
Abstract
Consumer-targeted sleep tracking applications (STA) that run on mobile devices (e.g., smartphones) promise to be useful tools for the individual user. Assisted by built-in and/or external sensors, these apps can analyze sleep data and generate assessment reports for the user on their sleep duration and quality. However, STA also raise ethical questions, for example, on the autonomy of the sleeping person, or potential effects on third parties. Nevertheless, a specific ethical analysis of the use of these technologies is still missing so far. The aim of the current analysis is to identify the characteristics of sleep tracking apps and to explore the specific ethical aspects associated with this form of self-tracking. Firstly, the field of mobile health applications was screened for STA to explore their typical functions and target user groups. Secondly, an ethical analysis was conducted focusing on the three ethical dimensions: (1) medicalization, (2) vulnerability, and (3) relationality. The analysis indicates that these three normative dimensions are decisive for assessing STA and that the ethical profile of this technology varies greatly depending on the respective user group. As the three dimensions medicalization, vulnerability, and relationality play a distinguishing role in the use of STA, they should be especially addressed in responsible development and implementation of STA. In addition, the analysis helps to evaluate the use of STA, in terms of different risks for specific user groups, the sensitive contexts of usage, and potential interference with the intimacy of third parties.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sleep as ‘the other third of life’ (Doug et al., 2013) has been subject to many areas: from art (Kryger, 2019) to psychology, philosophy and history (Espie & Morin, 2012), from medicine (Stuck et al., 2020) to management (Rosekind et al., 2010; Spreitzer & Barne, 2015). In recent years, the topic of sleep has also attracted the interest of technology companies and developers. Consumer-targeted sleep tracking applications (STA) to monitor, measure and/or influence sleep duration and/or quality are among the most downloaded apps for iOS and Android (Choi et al., 2018; SimilarWeb, 2022). Assisted by built-in sensors, additional external sensing devices and scoring algorithms, such applications promise to analyze and score sleep data without human assistance, and generate assessment reports for the user with real-time feedback on their quality of sleep and specific sleep parameters (Van de Water et al., 2011). Although such consumer STA still come with lack in accuracy, for example, regarding wake and deep sleep detection (Fino et al., 2020), they have increasingly proliferated. Given their significant market share, the raising awareness for sleep-hygiene (Irish et al., 2015) and the growing phenomenon of self-tracking (Lupton, 2016), it is not far-fetched that sleep tracking might become the new ‘step tracking’. However, other than tracking steps or food intake, the activities and sensations tracked while sleeping are usually not conscious to oneself. Hence, STA provide access to completely new personal information. This information can concern the STA user themselves, but also another person sleeping in the same room. Other than for tracking steps, heart rates or alike, most currently available STA operate without body contact to the user. However, the majority of STA cannot distinguish if it is the user themselves snoring or rolling around in bed—or, for example, the user’s significant other who did not consent to be tracked. Consequently, sleep is not only a ‘sensitive’ part of humans’ life and health, but sleep tracking must also be distinguished from the tracking of other health-related behaviour.
Former work has mainly focused on the usage of sleep tracking devices (Baron et al., 2018), their functions (Ong & Gillespie, 2016), the accuracy and reliability of devices (Berryhill et al., 2020; Fino & Mazzetti, 2019), the validity of the information contained within the apps that run on the devices (Lee-Tobin et al., 2017), the screening quality for sleep disorders (Behar et al., 2013), in particular regarding mental illness (Aledavood et al., 2019), and their use in therapy (Stippig et al., 2015), clinical care and research (Shelgikar et al., 2016). Despite this strong interest and to the best of our knowledge previous publications have not discussed ethical implications associated with consumer-targeted STA in depth. The differences between sleep-tracking and other forms of self-tracking (e.g., step-tracking) outlined above suggest that to fill this gap, the first step should be to address the particular ethical challenges associated with the use of STA that distinguish it from the tracking of other forms of health behaviours/activities. Hence, this article sets out to identify the specifics of STA (compared to other applications of self-tracking) and the particular ethical issues involved. The aim is not to systematically locate all relevant literature and to discuss STA comprehensively, but to debate ethical issues that especially arise in the use of STA. The two main research questions for this article were (1) what are the specific functions of STA and, derived therefrom, (2) what are the most distinctive ethical aspects of STA. Within this paper, STA refer to consumer-targeted wearable devices or mobile applications installed on a smartphone to record and analyze data related to sleep. The applications in question are publicly accessible and usable without guidance by healthcare professionals. Internet based programmes, sleep tracking devices that are used in biomedical research and sleep apps intended for use by healthcare professionals were excluded for analysis.
