
Abstract
Background
Total knee arthroplasty (TKA) and related interventions such as revision TKA and the treatment of infected TKAs are commonly performed procedures. Hospital readmission rates are used to measure hospital performance, but risk factors (both medical and surgical) for readmission after TKA, revision TKA, and treatment for the infected TKA have not been well characterized.
Questions/purposes
We measured (1) the unplanned hospital readmission rate in primary TKA and revision TKA, including antibiotic-spacer staged revision TKA to treat infection. We also evaluated (2) the medical and surgical causes of readmission and (3) risk factors associated with unplanned hospital readmission.
Methods
This retrospective cohort study included a total of 1408 patients (1032 primary TKAs, 262 revision TKAs, 113 revision of infected TKAs) from one institution. All hospital readmissions within 90 days of discharge were evaluated for timing and cause. Diagnoses at readmission were categorized as surgical or medical. Readmission risk was assessed using a Cox proportional hazards model that incorporated patient demographics and medical comorbidities.
Results
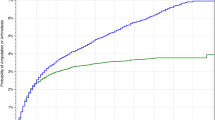
The unplanned readmission rate for the entire cohort was 4% at 30 days and 8% at 90 days. At 90 days postoperatively, revision of an infected TKA had the highest readmission rate, followed by revision TKA, with primary TKA having the lowest rate. Approximately three-fourths of readmissions were the result of surgical causes, mostly infection, arthrofibrosis, and cellulitis, whereas the remainder of readmissions were the result of medical causes. Procedure type (primary TKA versus revision TKA or staged treatment for infected TKA), hospital stay more than 5 days, discharge destination, and a fluid/electrolyte abnormality were each associated with risk of unplanned readmission.
Conclusions
Patients having revision TKA, whether for infection or other causes, are more likely to have an unplanned readmission to the hospital than are patients having primary TKA. When assessing hospital performance for TKA, it is important to distinguish among these surgical procedures.
Level of Evidence
Level III, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.

Similar content being viewed by others

References
Bozic KJ, Chiu V. Emerging ideas: shared decision making in patients with osteoarthritis of the hip and knee. Clin Orthop Relat Res. 2011;469:2081–2085.
Brown NM, Sheth NP, Davis K, Berend ME, Lombardi AV, Berend KR, Della Valle CJ. Total knee arthroplasty has higher postoperative morbidity than unicompartmental knee arthroplasty: a multicenter analysis. J Arthroplasty. 2012;27(Suppl):86–90.
Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991–2010. JAMA. 2012;308:1227–1236.
Crowe J, Henderson J. Pre-arthroplasty rehabilitation is effective in reducing hospital stay. Can J Occup Ther. 2003;70:88–96.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
Huddleston JI, Maloney WJ, Wang Y, Verzier N, Hunt DR, Herndon JH. Adverse events after total knee arthroplasty: a national Medicare study. J Arthroplasty. 2009;24:95–100.
Iezzoni LI, Ash AS, Shwartz M, Landon BE, Mackiernan YD. Predicting in-hospital deaths from coronary artery bypass graft surgery. Do different severity measures give different predictions? Med Care. 1998;36:28–39.
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428.
Jones S, Alnaib M, Kokkinakis M, Wilkinson M, St Clair Gibson A, Kader D. Pre-operative patient education reduces length of stay after knee joint arthroplasty. Ann R Coll Surg Engl. 2011;93:71–75.
Joynt KE, Jha AK. Characteristics of hospitals receiving penalties under the Hospital Readmissions Reduction Program. JAMA. 2013;309:342–343.
Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675–681.
Kim J, Nelson CL, Lotke PA. Stiffness after total knee arthroplasty. Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am. 2004;86:1479–1484.
Kurtz SM, Lau E, Ong K, Zhao K, Kelly M, Bozic KJ. Future young patient demand for primary and revision joint replacement: national projections from 2010 to 2030. Clin Orthop Relat Res. 2009;467:2606–2612.
Lavernia CJ, Villa JM, Iacobelli DA. Readmission rates in the state of Florida: a reflection of quality? Clin Orthop Relat Res. 2013 Feb 20 [Epub ahead of print].
Losina E, Walensky RP, Kessler CL, Emrani PS, Reichmann WM, Wright EA, Holt HL, Solomon DH, Yelin E, Paltiel AD, Katz JN (2009) Cost-effectiveness of total knee arthroplasty in the United States: patient risk and hospital volume. Arch Intern Med. 169:1113–1121; discussion 1121–1122.
Mahomed NN, Barrett JA, Katz JN, Phillips CB, Losina E, Lew RA, Guadagnoli E, Harris WH, Poss R, Baron JA. Rates and outcomes of primary and revision total hip replacement in the United States medicare population. J Bone Joint Surg Am. 2003;85:27–32.
Marshall DA, Wasylak T, Khong H, Parker RD, Faris PD, Frank C. Measuring the value of total hip and knee arthroplasty: considering costs over the continuum of care. Clin Orthop Relat Res. 2012;470:1065–1072.
Medicare Payment Advisory Commission (MedPAC). Medicare Payment Policy. Washington, DC, USA: Medicare Payment Advisory Commission (MedPAC); 2012.
Pulido L, Parvizi J, Macgibeny M, Sharkey PF, Purtill JJ, Rothman RH, Hozack WJ. In hospital complications after total joint arthroplasty. J Arthroplasty. 2008;23:139–145.
Rathore SS, Foody JM, Wang Y, Smith GL, Herrin J, Masoudi FA, Wolfe P, Havranek EP, Ordin DL, Krumholz HM. Race, quality of care, and outcomes of elderly patients hospitalized with heart failure. JAMA. 2003;289:2517–2524.
Stranges E, Russo CA, Friedman B. Procedures With the Most Rapidly Increasing Hospital Costs, 2004–2007. Rockville, MD, USA: Agency for Healthcare Research and Quality; December 2009.
Weingarten S, Riedinger MS, Sandhu M, Bowers C, Ellrodt AG, Nunn C, Hobson P, Greengold N. Can practice guidelines safely reduce hospital length of stay? Results from a multicenter interventional study. Am J Med. 1998;105:33–40.
Wier LM, Barrett M, Steiner C, Jiang HJ. All-cause Readmissions by Payer and Age, 2008: Statistical Brief #115. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville, MD, USA: Healthcare Cost and Utilization Project (HCUP); 2006.
Acknowledgments
We thank Vanessa Chan MPH, for her help in preparing this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (TPV) certifies that he has received or may receive payments or benefits, during the study period, an amount in excess of USD 10,000 from DePuy Orthopaedics, Inc (Warsaw, IN, USA). The institution of one or more of the authors (KJB) has received, during the study period, funding from the Orthopaedic Research and Education Foundation (Rosemont, IL, USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that institution where the work was performed approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
About this article
Cite this article
Schairer, W.W., Vail, T.P. & Bozic, K.J. What Are the Rates and Causes of Hospital Readmission After Total Knee Arthroplasty?. Clin Orthop Relat Res 472, 181–187 (2014). https://doi.org/10.1007/s11999-013-3030-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-013-3030-7