
Abstract
Background
Recovery is common after subarachnoid hemorrhage (SAH), even in patients who are severely disabled at hospital discharge. Little is known about predictors of late recovery in such patients, even though such knowledge may influence treatment decisions. We hypothesized that cerebral infarction volume would be associated with 3 months outcomes in patients who are severely disabled at 14 days.
Methods
We prospectively identified consecutive aneurysmal SAH patients, documented the development of cerebral infarction, and ascertained the modified Rankin Scale (mRS) at 14 days and 3 months. We included patients with mRS 4 or 5 and NIH Stroke Scale (NIHSS) at least 8 on hospital day 14 (i.e., severe neurologic impairment) and calculated infarct volume in a semi-automated fashion using CT imaging. We explored outcome determinants with ordinal regression.
Results
At 14 days, 66 patients were severely disabled, 65 (98.5 %) of whom had mRS of 5; the median NIHSS was 21 [14–24]. At 3 months, 20 (32.8 %) of the 61 patients with known outcomes were independent. Larger infarction volumes were associated with death (20.4 vs. 0.85 mL, P = 0.02). In ordinal regression, increased infarct volume was associated with the worse mRS after correction for WFNS grade, age, and withdrawal of life support (OR 1.01 per mL of infarct, 95 % CI 1.01–1.03, P = 0.01).
Conclusions
After SAH, even with severe neurological injury at 14 days, good recovery is frequent and is associated with lower infarction volume. These data may help clinicians inform surrogate decision makers as they plan the future care of such severely disabled patients.
Similar content being viewed by others


Introduction
Following aneurysmal subarachnoid hemorrhage (SAH), approximately 51–60 % of patients are functionally independent at 3–12 months [1, 2]. Even patients whose hospital courses leave them severely disabled at discharge may regain independence, including 38 % of patients discharged to nursing homes and patients with prolonged coma [3, 4]. Knowing the likelihood of late recovery, despite short-term disability, could be useful to patients and their families when making treatment decisions [5]. The likelihood of favorable outcome is obvious in patients with good functional status at 2 weeks, making prognostication nearly irrelevant in clinical decision making. Little information is available regarding prognostic features among severely disabled patients at that same stage, where goals of care considerations and planning for future care are major concerns for clinicians advising surrogate decision makers.
The presence of radiographic cerebral infarction (RCI) has been associated with poor long-term functional outcomes, independently of clinical grade at presentation, subsequent clinical deterioration, or radiographic vasospasm [6–9]. However, dichotomous identification of infarcts as either present or absent might overestimate the consequences of small infarctions and underestimate the impact of large ones [8]. In patients with ischemic stroke, larger infarct volumes are independently associated with worse outcomes [10]. Thus, we hypothesized that among patients who remain severely disabled at 14 days following SAH, larger total infarct volumes would be associated with worse long-term functional outcomes.
Methods
We prospectively enrolled patients with SAH admitted to our institution from January 2006 to August 2011. SAH was diagnosed by the admission CT scan or by xanthochromia of the cerebrospinal fluid, if the CT was non-diagnostic. SAH due to trauma, arteriovenous malformation rupture, vasculitis, or other non-aneurysmal structural lesions was excluded. We prospectively recorded clinical variables, documenting demographic data and past medical history on standardized forms. Neurological status on admission was assessed by a board-certified neurologist using the World Federation of Neurosurgical Societies (WFNS) scale [11], and the NIH Stroke Scale (NIHSS) was recorded on admission and at the earlier of hospital discharge or 14 days [12]. The admission CT was graded according to the Claassen scale [13]. Functional outcomes were obtained at the earlier of 14 days or discharge, 28 days, and 3 months with the modified Rankin scale (mRS), using a validated questionnaire [14, 15]. The mRS is scored from 0 (no symptoms) to 6 (dead), with scores ≤3 indicating independence for daily living.
