. Our data evidence that there exist at least two types of Xq28 microdeletions affecting MECP2: small deletions spanning about 100 kb and larger deletions spanning >100 kb (0.5-1 Mb). The former is likely to cause mild classic RTT, whereas the latter seems to result in mild atypical RTT forms. Finally, we conclude that Xq28 (MECP2) deletions are common in mutation-negative RTT girls and cause mild subtypes of the disease.
Methods
Patients
Thirty nine MECP2-mutation-negative females were recruited for molecular cytogenetic analysis according to molecular genetic data from the Russian RTT cohort (354 patients). All the girls fulfill clinical criteria for RTT either classic or atypical form. The information about Russian RTT cohort was provided previously [8, 12, 14, 15] and is partially given in Figure 1. The DNA samples studied were isolated from peripheral blood leukocytes following standard techniques. Written informed consent was obtained from the patients’ parents. The research was approved by the ethical committee at the Mental Health Research Center (Russian Academy of Medical Sciences) and by Russian Rett Syndrome Association.
Sequencing
The performance and results (partially) of Sanger sequencing was previously described [14, 15, 46]. The lack of a sequence variation in MECP2 known to be associated with RTT or to have a functional consequence was a criterion for entry into the study.
Array CGH
BAC-array CGH was performed using customized Constitutional Chip®4.0 (Human BAC Array-System, Perkin Elmer, USA) as described earlier [7, 47]. The resolution of the BAC-array has been estimated as 0.3 Mb for scanning chromosome X.
Oligonucleotide array CGH was performed using NimbleGen 135 K whole genome tiling array (described in parts by Duker et al. [48]). The calculated functional resolution was estimated 10–20 kb (95% confidence). Sample and reference DNA was labeled using Cy3-dUTP and Cy5-dUTP, respectively, and hybridized according to the manufacturer’s protocols (NimbleGen Arrays User’s Guide CGH and CGH/LOH Arrays v9.1, Roche NimbleGen, Madison, WI, USA). Scanning and image acquisition has been processed in the same way as for BAC-Perkin Elmer Array [7, 47].
FISH
FISH (probe labeling, hybridization and detection) was performed according to previously described protocols [12, 13, 35, 49]. The DNA probe was a YAC (yeast artificial chromosome) containing almost exactly MECP2 sequence and was kindly provided by Dr. Maurizio D’Esposito (Naples, Italy). The probe (localization and DNA sequence) was described previously [50].
Cytogenetic/cytological analysis of epigenetic phenomena
Unusual replication pattern or type C (detectable in nearly 90% of RTT children and unobserved in females without RTT [12, 43, 49]) i.e. disturbances in the replication sequence of an inactive chromosome X, was assessed by replication staining of metaphase chromosomes obtained from cultivated peripheral blood lymphocytes in the presence of 5-bromo-20-deoxyuridine as described in detail earlier [12, 43]. The presence of type C was evaluated by analyzing 50–100 metaphase plates.
Data analysis (bioinformatics)
The raw array CGH data (log 2 intensity ratios) were processed for CNV detection as proposed earlier [51, 52]. The protocol was modified to achieve comprehensive data on CNVs according to intensity ratios values for 4 oligonucleotide and 2 interchangeable BAC probes. Using different threshold schemes and background correction, the intensity ratios corresponding to CNVs spanning MECP2 were established empirically. Localization of probes in the oligonucleotide array CGH assay corresponding to MECP2 sequence was as follows: 153,299,881; 153,306,195; 153,308,602; 153,312,854. In BAC array CGH assay, there were 3 BAC probes for the X chromosome sequence encompassing the MECP2 gene. It is to note, that deletions have spanned larger regions than those covered by the probes strictly corresponding to MECP2 loci. The established threshold allowed the detection of non-mosaic and mosaic CNVs through the comparison of mean values of chromosome-specific intensity ratios and mean values of a locus of interest in Xq28.
