
Abstract
Background
Several studies have reported that glucosamine sulfate (GS) can improve knee osteoarthritis (OA) symptomatology. In parallel, the disease-modifying effects of non-steroidal anti-inflammatory drugs (NSAIDs) in knee OA have also been investigated. However, limited literature has reported the combined effect of GS and NSAIDs. The aim of this scoping review is to describe the scope and volume of the literature investigating the potential benefits and synergistic effect of a combination of GS and NSAIDs in patients with knee OA.
Methods
PubMed and Embase were searched for studies published from inception through April 2022, evaluating the effects of the combination of GS and NSAIDs in OA patients, versus either treatment alone. Data are reported narratively.
Results
Five studies were included in this review; 4 were randomized control trials and one was a prospective observational study. The duration of combination treatment was 6 to 12 weeks. The combination was compared to celecoxib in 2 studies, meloxicam in 1, etoricoxib in 1, and a conventional NSAID in 1 (ibuprofen or piroxicam). All 5 studies reported that in patients with knee OA, the combination of GS plus NSAID yielded a significantly greater benefit than single-agent therapy, in terms of outcomes including pain reduction, function, joint stiffness, and markers of inflammatory activity and cartilage degradation.
Conclusion
The 5 studies included in this scoping review all report a significantly greater clinical benefit with a combination of GS plus NSAID compared to either treatment alone. The evidence supports efficacy in reducing pain, improving function, and possibly regulating joint damage. However, further randomized trials with larger sample sizes are warranted to confirm these findings.
Similar content being viewed by others
Background
Osteoarthritis (OA) is a common degenerative musculoskeletal disorder that causes significant health-related and social problems. The major symptoms of OA include chronic pain, functional impairment, instability, and deformity, which can lead to impaired quality of life [1, 2]. Recently, data from the 2019 Global Burden of Disease study have shown that the prevalence of OA increased dramatically, from 247.51 million in 1990 to 527.81 million in 2019, at a rate of 113.25%. Over the same period, the global trend in years lived with disability due to OA increased by 114.5% [3].
Current treatment options for OA include non-pharmacological, pharmacological, and surgical interventions, based on disease severity and joint site [4]. Among the various pharmacological interventions, the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) algorithm recommends the use of symptomatic slow-acting drugs for osteoarthritis (SYSADOAs). This includes prescription-grade glucosamine sulfate (pGS) or chondroitin sulfate (CS) as first-line therapy for long-term background treatment, and paracetamol as short-term rescue medication [5]. Although other guidelines, for example, those from AAOS [6], ACR [7], NICE [8], OARSI [9] do not recommend the use of GS or CS as first-line therapy for OA, we believe that available data on efficacy and safety of pGS support its use as a first-line background therapy, particularly as an alternative to widely used drugs, such as paracetamol, which has been reported to have limited clinical efficacy [10] with some safety concerns [11].
Glucosamine, a natural amino monosaccharide, is a normal constituent of glycosaminoglycans. It is present in the extracellular matrix of the cartilage, in the synovial fluid, and in higher quantities in articular cartilage [12]. Glucosamine sulfate (GS) is both an oral supplement of glucosamine and is registered as a drug when prescription-grade. It is thought to have anti-inflammatory and anti-apoptotic effects on articular cartilage and bone, and reportedly also has prebiotic properties [13,14,15]. Not all guidelines for the treatment of OA have taken into consideration the distinction between studies that used prescription drugs, and studies that used food supplements, or the distinction between studies carried out with GS and Glucosamine hydrochloride (characterized by a low pharmacokinetic profile compared to GS).
International guidelines [7, 9, 16] provide (strong or conditional) recommendations for the usage of oral non-steroidal anti-inflammatory drugs (NSAIDs) for patients with knee, hip, and/or hand OA. NSAIDs can be categorized into conventional NSAIDs and selective cyclooxygenase 2 inhibitors (COX-2) [16], with existing evidence that certain drugs in the NSAID class may have a more favourable safety profile than others. In this context, it is suggested that selective COX-2 inhibitors be preferred in individuals with gastrointestinal (GI) comorbidities [7, 9, 16] because they have a more favourable upper GI safety profile than non-selective NSAIDs. Oral NSAID therapy is the mainstay of pharmacological management in knee OA (KOA) [7], although few international OA guidelines address the relative merits of different drugs among the selective and non-selective NSAIDs. There is nonetheless consensus that NSAID dosage should be as low as possible, and treatment duration should be as short as possible [7, 9]. The ESCEO clearly recommends the use of oral NSAIDs (selective or non-selective) in the second step of its management algorithm, when subjects still have pain or functional limitation after background therapy with SYSADOAs. In the ESCEO algorithm [5], it is suggested that NSAIDs be used only intermittently for longer cycles, and the appropriate molecule should be selected based on the patient’s risk profile.