Methods
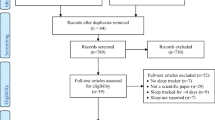
In a first step, the field of mobile health applications was screened for STA to explore applications, their specific functions and target user groups. Since there are already sufficient and well-conducted scientific reviews (Baron et al., 2018; Behar et al., 2013; Choi et al., 2018; Fino & Mazzetti, 2019; Ko et al., 2015; Lee-Tobin et al., 2017; Ong & Gillespie, 2016; Shelgikar et al., 2016; Stippig et al., 2015), no additional review was conducted for this article, but rather the results of the existing reviews were used as a basis. Considering the highly dynamic market and fast development of new applications, the ‘Best Sleep-Tracker’ lists of 2020 and 2021 by Anglo-American media such as BBC, NY Times and The Men Journal as well as by independent, consumer-driven test reports were scanned. For apps that had not been included in the existing reviews the user information by the developer was consulted to get an overview over the app functions. This comprehensive screening and detailed presentation of STA, their functions and potential user groups that will follow below has been conducted to catch as many facets of the technology as possible, take its conceptual and practical particularities into account and, ultimately, come up with an ethical analysis that is close to the users’ experience with STA.
In a second step, the specific normative dimensions from the user perspective of STA were elaborated. Since many ethical aspects regarding tracking apps have already been analyzed, e.g., autonomy (Owens & Cribb, 2019; Sharon, 2017) or privacy (Lanzing, 2019), and the overall rationale can be transferred to STA, the guiding question was: Which ethical aspects are specific to STA that do not have the same relevance for other tracking apps? Consequently, our analysis does not provide a comprehensive listing of ethical aspects of STA. Instead, the focus is on an in-depth analysis of three key issues that have not received sufficient attention in scholarship so far, but are highly relevant for the ethical debate surrounding STA and the particularities of sleep and sleep-tracking: (1) medicalization of everyday sleeping experience, (2) vulnerability, and (3) relationality.
Role of sleep
Sleep is an essential part of human life and good health (Centers for Disease Control & Prevention, 2021). Although the question of why humans sleep has not yet been answered conclusively (Assefa et al., 2015; Rial et al., 2007), current research highlights the importance of sleep for neural regeneration processes (Mendelsohn & Larrick, 2013) and the organization of memory and learning, so called neurocognitive consolidation (Diekelmann & Born, 2010). Hence, physical and cognitive performance is dependent on sufficient sleep. Likewise, poor sleep can have profound negative effects on the quality of life, lead to multiple diseases, including chronic conditions (Liu et al., 2013), and be a warning signal for early phases of mental disorders, such as bipolar disorder (Gold & Sylvia, 2016) or depression (Nutt et al., 2008). However, sleep is not only an essential component of one’s life, but at the same time also a very vulnerable one, which can easily be disrupted by a wide variety of factors such as noise or light, behavioural habits, (digital) social interactions (Murnane et al., 2015), and psychological or emotional factors such as stress (Kim & Dimsdale, 2007). In addition, sleep usually takes place in private space and is very intimate.
