
Abstract
Background
Enhanced recovery after surgery (ERAS) guidelines, fast-track protocols, and alternative clinical pathways have been widely promoted in a variety of disciplines leading to improved outcomes in post-operative morbidity and length of stay (LOS). This meta-analysis assesses the implications of standardized management protocols in bariatric surgery.
Methods
The PRISMA guidelines were adhered to. Databases were searched with the application of pre-defined inclusion and exclusion criteria. Results were reported as mean differences or pooled odds ratios (OR) with 95% confidence intervals (95% CI). Individual protocols and surgical approaches were assessed through subgroup analysis, and sensitivity analysis of methodological quality was performed.
Results
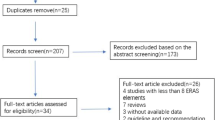
A total of 1536 studies were screened; 13 studies were eventually included for meta-analysis involving a total of 6172 patients. Standardized perioperative techniques were associated with a savings of 19.5 min in operative time (p < 0.01), as well as a LOS which was shortened by 1.5 days (p < 0.01). Pooled post-operative morbidity rates also favored enhanced recovery care protocols (OR 0.7%, 95% CI 0.6–0.9%, p < 0.01).
Conclusion
Bariatric surgery involves a complex cohort of patients who require high-quality evidence-based care to improve outcomes. Consensus guidelines on the feasibility of ERAS and alternative clinical pathways are required in the setting of bariatric surgery.



Similar content being viewed by others


References
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. Jama.2014;311(8):806–14. https://doi.org/10.1001/jama.2014.732.
Stevens GA, Singh GM, Lu Y, Danaei G, Lin JK, Finucane MM et al. National, regional, and global trends in adult overweight and obesity prevalences. Population health metrics. 2012;10(1):22.
Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2011. Obesity surgery. 2013;23(4):427–36.
Santry HP, Gillen DL, Lauderdale DS. Trends in bariatric surgical procedures. Jama. 2005;294(15):1909–17.
Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. British journal of anaesthesia. 1997;78(5):606–17.
Coolsen MM, Wong-Lun-Hing EM, Dam RM, Wilt AA, Slim K, Lassen K et al. A systematic review of outcomes in patients undergoing liver surgery in an enhanced recovery after surgery pathways. HPB. 2013;15(4):245–51.
Varadhan KK, Neal KR, Dejong CH, Fearon KC, Ljungqvist O, Lobo DN. The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: a meta-analysis of randomized controlled trials. Clinical nutrition. 2010;29(4):434–40.
Arsalani-Zadeh R, ElFadl D, Yassin N, MacFie J. Evidence-based review of enhancing postoperative recovery after breast surgery. British Journal of Surgery. 2011;98(2):181–96.
Singh PM, Panwar R, Borle A, Goudra B, Trikha A, van Wagensveld BA et al. Efficiency and safety effects of applying ERAS protocols to bariatric surgery: a systematic review with meta-analysis and trial sequential analysis of evidence. Obesity surgery. 2017:1–13.
Panella M, Marchisio S, Di Stanislao F. Reducing clinical variations with clinical pathways: do pathways work? International Journal for Quality in Health Care. 2003;15(6):509–21.
Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Annals of surgery. 2008;248(2):189–98.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ journal of surgery. 2003;73(9):712–6.
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled clinical trials. 1996;17(1):1–12.
Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC medical research methodology. 2005;5(1):13.
Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons; 2011.
Campillo-Soto Á, Martín-Lorenzo JG, Lirón-Ruíz R, Torralba-Martínez JA, Bento-Gerard M, Flores-Pastor B et al. Evaluation of the clinical pathway for laparoscopic bariatric surgery. Obesity surgery. 2008;18(4):395–400.
Cooney RN, Bryant P, Haluck R, Rodgers M, Lowery M. The impact of a clinical pathway for gastric bypass surgery on resource utilization. Journal of Surgical Research. 2001;98(2):97–101.
Ronellenfitsch U, Schwarzbach M, Kring A, Kienle P, Post S, Hasenberg T. The effect of clinical pathways for bariatric surgery on perioperative quality of care. Obesity Surgery. 2012;22(5):732–9.
van Wezenbeek MR, Pouwels S, Buise MP, Smulders JF, Nienhuijs SW, van Montfort G. Conventional versus fast track anaesthesia in an unselected group of patients undergoing revisional bariatric surgery. International Journal of Surgery Open. 2015;1:22–7.
Petrick AT, Still CD, Wood CG, Vitunac MA, Plank M, McGrail L et al. Feasibility and impact of an evidence-based program for gastric bypass surgery. Journal of the American College of Surgeons. 2015;220(5):855–62.
Pimenta GP, Capellan DA, de Aguilar-Nascimento JE. Sleeve gastrectomy with or without a multimodal perioperative care. A randomized pilot study. Obesity surgery. 2015;25(9):1639–46.
Dogan K, Kraaij L, Aarts EO, Koehestanie P, Hammink E, van Laarhoven, CJHM et al. Fast-Track Bariatric Surgery Improves Perioperative Care and Logistics Compared to Conventional Care. Obesity Surgery. 2014.
Geubbels N, Bruin SC, Acherman YIZ, VandeLaar AWJM, Hoen MB, De Brauw LM. Fast track care for gastric bypass patients decreases length of stay without increasing complications in an unselected patient cohort. Obesity Surgery. 2014;24(3):390–6.