Celecoxib (a COX-2 inhibitor) may be considered the preferred oral NSAID, due to its favourable balance between good short-term efficacy in OA and a lower propensity for toxicity, especially at the GI and cardiovascular (CV) levels [5]. In a pre-specified secondary analysis of the PRECISION trial, Obeid et al. reported a significantly lower risk of the composite cardiorenal outcome (adjudicated renal event, hospitalization for congestive heart failure or for hypertension) with celecoxib as compared to ibuprofen, and a trend towards a lower risk as compared with naproxen, highlighting the more favourable cardiorenal safety profile of celecoxib [17]. Another clinical trial reported a significantly lower risk of clinically significant upper or lower GI events with celecoxib, as compared to a combination of diclofenac plus omeprazole [18]. Recent evidence further suggests that COX-2 inhibitors may exhibit disease-modifying effects, in addition to their analgesic and anti-inflammatory properties [19,20,21,22]. Several in vitro and in vivo studies have reported that celecoxib in particular demonstrates disease-modifying OA effects [19, 23,24,25]. A recent in vitro study also suggested that a combination of pGS and celecoxib provides a synergistic chondroprotective and anti-inflammatory effect on chondrocyte cultures [26].
To provide a complete understanding of the possible synergistic effects of the combination of GS and NSAIDs, we conducted a scoping review. A scoping review is an ideal tool to assess the extent of the current literature in terms of volume and scope, with a view to summarizing the available body of research evidence. It applies the same rigorous methods as a systematic review for the selection and analysis of potentially eligible publications in the field of interest [27]. Finally, it provides a descriptive overview of the relevant literature, albeit without evaluating individual studies or synthesizing evidence from different studies [28].
Therefore, the objective of this scoping review was to systematically review the literature and summarize available evidence regarding the possible synergistic effect of a combination of GS plus NSAIDs, in reducing pain and improving function, and potentially regulating cartilage damage, as compared to either GS or NSAIDs alone, in people affected by KOA.
Methods
Study design
For this scoping review, a comprehensive literature search was performed to identify all studies related to the question “Does a synergistic action of NSAIDs and GS exist in human beings for the treatment knee osteoarthritis?” The scoping review was designed using the following steps: (1) Convening a research team comprised of health care professionals, and experts in the field of osteoarthritis and research analysis; (2) developing a search strategy; (3) determining the inclusion and exclusion criteria; (4) identifying the relevant studies through a database search; (5) screening and study selection; (6) data extraction and charting; (7) summarizing and reporting the results. This report of the scoping review results follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) extension for Scoping Reviews. The review followed a pre-planned protocol, which is available from the corresponding author on reasonable written request.
Search strategy
The literature search was run in MEDLINE, Cochrane Central, and Embase. The following key search terms were combined: ‘Glucosamine sulfate’, ‘Non-steroidal anti-inflammatory drugs’, ‘Celecoxib’, ‘Cyclooxygenase 2 inhibitors’, and ‘Human beings’. Medical subject headings (MeSH) and other relevant keywords (for e.g., NSAIDs, 2-Amino-2-Deoxyglucose, etc.) were used depending on the database. The search terms were combined using Boolean operators such as AND/OR to extract the appropriate results. The search included all studies available in the databases from inception through April 2022 and was restricted to literature published in the English language. The detailed search strategy and search strings are presented in Additional file 1.
Eligibility criteria
We included studies that met the following inclusion criteria: Randomized controlled trials (RCTs), prospective cohort studies, non-randomized controlled trials, quasi-experimental studies, retrospective cohort studies or case–control studies investigating the concomitant use of GS plus NSAIDs compared to either GS or NSAIDs alone. We excluded studies not published in English, as well as reviews, case reports, consensus statements, and study protocols. Non-human studies and studies reporting a head-to-head comparison of NSAIDs vs GS were also excluded.
