
Abstract
Introduction
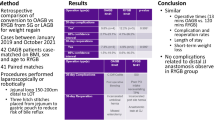
In bariatric surgery, new surgical techniques are continually being developed. The one anastomosis gastric bypass (OAGB) has become increasingly common since 2001. However, some patients experience bile reflux or excessive weight loss. This study aimed to assess a new bariatric procedure designed to avoid some of the drawbacks of conventional OAGB.
Material and Methods
To lower the complication rate and pathophysiological impact after OAGB, we performed an omega loop gastroileal bypass (OLGIBP/SAGI) with a 300-cm common limb. We compared this technique with OAGB.
Results
Seventeen patients underwent OLGIBP and 23 underwent OAGB. Mean operative time was 108 min for OLGIBP vs 103 min for OAGB. The mean hospital length of stay was 3 days (1 to 7). No complications related to the gastroenterostomy occurred. At 3 years, among OAGB patients, there were 5 (21.7%) cases of bile reflux including 2 (8.7%) requiring a revision to Roux-en-Y gastric bypass. Among OLGIBP patients, there were 3 (17.6%) cases of bile reflux 1 (5.9%) requiring a revision to Roux-en-Y gastric bypass. There was no albumin deficiency. At 3 years, % of total weight loss (TWL) was 43.6 + − 6.2 in the OAGB group vs 48.2 + − 7.4 in the OLGIBP group.
Conclusions
The bariatric and metabolic outcomes of OLGIBP are expected to be similar to those of OAGB. The OLGIBP technique should reduce the risks of malnutrition and bile reflux. The two techniques can be safely performed and offer alternatives in bariatric surgery.
Similar content being viewed by others


References
Rutledge R. The mini-gastric bypass: experience with the first 1,274 cases. Obes Surg juin. 2001;11(3):276–80.
Angrisani L, Santonicola A, Iovino P, et al. IFSO Worldwide Survey 2016: primary, endoluminal, and revisional procedures. Obes Surg. 2018;28(12):3783–94.
Lafarge J-C. Traitement chirurgical de l’obésité sévère et massive par court-circuit (bypass) gastrojéjunal avec anse en oméga. Haute Autorité de Santé. 2019;71
Ruiz-Tovar J, Carbajo MA, Jimenez JM, et al. Are there ideal small bowel limb lengths for one-anastomosis gastric bypass (OAGB) to obtain optimal weight loss and remission of comorbidities with minimal nutritional deficiencies? World J Surg mars. 2020;44(3):855–62.
Caiazzo R, Torres F, Sterkers A, et al. Complications du bypass gastrique. In: Complications de la chirurgie bariatrique. Montrouge: John Libbey Eurotext; 2016. p. 97. (Monographies de l’association française de chirurgie)
Tacchino RM. Bowel length: measurement, predictors, and impact on bariatric and metabolic surgery. Surg Obes Relat Dis avr. 2015;11(2):328–34.
Scolapio JS. Current update of short-bowel syndrome. Curr Opin Gastroenterol. 2004;20(2):143–5.
Mahawar KK, Himpens J, Shikora SA, et al. The first consensus statement on one anastomosis/mini gastric bypass (OAGB/MGB) using a modified Delphi approach. Obes Surg. 2018;28(2):303–12.
Fisher BL, Buchwald H, Clark W, et al. Mini-gastric bypass controversy. Obes Surg. 2001;11(6):773.
Bruzzi M, Duboc H, Gronnier C, et al. Long-term evaluation of biliary reflux after experimental one-anastomosis gastric bypass in rats. Obes Surg. 2017;27(4):1119–22.
Sánchez-Pernaute A, Herrera MAR, Pérez-Aguirre ME, et al. Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). One to three-year follow-up. Obes Surg déc. 2010;20(12):1720–6.
Mitzman B, Cottam D, Goriparthi R, et al. Stomach intestinal pylorus sparing (SIPS) surgery for morbid obesity: retrospective analyses of our preliminary experience. Obes Surg. 2016;26(9):2098–104.
Russell DW. Fifty years of advances in bile acid synthesis and metabolism. J Lipid Res. 2009;50 Suppl:S120–125.
Di Ciaula A, Garruti G, Lunardi Baccetto R, et al. Bile acid physiology. Ann Hepatol. 2017;16(Suppl. 1: s3–105):s4–14.
Reuben A. The biliary cycle of Moritz Schiff. Hepatology. 2005;42(2):500–5.