This analysis considered only patients with mRS scores of 4 or 5 (dependent or bed-bound) and NIHSS scores ≥8 (a moderately severe deficit) at 14 days from symptom onset (all but one had mRS 5). These values were chosen to select for patients with disability due to neurological deficits rather than those with restricted mobility due to ventricular drains or other devices, and are consistent with groupings used in other studies [16, 17].
Diagnostic catheter or CT angiography and aneurysm obliteration with surgical clipping or endovascular coiling were performed as soon as possible. Enteric nimodipine was given unless the systolic blood pressure was <120 mmHg. Patients received pravastatin 40 mg daily as part of routine care [18]. Transcranial Doppler (TCD) sonography was performed daily. We prospectively recorded the presence of mean transcranial Doppler velocities >120 and >200 cm/s, as well as new focal neurologic deficit or depressed mental status without other explanation (clinical deterioration due to delayed cerebral ischemia, DCI). Patients with such deterioration were treated with hyperdynamic therapy [19]. Diagnostic angiography was performed with balloon angioplasty and/or intra-arterial vasodilators at the discretion of the treating team.
We obtained neuroimaging on admission, post-operatively, and at the time of any clinical change. All RCIs were prospectively recorded during the index hospitalization by study staff as a new hypodensity on computed tomography (CT) not present on admission or due to post-operative changes, resolving edema or resolving hemorrhage [20]. Because of its high inter-rater reliability, we believe that RCI is a better endpoint than the historical alternatives “delayed cerebral ischemia” and “symptomatic vasospasm”, and this endpoint has been suggested by recent guidelines and consensus panels [20, 21]. For consistency throughout the cohort, only CT volumes corresponding to the first detected infarction were measured, using Analyze software (AnalyzeDirect, Inc., Overland Park, KS) software, as previously described [22, 23]. Since this analysis concerns patients evaluated at 14 days from symptom onset, those with infarcts detected beyond 14 days were considered to have no infarction.
Non-normally distributed variables were compared with the Mann–Whitney U test (2 groups) or Kruskal–Wallis H test (>2 groups), the Chi square test with Yates continuity correction, Fisher’s Exact Test or correlated with Spearman’s rho as appropriate. Data are presented as mean ± SD (for normally distributed variables) or median [Q1–Q3] (for non-normally distributed variables). Ordinal regression was performed to evaluate the relationship between patient characteristics and outcomes [24, 25], using mRS of 6 (dead) as a reference category. Proportionate odds assumptions were assessed with the test of parallel lines, and overall model fit was assessed by the −2 log-likelihood test. A multivariate ordinal regression model was constructed using infarct volume along with age and neurological grade as prespecified covariates [26, 27]. To assess the contribution of shifts in goals of care, a term for withdrawal of life support was included in the multivariate model. Using α = 0.05, statistical calculations were made with standard commercial software (SPSS, version 20; SPSS Inc., Chicago, IL).
The study was approved by the Institutional Review Board. Written informed consent was obtained from the patient or a legally authorized representative except when the patient died in the hospital or no legally authorized representative could be located for an incapacitated patient, in which case the Institutional Review Board approved a waiver of consent.
Results
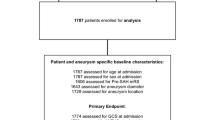
Of 272 patients admitted during the study period, 66 patients with SAH had severe neurological injury at 14 days (Table 1). More than half of those with severe neurological injury were WFNS grade 4 or 5 (34, 51.6 %) or had thick (i.e., completely filling at least one cistern or fissure) subarachnoid blood (55, 83.3 %) on admission. Among the 193 patients admitted with WFNS grades of 1 or 2, compared to those who were not, those who were severely neurologically injured at 14 days (n = 29, 15 %) were more likely to have received ventriculostomies (75.9 vs. 46.3 %, P = 0.006), developed pneumonia (27.6 vs. 3 %, P < 0.001), or to have developed low blood pressure requiring treatment with pressors (13.8 vs. 2.4 %, P = 0.019). During the first 14 days after hemorrhage, they also had fewer ventilator-free days (7 [4.5–10] vs. 14 [14–14], P < 0.001) and more days with fever (7 [4.5–9.5] vs. 2 [0–6], P < 0.001). Among the 69 patients admitted with radiographic grades of 2 or lower, 11 (15.9 %) were severely injured at 14 days. Compared to those who were not, severely injured patients were more likely to have received ventriculostomies (72.7 vs. 32.8 %, P = 0.019) or developed pneumonia (36.4 vs. 1.7 %, P = 0.002). They also had fewer ventilator-free days (4 [0–9] vs. 14 [14–14], P < 0.001) and more days febrile (7 [3–9] vs. 1 [0–4.25], P = 0.004). By day 14, 38 (57.6 %) patients developed radiographic infarcts, detected at a median of 3.5 [1.5–5.3] days from hemorrhage. Infarcts had a median volume of 9.4 [2.7–45.1] mL.