Authors’ information
Ivan Y Iourov and Svetlana G Vorsanova are joint first authors.
Abbreviations
- CNVs:
-
Copy number variations
- CGH:
-
Comparative genomic hybridization
- FISH:
-
Fluorescence in situ hybridization
- MECP2:
-
Gene encoding methyl-CpG binding protein 2
- RTT:
-
Rett syndrome
- YAC:
-
Yeast artificial chromosome.
References
Amir RE, Van den Veyver IB, Wan M, Tran CQ, Francke U, Zoghbi HY: Rett syndrome is caused by mutations in X-linked MECP2, encoding methyl-CpG-binding protein 2. Nat Genet 1999, 23: 185–188. 10.1038/13810
Dragich J, Houwink-Manville I, Schanen C: Rett syndrome: a surprising result of mutation in MECP2. Hum Mol Genet 2000, 9: 2365–2375. 10.1093/hmg/9.16.2365
Vorsanova SG, Iourov IY, Yurov YB: Neurological, genetic and epigenetic features of Rett syndrome. J Pediatr Neurol 2004, 2: 179–190.
Weaving LS, Ellaway CJ, Gécz J, Christodoulou J: Rett syndrome: clinical review and genetic update. J Med Genet 2005, 42: 1–7. 10.1136/jmg.2004.027730
Chahrour M, Zoghbi HY: The story of Rett syndrome: from clinic to neurobiology. Neuron 2007, 56: 422–437. 10.1016/j.neuron.2007.10.001
Matsuishi T, Yamashita Y, Takahashi T, Nagamitsu S: Rett syndrome: the state of clinical and basic research, and future perspectives. Brain Dev 2011, 33: 627–631. 10.1016/j.braindev.2010.12.007
Iourov IY, Vorsanova SG, Kurinnaia OS, Zelenova MA, Silvanovich AP, Yurov YB: Molecular karyotyping by array CGH in a Russian cohort of children with intellectual disability, autism, epilepsy and congenital anomalies. Mol Cytogenet 2012, 5: 46. 10.1186/1755-8166-5-46
Vorsanova SG, Iurov II, Voinova VI, Kurinnaia OS, Zelenova MA, Demidova IA, Ulas EV, Voinova VI, Iurov IB: Subchromosomal microdeletion identified by molecular karyotyping using DNA microarrays (array CGH) in Rett syndrome girls negative for MECP2 gene mutations. Zh Nevrol Psikhiatr Im S S Korsakova 2013, 113(10):47–52.
Artuso R, Papa FT, Grillo E, Mucciolo M, Yasui DH, Dunaway KW, Disciglio V, Mencarelli MA, Pollazzon M, Zappella M, Hayek G, Mari F, Renieri A, Lasalle JM, Ariani F: Investigation of modifier genes within copy number variations in Rett syndrome. J Hum Genet 2011, 56: 508–515. 10.1038/jhg.2011.50
Grillo E, Lo Rizzo C, Bianciardi L, Bizzarri V, Baldassarri M, Spiga O, Furini S, De Felice C, Signorini C, Leoncini S, Pecorelli A, Ciccoli L, Mencarelli MA, Hayek J, Meloni I, Ariani F, Mari F, Renieri A: Revealing the complexity of a monogenic disease: Rett syndrome exome sequencing. PLoS One 2013., 8: e56599
Neul JL, Kaufmann WE, Glaze DG, Christodoulou J, Clarke AJ, Bahi-Buisson N, Leonard H, Bailey ME, Schanen NC, Zappella M, Renieri A, Huppke P, Percy AK: RettSearch Consortium: Rett syndrome: revised diagnostic criteria and nomenclature. Ann Neurol 2010, 68: 944–950. 10.1002/ana.22124
Vorsanova SG, Yurov YB, Ulas VY, Demidova IA, Sharonin VO, Kolotii AD, Gorbatchevskaia NL, Beresheva AK, Soloviev IV: Cytogenetic and molecular-cytogenetic studies of Rett syndrome (RTT): a retrospective analysis of a Russian cohort of RTT patients (the investigation of 57 girls and three boys). Brain Dev 2001, 23(Suppl 1):S196-S201.
