
Abstract
Background
Though the nephrotoxicity and carcinogenicity of aristolochic acid (AA) are known, its safety in clinical usage is not clear. This study aims to evaluate the safety of Duhuo Jisheng Tang (DJT) in a four-week study to treat osteoarthritis (OA) of the knee.
Methods
A qualitative and quantitative investigations on DJT were conducted. A list of adverse events (AEs), complete blood counts, and liver and kidney function tests were measured for participants with knee OA at their scheduled hospital visits. Each detected AEs was independently assessed for severity and causality by site investigators (Chinese medical doctors) and study nurses.
Results
A total of 71 eligible subjects were included in the clinical study where 287 AEs were reported. DJT did not contain detectable aristolochic acid (AA) under thin-layer chromatography (TLC) analysis and gas chromatography coupled with mass spectrometry (GC-MS). There were no significant changes in liver or kidney functions.
Conclusion
In four-week use of DJT, no renal tubular damage, no severe incidences of AEs and adverse drug reactions (ADRs) were observed. The present study obtained safety data from active surveillance of DJT.
Similar content being viewed by others

Background
While medicinal herbal products are widely used [1, 2] with a presumption that natural herbs are safe, there is a lack of safety evidence to support such products. Since the discovery of nephrotoxicity and carcinogenicity of aristolochic acid (AA) [3–5], the International Agency for Research into Cancer (IARC) has considered herbal remedies containing plants of aristolochia genus as Group 1 human carcinogens and those containing naturally occurring mixtures of AAs as 2A carcinogens [6]. Medicinal plants that contain AAs are banned in certain countries, including USA, UK, Canada, and Taiwan [7, 8].
Xixin (Radix et Rhizoma Asari), also known as Saishin in Japan or Sesin in Korea, is widely used in many parts of Asia despite that it contains AAs [9–11]. For example, since 2004, a total of 393 Chinese herbal products (CHPs) containing Xixin have been reimbursed under the National Health Insurance (NHI) in Taiwan [12] where the regulations stipulate that AA must be undetectable in final herbal products [13]. Our preliminary analysis of NHI data found that about 1.57 million in Taiwan have been prescribed with CHPs containing Xixin. Duhuo Jisheng Tang (DJT), an herbal formula described by the ancient Chinese physician Sun Simiao in 652 AD to treat low back/knee pain [14–16], was prescribed to 725,549 patients between 1996 and 2004. DJT was attributed to AA-related nephropathy in a case report [17].
In another aspect, many clinical trials of Chinese herbal medicines (CHMs) have been rated as having poor methodological quality [18], though CHMs is regarded by the World Health Organization (WHO) as in the urgent need to establish evidence-based information [19]. The active monitoring of safety profile demonstrated in our previous study is proved useful to supplement the current pharmacovigilance function [20]. Therefore, the present study aims to determine whether AA is present in Xixin-containing CHPs such as DJT and whether DJT use causes acute nephrotoxicity by qualitative and quantitative methods incorporated in active safety surveillance system. The results of efficacy evaluation were reported in a separate paper [21].
Methods
DJT preparation
The investigational DJT was supplied by Sun Ten Pharmaceutical Company (Taiwan) in a standardized form of 15 concentrated herbal extracts, namely Duhuo (Radix Angelicae Pubescentis), Qinjiao (Radix Gentianae Macrophyllae), Fangfeng (Radix Saposhnikoviae), Xixin, Rougui (Cortex Cinnamomi), Sangjisheng (Herba Taxilli), Duzhong (Cortex Eucommiae), Shudihuang (Radix Rehmanniae), Niuxi (Radix Cyathulae), Danggui (Radix Angelicae Sinensis), Baishao (Radix Paeoniae Alba), Chuanxiong (Rhizoma Chuanxiong), Renshen (Radix et Rhizoma Ginseng), Fuling (Poria) and Gancao (Radix et Rhizoma Glycyrrhizae). The final product is 2.5 g of granules packed in a sachet.
The investigational DJT, three other brands of each of DJT and Xixin were produced by pharmaceutical companies with good manufacturing practice (GMP) certification. All samples were sent to the Bureau of Food and Drug Analysis of Taiwan for chemical analysis. Thin-layer chromatography (TLC) and gas chromatography coupled with mass spectrometry (GC-MS) were used to confirm Xixin in these samples by identifying their characteristic peaks of Asarinin. High-performance liquid chromatography (HPLC) and liquid chromatography coupled with tandem mass spectrometer (LC/MS/MS) were then carried out to detect AA in these samples [22].