Three-month outcomes were known in 61 (92.4 %) patients, of whom 9 (14.8 %) died at a mean of 32.8 (±22.9) days from hemorrhage (Fig. 1). The causes of death included withdrawal of life support (n = 5), cardiac arrest (n = 1), and other/unknown causes in a non-healthcare setting (n = 3). Death at 3 months was associated with larger infarct volumes (20.4 [4.55–112.2] vs. 0.85 [0–8] mL, P = 0.02). The median mRS score was 4 [3–5] (moderately severe disability), while 20 (32.8 %) patients recovered to independence (mRS 0–3).Their characteristics are presented in Table 2.

Cerebral infarction volume stratified by 3-month mRS Horizontal lines represent medians, boxes represent Q1 and Q3, and whiskers represent the 5th and 95th percentiles. Larger volumes of infarction were related to worse outcome (see text)
In univariate ordinal regression, larger infarct volume was related to higher (worse) 3-month mRS score (OR 1.01 per mL of infarction, 95 % CI 1.00–1.02, P = 0.041). Neither infarct volume in specific vascular territories (e.g., middle cerebral artery; all P > 0.1) nor time to infarct detection (P = 0.52) were associated with outcome. In the prespecified multivariate ordinal regression, larger infarct volumes were associated with higher (worse) 3-month mRS scores (OR 1.01 per mL of infarction, 95 % CI 1.00–1.03, P = 0.01) independently of age, WFNS grade, and withdrawal of care. Infarct volume remained a significant predictor of outcome when aneurysmal rebleeding, external ventricular drain placement, and time to infarct detection were each forced into the model.
Discussion
These results demonstrate that, in patients who are severely neurologically disabled at 14 days following SAH, including those who were admitted with a good clinical grade but subsequently deteriorated, recovery to functional independence occurs in a substantial proportion of patients, and larger infarct volumes are associated with worse outcomes at 3 months. This association remained even after accounting for age, admission grade, and withdrawal of life support.
Current prognostic schemes for SAH primarily consider disease severity and patient characteristics present on admission [26]. However, events that occur during hospitalization, such as aneurysmal rebleeding or medical complications, further modify prognosis [26, 28]. For critically ill patients, accounting for hospital complications allows more accurate prediction of outcome than considering admission characteristics alone [29]. This is illustrated by our finding that even in patients with good clinical or radiographic grades on admission, medical complications are associated with disability at 14 days, and approximately half of these disabled patients remain disabled at 3 months.
Cerebral infarcts develop during hospitalization in 40–54 % of SAH patients and are independently associated with outcomes [6–9, 30]. Historically, these have been identified dichotomously, as either present or absent. This strategy may overestimate the consequences of small infarctions and underestimate the impact of larger ones [8]. We propose that considering infarct volume is a more biologically relevant way to assess the impact of RCI on outcomes. Thus, when assessed at 14 days, when planning for long-term care (e.g., placement of tracheostomy or feeding tubes) becomes a more immediate consideration, infarct volume may be a useful late measure for predicting recovery in severely disabled patients [26].