Data extraction
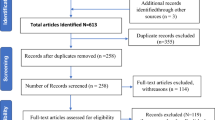
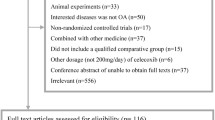
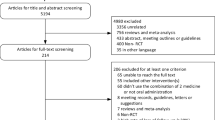
In the first stage, all the titles and abstracts resulting from the literature search were reviewed by two independent authors (NV and SM). Duplicate studies, studies not published in English, and studies without abstracts were removed. In the next stage, the inclusion and exclusion criteria were verified, and articles were filtered as per the eligibility criteria, by two independent authors (NV and SM). In case of disagreement, a consensus was obtained after a thorough discussion. The full text of the eligible articles were retrieved, and the reference lists of the full-text articles were manually checked to ensure no relevant eligible studies were overlooked. Then, the following key information was extracted and summarized: name of the study, date of publication, first author, population included, study design, sample size, medications taken in the intervention and control groups, and main findings. Further details of the data extraction are presented in Fig. 1.

Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow chart
Results
Literature search
The database search yielded a total of 659 articles. Of these, 267 studies were excluded because they were either published in a language other than English or were present in duplicate. The title and abstracts of the remaining 392 articles were screened; 378 were excluded due to the nature of the study design (reviews, case reports, consensus statements, or study protocols) or because they did not involve either GS or NSAIDs. After screening, 14 full-text articles were assessed against the eligibility criteria, of which nine were excluded. Finally, 5 studies (4 RCTs and 1 prospective observational study) were included in the scoping review [29,30,31,32,33] (Fig. 1). A summary of the findings of the 5 included studies is presented in Table 1.
Evidence of the synergistic and beneficial effects of the combination of GS and NSAIDs
All 5 studies reported a significant benefit of GS plus NSAIDs compared to GS or NSAID alone in OA. There were no other concomitant interventions in the studies included.
Four RCTs [30,31,32,33] were designed to evaluate the effect of a combination of GS plus NSAIDs versus either agent alone in patients with KOA were included in the scoping review.
Lu Zhijun et al. compared GS plus meloxicam vs meloxicam alone in 88 patients in OA; 20 males and 24 females aged 62 ± 3 years in the treatment group, and 21 males and 23 females aged 60 ± 3 years in the control group [30]. The course of disease was around 8 years on average in both groups. They reported a significant improvement in the primary outcome of clinical symptoms, evaluated by the Lequesne index, in the GS + meloxicam group. Pain scores evaluated by the visual analogue scale (VAS) and motor function, assessed by the Lysholm knee joint score, were also significantly improved with combination therapy, as compared to meloxicam alone. Serum biomarkers of disease activity (C-terminal telopeptide type 1 (CTX-I), CTX-II, cartilage oligomeric matrix protein (COMP), and matrix metalloproteinase-3 (MMP-3)) were also significantly lower in the combination therapy group after treatment. In total, overall clinical effectiveness was significantly higher in the intervention group vs the meloxicam alone group (92.7% vs 75%; p = 0.015). Adverse reactions during treatment were mainly gastrointestinal and pruritus, but were of short duration and spontaneously resolved. No adverse reaction required treatment. The authors therefore concluded that treatment with a combination of meloxicam and GS was more effective than meloxicam alone, in reducing the serum markers and clinical symptoms of OA [30].
In the study by Gang Deng et al., 120 patients with KOA were randomly assigned to a combination of GS plus celecoxib versus celecoxib alone for 8 weeks [31]. The population consisted of 72 males and 48 females aged 45 to 75 years (mean 60.5 ± 5.8 years). The disease duration ranged from 6 months to 15 years, and 64 patients had mild disease, 40 had moderate and 19 had severe disease according to the authors. The primary outcome of total effectiveness was significantly higher in the combination therapy group, vs celecoxib alone (93.33% vs 71.66%, p < 0.05). Similarly, the combination of GS and celecoxib yielded statistically significant improvements in inflammatory markers (TNF-α [15.28 ± 3.60 vs 12.56 ± 3.50], IL-1 [47.51 ± 7.32 vs 41.25 ± 7.58], PGE2 [134.64 ± 17.21 vs 121.38 ± 28.68]), oxidative stress parameters such as malondialdehyde (14.54 ± 7.23 vs 8.35 ± 5.10), pain score (VAS [5.34 ± 1.01 vs 2.36 ± 0.52], Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score [54.23 ± 3.63 vs 40.35 ± 2.36]), and Lysholm knee joint score [75.63 ± 9.15 vs 87.29 ± 10.38] compared with the control group. During treatment, adverse reactions in the observation group (6 events, 10%) were significantly lower than those in control group (13 events, 21.67%, p < 0.05). These findings suggest a benefit of the combination of GS and celecoxib in inhibiting the progression of OA and improving joint function [31].
