
Abstract
Background
Retrospective studies investigating fast track care involve selected patients. This study evaluates the implementation of fast track care in unselected bariatric patients in a high volume teaching hospital in the Netherlands.
Methods
Consecutive patients who underwent a primary laparoscopic gastric bypass in our center were reviewed in the years before (n = 104) and after implementation of fast track care (n = 360). Fast track involved the banning of tubes/catheters, anesthetic management and early ambulation. Primary outcome was the length of stay. Perioperative times, complications (<30 days), readmissions and prolonged length of stay were secondary outcomes.
Results
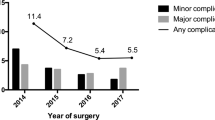
The median length decreased after implementation of fast track (3 days versus 1 day, p < 0.001). Overall complication rate remained stable after implementation of fast track care (17.3 % versus 18.3 %, not significant). Readmission rate did not differ between groups (4.8 % conventional care versus 8.1 % fast track, not significant). More grades I–IVa complications occurred outside the hospital after the implementation of fast track care (24.8 % versus 51.5 %). Lower age (b = 0.118, 95 % CI: 0.002–0.049, p < 0.05) and the implementation of fast track (b = −0.270, 95 % CI: -1.969 to −0.832, p < 0.001) were the only factors that significantly shortened the length of stay.
Conclusions
Patients that received fast track care had a decreased length of stay. Although more complications occurred after discharge in the fast track care group, this did not lead to adverse outcomes. Fast track does enhance recovery and is suitable for unselected patients. Care providers should select their patients for early discharge and pursue a low threshold for readmission.




Similar content being viewed by others


References
Wilmore DW, Kehlet H. Management of patients in fast track surgery. BJM. 2001;322:473–6.
Spanjersberg W, Reurings J. Fast track surgery versus conventional recovery strategies for colorectal surgery. Cochrane Database Syst Rev. 2011;16(2):CD007635. http://onlinelibrary.wiley.com/ doi/10.1002/14651858.CD007635.pub2/full 2011. Accessed 2012 Nov 9.
Vlug MS, Wind J, Hollmann MW, et al. Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery. Ann Surg. 2011;254(6):868–75. http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00000658-201112000-00007. Accessed 2012 May 7.
Lemanu DP, Srinivasa S, Singh PP, et al. Optimizing perioperative care in bariatric surgery patients. Obesity Surg. 2012;22(6):979–90. http://www.springerlink.com/index/ 10.1007/s11695-012-0648-6. Accessed 2012 May 7.
Dindo D, Demartines N, Clavien P-A. Classification of surgical complications. Ann Surg. 2004;240(2):205–13. http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00000658-200408000-00003. Accessed 2013 Sep 17.
Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien–Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–96.
Elliott JA, Patel VM, Kirresh A, et al. Fast-track laparoscopic bariatric surgery: a systematic review. Updates Surg. 2013;65(2):85–94.
McCarty TM, Arnold DT, Lamont JP, et al. Optimizing outcomes in bariatric surgery. Trans Meeting Am Surg Assoc. 2005;123:188–95. http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00153307-200501230-00020. Accessed 2012 May 7.
Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. 2002;183(6):630–41. http://www.ncbi.nlm.nih.gov/pubmed/12095591.
DBC Information System. Dutch Hospital Data. 2012.
White PF, Kehlet H, Neal JM, et al. The role of the anesthesiologist in fast-track surgery: from multimodal analgesia to perioperative medical care. Anesth Anal. 2007;104(6):1380–96. http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00000539-200706000-00013. Accessed 2012 May 4.
Bergland A, Gislason H, Raeder J. Fast-track surgery for bariatric laparoscopic gastric bypass with focus on anaesthesia and peri-operative care. Experience with 500 cases. Acta Anaesthesiol Scand. 2008;52(10):1394–9. doi:10.1111/j.1399-6576.2008.01782.x.