A clinical study with active safety surveillance [20] on detection and causality assessment of adverse events (AEs) was launched at the Yangming and Chinese Medicine Branches of Taipei City Hospital. This study was approved by the Joint Institutional Review Board for Traditional Chinese Medicine, and received regular external monitoring and auditing by a third Research Organization during the study period.
Inclusion and exclusion criteria for study subjects
Adult patients with osteoarthritis in at least one knee in the previous six months were recruited for the study. Exclusion criteria are as follows: (1) intra-articular injections of non-steroidal anti-inflammatory drugs within one month; (2) secondary arthritis related to syphilitic neuropathy, ochronosis, metabolic bone disease or acute trauma, severe osteoporosis (≥ grade 3) [23] or acute rheumatic arthritis; (3) significant co-morbidities, such as hypertension, severe hepatitis, kidney diseases or malignant carcinoma; (4) spinopathy caused by tumor (benign or malignant); (5) the use of any other investigational drugs within the past 30 days; (6) women with childbearing potential who had not used adequate contraception since their last menstruation or would not continuously use adequate contraception during the study period; and (7) women who were lactating or positive in a urine pregnancy test within 14 days prior to the study. Quota for recruiting participants from Yangming and Chinese Medicine Branches of Taipei City Hospital was 40. All recruited subjects were required to sign an informed consent form and to discontinue any form of treatment and current medications, including western medicine and CHPs, at least two weeks prior to the screening for the study.
Active surveillance for safety
A surveillance list of 20 pre-hypothesized AEs was compiled with spaces allowed for AEs not in the list. The AE-specific form with the description of the signs and symptoms was used to ask subjects questions for causality information [24], including necessary criteria (temporality), quasi-necessary criteria (consistency, chance elimination and confounders as alternative explanations and coherence with other highly corroborated theories) and other supportive criteria (e.g. strength and specificity of association, dose response relationship and biological plausibility). The information on every reported AE was collected in respective structured forms for causality assessment. Through a prospective design, we collected the quantitative and qualitative data related to each AE and looked for possible explanation during each incidence. Moreover, we adopted a consensual approach to minimize disagreements and reach a more credible conclusion in causality assessment for AE-drug combinations [25, 26].
The recruited subjects were required to take two sachets (5 g) of the investigational DJT per day for four weeks, an adequate treatment course estimated by the clinicians for the measurement of DJT efficacy and for the detection of early tubular damage to the kidney. Laboratory tests were conducted at baseline visit and four weeks after taking DJT, including routine urinalysis, complete blood and platelet counts, biochemistry measures and urinary N-acetyl-glucosaminidase (NAG) and retinal binding protein (RBP) [27, 28].
Every detected/reported AE was independently assessed by onsite investigators (Chinese medical doctors) and study nurses. The investigators applied unstructured clinical judgment [29] to rate the AEs severity as mild (transient or mild discomfort; no medical intervention required), moderate (some assistance needed; no medical intervention required) or severe (marked limitation in activity; medical intervention required and possible hospitalization); and rate the AE-drug causality as uncertain, probable/likely, possible, unlikely, conditional/unclassified and unassessable/unclassifiable [30]. The study nurses adopted the Common Terminology Criteria for Adverse Events (CTCAE) v3.0 [31] to judge the severity of the AEs and Naranjo scale [32] to assess causality. Any severe AEs, or any AEs judged to be highly correlated to DJT was be submitted to the research panel for final decision.
Data analysis
The data were analyzed using simple statistics. The outcome variables were the incidence rates of AEs and adverse drug reactions (ADRs), which were calculated by dividing the event counts of the AEs and ADRs (the numerator) by the exposure level, in terms of person-days or person-sachets (the denominator). The former was the total number of all the participants' exposed (intend-to-treat) person-days to the study drug, while the latter was the actual number of sachets which participants had taken during the study period.
Results
Laboratory tests
TLC results revealed that seven samples contained Xixin. GC-MS results also confirmed Asarinin, the main component of Xixin. LC/MS/MS or HPLC detected AAI and AAII only in the three brands of Xixin samples when those were condensed 25 times (Table 1).
Subjects
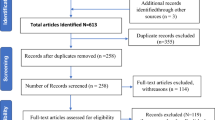
A total of 87 subjects who signed the informed consent form were screened. Sixteen subjects did not receive medication due to various reasons (Figure 1). Intent-to-treat monitoring was given to all the rest of 71 subjects.

