
Abstract
Background
The optimal time between neoadjuvant chemotherapy (NAC) and gastrectomy for gastric cancer (GC) remains unknown. This study aimed to investigate the association between the time-to-surgery (TTS) interval and the major pathologic response (mPR).
Methods
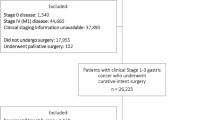
In this study, 280 consecutive GC patients who underwent NAC followed by gastrectomy between 2014 and 2018 were retrospectively analyzed by the use of prospectively collected databases from three major GC treatment centers in Lithuania and Estonia. Based on TTS, they were grouped into three interval categories: the early-surgery group (ESG: ≤ 30 days; n = 70), the standard-surgery group (SSG: 31–43 days; n = 138), and the delayed-surgery group (DSG: ≥ 44 days, n = 72). The primary outcome of the study was the mPR rate. The secondary end points were postoperative morbidity, mortality, oncologic safety (measured as the number of resected lymph nodes and radicality), and long-term outcomes.
Results
The mPR rate for the ESG group (32.9%) was significantly higher than for the SSG group (20.3%) or the DSG group (16.7%) (p = 0.047). Furthermore, after adjustment for patient, tumor, and treatment characteristics, the odds for achievement of mPR were twofold higher for the patients undergoing early surgery (odds ratio [OR] 2.09; 95% conflidence interval [CI] 1.01–4.34; p = 0.047). Overall morbidity, severe complications, 30-day mortality, R0 resection, and retrieval of at least 15 lymph nodes rates were similar across the study groups. In addition, the long-term outcomes did not differ between the study groups.
Conclusions
This study suggests that an interval of no more than 30 days between the end of NAC and gastrectomy is associated with a higher mPR rate, the same oncologic safety of surgery, and similar morbidity and mortality.



Similar content being viewed by others


Change history
15 July 2021
A Correction to this paper has been published: https://doi.org/10.1245/s10434-021-10462-8
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.
Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJH, Nicolson M, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11–20.
Ychou M, Boige V, Pignon J-P, Conroy T, Bouché O, Lebreton G, et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol Off J Am Soc Clin Oncol. 2011;29:1715–21.
Tokunaga M, Sato Y, Nakagawa M, Aburatani T, Matsuyama T, Nakajima Y, et al. Perioperative chemotherapy for locally advanced gastric cancer in Japan: current and future perspectives. Surg Today. 2020;50:30–7.
Reddavid R, Sofia S, Chiaro P, Colli F, Trapani R, Esposito L, et al. Neoadjuvant chemotherapy for gastric cancer: Is it a must or a fake? World J Gastroenterol. 2018;24:274–89.
Li Z, Shan F, Wang Y, Zhang Y, Zhang L, Li S, et al. Correlation of pathological complete response with survival after neoadjuvant chemotherapy in gastric or gastroesophageal junction cancer treated with radical surgery: a meta-analysis. PLOS ONE. Pub Library Sci. 2018;13:e0189294.
Al-Batran S-E, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393:1948–57.
Uson Junior PLS, Santos VM, Bugano DDG, Victor E da S, Rother ET, Maluf FC. Systematic review and meta-analysis of docetaxel perioperative chemotherapy regimens in gastric and esophagogastric tumors. Sci Rep Nature Publishing Group. 2019;9:15806.
Al-Batran S-E, Hofheinz RD, Pauligk C, Kopp H-G, Haag GM, Luley KB, et al. Histopathological regression after neoadjuvant docetaxel, oxaliplatin, fluorouracil, and leucovorin versus epirubicin, cisplatin, and fluorouracil or capecitabine in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4-AIO): results from the phase 2 part of a multicentre, open-label, randomised phase 2/3 trial. Lancet Oncol. 2016;17:1697–708.