The study conducted by Sun et al. compared 40 KOA patients receiving etoricoxib alone (control group, 9 males, 31 females, mean age 62 ± 11 years) to 66 patients receiving a combination of GS plus etoricoxib (experimental group, 14 males, 52 females, mean age 61 ± 10) [32]. Disease course was 3.59 and 3.74 years in the control and experimental groups respectively. In terms of the Kellgren-Lawrence classification, there were 9 cases of grade I, 15 cases of grade II, and 16 cases of grade III. Patients were evaluated for knee function, as assessed using the WOMAC, and for clinical efficacy. Bone metabolism indices, growth factors, inflammatory factors, MMPs, nitric oxide (NO)-induced apoptosis-related factors, and mRNA levels of C-Jun N-terminal kinase (JNK) and Wnt5a were determined. The authors found that compared to monotherapy, combination therapy yielded a significant improvement in total clinical efficacy (92.42% vs. 67.50%, P < 0.0001), and significantly reduced WOMAC pain scores (41.83 ± 4.09 vs 63.57 ± 7.3) and inflammatory markers (IL-1β [51.48 ± 4.89 vs 38.56 ± 3.74], IL-17 [205.38 ± 19.76 vs 276.41 ± 26.11], IL-18 [148.73 ± 13.25 vs 184.67 ± 17.13], TNF-α [52.45 ± 5.02 vs 30.52 ± 2.86], MMP-3 [98.46 ± 9.75 vs 158.37 ± 14.82], MMP-9 [30.26 ± 2.97 vs 45.38 ± 4.62], and MMP-13 [152.43 ± 14.72 vs 193.76 ± 18.69]). Furthermore, combination therapy yielded an improvement in markers of bone metabolism and lowered the expression of JNK and Wnt5a, which inhibited the secretion of MMPs, thereby leading to a decrease in the degradation of the cartilage matrix [32].
The fourth RCT, reported by Selvan et al., evaluated the effectiveness of the combination of GS plus a conventional NSAID (ibuprofen or piroxicam) compared with GS alone in patients with mild to moderate OA recruited through the rheumatology outpatient department [33]. A total of 43 patients were treated with GS alone and 39 GS plus either ibuprofen or piroxicam. The average age of females in the study population was lower than that of male participants overall (47.96 ± 5.09 vs 48.98 ± 8.94 respectively), but the average age of the overall population was not specified. WOMAC and VAS scores were used to evaluate the effectiveness of the combination treatment. There were significantly greater decreases in mean WOMAC pain, stiffness and function scores in the combination therapy group after 12 weeks of treatment (mean difference 5.37 (95% CI: 4.97–5.78, p < 0.01) for pain, 2.23 (95% CI: 2.21–2.44, p < 0.01) for stiffness, and 8.20 (95% CI: 7.51–8.89, p < 0.01) for function). There was a significant decrease in mean VAS score in both groups over the treatment period, but the decrease was of significantly greater magnitude in the combination therapy group (p < 0.01). These results confirmed the greater benefit observed with a combination of GS plus a conventional NSAID versus GS alone in mild to moderate OA [33].
Finally, in a prospective observational study by Amuzadeh et al., 30 women ranging in age from 37 to 49 years, with mild KOA treated with celecoxib alone (mean age 45.77 ± 3.42 years) were compared to 30 women treated with a combination of celecoxib and GS (mean age 45.13 ± 3.45 years) [29]. The primary endpoint was the WOMAC index after 8 weeks of treatment. There was a significant reduction in WOMAC pain and morning stiffness scores and a statistically significant improvement in performance (p < 0.0001) in the group receiving combination therapy. The authors concluded that the use of GS and celecoxib in combination is more effective than celecoxib alone in women with early KOA [29].