Yurov YB, Vorsanova SG, Kolotii AD, Iourov IY: Molecular-cytogenetic investigation of skewed chromosome X inactivation in Rett syndrome. Brain Dev 2001, 23(Suppl 1):S214-S217.
Vorsanova SG, Ulas VI, Iurov IB, Giovanucci-Uzielli ML, Demidova IA, Gianti L, Villard L, Iurov II, Beresheva AK, Novikov PV: Genotype-phenotype correlations in Rett syndrome: the study of Russian cohort of patients. Zh Nevrol Psikhiatr Im S S Korsakova 2002, 102(10):23–29.
Iurov II, Vorsanova SG, Voinova-Ulas VI, Villard L, Demidova IA, Giunti L, Guivabyccu-Uzielli ML, Budilov AV, Beresheva AK, Novikov PV, Iurov IB: Epigenetic study of Rett’s syndrome as an adequate model for autistic disorders. Zh Nevrol Psikhiatr Im S S Korsakova 2005, 105(7):4–11.
Trevathan E, Moser H, Rett Syndrome Diagnostic Criteria Work Group: Diagnostic criteria for Rett syndrome. The rett syndrome diagnostic criteria work group. Ann Neurol 1988, 23: 425–428.
Temudo T, Santos M, Ramos E, Dias K, Vieira JP, Moreira A, Calado E, Carrilho I, Oliveira G, Levy A, Barbot C, Fonseca M, Cabral A, Cabral P, Monteiro J, Borges L, Gomes R, Mira G, Pereira SA, Santos M, Fernandes A, Epplen JT, Sequeiros J, Maciel P: Rett syndrome with and without detected MECP2 mutations: an attempt to redefine phenotypes. Brain Dev 2011, 33: 69–76. 10.1016/j.braindev.2010.01.004
Iourov IY, Vorsanova SG, Yurov YB: Molecular cytogenetics and cytogenomics of brain diseases. Curr Genomics 2008, 9: 452–465. 10.2174/138920208786241216
Mencarelli MA, Kleefstra T, Katzaki E, Papa FT, Cohen M, Pfundt R, Ariani F, Meloni I, Mari F, Renieri A: 14q12 Microdeletion syndrome and congenital variant of Rett syndrome. Eur J Med Genet 2009, 52: 148–152. 10.1016/j.ejmg.2009.03.004
Bourdon V, Philippe C, Labrune O, Amsallem D, Arnould C, Jonveaux P: A detailed analysis of the MECP2 gene: prevalence of recurrent mutations and gross DNA rearrangements in Rett syndrome patients. Hum Genet 2001, 108: 43–50. 10.1007/s004390000422
Ravn K, Nielsen JB, Skjeldal OH, Kerr A, Hulten M, Schwartz M: Large genomic rearrangements in MECP2. Hum Mutat 2005, 25: 324.
Archer HL, Whatley SD, Evans JC, Ravine D, Huppke P, Kerr A, Bunyan D, Kerr B, Sweeney E, Davies SJ, Reardon W, Horn J, MacDermot KD, Smith RA, Magee A, Donaldson A, Crow Y, Hermon G, Miedzybrodzka Z, Cooper DN, Lazarou L, Butler R, Sampson J, Pilz DT, Laccone F, Clarke AJ: Gross rearrangements of the MECP2 gene are found in both classical and atypical Rett syndrome patients. J Med Genet 2006, 43: 451–456.