General functions of sleep tracking applications
There are different types of mobile technologies, software programmes, wearables and non-contact devices available at the market that offer consumers various functions to track, analyze and enhance their sleep outside of the clinical context (Ko et al., 2015; Van den Bulck, 2015; Ong & Gillespie, 2016; Baron et al., 2018; Choi et al., 2018; Sadek et al., 2020). These apps, which typically run on smartphones or tablets, either use in-built sensors and devices of smartphones or tablets (e.g., microphone or accelerometer) or can be connected to additional wearables (e.g., smartwatches or smart rings) and non-contact tracing devices that are placed in the immediate surrounding of the bed (e.g., under the mattress or on the bedside table). Depending on the technology and sensors used, STA are designed to track several user-related parameters, e.g., movement or body temperature. Most STA can share the tracked data with other health and fitness apps to gather a broader data basis for subsequent analysis. Some applications allow adding information manually, for example, trough sleep diaries, where daily patterns of activity, stress level or nutrition can be added to evaluate possible correlation with sleep quality. Furthermore, some apps monitor the immediate bedroom environment and collect further information such as room temperature or light level. Based on these different parameters tracked, algorithms are used to estimate sleep efficiency and sleep quality. The STA then offer an analysis of personal trends and give recommendations to improve sleep parameters and experience. To get a comprehensive and systematic overview of the various functions of the apps, the features of STA can be clustered around three phases: (1) going to bed and falling asleep, (2) sleeping, and (3) waking up.
Falling asleep
Specific functions of STA aim to help users fall asleep more easily and at the ‘right’ time in order to improve sleep quality, reduce sleep disturbances and feel more refreshed during daytime. Depending on the self-chosen or recommended amount of sleep, STA send users personal reminders when it is time to go to bed and sometimes even offer rewards (e.g., in form of badges) if users follow the request within a certain time frame. Applications’ recommendations for sleeping goals (e.g., bedtime) can be more or less individualized. Some STA base their recommended sleeping goals simply on averages for age and gender. Other STA take a more individualized approach and use already tracked sleep parameters of the user as a basis for recommendations. Other functions that are designed to fall asleep more easily are, for example, collections of lullabies, relaxing music and soundscapes, stories or poetry. Sleep aid functions can in some cases be individualized by including a personalized composition of music or sounds into the app or by using relaxation functions that are based on the concept of biofeedback. Further functions include the possibility to take written or oral notes with the aim to get pressing issues off the users’ mind that could have adverse effects on falling asleep. Furthermore, STA offer the possibility to automatically turn off other applications, such as texting, calling, and social media applications whilst still enabling sleep tracking functions.
Sleeping
In the phase of sleeping, STA primarily track and analyze various user-related sleep parameters, e.g., movement, breathing rate and volume, heart rate, body temperature and noise. Some STA use audio recording to detect snoring, sleep apnea and sleep talking. In addition, some of these applications offer anti-snoring functions that react with vibrations or sounds to stop users snoring. The applications do not only vary according to the number of parameters they track, but also according to the comprehensiveness of tracking. For example, some applications only offer the possibility to instantaneously measure heart rate at a definite point in time, whereas other devices continuously record heart rate during sleep and, hence, enable a more comprehensive algorithm-based analysis. In addition, some devices monitor the immediate bedroom environment and gather information on room temperature or noise and light level, in order to identify influences that have an impact on the experienced or estimated quality of sleep. Most STA claim that the presence of a second person (or pet) in bed does not affect the outcomes of the tracking apps if the devices are carefully positioned. However, some devices (especially those that use radio or sonar waves) exclude the possibility that two persons use the same type of device whilst sharing a bed. Some applications enable geotagging to help identify variations in sleep patterns in terms of location. Depending on the type and comprehensiveness of data, algorithms are used to differentiate between different phases and cycles of sleep (awake, light and deep sleep, rapid eye movement), as well as to estimate sleep efficiency and sleep quality. To estimate the sleep quality, indexes or scores are frequently used. However, not every application discloses transparently how the sleep quality and the relevant scores are calculated.
