
Abstract
Background
Adjuvant chemotherapy with or without radiation in patients with completely resected gastric and gastroesophageal (GE) junction cancer has been associated with better outcomes. In practice, however, there are often delays in commencing adjuvant therapy. The study aims to determine the prognostic importance of timing of adjuvant therapy in such patients.
Methods
A cohort of patients with early stage (IB–IVM0) gastric and GE junction cancer diagnosed between 2002 and 2007 in the province of Saskatchewan was assessed. Cox proportional hazard analysis was used to identify various clinic-pathological factors that correlate with disease-free survival (DFS).
Results
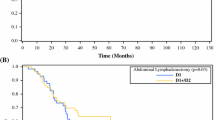
One hundred seventy-four eligible patients with a median age of 71 years (range 36–93) and M/F ratio of 113:61 were identified. Of 174 patients, 60 (35 %) received adjuvant therapy. Median follow-up was 18 months (interquartile range 9–37). Twenty-eight percent received adjuvant therapy within 56 days. Median DFS of patients who received adjuvant therapy within 56 days was 37 months (95 % CI 6.6–67.3) versus 33 months (95 % CI 18.3–47.7) if adjuvant therapy was administered beyond 56 days (p = 0.67). On multivariate analysis, state III–IVM0 disease, hazard ratio (HR) 2.4 (95%CI 1.6–3.5), and age ≥65 years, HR 2.2 (95 % CI 1.4–3.5), were significantly correlated with inferior disease-free survival.
Conclusions
Only about one third of patients who received adjuvant therapy were treated within 56 days of surgery. Although stages III and IVM0 and older age were associated with inferior outcome, delay in adjuvant therapy was not associated with inferior survival.



Similar content being viewed by others


References
Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin. 2011;61:69.
Siegel R, Naishadham D, Jemal A. Cancer statistics. CA Cancer J Clin. 2013;63:11.
Paoletti X, Oba K, Burzykowski T, Michiels S, Ohashi Y, et al. Benefit of adjuvant chemotherapy for resectable gastric cancer: a meta-analysis. JAMA. 2010;303:1729–37.
Macdonald JS, Smalley SR, Benedetti J, et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med. 2001;345:725.
Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11.
Sakuramoto S, Sasako M, Yamaguchi T, et al. Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N Engl J Med. 2007;357:1810–20.
Bang Y, Kim Y, Yang H, et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomized controlled trial. Lancet. 2012;379:315–21.
Lohrisch C, Paltiel C, Gelmon K, et al. Impact on survival of time from definitive surgery to initiation of adjuvant chemotherapy for early-stage breast cancer. J Clin Oncol. 2006;24:4888–94.
Biagi JJ, Raphael MJ, Mackillop WJ, et al. Association between time to initiation of adjuvant chemotherapy and survival in colorectal cancer: a systematic review and meta-analysis. JAMA. 2011;305:2335–42.
Greene FL, Page DL, Fleming ID, et al. American Joint Committee on Cancer. American Cancer Society. AJCC cancer staging manual. 6th ed. New York: Springer; 2002. p. 99–106.
Hundahl SA, Phillips JL, Menck HR. The National Cancer Data Base report on poor survival of U.S. gastric carcinoma patients treated with gastrectomy: fifth edition American Joint Committee on Cancer staging, proximal disease, and the “different disease” hypothesis. Cancer. 2000;88:921–32.
Theuer CP, Kurosaki T, Taylor TH, et al. Unique features of gastric carcinoma in the young: a population-based analysis. Cancer. 1998;83:25–33.
Cronin-Fenton DP, Mooney MM, Clegg LX, et al. Treatment and survival in a population-based sample of patients diagnosed with gastroesophageal adenocarcinoma. World J Gastroenterol. 2008;14:3165–73.
Nagata T, Ichikawa D, Komatsu S, et al. Prognostic impact of microscopic positive margin in gastric cancer patients. J Surg Oncol. 2011;104:592–7.
Wang SY, Yeh CN, Lee HL, et al. Clinical impact of positive surgical margin status on gastric cancer patients undergoing gastrectomy. Ann Surg Oncol. 2009;16(10):2738–43.
Schwarz RE, Smith D. Clinical impact of lymphadenectomy extent in resectable gastric cancer of advanced stage. Ann Surg Oncol. 2007;14:317–28.
Cancer Care Ontario. Target wait times for cancer surgery in Ontario https://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=43244.
Witzig R, Schönberger B, Fink U, et al. Delays in diagnosis and therapy of gastric cancer and esophageal adenocarcinoma. Endoscopy. 2006;38:1122–6.
Acknowledgment
We would like to thank to Dr. Tong Zhu, Mrs. Carla Woites, and Mrs. Coralee Prodaehl for their contribution to this project, and the Saskatchewan Cancer Agency for providing the research grant.
Funding Source
This study is part of a project funded by the Saskatchewan Cancer Agency.
Conflicts of Interest
None of the authors have any conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ahmed, S., Iqbal, N., Yadav, S. et al. Time to Adjuvant Therapy and Other Variables in Localized Gastric and Gastroesophageal Junction (GEJ) Cancer (IJGC-D-13-00162). J Gastrointest Canc 45, 284–290 (2014). https://doi.org/10.1007/s12029-014-9585-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-014-9585-z