Bebbington A, Downs J, Percy A, Pineda M, Zeev BB, Bahi-Buisson N, Leonard H: The phenotype associated with a large deletion on MECP2. Eur J Hum Genet 2012, 20: 921–927. 10.1038/ejhg.2012.34
Kobayashi Y, Ohashi T, Akasaka N, Tohyama J: Congenital variant of Rett syndrome due to an intragenic large deletion in MECP2. Brain Dev 2012, 34: 601–604. 10.1016/j.braindev.2011.09.014
Chen RZ, Akbarian S, Tudor M, Jaenisch R: Deficiency of methyl-CpG binding protein-2 in CNS neurons results in a Rett-like phenotype in mice. Nat Genet 2001, 27: 327–331. 10.1038/85906
Guy J, Hendrich B, Holmes M, Martin JE, Bird A: A mouse Mecp2-null mutation causes neurological symptoms that mimic Rett syndrome. Nat Genet 2001, 27: 322–326. 10.1038/85899
Agarwal N, Becker A, Jost KL, Haase S, Thakur BK, Brero A, Hardt T, Kudo S, Leonhardt H, Cardoso MC: MeCP2 Rett mutations affect large scale chromatin organization. Hum Mol Genet 2011, 20: 4187–4195. 10.1093/hmg/ddr346
Singleton MK, Gonzales ML, Leung KN, Yasui DH, Schroeder DI, Dunaway K, LaSalle JM: MeCP2 is required for global heterochromatic and nucleolar changes during activity-dependent neuronal maturation. Neurobiol Dis 2011, 43: 190–200. 10.1016/j.nbd.2011.03.011
Guy J, Cheval H, Selfridge J, Bird A: The role of MeCP2 in the brain. Annu Rev Cell Dev Biol 2011, 27: 631–652. 10.1146/annurev-cellbio-092910-154121
Iourov IY, Vorsanova SG, Yurov YB: Chromosomal mosaicism goes global. Mol Cytogenet 2008, 1: 26. 10.1186/1755-8166-1-26
Iourov IY, Vorsanova SG, Yurov YB: Somatic genome variations in health and disease. Curr Genomics 2010, 11: 387–396. 10.2174/138920210793176065
Iourov IY, Vorsanova SG, Yurov YB: Chromosomal variation in mammalian neuronal cells: known facts and attractive hypotheses. Int Rev Cytol 2006, 249: 143–191.
Vorsanova SG, Yurov IY, Demidova IA, Voinova-Ulas VY, Kravets VS, Solov’ev IV, Gorbachevskaya NL, Yurov YB: Variability in the heterochromatin regions of the chromosomes and chromosomal anomalies in children with autism: identification of genetic markers of autistic spectrum disorders. Neurosci Behav Physiol 2007, 37: 553–558. 10.1007/s11055-007-0052-1
Vorsanova SG, Voinova VY, Yurov IY, Kurinnaya OS, Demidova IA, Yurov YB: Cytogenetic, molecular-cytogenetic, and clinical-genealogical studies of the mothers of children with autism: a search for familial genetic markers for autistic disorders. Neurosci Behav Physiol 2010, 40: 745–756. 10.1007/s11055-010-9321-5
Yurov YB, Vorsanova SG, Iourov IY, Demidova IA, Beresheva AK, Kravetz VS, Monakhov VV, Kolotii AD, Voinova-Ulas VY, Gorbachevskaya NL: Unexplained autism is frequently associated with low-level mosaic aneuploidy. J Med Genet 2007, 44: 521–525. 10.1136/jmg.2007.049312
Abrahams BS, Geschwind DH: Advances in autism genetics: on the threshold of a new neurobiology. Nat Rev Genet 2008, 9: 341–355. 10.1038/nrg2346
Neul JL: The relationship of Rett syndrome and MECP2 disorders to autism. Dialogues Clin Neurosci 2012, 14: 253–262.