Dumon KR, Murayama KM. Bariatric surgery outcomes. Surg Clin North Am. 2011;91(6):1313–38, x. http://www.ncbi.nlm.nih.gov/pubmed/22054156. Accessed 2012 Oct 29.
Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142(7):547–59.
Parikh MS, Laker S, Weiner M, et al. Objective comparison of complications resulting from laparoscopic bariatric procedures. J Am Coll Surg. 2006;202(2):252–61.
Farrell TM, Haggerty SP, Overby DW, et al. Clinical application of laparoscopic bariatric surgery: an evidence-based review. Surg Endosc. 2009;23(5):930–49.
Jacobsen HJ, Bergland A, Raeder J, et al. High-volume bariatric surgery in a single center: safety, quality, cost-efficacy and teaching aspects in 2,000 consecutive cases. Obesity Surg 2011;22(1):158–66. http://www.springerlink.com/index/ 10.1007/s11695-011-0557-0. Accessed 2012 May 7.
Banka G, Woodard G, Hernandez-Boussard T, Morton JM. Laparoscopic vs open gastric bypass surgery: differences in patient demographics, safety, and outcomes. Arch Surg. 2012;147(6):550–6. doi: 10.1001/archsurg.2012.195.
Haddad A, Tapazoglou N, Singh K, et al. Role of intraoperative esophagogastroenteroscopy in minimizing gastrojejunostomy-related morbidity: experience with 2,311 laparoscopic gastric bypasses with linear stapler anastomosis. Obesity Surg. 2012;22(12)1928–33. http://www.ncbi.nlm.nih.gov/pubmed/22941393. Accessed 2012 Nov 7.
Shikora SA, Kim JJ, Tarnoff ME, et al. Laparoscopic Roux-en-Y gastric bypass: results and learning curve of a high-volume academic program. Arch Surg. 2005;140(4):362–7.
Suter M, Donadini A, Romy S, Demartines N, Giusti V. Laparoscopic Roux-en-Y gastric bypass: significant long-term weight loss, improvement of obesity-related comorbidities and quality of life. Ann Surg 2011;254(2):267–73. http://www.ncbi.nlm.nih.gov/pubmed/21772127. Accessed 2012 Nov 7.
LABS Consortium. Perioperative safety in the longitudinal assessment of bariatric surgery. N Eng J Med. 2009;361(5):445–54.
Omalu BI, Ives DG, Buhari AM, et al. Death rates and causes of death after bariatric surgery for Pennsylvania residents, 1995 to 2004. Arch Surg (Chicago, IL: 1960). 2007;142(10):923–8. discussion 929.
Bamgbade OA, Adeogun BO, Abbas K. Fast-track laparoscopic gastric bypass surgery: outcomes and lessons from a bariatric surgery service in the United Kingdom. Obesity Surg. 2011;22(3):398–402. http://www.springerlink.com/index/ 10.1007/s11695-011-0473-3. Accessed 2012 May 7.
Grantcharov TP, Kehlet H. Laparoscopic gastric surgery in an enhanced recovery programme. Br J Surg. 2010;97(10):1547–51. doi:10.1002/bjs.7184.
Morton JM, DeMaria E, Winegar D, Sherif B, Hutcher N, Blackstone R, et al. PL-110 Is ambulatory laparoscopic Roux-en-Y gastric bypass from the bariatric outcomes longitudinal database (BOLD) associated with higher adverse events? Surg Obes Rel Dis 2011 ;7(3):342–3. http://linkinghub.elsevier.com/retrieve/pii/S1550728911003340. Accessed 2013 Sep 17.
Conflict of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Geubbels, N., Bruin, S.C., Acherman, Y.I.Z. et al. Fast Track Care for Gastric Bypass Patients Decreases Length of Stay Without Increasing Complications in an UnselectedPatient Cohort. OBES SURG 24, 390–396 (2014). https://doi.org/10.1007/s11695-013-1133-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-013-1133-6