Recruitment of participants' inclusion, withdrawal, and completion during follow-up.
Occurrences of adverse events
None of the subjects showed any abnormality of urinalysis, creatinine or blood urea nitrogen, NAG or RBP. A total of 287 AEs were detected/reported during the study period (Additional file 1) and were coded according to the Coding Symbols for Thesaurus of Adverse Reaction Terms (COSTART) [33]. The most often reported AEs were rashes, abdominal fullness, coughs, somnolence, muscle cramps and diarrhea with the incidence rates of 14.5, 12.9, 12.4, 11.9, 10.3, and 10.3 per 1000 person-days respectively; and 7.5, 6.9, 6.6, 6.3, 5.5, 5.5 per 1000 person-sachets respectively. All of these AEs were monitored according to the original surveillance list. No additional AE was found.
Severity of the adverse events and association with DJT
All recorded AEs were classified as 'mild' to 'moderate' according to the investigators (Chinese medical doctors), and as 'Grade 1' or 'Grade 2' according to the study nurses. These AEs were tolerable and did not have any significant effects on the subjects' daily activities. The probable ADRs separately detected by the investigators (Chinese medical doctors) and study nurses are summarized in Table 2.
Discussion
In the present study, AA was undetectable in the investigational DJT and three other brands of DJT, whereas the main peaks of the active ingredients (e.g. Asarinin) of Xixin were present in the samples. This result supports the regulations set by the Committee on Chinese Medicine and Pharmacy of Taiwan, which stipulates that only the root portion of Xixin can be used for herbal products, and therefore the final product should not contain any detectable AA [13]. However, care must be taken to prevent people from using raw herbs of Xixin which may contain higher levels of AA.
The possible existence of AA in DJT may pose a potential hazard to patients' health [34–37]. We attempted to indirectly estimate the average levels of AA in DJT from concentrated Xixin. As shown in Table 1, AAI was detected only in concentrated (25 times) Xixin products. Those subjects who completed the study would have ingested a maximum daily dosage of 0.04-0.08 μg of AAI, which was a total of 1.34-2.01 μg for the study period. None of these subjects showed any significant renal tubular damage.
A four-week study of Duhua Jisheng Wan[38], which has the same ingredients of DJT, also did not result in any kidney-related damage. As compared to the reported case of the AA-related nephropathy patient [17] ingesting 400 g of DJT powder for over four months, the ingestion levels of AA in this study were very low. However, the holistic effect stressed by CHMs theory [16] in mixing different herbs as a meaning of enhancing efficacy and minimizing toxicity cannot be completely ruled out. To evaluate the overall safety of the final DJT product as a formulated herbal preparation of 15 herbs, we list AEs for DJT in additional file 1.
The absence of a control group makes the observed results from the present study subject to potential confounders. To minimize confounders, we implemented two independent assessments by site investigators (Chinese medical doctors) and study nurses, respectively. In addition, the sample size of the present study is small.
Conclusion
In four-week use of DJT, no renal tubular damage, no severe incidence of AEs and ADRs were observed. The present study obtained safety data from active surveillance of DJT.
Abbreviations
- DJT:
-
Duhuo Jisheng Tang
- AA:
-
aristolochic acid
- OA:
-
osteoarthritis
- GCP:
-
good clinical practice
- AEs:
-
adverse events
- ADR:
-
adverse drug reactions
- TLC:
-
thin-layer chromatography analysis
- GC-MS:
-
gas chromatography coupled with mass spectrometry
- CHPs:
-
Chinese herbal products
- NHI:
-
National Health Insurance
- CHMs:
-
Chinese herbal medicines
- IARC:
-
International Agency for Research into Cancer
- GMP:
-
good manufacturing practice
- HPLC:
-
high-performance liquid chromatography
- LC/MS/MS:
-
liquid chromatography coupled with tandem mass spectrometer
- NAG:
-
N-acetyl-glucosaminidase
- RBP:
-
retinal binding protein
- CTCAE:
-
Common Terminology Criteria for Adverse Events
- WHO:
-
World Health Organization.
References
Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC: Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA. 1998, 280: 1569-1575. 10.1001/jama.280.18.1569.
Kessler RC, Davis RB, Foster DF, Van Rompay MI, Walters EE, Wilkey SA, Kaptchuk TJ, Eisenberg DM: Long-term trends in the use of complementary and alternative medical therapies in the United States. Ann Intern Med. 2001, 135: 262-268.