Waking up
Smart alarm is probably the most common function of STA that addresses the waking up phase. In order to make users feel more rested, smart alarm tries to choose an optimal period for waking up, which generally is a phase of light sleep close to the time users need to get up. Some STA allow connecting smart alarm to external devices such as smart light devices that simulate sunrise during the waking up phase. To ensure that the person actually gets up, several STA set additional tasks to mute alarm, such as entering a code or solving an arithmetical task. Furthermore, some STA ask the user immediately after waking up to rate their mood, sleep quality and make some notes on their sleeping experience to broaden their data basis.
Sleep tracking applications: sleep lab in the pocket?
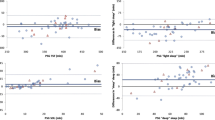
Because of the paramount importance of sleep for health from a medical and psycho-social point of view, methods for monitoring or detecting disturbed sleep are of particular interest. In the clinical context, this includes the sleep laboratory in particular. However, such diagnostic measures are not only expensive, but also unavailable to many individuals and associated with effort and stress. STA are, on the contrary, mobile and inexpensive tools that are easily accessible. Several studies have shown, however, that most freely available STA have limitations. These concern, for example, the accurate detection of wake and deep sleep phases and, hence, the estimation of total sleep time and sleep efficiency, especially when compared to polysomnography (PSG)Footnote 1 or clinically developed polygraphy (Asgari Mehrabadi et al., 2020; Bhat et al., 2015; de Zambotti et al., 2015a, 2015b, 2016; Fino et al., 2020; Meltzer et al., 2015; Toon et al., 2016). The STA can be seen as strongly reduced versions of polygraphy and PSG that only contain few elements of these clinical diagnostic instruments and are of much lower quality (Fig. 1). Consequently, most STA are not approved for clinical use, i.e., to diagnose or treat sleep disorders. Nevertheless, it might be assumed that individuals affected by symptoms of sleep disorders use STA, especially as sleep laboratories have waiting times of several months, depending on country and region. Individuals who are affected by sleep disorders may use STA and their features in other ways than healthy users; and the functions of STA potentially have not the same effects on the different user groups. For the subsequent ethical analysis of STA, a threefold distinction is therefore made between the following groups of STA users: (1) potential patients, (2) optimizers, and (3) explorers.

Comparison of polysomnography, reduced polygraphy and STA
The first group of users, the potential patients, may begin to use STA because of symptoms that can be linked to sleep disorders. The exact global prevalence of people with symptoms of sleep disorders is unknown, for example, due to varying estimated prevalence in different countries. However, more than a third of U.S. adults report insufficient sleep (Liu et al., 2016). The group of individuals with symptoms of sleep disorders consists of potential candidates for PSG and a clinical evaluation of their sleep disturbances. Their use of STA can be described as unregulated and non-embedded because these devices are neither approved for clinical use nor embedded in a patient-physician-relationship. The second group, the optimizers, may turn to STA because they generally feel unsatisfied with aspects of their daily performance, e.g., productivity or concentration. These STA users do not suffer from actual sleep disorders but rather from an impairment of their general well-being that may be due to psychosocial factors (e.g., workload, emotional distress), a general dissatisfaction with their performance, or the wish to become more efficient. The use of STA can be described in this group as an attempt to improve the own performance in order to compensate for the alleged or experienced lack of productivity, concentration or resilience. The third group, the explorers, may use STA just out of curiosity, for example, because these functions are integrated in fitness trackers that they have bought for other purposes or they count themselves to the Quantified Self community (Sharon, 2017).
The distinction between these user groups is not always straightforward. For example, explorers may come to appreciate a possible sleep-improving effect of STA, or potential patients may come to understand that their sleep behavior is on a normal spectrum. The distinction between these user groups may nevertheless be a useful heuristic, as it involves not only different needs of individuals, but also ethically relevant dimensions.
