
Abstract
Background
Gemifloxacin is a synthetic fluoroquinolone antimicrobial agent, which has potent activity against most Gram-negative and Gram-positive organisms. It is indicated for the treatment of community-acquired pneumonia and acute bacterial exacerbation of chronic bronchitis.
Objective
The aim of this study was to assess the clinical potential of a new gemifloxacin 200 mg intravenous formulation by comparing its pharmacokinetic characteristics with those of the branded Factive® gemifloxacin tablet.
Methods
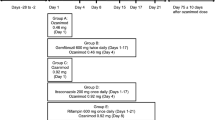
A single-dose, open-label, randomized-sequence, two-period crossover study was performed with 17 healthy male volunteers. The two treatment periods were separated by a 1-week washout period. Blood samples were taken for up to 48 h post-dose. Plasma gemifloxacin concentrations were determined by a validated high-performance liquid chromatography–tandem mass spectrometry method. To calculate the pharmacokinetic parameters, noncompartmental analysis was performed. The two formulations were considered to be pharmacokinetically equivalent if the 90 % confidence intervals (CIs) of the log-transformed ratios (intravenous/oral formulations) of the area under the plasma concentration–time curve (AUC) from time zero to the time of the last measurable concentration (AUClast) and the AUC from time zero to infinity (AUC∞) were within the standard bioequivalence range (0.8–1.25). Safety and tolerability were evaluated on the basis of physical examinations, vital signs, electrocardiograms, clinical laboratory tests and adverse event monitoring.
Results
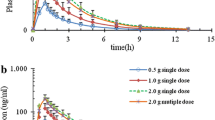
Seventeen subjects were enrolled, and 15 subjects completed the study. Sixteen subjects received intravenous 200 mg gemifloxacin and 15 received oral 320 mg gemifloxacin. The 15 subjects in the pharmacokinetic analysis set had a mean (standard deviation [SD]) age, height and weight of 27.2 (5.3) years, 173.5 (4.4) cm and 67.3 (7.4) kg, respectively. Both formulations had similar pharmacokinetic profiles. For the intravenous formulation, the mean (SD) AUClast, AUC∞ and maximum plasma concentration (C max) values were 9.12 (4.03) μg·h/mL, 9.26 (4.07) μg·h/mL and 2.90 (1.65) μg/mL, respectively, while these values for the oral formulation were 9.44 (3.34) μg·h/mL, 9.60 (3.49) μg·h/mL and 2.03 (0.95) μg/mL, respectively. For the intravenous and oral formulations, the median (range) time to reach C max (t max) values were 0.9 (0.7–1.0) and 1.0 (0.5–2.0) h, respectively. The mean relative bioavailability was 68.99 %. The 90 % CI of the ratios of the log-transformed values of AUClast and AUC∞ was 0.82–1.07. There were no serious adverse events. The intravenous and oral formulations were associated with treatment-emergent adverse event incidences of 63 % (10/16) and 13 % (2/15), respectively. After the intravenous formulation was administered, application site pain and paraesthesia were the most frequently reported adverse events (31 and 25 %, respectively). All adverse events resolved spontaneously without treatment.
Conclusion
Intravenous 200 mg and oral 320 mg formulations of gemifloxacin are equivalent in terms of AUC following a single dose in healthy male subjects.


Similar content being viewed by others

References
Bhavnani SM, Andes DR. Gemifloxacin for the treatment of respiratory tract infections: in vitro susceptibility, pharmacokinetics and pharmacodynamics, clinical efficacy, and safety. Pharmacotherapy. 2005;25(5):717–40.
Gee T, Andrews JM, Ashby JP, et al. Pharmacokinetics and tissue penetration of gemifloxacin following a single oral dose. J Antimicrob Chemother. 2001;47(4):431–4.
Morrissey I, Clark S, Mathias I. The bactericidal activity of gemifloxacin (SB-265805). J Med Microbiol. 2000;49(9):841–4.