Dawson PA. Role of the intestinal bile acid transporters in bile acid and drug disposition. Drug Transporters. 2011:169–203.
De Luca M, Himpens J, Angrisani L, et al. A new concept in bariatric surgery. Single anastomosis gastro-ileal (SAGI): technical details and preliminary results. Obes Surg. 2017;27(1):143–7.
Bolckmans R, Arman G, Himpens J. Efficiency and risks of laparoscopic conversion of omega anastomosis gastric bypass to Roux-en-Y gastric bypass. Surg Endosc. 2019;33(8):2572–82.
Robert M, Espalieu P, Pelascini E, et al. Efficacy and safety of one anastomosis gastric bypass versus Roux-en-Y gastric bypass for obesity (YOMEGA): a multicentre, randomised, open-label, non-inferiority trial. Lancet. 2019;393(10178):1299–309.
Rutledge R, Walsh TR. Continued excellent results with the mini-gastric bypass: six-year study in 2,410 patients. Obes Surg. 2005;15(9):1304–8.
Noun R, Skaff J, Riachi E, et al. One thousand consecutive mini-gastric bypass: short- and long-term outcome. Obes Surg. 2012;22(5):697–703.
Ahuja A, Tantia O, Goyal G, et al. MGB-OAGB: effect of biliopancreatic limb length on nutritional deficiency, weight loss, and comorbidity resolution. Obes Surg. 2018;28(11):3439–45.
Komaei I, Sarra F, Lazzara C, et al. One anastomosis gastric bypass–mini gastric bypass with tailored biliopancreatic limb length formula relative to small bowel length: preliminary results. Obes Surg. 2019;29(9):3062–70.
Nabil TM, Khalil AH, Mikhail S, et al. Conventional versus distal laparoscopic one-anastomosis gastric bypass: a randomized controlled trial with 1-year follow-up. Obes Surg. 2019;29(10):3103–10.
Soong T-C, Almalki OM, Lee W-J, et al. Measuring the small bowel length may decrease the incidence of malnutrition after laparoscopic one-anastomosis gastric bypass with tailored bypass limb. Surg Obes Relat Dis. 2019;15(10):1712–8.
Abellan I, Luján J, Frutos MD, et al. The influence of the percentage of the common limb in weight loss and nutritional alterations after laparoscopic gastric bypass. Surg Obes Relat Dis. 2014;10(5):829–33.
Scopinaro N, Gianetta E, Civalleri D, et al. Bilio-pancreatic bypass for obesity: II. Initial experience in man. Br J Surg. 1979;66(9):618–20.
Neichoy BT, Schniederjan B, Cottam DR, et al. Stomach intestinal pylorus-sparing surgery for morbid obesity. JSLS. 2018;22(1)
Brown WA, Ooi G, Higa K, et al. IFSO-appointed task force reviewing the literature on SADI-S/OADS. Single anastomosis duodenal-Ileal bypass with sleeve gastrectomy/one anastomosis duodenal switch (SADI-S/OADS) IFSO position statement. Obes Surg. 2018;28(5):1207–16.
Grueneberger JM, Karcz-Socha I, Marjanovic G, et al. Pylorus preserving loop duodeno-enterostomy with sleeve gastrectomy - preliminary results. BMC Surg. 2014;14:20.
Obeid A, Long J, Kakade M, et al. Laparoscopic Roux-en-Y gastric bypass: long term clinical outcomes. Surg Endosc. 2012;26(12):3515–20.
Swartz DE, Mobley E, Felix EL. Bile reflux after Roux-en-Y gastric bypass: an unrecognized cause of postoperative pain. Surgery for Obesity and Related Diseases. 2009;5(1):27–30.
Debs T, Petrucciani N, Ben Amor I, et al. Laparoscopic conversion of failed sleeve gastrectomy to single anastomosis gastro ileal bypass (SAGI) (with video). J Visceral Surg. 2019;156(4):358–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Statement of Informed Consent
“Informed consent was obtained from all individual participants included in the study.”
Statement of Human and Animal Rights
“Informed consent was obtained from all individual participants included in the study.”
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kassir, R., Giudicelli, X., Lointier, P. et al. Omega Loop Gastroileal Bypass (OLGIBP/SAGI) Versus One Anastomosis Gastric Bypass (OAGB): Medium-Term Results. OBES SURG 31, 1597–1602 (2021). https://doi.org/10.1007/s11695-020-05165-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-020-05165-0