Shaffer LG, Bejjani BA, Torchia B, Kirkpatrick S, Coppinger J, Ballif BC: The identification of microdeletion syndromes and other chromosome abnormalities:cytogenetic methods of the past, new technologies for the future. Am J Med Genet C Semin Med Genet 2007, 145C: 335–345. 10.1002/ajmg.c.30152
Vorsanova SG, Yurov YB, Iourov IY: Human interphase chromosomes: a review of available molecular cytogenetic technologies. Mol Cytogenet 2010, 3: 1. 10.1186/1755-8166-3-1
Iourov IY, Vorsanova SG, Yurov YB: Single cell genomics of the brain: focus on neuronal diversity and neuropsychiatric diseases. Curr Genomics 2012, 13: 477–488. 10.2174/138920212802510439
Bauters M, Van Esch H, Friez MJ, Boespflug-Tanguy O, Zenker M, Vianna-Morgante AM, Rosenberg C, Ignatius J, Raynaud M, Hollanders K, Govaerts K, Vandenreijt K, Niel F, Blanc P, Stevenson RE, Fryns JP, Marynen P, Schwartz CE, Froyen G: Nonrecurrent MECP2 duplications mediated by genomic architecture-driven DNA breaks and break-induced replication repair. Genome Res 2008, 18: 847–858. 10.1101/gr.075903.107
El-Hattab AW, Fang P, Jin W, Hughes JR, Gibson JB, Patel GS, Grange DK, Manwaring LP, Patel A, Stankiewicz P, Cheung SW: Int22h-1/int22h-2-mediated Xq28 rearrangements: intellectual disability associated with duplications and in utero male lethality with deletions. J Med Genet 2011, 48: 840–850. 10.1136/jmedgenet-2011-100125
Vorsanova SG, Demidova IA, Ulas VY, Soloviev IV, Kazantzeva LZ, Yurov YB: Cytogenetic and molecular-cytogenetic investigation of Rett syndrome: analysis of 31 cases. Neuroreport 1996, 8: 187–189. 10.1097/00001756-199612200-00038
Hochstenbach R, Buizer-Voskamp JE, Vorstman JA, Ophoff RA: Genome arrays for the detection of copy number variations in idiopathic mental retardation, idiopathic generalized epilepsy and neuropsychiatric disorders: lessons for diagnostic workflow and research. Cytogenet Genome Res 2011, 135: 174–202. 10.1159/000332928
Iourov IY, Vorsanova SG, Yurov YB: Somatic cell genomics of brain disorders: a new opportunity to clarify genetic-environmental interactions. Cytogenet Genome Res 2013, 139: 181–188. 10.1159/000347053
Giunti L, Pelagatti S, Lazzerini V, Guarducci S, Lapi E, Coviello S, Cecconi A, Ombroni L, Andreucci E, Sani I, Brusaferri A, Lasagni A, Ricotti G, Giometto B, Nicolao P, Gasparini P, Granatiero M, Uzielli ML: Spectrum and distribution of MECP2 mutations in 64 Italian Rett syndrome girls: tentative genotype/phenotype correlation. Brain Dev 2001, 23(Suppl 1):S242-S245.
Vorsanova SG, Iurov II, Kurinnaia OS, Voinova VI, Iurov IB: Genomic abnormalities in children with mental retardation and autism: the use of comparative genomic hybridization in situ (HRCGH) and molecular karyotyping with DNA-microchips (array CGH). Zh Nevrol Psikhiatr Im S S Korsakova 2013, 113(8):46–49.
Duker AL, Ballif BC, Bawle EV, Person RE, Mahadevan S, Alliman S, Thompson R, Traylor R, Bejjani BA, Shaffer LG, Rosenfeld JA, Lamb AN, Sahoo T: Paternally inherited microdeletion at 15q11.2 confirms a significant role for the SNORD116 C/D box snoRNA cluster in Prader-Willi syndrome. Eur J Hum Genet 2010, 18: 1196–1201. 10.1038/ejhg.2010.102
Vorsanova SG, Yurov YB, Kolotii AD, Soloviev IV: FISH analysis of replication and transcription of chromosome X loci: new approach for genetic analysis of Rett syndrome. Brain Dev 2001, 23(Suppl 1):S191-S195.