Simonelli V, Goergen M, Orlando GG, Arru L, Zolotas CA, Geeroms M et al. Fast-track in bariatric and metabolic surgery: feasibility and cost analysis through a matched-cohort study in a single centre. Obesity surgery. 2016;26(8):1970–7.
Mannaerts GH, van Mil SR, Stepaniak PS, Dunkelgrun M, de Quelerij M, Verbrugge SJ et al. Results of Implementing an Enhanced Recovery After Bariatric Surgery (ERABS) Protocol. Obes Surg. 2016;26(2):303–12. https://doi.org/10.1007/s11695-015-1742-3.
Lemanu DP, Singh PP, Berridge K, Burr M, Birch C, Babor R et al. Randomized clinical trial of enhanced recovery versus standard care after laparoscopic sleeve gastrectomy. Br J Surg. 2013;100(4):482–9. https://doi.org/10.1002/bjs.9026.
Barreca M, Renzi C, Tankel J, Shalhoub J, Sengupta N. Is there a role for enhanced recovery after laparoscopic bariatric surgery? Preliminary results from a specialist obesity treatment center. Surgery for Obesity and Related Diseases. 2016;12(1):119–26.
Proczko M, Kaska L, Twardowski P, Stepaniak P. Implementing enhanced recovery after bariatric surgery protocol: a retrospective study. J Anesth. 2016;30(1):170–3. https://doi.org/10.1007/s00540-015-2089-6.
Birkmeyer JD. Progress and challenges in improving surgical outcomes. British Journal of Surgery. 2012;99(11):1467–9. https://doi.org/10.1002/bjs.8933.
Hamilton MA, Cecconi M, Rhodes A. A Systematic Review and Meta-Analysis on the Use of Preemptive Hemodynamic Intervention to Improve Postoperative Outcomes in Moderate and High-Risk Surgical Patients. Anesthesia & Analgesia. 2011;112(6):1392–402. https://doi.org/10.1213/ANE.0b013e3181eeaae5.
Cleveland E, Peirce G, Brown S, Freemyer J, Rice W, Lee L et al. A short-duration restrictive diet reduces visceral adiposity in the morbidly obese surgical patient. The American Journal of Surgery. 2016;212(5):927–30. https://doi.org/10.1016/j.amjsurg.2016.01.040.
Ratti F, Cipriani F, Reineke R, Catena M, Comotti L, Beretta L et al. Impact of ERAS approach and minimally-invasive techniques on outcome of patients undergoing liver surgery for hepatocellular carcinoma. Digestive and Liver Disease. 2016;48(10):1243–8. https://doi.org/10.1016/j.dld.2016.06.032.
Małczak P, Pisarska M, Piotr M, Wysocki M, Budzyński A, Pędziwiatr M. Enhanced recovery after bariatric surgery: systematic review and meta-analysis. Obesity surgery. 2017:1–10.
Hoerger TJ, Zhang P, Segel JE, Kahn HS, Barker LE, Couper S. Cost-Effectiveness of Bariatric Surgery for Severely Obese Adults With Diabetes. Diabetes Care. 2010;33(9):1933–9. https://doi.org/10.2337/dc10-0554.
McCarney R, Warner J, Iliffe S, van Haselen R, Griffin M, Fisher P. The Hawthorne Effect: a randomised, controlled trial. BMC Med Res Methodol. 2007;7:30. https://doi.org/10.1186/1471-2288-7-30.
Thorell A, MacCormick A, Awad S, Reynolds N, Roulin D, Demartines N et al. Guidelines for perioperative care in bariatric surgery: Enhanced Recovery After Surgery (ERAS) society recommendations. World journal of surgery. 2016;40(9):2065–83.
Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Aminian A, Brethauer SA et al. Bariatric Surgery versus Intensive Medical Therapy for Diabetes—5-Year Outcomes. New England Journal of Medicine. 2017;376(7):641–51. https://doi.org/10.1056/NEJMoa1600869.
Grol R, Grimshaw J. From best evidence to best practice: effective implementation of change in patients’ care. The Lancet. 2003;362(9391):1225–30. https://doi.org/10.1016/S0140-6736(03)14546-1.
Polle SW, Wind J, Fuhring JW, Hofland J, Gouma DJ, Bemelman WA. Implementation of a fast-track perioperative care program: what are the difficulties? Digestive surgery. 2007;24(6):441–9.
Kahokehr A, Sammour T, Zargar-Shoshtari K, Thompson L, Hill AG. Implementation of ERAS and how to overcome the barriers. International Journal of Surgery. 2009;7(1):16–9. https://doi.org/10.1016/j.ijsu.2008.11.004.
Schauer PR, Kashyap SR, Wolski K, Brethauer SA, Kirwan JP, Pothier CE et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. The New England journal of medicine. 2012;366(17):1567–76. https://doi.org/10.1056/NEJMoa1200225.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
OSA acquired and analyzed the data and drafted the manuscript.
ACR acquired and analyzed the data and revised the manuscript.
JB and AM revised the manuscript.
WBR conceived and designed the study, revised, and gave final approval to the manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Ahmed, O.S., Rogers, A.C., Bolger, J.C. et al. Meta-Analysis of Enhanced Recovery Protocols in Bariatric Surgery. J Gastrointest Surg 22, 964–972 (2018). https://doi.org/10.1007/s11605-018-3709-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-018-3709-x