Cosyns JP: Aristolochic acid and 'Chinese herbs nephropathy': a review of the evidence to date. Drug Saf. 2003, 26 (1): 33-48. 10.2165/00002018-200326010-00004.
Arlt VM, Stiborova M, Schmeiser HH: Aristolochic acid as a probable human cancer hazard in herbal remedies: a review. Mutagenesis. 2002, 17 (4): 265-277. 10.1093/mutage/17.4.265.
Nortier JL, Martinez MC, Schmeiser HH, Arlt VM, Bieler CA, Petein M, Depierreux MF, De Pauw L, Abramowicz D, Vereerstraeten P, Vanherweghem JL: Urothelial carcinoma associated with the use of a Chinese herb (aristolochia fangchi). N Engl J Med. 2000, 342 (23): 1686-1692. 10.1056/NEJM200006083422301.
International Agency for Research on Cancer. Complete list of agents evaluated and their classification. [http://monographs.iarc.fr/ENG/Classification/index.php]
Kessler DA: Cancer and herbs. N Engl J Med. 2000, 342 (23): 1742-1743. 10.1056/NEJM200006083422309.
U.S. Food & Drug Administration. Dietary Supplements: Aristolochic Acid. [http://www.fda.gov/Food/DietarySupplements/Alerts/ucm095272.htm]
Drew AK, Whyte IM, Bensoussan A, Dawson AH, Zhu X, Myers SP: Chinese herbal medicine toxicology database: monograph on herba asari, "xi xin". l Clin Toxicol. 2002, 40 (2): 169-172. 10.1081/CLT-120004405.
Jong TT, Lee MR, Hsiao SS, Hsai JL, Wu TS, Chiang ST, Cai SQ: Analysis of aristolochic acid in nine sources of xixin, a traditional Chinese medicine, by liquid chromatography/atmospheric pressure chemical ionization/tandem mass spectrometry. J Pharm Biomed Anal. 2003, 33 (4): 831-837. 10.1016/S0731-7085(03)00310-8.
Hashimoto K, Higuchi M, Makino B, Sakakibara I, Kubo M, Komatsu Y, Maruno M, Okada M: Quantitative analysis of aristolochic acids, toxic compounds, contained in some medicinal plants. J Ethnopharmacol. 1999, 64 (2): 185-189. 10.1016/S0378-8741(98)00123-8.
Committee on Chinese Medicine and Pharmacy, Department of Health, Executive Yuan Taiwan. Reference list of registered Chinese herbal medicines. [http://www.ccmp.gov.tw/public/public.asp?selno=492&relno=492&level=C]
Committee on Chinese Medicine and Pharmacy, Department of Health, ExecutiveYuan Taiwan. Drug Registration-related Regulations-Xixin herbs and products. [http://www.ccmp.gov.tw/public/public.asp?selno=601&relno=601&level=C]
Committee on Chinese Medicine and Pharmacy, Department of Health, Executive Yuan Taiwan. Chinese Pharmacopoeia of Chinese Medicine. [http://www.ccmp.gov.tw/public/public.asp?selno=525&relno=525&level=C]
Dharmananda, S. An Analysis of Chinese herb prescriptions for rheumatoid articles. [http://www.itmonline.org/arts/arthritis.htm]
Molony D: The American Association of Oriental Medicine's Complete Guide to Chinese Herbal Medicine. 1998, New York: Berkley Books
Yang HY, Lin JL, Chen KH, Yu CC, Hsu PY, Lin CL: Aristolochic acid-related nephropathy associated with the popular Chinese herb Xi Xin. J Nephrol. 2006, 19 (1): 111-114.
Tang JL, Zhan SY, Ernst E: Review of randomized controlled trials of traditional Chinese medicine. BMJ. 1999, 319: 160-161.
World Health Organization. WHO medicine strategy: countries at the core. 2004http://whqlibdoc.who.int/hq/2004/WHO_EDM_2004.5.pdf2007
Hsieh SC, Lai JN, Chen PC, Chen HJ, Wang JD: Development of active safety surveillance system for traditional Chinese medicine: an empirical study in treating climacteric women. Pharmacoepidemiol Drug Saf. 2006, 15 (12): 889-899. 10.1002/pds.1340.
Lai JN, Chen HJ, Chen CC, Lin JH, Hwang JS, Wang JD: Duhuo Jisheng Tang for treating osteoarthritis of the knee: a prospective clinical observation. Chin Med. 2007, 2: 4-10.1186/1749-8546-2-4.