In addition to infarct volume, we sought to control for age and admission neurological grade, because these are robust predictors of outcome in patients with SAH [26, 27]. Even though our patients with 3-month mRS 4–6 were older than those with mRS 0–3, infarct volume remained an independent predictor of long-term outcome. While aneurysmal rebleeding and hydrocephalus have also been associated with long-term outcomes in poor-grade patients [31], addition of these terms to the model did not change the predictive value of infarct volume, probably because rebleeding was very uncommon, while placement of a ventricular drain was routine in this cohort. We did not include radiographic grade in our analysis because its importance is mainly as a predictor of infarction or “vasospasm”, and as noted above, we instead measured infarction directly [13, 32].
The phenomenon of self-fulfilling prophecy, where severe neurological injury leads to expectations of poor outcome and subsequent withdrawal of care, has been well-documented in intracerebral hemorrhage [33, 34], but there are few data on this phenomenon after SAH. In our sample of severely disabled patients, withdrawal of life support was uncommon and did not significantly influence the results. This may reflect a predisposition not to “give up on” a patient who has already received medical interventions and intensive care [35], or be a consequence of the paucity of published prognostic data directly applicable to these patients with which to guide decision making. Clinicians may make subjective judgments about likely outcomes based on a qualitative interpretation of the CT, but unlike hematoma size in intracerebral hemorrhage, infarct volume has not been calculated routinely following SAH. Our methods of measuring infarct volume with validated techniques may support such judgments and improve their accuracy. Nevertheless, the potential for self-fulfilling prophecies warrants caution when prognosticating after SAH.
Several limitations deserve mention. First, we routinely performed CT scans on admission and postoperatively, with other imaging obtained as clinically indicated. Using such a strategy might create detection bias if patients in worse clinical condition receive more frequent imaging and had infarcts detected earlier, but we found no relationship between outcome and time to infarct detection, and infarct volume remained predictive of outcome independently of time to detection. Second, if scans were instead obtained at regular or later intervals, such as at 6 weeks from hemorrhage [6], the number of infarcts and their total volume may have been greater. Such data might be less useful for planning the end of an acute hospitalization, and since outcomes at 1 month are similar to those at 3 months [36], an evaluation as late as 6 weeks might be considered an ascertainment of medium-term outcome rather than an assessment of prognosis. Third, routine MRI scans might detect infarcts earlier than CT, with volumes below the resolution of CT, or in locations that are difficult to assess by CT (e.g., posterior fossa) [37–39]. These may further refine the relationship between infarction and outcome, but since CT is widely available and typically obtained more frequently, infarct volume on CT is generalizable across institutions. Fourth, this investigation was carried out in a single center, although the techniques for CT acquisition, determination of infarct volume, and clinical grading should not vary substantially between institutions.
Strengths of our data include prospective identification of patients, volumetric analysis of CT scans with a validated method, and assessment of outcomes at multiple time points with validated clinical assessments.
Conclusions
We found that infarct volume was associated with functional outcomes at 3 months in patients who were severely neurologically disabled at 14 days after SAH onset, independent of initial disease severity. In this cohort, substantial recovery at 3 months was common and associated with a low volume of cerebral infarction. Compared to patients with intracerebral hemorrhage, withdrawal of life support was uncommon. These data may assist clinicians in establishing prognosis and setting reasonable expectations for discharge planning when patients are likely to require extended medical care following SAH.
References
Nieuwkamp DJ, Setz LE, Algra A, Linn FH, de Rooij NK, Rinkel GJ. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol. 2009;8:635–42.
Lovelock CE, Rinkel GJ, Rothwell PM. Time trends in outcome of subarachnoid hemorrhage. Population-based study and systematic review. Neurology. 2010;74:1494–501.
Harrison N, Wilson FC. Independent living following a ‘Do Not Resuscitate’ order after subarachnoid haemorrhage. Disabil Rehabil. 2007;29:347–52.
Greebe P, Rinkel GJ, Algra A. Long-term outcome of patients discharged to a nursing home after aneurysmal subarachnoid hemorrhage. Arch Phys Med Rehabil. 2010;91:247–51.