Allen A, Bygate E, Vousden M, et al. Multiple-dose pharmacokinetics and tolerability of gemifloxacin administered orally to healthy volunteers. Antimicrob Agents Chemother. 2001;45(2):540–5.
Gajjar DA, LaCreta FP, Uderman HD, et al. A dose-escalation study of the safety, tolerability, and pharmacokinetics of intravenous gatifloxacin in healthy adult men. Pharmacotherapy. 2000;20(6 Pt 2):49S–58S.
Lowe MN, Lamb HM. Gemifloxacin. Drugs. 2000;59(5):1137–47 (discussion 1148).
Korean Pharmaceutical Information Service. http://www.kpis.or.kr/st/StfMedsearch/rrMedSearchView01.do. Accessed 30 Sep 2013.
LG Life Sciences Ltd. Factive: prescribing information. 2008. http://www.accessdata.fda.gov/drugsatfda_docs/label/2008/021158s013lbl.pdf. Accessed 30 Sep 2013.
WMA. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. 2008. http://www.wma.net/en/30publications/10policies/b3/17c.pdf. Accessed 30 Sep 2013.
Doyle E, Fowles SE, McDonnell DF, et al. Rapid determination of gemifloxacin in human plasma by high-performance liquid chromatography-tandem mass spectrometry. J Chromatogr B Biomed Sci Appl. 2000;746(2):191–8.
Cohen JS. Peripheral neuropathy associated with fluoroquinolones. Ann Pharmacother. 2001;35(12):1540–7.
Allen A, Bygate E, Oliver S, et al. Pharmacokinetics and tolerability of gemifloxacin (SB-265805) after administration of single oral doses to healthy volunteers. Antimicrob Agents Chemother. 2000;44(6):1604–8.
Data on File: Dixon RM. A single-blind dose rising study to assess the tolerability and preliminary pharmacokinetics of intravenous gemifloxacin in healthy male volunteers. Harlow: SmithKline Beecham Pharmaceuticals; 1999.
LaCreta FP, Kaul S, Kollia GD, et al. Interchangeability of 400-mg intravenous and oral gatifloxacin in healthy adults. Pharmacotherapy. 2000;20(6 Pt 2):59S–66S.
LaPlante KL, Rybak MJ, Tsuji B, et al. Fluoroquinolone resistance in Streptococcus pneumoniae: area under the concentration–time curve/MIC ratio and resistance development with gatifloxacin, gemifloxacin, levofloxacin, and moxifloxacin. Antimicrob Agents Chemother. 2007;51(4):1315–20.
Martinez FJ, Anzueto A. Appropriate outpatient treatment of acute bacterial exacerbations of chronic bronchitis. Am J Med. 2005;118(Suppl 7A):39S–44S.
LaCreta FP, Kollia GD, Duncan G, et al. Age and gender effects on the pharmacokinetics of gatifloxacin. Pharmacotherapy. 2000;20(6 Pt 2):67S–75S.
Acknowledgments
The authors acknowledge the in-house support provided by the Clinical Trial Center at Asan Medical Center (Seoul, Korea). All authors approved this manuscript and the corresponding author made the final decision regarding its submission.
This research was conducted by Asan Medical Center and was sponsored by LG Life Sciences (Seoul, Korea). None of the authors has any affiliations with or involvement in any organization or entity with any financial interests (such as honoraria; educational grants; participation in speaker’s bureaus; membership, employment, consultations, stock ownership, other equity interests; and expert testimony or patent licensing arrangements), or non-financial interests (such as personal or professional relationships, affiliations, knowledge or benefits) in the subject matter or materials discussed in this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, M.J., Lim, HS., Cho, SH. et al. Comparative Pharmacokinetics and Bioavailability of Gemifloxacin Administered as an Intravenous 200 mg Formulation or an Oral 320 mg Tablet. Clin Drug Investig 34, 195–201 (2014). https://doi.org/10.1007/s40261-013-0164-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-013-0164-z