Discussion
The aim of this scoping review was to explore the possible synergistic effects of the combination of GS and NSAIDs in the management of OA symptoms. Overall, based on the findings of available publications, it seems that the combination of GS plus NSAIDs could yield greater benefit than either medication alone in terms of clinical outcomes and molecular profiles.
Inadequate pain relief, reduced functional capacity and impaired quality of life are common among patients with KOA [34]. Therefore, the key objective of OA treatment is to provide adequate pain relief and avoid disability. In this regard, oral NSAIDs are widely prescribed for KOA patients and are recommended by recently published guidelines [5, 7, 9].
GS has been reported to have prebiotic properties, in addition to its anti-inflammatory and anti-apoptotic effects on cartilage and bone. It works as a substrate for gut microbiota (i.e. sulfate-reducing bacteria that are implicated in the synthesis of anti-inflammatory compounds). Furthermore, GS is a component of the intestinal mucin that is protected from degradation, thus positively affecting gut permeability and reducing low-grade inflammation [15]. However, despite the use of GS as background therapy, many people with KOA may still suffer from pain and limited function. Therefore, a multimodal treatment approach combining GS with NSAIDS may aid in alleviating symptoms.
In this scoping review, we identified five studies that investigated the potential benefits of co-administration of GS and NSAIDs. In 2 of the 5 studies, celecoxib was used, and in all the studies, the treatment duration was between 6 and 12 weeks. In the study conducted by Sun et al. the prescription-grade crystalline GS (pCGS, Rottapharm Ltd) was used [32], while in the remaining studies, GS was used. Only 2 of the studies included in this review reported data regarding the safety of use of GS; one reported no adverse events requiring treatment, while the other reported fewer adverse events in the observation group than in the control group. In the absence of detailed information about the safety profile of the products used, it is difficult to draw any comparisons or conclusions regarding the potential effects of long-term treatment with GS. This point warrants further investigation in long-term, randomized studies that record adverse events using standardized definitions and validated systems for the classification of severity. All the studies identified in this scoping review reported a significantly greater benefit with a combination of GS plus NSAID, compared to either treatment alone. The results of these studies are corroborated by a recent in vitro study that investigated the possible anti-inflammatory and chondroprotective effects of celecoxib plus GS in human OA chondrocytes [26]. In this study, the human OA chondrocytes were incubated with prescription-grade crystalline GS (pCGS), or celecoxib, or both. The findings showed that the combination of GS plus celecoxib significantly reduced gene expression and supernatant release of COX-2, prostaglandin E2, IL-1β, IL-6, TNF-α, MMP-1, MMP-3, MMP-13, while it increased type II collagen (Col2a1), in comparison with basal conditions or IL-1β stimulated cells. The authors further demonstrated a synergistic effect of celecoxib plus GS on OA chondrocyte apoptosis and oxidative stress and postulated that the observed effects were likely mediated by modulation of the nuclear factor (NF)-κB signaling pathway. This study indirectly supports the use of combination therapy of pCGS and celecoxib for the treatment of patients with OA [26].
KOA is a disease with a high rate of treatment failure, often with sub-optimal control of symptoms (i.e. persistent pain and physical impairment), ultimately leading to poor quality of life. A multimodal approach may be more effective in improving patient wellbeing and treatment success rates as compared to a single pharmacological agent. International guidelines [16] and global consensus documents [35,36,37,38,39,40,41] support this strategy. Further, the ESCEO algorithm recommends a stepwise multimodal approach, combining oral NSAIDs with SYSADOAs in patients with persistent symptoms. The combination of non-pharmacological and pharmacological approaches is the best option, and among the pharmacological therapies, add-on treatment with drugs working synergistically can provide better control. The findings of this scoping review support the use of a multimodal approach, using the combination of background therapy with GS plus an NSAID to manage symptoms related to KOA and to delay disease progression, with a potential benefit on the joint structure. However, treatment decisions should be made by the physician according to each patient’s individual risk/benefit profile (e.g., celecoxib is suggested for up to 30 days in patients with increased CV risk, whereas nonselective NSAIDs should be given for less than 7 days). Further, treatment decisions should also take account of patients’ preferences [42, 43].