The Japanese Pharmacopoeia, JP XIV. General Information: Aristolochic Acid. [http://jpdb.nihs.go.jp/jp14e/contents.html]
Kellgren JH, Lawrence JS: Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957, 16 (4): 494-502. 10.1136/ard.16.4.494.
Wang JD: Causal inference and decision. Basic Principles and Practical Applications in Epidemiological Research. 2002, Singapore: World Scientific, 57-79.
Miremont G, Haramburu F, Bégaud B, Péré JC, Dangoumau J: Adverse drug reactions: physicians' opinions versus a causality assessment method. Eur J Clin Pharmacol. 1994, 46 (4): 285-289. 10.1007/BF00194392.
Arimone Y, Bégaud B, Miremont-Salamé G, Fourrier-Réglat A, Moore N, Molimard M, Haramburu F: Agreement of expert judgment in causality assessment of adverse drug reactions. Eur J Clin Pharmacol. 2005, 61 (3): 169-173. 10.1007/s00228-004-0869-2.
D'Amico G, Bazzi C: Urinary protein and enzyme excretion as markers of tubular damage. Curr Opin Nephrol Hypertens. 2003, 12 (6): 639-643. 10.1097/00041552-200311000-00011.
Flynn FV: Assessment of renal function: selected developments. Clin Biochem. 1990, 23 (1): 49-54. 10.1016/0009-9120(90)90435-W.
Jones JK: Determining causation from case reports. Pharmacoepidemiology. Edited by: Strom BL. 2000, New York: John Wiley & Sons, 531-538. 3
Uppsala Monitoring Center. Safety monitoring of medicinal products: guidelines for setting up and running a pharmacovigilance Center. 2002.http://www.who-umc.org/graphics/4807.pdf
National Cancer Institute. Common Terminology Criteria for Adverse Events v3.0. [http://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/ctcaev3.pdf
Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, Janecek E, Domecq C, Greenblatt DJ: A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981, 30: 239-245.
United States Food and Drug Administration: COSTART: Coding Symbols for Thesaurus of Adverse Reaction Terms. 1995, Rockville, MD: Public Health Service, Food and Drug Administration
Lai MN, Lai JN, Chen PC, Tseng WL, Chen YY, Hwang JS, Wang JD: Increased risks of chronic kidney disease associated with prescribed Chinese herbal products suspected to contain aristolochic acid. Nephrology. 2009, 14: 227-234. 10.1111/j.1440-1797.2008.01061.x.
Yang HY, Wang JD, Lo TC, Chen PC: Increased mortality risk of kidney and other urinary organs cancers in Chinese herbalists. J Epidemiol. 2009, 19 (1): 17-23. 10.2188/jea.JE20080035.
Lai MN, Wang SM, Chen PC, Chen YY, Wang JD: Population-based case-control study of Chinese herbal products containing aristolochic acid and urinary tract cancer risk. J Natl Cancer Inst. 2010, 10.1093/jnci/djp467.
Lai MN, Lai JN, Chen PC, Hsieh SC, Hu FC, Wang JD: Risk of kidney failure associated with consumption of herbal products containing Mu Tong or Fangchi : A population-based case-control study. AJKD.
Teekachunhatean S, Kunanusorn P, Rojanasthien N, Sananpanich K, Pojchamarnwiputh S, Lhieochaiphunt S, Pruksakorn S: Chinese herbal recipe versus diclofenac in symptomatic treatment of osteoarthritis of the knee: a randomized controlled trial. BMC Complement Altern Med. 2004, 4: 19-10.1186/1472-6882-4-19.
Acknowledgements
This study was supported by a grant from the Committee on Chinese Medicine and Pharmacy at the Department of Health, Executive Yuan, Taiwan (CCMP 94-CP-005). We would like to express our gratitude to all of the subjects in this study for their valuable participation and to the staff members at each of the sites and the Bureau of Food and Drug Analysis for their contributions and support.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
SCH performed the study design and statistical analysis, monitored the study, and prepared the manuscript. JNL designed the study and assisted in patient recruitment with assistance from HJC and CCC. PCC conducted the statistical analysis and data interpretation. JDW conceived, designed and coordinated the study, and drafted the manuscript. All authors read and approved the final manuscript.
Electronic supplementary material
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Hsieh, SC., Lai, JN., Chen, PC. et al. Is Duhuo Jisheng Tang containing Xixin safe? A four-week safety study. Chin Med 5, 6 (2010). https://doi.org/10.1186/1749-8546-5-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1749-8546-5-6