Spoerl S, Novotny A, Al-Batran S-E, Lordick F, Thuss-Patience P, Pauligk C, et al. Histopathological regression predicts treatment outcome in locally advanced esophagogastric adenocarcinoma. Eur J Cancer. 2018;90:26–33.
Becker K, Langer R, Reim D, Novotny A, Meyer zum Buschenfelde C, Engel J, et al. Significance of histopathological tumor regression after neoadjuvant chemotherapy in gastric adenocarcinomas: a summary of 480 cases. Ann Surg. 2011;253:934–9.
Achilli P, De Martini P, Ceresoli M, Mari GM, Costanzi A, Maggioni D, et al. Tumor response evaluation after neoadjuvant chemotherapy in locally advanced gastric adenocarcinoma: a prospective, multi-center cohort study. J Gastrointest Oncol. 2017;8:1018–25.
Liu Y, Zhang K-C, Huang X-H, Xi H-Q, Gao Y-H, Liang W-Q, et al. Timing of surgery after neoadjuvant chemotherapy for gastric cancer: impact on outcomes. World J Gastroenterol. 2018;24:257–65.
Francois Y, Nemoz CJ, Baulieux J, Vignal J, Grandjean JP, Partensky C, et al. Influence of the interval between preoperative radiation therapy and surgery on downstaging and on the rate of sphincter-sparing surgery for rectal cancer: the Lyon R90-01 randomized trial. J Clin Oncol Off J Am Soc Clin Oncol. 1999;17:2396.
Tulchinsky H, Shacham-Shmueli E, Klausner JM, Inbar M, Geva R. Should a loop ileostomy closure in rectal cancer patients be done during or after adjuvant chemotherapy? J Surg Oncol. 2014;109:266–9.
de Campos-Lobato LF, Geisler DP, da Luz Moreira A, Stocchi L, Dietz D, Kalady MF. Neoadjuvant therapy for rectal cancer: the impact of longer interval between chemoradiation and surgery. J Gastrointest Surg Off J Soc Surg Aliment Tract. 2011;15:444–50.
Wolthuis AM, Penninckx F, Haustermans K, De Hertogh G, Fieuws S, Van Cutsem E, et al. Impact of interval between neoadjuvant chemoradiotherapy and TME for locally advanced rectal cancer on pathologic response and oncologic outcome. Ann Surg Oncol. 2012;19:2833–41.
Probst CP, Becerra AZ, Aquina CT, Tejani MA, Wexner SD, Garcia-Aguilar J, et al. Extended intervals after neoadjuvant therapy in locally advanced rectal cancer: the key to improved tumor response and potential organ preservation. J Am Coll Surg. 2015;221:430–40.
Shaikh T, Ruth K, Scott WJ, Burtness BA, Cohen SJ, Konski AA, et al. Increased time from neoadjuvant chemoradiation to surgery is associated with higher pathologic complete response rates in esophageal cancer. Ann Thorac Surg. 2015;99:270–6.
Ruol A, Portale G, Zaninotto G, Cagol M, Cavallin F, Castoro C, et al. Results of esophagectomy for esophageal cancer in elderly patients: age has little influence on outcome and survival. J Thorac Cardiovasc Surg. 2007;133:1186–92.
Omarini C, Guaitoli G, Noventa S, Andreotti A, Gambini A, Palma E, et al. Impact of time to surgery after neoadjuvant chemotherapy in operable breast cancer patients. Eur J Surg Oncol J Eur Soc Surg Oncol Br Assoc Surg Oncol. 2017;43:613–8.
Japanese gastric cancer treatment guidelines 2014 (version 4). Gastric Cancer. 2017;20:1–19.
Dikken JL, van Sandick JW, Maurits Swellengrebel H, Lind PA, Putter H, Jansen EP, et al. Neoadjuvant chemotherapy followed by surgery and chemotherapy or by surgery and chemoradiotherapy for patients with resectable gastric cancer (CRITICS). BMC Cancer. 2011;11:329.