D’Esposito M, Quaderi NA, Ciccodicola A, Bruni P, Esposito T, D’Urso M, Brown SD: Isolation, physical mapping, and northern analysis of the X-linked human gene encoding methyl CpG-binding protein, MECP2. Mamm Genome 1996, 7: 533–535. 10.1007/s003359900157
Griswold AJ, Ma D, Cukier HN, Nations LD, Schmidt MA, Chung RH, Jaworski JM, Salyakina D, Konidari I, Whitehead PL, Wright HH, Abramson RK, Williams SM, Menon R, Martin ER, Haines JL, Gilbert JR, Cuccaro ML, Pericak-Vance MA: Evaluation of copy number variations reveals novel candidate genes in autism spectrum disorder-associated pathways. Hum Mol Genet 2012, 21: 3513–3523. 10.1093/hmg/dds164
Rio M, Royer G, Gobin S, de Blois MC, Ozilou C, Bernheim A, Nizon M, Munnich A, Bonnefont JP, Romana S, Vekemans M, Turleau C, Malan V: Monozygotic twins discordant for submicroscopic chromosomal anomalies in 2p25.3 region detected by array CGH. Clin Genet 2013, 84: 31–36. 10.1111/cge.12036
Acknowledgments
We would like to express our deepest gratitude to Olga V. Timutsa from the Russian Rett Syndrome Association for continuous support and kind assistance. We also thank children who took part in our study and their parents. Dr. M. D’Esposito (Naples, Italy) is acknowledged for providing MECP2- specific FISH probe. The study was supported by the Russian Rett Syndrome Association and by the Grant of the President of the Russian Federation MD-4401.2013.7.
Presented in part at the European Human Genetics Conference 2012, Nürnberg, Germany, June 23–26, 2012.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
IYY, SGV and YBY conceived the research, designed the study, and wrote the manuscript; IYY, SGV, VYV and YBY conceived the project and obtained the funding; VYV and SGV referred the patients for the study; IYI, OSK, MAZ and IAD performed the experiments and participated in the diagnostic service. All authors have read and approved the final manuscript.
Electronic supplementary material
13039_2013_199_MOESM1_ESM.tiff
Additional file 1: Figure S1: The deleted Xq28 region spanning 502.428 kb displayed using UCSC Genome Browser on Human Feb. 2009 (GRCh37/hg19) Assembly (http://genome-euro.ucsc.edu/index.html). (TIFF 3 MB)
13039_2013_199_MOESM2_ESM.tiff
Additional file 2: Figure S2: The deleted Xq28 region spanning 539.545 kb displayed using UCSC Genome Browser on Human Feb. 2009 (GRCh37/hg19) Assembly (http://genome-euro.ucsc.edu/index.html). (TIFF 3 MB)
13039_2013_199_MOESM3_ESM.tiff
Additional file 3: Figure S3: The deleted Xq28 region spanning 877.444 kb displayed using UCSC Genome Browser on Human Feb. 2009 (GRCh37/hg19) Assembly (http://genome-euro.ucsc.edu/index.html). (TIFF 3 MB)
13039_2013_199_MOESM4_ESM.tiff
Additional file 4: Figure S4: The deleted Xq28 region spanning 99.371 kb displayed using UCSC Genome Browser on Human Feb. 2009 (GRCh37/hg19) Assembly (http://genome-euro.ucsc.edu/index.html). (TIFF 1 MB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Iourov, I.Y., Vorsanova, S.G., Voinova, V.Y. et al. Xq28 (MECP2) microdeletions are common in mutation-negative females with Rett syndrome and cause mild subtypes of the disease. Mol Cytogenet 6, 53 (2013). https://doi.org/10.1186/1755-8166-6-53
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1755-8166-6-53