This review has some limitations. First, we searched only the published literature in PubMed, Cochrane and Embase, and we did not search unstructured databases or the grey literature. As a result, only 5 studies, with limited sample sizes were identified and included in the review. Additionally, among the eligibility criteria, we selected only studies published in the English language. We cannot rule out the possibility that informative studies published in languages other than English may have been overlooked. Second, the follow-up was short in all studies. Third, the treatment combinations varied in the studies included, and different molecules may have different effects on KOA symptomatology. Furthermore, only crystalline GS available as pCGS has been shown to have evidence-based clinical efficacy [44,45,46]. Finally, only two of the studies included in this review reported information about adverse events.
Conclusions
This is the first scoping review to investigate existing literature about the potential benefits or synergistic effect of a combination of GS plus NSAIDs in KOA. This review provides an overview of 5 available clinical studies, which all reported a significantly greater benefit with combination therapy as compared to single-agent therapy, in terms of pain reduction, improvement in function and stiffness, and improvement in biomarkers of inflammation and cartilage degradation. Available data therefore suggest that the combination of GS and NSAIDs may be useful in a multimodal approach in patients with KOA. However, further randomized, controlled studies with larger sample sizes and longer-term follow-up are necessary to draw more robust conclusions about the efficacy and safety of this combination therapy, and to identify the best NSAID to associate with GS in this combination.
Availability of data and materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
Abbreviations
- Col2a1:
-
Type II Collagen
- COX-2:
-
Cyclooxygenase 2 Inhibitors
- CS:
-
Chondroitin Sulfate
- CTX-I:
-
C-terminal telopeptide type 1
- CTX-II:
-
C-terminal telopeptide type 2
- CV:
-
Cardiovascular
- ESCEO:
-
European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases
- GI:
-
Gastrointestinal
- GS:
-
Glucosamine Sulfate
- IL:
-
Interleukin
- JNK:
-
C-Jun N-terminal kinase
- KOA:
-
Knee Osteoarthritis
- LKSS:
-
Lysholm Knee Score Scale
- MMP:
-
Matrix Metalloproteinase
- NF:
-
Nuclear Factor
- NO:
-
Nitric Oxide
- NSAIDs:
-
Non-Steroidal Anti-Inflammatory Drugs
- OA:
-
Osteoarthritis
- pCGS:
-
Prescription-Grade Crystalline GS
- PGE2:
-
Prostaglandin-2
- PRISMA:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses
- RCT:
-
Randomized Control Trials
- SOD:
-
Superoxide Dismutase
- SYSADOAs:
-
Symptomatic Slow-Acting Drugs for Osteoarthritis
- TNF-α:
-
Tumor Necrosis Factor α
- VAS:
-
Visual Analogue Scale
- WOMAC:
-
Western Ontario and McMaster Universities Arthritis Index
References
Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393:1745–59.
Tenti S, et al. Impact of thumb osteoarthritis on pain, function, and quality of life: a comparative study between erosive and non-erosive hand osteoarthritis. Clin Rheumatol. 2020;39:2195–206.
Long H, et al. Prevalence Trends of Site-Specific Osteoarthritis From 1990 to 2019: Findings From the Global Burden of Disease Study 2019. Arthritis Rheumatol. 2022;74:1172–83.
Arden NK, et al. Non-surgical management of knee osteoarthritis: comparison of ESCEO and OARSI 2019 guidelines. Nat Rev Rheumatol. 2021;17:59–66.
Bruyere O, et al. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Semin Arthritis Rheum. 2019;49:337–50.
Brophy RH, Fillingham YA. AAOS Clinical Practice Guideline Summary: Management of Osteoarthritis of the Knee (Nonarthroplasty), Third Edition. J Am Acad Orthop Surg. 2022;30:e721–9.
Kolasinski SL, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Rheumatol. 2020;72:220–33.
Birch S, Lee MS, Robinson N, Alraek T, The UKNICE. Guidelines for Osteoarthritis of the Knee: Lessons Learned in a Narrative Review Addressing Inadvertent Limitations and Bias. J Altern Complement Med. 2014;2017(23):242–6.
Bannuru RR, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27:1578–89.
Leopoldino AO, et al. Paracetamol versus placebo for knee and hip osteoarthritis. Cochrane Database Syst Rev. 2019;2:CD013273.