Lloyd CB, Nietert PJ, Silvestri GA. Intensive care decision making in the seriously ill and elderly. Crit Care Med. 2004;32:649–54.
Vergouwen MD, Ilodigwe D, Macdonald RL. Cerebral infarction after subarachnoid hemorrhage contributes to poor outcome by vasospasm-dependent and -independent effects. Stroke. 2011;42:924–9.
Vergouwen MD, Etminan N, Ilodigwe D, Macdonald RL. Lower incidence of cerebral infarction correlates with improved functional outcome after aneurysmal subarachnoid hemorrhage. J Cereb Blood Flow Metab. 2011;31:1545–53.
Naidech AM, Bendok BR, Bassin SL, Bernstein RA, Batjer HH, Bleck TP. Classification of cerebral infarction after subarachnoid hemorrhage impacts outcome. Neurosurgery. 2009;64:1052–8.
Schmidt JM, Wartenberg KE, Fernandez A, et al. Frequency and clinical impact of asymptomatic cerebral infarction due to vasospasm after subarachnoid hemorrhage. J Neurosurg. 2008;109:1052–9.
Vora NA, Shook SJ, Schumacher HC, et al. A 5-item scale to predict stroke outcome after cortical middle cerebral artery territory infarction: validation from results of the diffusion and perfusion imaging evaluation for understanding stroke evolution (DEFUSE) Study. Stroke. 2011;42:645–9.
Anonymous Report of World Federation of Neurological Surgeons Committee on a Universal Subarachnoid Hemorrhage Grading Scale. J Neurosurg 1988;68:985–986.
Brott T, Adams HP Jr, Olinger CP, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. 1989;20:864–70.
Claassen J, Bernardini GL, Kreiter K, et al. Effect of cisternal and ventricular blood on risk of delayed cerebral ischemia after subarachnoid hemorrhage: the fisher scale revisited. Stroke. 2001;32:2012–20.
Banks JL, Marotta CA. Outcomes validity and reliability of the modified Rankin scale: implications for stroke clinical trials: a literature review and synthesis. Stroke. 2007;38:1091–6.
Saver JL, Filip B, Hamilton S, et al. Improving the reliability of stroke disability grading in clinical trials and clinical practice: the Rankin Focused Assessment (RFA). Stroke. 2010;41:992–5.
Anonymous Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581–7.
Briggs DE, Felberg RA, Malkoff MD, Bratina P, Grotta JC. Should mild or moderate stroke patients be admitted to an intensive care unit? Stroke. 2001;32:871–6.
Tseng MY, Czosnyka M, Richards H, Pickard JD, Kirkpatrick PJ. Effects of acute treatment with pravastatin on cerebral vasospasm, autoregulation, and delayed ischemic deficits after aneurysmal subarachnoid hemorrhage: a phase II randomized placebo-controlled trial. Stroke. 2005;36:1627–32.
Sen J, Belli A, Albon H, Morgan L, Petzold A, Kitchen N. Triple-H therapy in the management of aneurysmal subarachnoid haemorrhage. Lancet Neurol. 2003;2:614–21.
Vergouwen MD, Vermeulen M, van Gijn J, et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke. 2010;41:2391–5.
Diringer MN, Bleck TP, Claude Hemphill J, et al. Critical care management of patients following aneurysmal subarachnoid hemorrhage: recommendations from the Neurocritical Care Society’s Multidisciplinary Consensus Conference. Neurocrit Care. 2011;15:211–40.
Naidech AM, Jovanovic B, Liebling S, et al. Reduced platelet activity is associated with early clot growth and worse 3 months outcome after intracerebral hemorrhage. Stroke. 2009;40:2398–401.
Naidech AM, Rosenberg NF, Maas MB, Bendok BR, Batjer HH, Nemeth AJ. Predictors of hemorrhage volume and disability after perimesencephalic subarachnoid hemorrhage. Neurology. 2012;78:811–5.