Becker K, Mueller JD, Schulmacher C, Ott K, Fink U, Busch R, et al. Histomorphology and grading of regression in gastric carcinoma treated with neoadjuvant chemotherapy. Cancer. 2003;98:1521–30.
Du D, Su Z, Wang D, Liu W, Wei Z. Optimal interval to surgery after neoadjuvant chemoradiotherapy in rectal cancer: a systematic review and meta-analysis. Clin Colorectal Cancer. 2018;17:13–24.
Terzi C, Bingul M, Arslan NC, Ozturk E, Canda AE, Isik O, et al. Randomized controlled trial of 8 weeks’ versus 12 weeks’ interval between neoadjuvant chemoradiotherapy and surgery for locally advanced rectal cancer. Colorectal Dis Off J Assoc Coloproctol G B Irel. 2020;22:279–88.
Werf LR van der, Dikken JL, Willik EM van der, Henegouwen MI van B, Nieuwenhuijzen Ga P, Wijnhoven BPL, et al. Time interval between neoadjuvant chemoradiotherapy and surgery for oesophageal or junctional cancer: a nationwide study. Eur J Cancer. 2018;91:76–85.
Haisley KR, Laird AE, Nabavizadeh N, Gatter KM, Holland JM, Vaccaro GM, et al. Association of intervals between neoadjuvant chemoradiation and surgical resection with pathologic complete response and survival in patients with esophageal cancer. JAMA Surg. 2016;151:e162743.
Lee A, Wong AT, Schwartz D, Weiner JP, Osborn VW, Schreiber D. Is there a benefit to prolonging the interval between neoadjuvant chemoradiation and esophagectomy in esophageal cancer? Ann Thorac Surg. 2016;102:433–8.
Sanford RA, Lei X, Barcenas CH, Mittendorf EA, Caudle AS, Valero V, et al. Impact of time from completion of neoadjuvant chemotherapy to surgery on survival outcomes in breast cancer patients. Ann Surg Oncol. 2016;23:1515–21.
Medler TR, Cotechini T, Coussens LM. Immune response to cancer therapy: mounting an effective antitumor response and mechanisms of resistance. Trends Cancer. 2015;1:66–75.
Monsellato I, Alongi F, Bertocchi E, Gori S, Ruffo G, Cassinotti E, et al. Standard (8 weeks) versus long (12 weeks) timing to minimally invasive surgery after neoadjuvant chemoradiotherapy for rectal cancer: a multicenter randomized controlled parallel group trial (TiMiSNAR). BMC Cancer. 2019;19:1215.
Norton L. Evolving concepts in the systemic drug therapy of breast cancer. Semin Oncol. 1997;24(4 Suppl 10):S10.
Zhu Y, Sun Y, Hu S, Jiang Y, Yue J, Xue X, et al. Comparison of five tumor regression grading systems for gastric adenocarcinoma after neoadjuvant chemotherapy: a retrospective study of 192 cases from National Cancer Center in China. BMC Gastroenterol. 2017;17(1):41.
Alderson D, Cunningham D, Nankivell M, Blazeby JM, Griffin SM, Crellin A, et al. Neoadjuvant cisplatin and fluorouracil versus epirubicin, cisplatin, and capecitabine followed by resection in patients with oesophageal adenocarcinoma (UK MRC OE05): an open-label, randomised phase 3 trial. Lancet Oncol. 2017;18:1249–60.
Acknowledgment
All data materials and analytical methods are available from the corresponding author upon a reasonable request.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
There are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article has been revised: the Conclusions section of the Abstract was corrected.
Rights and permissions
About this article

Cite this article
Bausys, A., Ümarik, T., Luksta, M. et al. Impact of the Interval Between Neoadjuvant Chemotherapy and Gastrectomy on Short- and Long-Term Outcomes for Patients with Advanced Gastric Cancer. Ann Surg Oncol 28, 4444–4455 (2021). https://doi.org/10.1245/s10434-020-09507-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-09507-1