Aweid O, Haider Z, Saed A, Kalairajah Y. Treatment modalities for hip and knee osteoarthritis: A systematic review of safety. J Orthop Surg (Hong Kong). 2018;26:2309499018808669.
Colletti A, Cicero AFG. Nutraceutical approach to chronic osteoarthritis: from molecular research to clinical evidence. Int J Mol Sci. 2021;22:12920.
Chiu HW, et al. Glucosamine inhibits IL-1beta expression by preserving mitochondrial integrity and disrupting assembly of the NLRP3 inflammasome. Sci Rep. 2019;9:5603.
Mousavi SH, Bakhtiari E, Hosseini A, Jamialahmadi K. Protective effects of glucosamine and its acetylated derivative on serum/glucose deprivation-induced PC12 cells death: Role of reactive oxygen species. Res Pharm Sci. 2018;13:121–9.
Shmagel A, et al. The effects of glucosamine and chondroitin sulfate on gut microbial composition: a systematic review of evidence from animal and human studies. Nutrients. 2019;11:294.
Jordan KM, et al. EULAR Recommendations 2003: an evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann Rheum Dis. 2003;62:1145–55.
Obeid S, et al. Cardiorenal risk of celecoxib compared to naproxen, or ibuprofen in arthritis patients: insights from the PRECISION trial. Eur Heart J Cardiovasc Pharmacother. 2022;8:611.
Chan FK, et al. Celecoxib versus omeprazole and diclofenac in patients with osteoarthritis and rheumatoid arthritis (CONDOR): a randomised trial. Lancet. 2010;376:173–9.
Zweers MC, et al. Celecoxib: considerations regarding its potential disease-modifying properties in osteoarthritis. Arthritis Res Ther. 2011;13:239.
Nakata K, et al. Disease-modifying effects of COX-2 selective inhibitors and non-selective NSAIDs in osteoarthritis: a systematic review. Osteoarthritis Cartilage. 2018;26:1263–73.
Fioravanti A, et al. In vitro effects of VA441, a new selective cyclooxygenase-2 inhibitor, on human osteoarthritic chondrocytes exposed to IL-1beta. J Pharmacol Sci. 2012;120:6–14.
Timur UT, et al. Chondroprotective Actions of Selective COX-2 Inhibitors In Vivo: A Systematic Review. Int J Mol Sci. 2020;21:6962.
Matsuda K, Nakamura S, Matsushita T. Celecoxib inhibits nitric oxide production in chondrocytes of ligament-damaged osteoarthritic rat joints. Rheumatol Int. 2006;26:991–5.
Ou Y, et al. Selective COX-2 inhibitor ameliorates osteoarthritis by repressing apoptosis of chondrocyte. Med Sci Monit. 2012;18:BR247-252.
Mastbergen SC, Jansen NW, Bijlsma JW, Lafeber FP. Differential direct effects of cyclo-oxygenase-1/2 inhibition on proteoglycan turnover of human osteoarthritic cartilage: an in vitro study. Arthritis Res Ther. 2006;8:R2.
Cheleschi S, et al. A combination of celecoxib and glucosamine sulfate has anti-inflammatory and chondroprotective effects: results from an in vitro study on human osteoarthritic chondrocytes. Int J Mol Sci. 2021;22:8980.
Munn Z, et al. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18:143.
Pham MT, et al. A scoping review of scoping reviews: advancing the approach and enhancing the consistency. Res Synth Methods. 2014;5:371–85.
Amuzadeh F, et al. Comparison of the efficacy of combination of glucosamine sulfate and celecoxib versus celecoxib alone for the pain, morning stiffness, function relief of females with osteoarthritis grade 1&2 of the knee (A comparative study). Indian J Fundam Appl Life Sci. 2015;5:129–36.
Lu Z, et al. Therapeutic effects of combined meloxicam and glucosamine sulfate treatment on patients with osteoarthritis, and its effect on serum CTX-I, CTX-II, COMP and MMP-3. Trop J Pharm Res. 2019;18:1553–7.
Deng G, Chen X, Yang K, Wu A, Zeng G. Combined effect of celecoxib and glucosamine sulfate on inflammatory factors and oxidative stress indicators in patients with knee osteoarthritis. Trop J Pharm Res. 2019;18:397–402.
Sun Y, Wang C, Gong C. Repairing effects of glucosamine sulfate in combination with etoricoxib on articular cartilages of patients with knee osteoarthritis. J Orthop Surg Res. 2020;15:150.