The Optimising Analysis of Stroke Trials (OAST) Collaboration. Can we improve the statistical analysis of stroke trials? Statistical reanalysis of functional outcomes in stroke trials. Stroke. 2007;38:1911–5.
Bath PM, Geeganage C, Gray LJ, Collier T, Pocock S. Use of ordinal outcomes in vascular prevention trials: comparison with binary outcomes in published trials. Stroke. 2008;39:2817–23.
Connolly ES, Rabinstein AA, Carhuapoma JR, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43:1711–37.
Hanel RA, Xavier AR, Mohammad Y, Kirmani JF, Yahia AM, Qureshi AI. Outcome following intracerebral hemorrhage and subarachnoid hemorrhage. Neurol Res. 2002;24(1):58–62.
Wartenberg KE, Schmidt JM, Claassen J, et al. Impact of medical complications on outcome after subarachnoid hemorrhage. Crit Care Med. 2006;34:617–23.
Minne L, Abu-Hanna A, de Jonge E. Evaluation of SOFA-based models for predicting mortality in the ICU: a systematic review. Crit Care. 2008;12:R161.
Rabinstein AA, Friedman JA, Weigand SD, et al. Predictors of cerebral infarction in aneurysmal subarachnoid hemorrhage. Stroke. 2004;35:1862–6.
van den Berg R, Foumani M, Schröder RD, et al. Predictors of outcome in World Federation of Neurologic Surgeons grade V aneurysmal subarachnoid hemorrhage patients. Crit Care Med. 2011;39:2722–7.
Kramer AH, Hehir M, Nathan B, et al. A comparison of 3 radiographic scales for the prediction of delayed ischemia and prognosis following subarachnoid hemorrhage. J Neurosurg. 2008;109:199–207.
Becker KJ, Baxter AB, Cohen WA, et al. Withdrawal of support in intracerebral hemorrhage may lead to self-fulfilling prophecies. Neurology. 2001;56:766–72.
Naidech AM, Bernstein RA, Bassin SL, et al. How patients die after intracerebral hemorrhage. Neurocrit Care. 2009;11:45–9.
Schwarze ML, Bradley CT, Brasel KJ. Surgical”buy-i”: the contractual relationship between surgeons and patients that influences decisions regarding life-supporting therapy. Crit Care Med. 2010;38:843–8.
Ovbiagele B, Saver JL. Day-90 acute ischemic stroke outcomes can be derived from early functional activity level. Cerebrovasc Dis. 2010;29:50–6.
Wartenberg KE, Sheth SJ, Michael Schmidt J, et al. Acute ischemic injury on diffusion-weighted magnetic resonance imaging after poor grade subarachnoid hemorrhage. Neurocrit Care. 2011;14:407–15.
Weidauer S, Lanfermann H, Raabe A, Zanella F, Seifert V, Beck J. Impairment of cerebral perfusion and infarct patterns attributable to vasospasm after aneurysmal subarachnoid hemorrhage: a prospective MRI and DSA study. Stroke. 2007;38:1831–6.
Shimoda M, Takeuchi M, Tominaga J, Oda S, Kumasaka A, Tsugane R. Asymptomatic versus symptomatic infarcts from vasospasm in patients with subarachnoid hemorrhage: serial magnetic resonance imaging. Neurosurgery. 2001;49:1341–8.
Acknowledgments
This work was departmentally funded. The infrastructure for automated data retrieval was funded in part by National Institutes of Health through a Grant to Northwestern University’s Clinical and Translational Sciences (NUCATS) UL1RR025741. Dr. Rosenberg received support from the Goldberg Charitable Trust of Northwestern Memorial Hospital to present these data in abstract form at the American Academy of Neurology Annual Meeting.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rosenberg, N.F., Liebling, S.M., Kosteva, A.R. et al. Infarct Volume Predicts Delayed Recovery in Patients with Subarachnoid Hemorrhage and Severe Neurological Deficits. Neurocrit Care 19, 293–298 (2013). https://doi.org/10.1007/s12028-013-9869-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-013-9869-3