Selvan T, Rajiah K, Nainar MS, Mathew EM. A clinical study on glucosamine sulfate versus combination of glucosamine sulfate and NSAIDs in mild to moderate knee osteoarthritis. Sci World J. 2012;2012:902676.
Conaghan PG, et al. Inadequate pain relief and large functional loss among patients with knee osteoarthritis: evidence from a prospective multinational longitudinal study of osteoarthritis real-world therapies. Rheumatology (Oxford). 2015;54:270–7.
Yeap SS, et al. 2019 revised algorithm for the management of knee osteoarthritis: the Southeast Asian viewpoint. Aging Clin Exp Res. 2021;33:1149–56.
Zhang Z, et al. 2021 revised algorithm for the management of knee osteoarthritis-the Chinese viewpoint. Aging Clin Exp Res. 2021;33:2141–7.
Yeap SS, et al. A Malaysian Delphi consensus on managing knee osteoarthritis. BMC Musculoskelet Disord. 2021;22:514.
Pradelli L, et al. Non-Surgical Treatment of Knee Osteoarthritis: Multidisciplinary Italian Consensus on Best Practice. Ther Clin Risk Manag. 2021;17:507–30.
Gnylorybov AM, et al. Expert Opinion on the Extensive Use of Prescription Crystalline Glucosamine Sulfate in the Multimodal Treatment of Osteoarthritis in Ukraine, Kazakhstan, Uzbekistan, and Armenia. Clin Med Insights Arthritis Musculoskelet Disord. 2020;13:1179544120946743.
Kucharz EJ, et al. Endorsement by Central European experts of the revised ESCEO algorithm for the management of knee osteoarthritis. Rheumatol Int. 2019;39:1117–23.
Alexander LAM, et al. Pharmacological Management of Osteoarthritis With a Focus on Symptomatic Slow-Acting Drugs: Recommendations From Leading Russian Experts. J Clin Rheumatol. 2021;27:e533–9.
Hiligsmann M, et al. Patients’ preferences for osteoarthritis treatment: the value of stated-preference studies. Aging Clin Exp Res. 2019;31:1–3.
Turk D, et al. Patient preferences for osteoarthritis pain and chronic low back pain treatments in the United States: a discrete-choice experiment. Osteoarthritis Cartilage. 2020;28:1202–13.
Beaudart C, et al. Symptomatic Efficacy of Pharmacological Treatments for Knee Osteoarthritis: A Systematic Review and a Network Meta-Analysis with a 6-Month Time Horizon. Drugs. 2020;80:1947–59.
Veronese N, et al. Glucosamine sulphate: an umbrella review of health outcomes. Ther Adv Musculoskelet Dis. 2020;12:1759720X20975927.
Kucharz EJ, et al. A review of glucosamine for knee osteoarthritis: why patented crystalline glucosamine sulfate should be differentiated from other glucosamines to maximize clinical outcomes. Curr Med Res Opin. 2016;32:997–1004.
Acknowledgements
Not applicable.
Funding
This work received no funding.
Author information
Authors and Affiliations
Contributions
NV, FE, SM, and AF made substantial contributions to the conception, study design, data analysis, and interpretation. SC was involved in the study design, data analysis, and interpretation. FE revised the manuscript critically for important intellectual content. All authors were involved in drafting the manuscript, read and approved the submitted version, and all authors agree to be held accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
NV and SC declare speaker fees from Viatris. AF worked as a paid consultant for and received speaker fees from Viatris. SM declares receiving grants from Sanofi, Takeda, MSD, GSK, and Pfizer, and has worked as a paid consultant for Sanofi, Takeda, MSD, GSK, Pfizer, Viatris, Merck, and Novavax, and declares speaker fees from Sanofi, Takeda, MSD, GSK, Pfizer, Viatris and Merck. FE has receiving speaker fees from GSK, outside the scope of this work.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Veronese, N., Ecarnot, F., Cheleschi, S. et al. Possible synergic action of non-steroidal anti-inflammatory drugs and glucosamine sulfate for the treatment of knee osteoarthritis: a scoping review. BMC Musculoskelet Disord 23, 1084 (2022). https://doi.org/10.1186/s12891-022-06046-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-06046-6