Ethical particularities of sleep-tracking
Various ethics guidelines and frameworks have been proposed in recent years for identifying, considering and resolving ethical questions associated with data-driven technologies in healthcare and research (Hagendorff, 2020; Ienca et al., 2018; Jobin et al., 2019; Vayena et al., 2018; Xafis et al., 2019). While various models tailored for the assessment of mHealth applications have been put forward recently (van Haasteren et al., 2019) and ethical aspects of self-tracking technologies are being increasingly discussed (Lupton, 2016), no framework has solely focused on STA so far. The existing frameworks often provide comprehensive lists of criteria to assess the quality of digital health technologies. Many of these ethical aspects can be transferred to STA. However, STA, and especially the context of sleep, comes with characteristics that are not found in other tracking devices. Since the aim of the current paper is to analyze the specifics of STA no reference to such a broad ethics framework is made, but the focus is on a more in-depth analysis of three particularly relevant key issues: (1) medicalization of everyday sleeping experience, (2) vulnerability, and (3) relationality. This focus leaves out ethical aspects of STA that also apply to other mHealth or lifestyle applications, such as issues of informational or decisional privacy (Lanzing, 2019). At the same time, the selected ethical dimensions highlight very specific requirements of sleep technology that distinguish it from other apps.
Medicalization of everyday sleeping experience
A common feature of most STA is that they integrate the tracked parameters in terms of sleep quality and sleep efficiency. Sleep quality and sleep efficiency are conceptual tools in medical diagnosis and treatment of sleeping disorders, especially insomnia. For example, sleep efficiency is not an absolute value that in itself provides useful information on the health status of the users. Although inconsistencies in operationally defining sleep efficiency have been noted (Reed & Sacco, 2016), on a conceptual level sleep efficiency is most often defined as the ratio of total sleep time to time in bed. Difficulties to fall asleep and to re-initiate sleep are important criteria for diagnosing insomnia (Rivera & Orff, 2020). Outside this specific context of sleeping disorders, sleep efficiency may be of no use at all in measuring sleep quality as individuals who do not suffer from sleep disturbances may enjoy an extended time in bed without sleeping.
The use of the conceptual diagnostic tools of sleep efficiency and sleep quality by freely available STA can be described as a medicalization of everyday sleeping experience. Medicalization has been a topic in social sciences for several decades and adopted as an analytic tool in various other disciplines (Conrad, 2007). Two specifications are important in the context of STA. First, STA entail medicalization of everyday sleeping experience on a conceptual level, as opposed to other levels of medicalization such as the institutional level or level of patient-physician interaction (Conrad & Schneider, 1980). STA reframe everyday sleeping experience by evaluating users’ sleeping experience in terms of the diagnostic and therapeutic concepts of sleep efficiency and sleep quality. Second, medicalization is in this case a consumer-driven process (Conrad, 2005). It is not an attempt by the medical profession to redefine a phenomenon in medical terms and, hereby, claim authority in managing this phenomenon. Rather, consumers use the medical concepts of sleep efficiency and sleep quality to track and optimize their sleeping experience. Ethical concerns regarding this consumer-driven process of medicalization differ for the three identified groups of STA users.
The group of potential patients may include users that are affected by symptoms of insomnia and currently do not receive treatment. The unregulated and non-embedded use of STA bears some risks for this group. On the one hand, if STA adequately distinguish between sleeping and time lying in bed trying to fall asleep, the use of STA by persons suffering from insomnia may accurately indicate a total sleep time and sleep efficiency that is rather low compared to some standard population. However, if the use of STA is not embedded in a therapeutic relationship, this information could reinforce inappropriate coping mechanism in those individuals, such as going to bed earlier in order to compensate for sleep deprivation of previous nights. This may worsen insomnia, as the attempt for sleep extension tends to intensify the frustrating experience of lying in bed and being unable to sleep, hence, increasing psychological stress that bears the risk of chronification of insomnia (Rivera & Orff, 2020). On the other hand, given the inaccuracy of STA with the tendency to overestimate sleeping time by mistaking time lying in bed trying to fall asleep as actual sleep, the resulting estimation of total sleep time and sleep efficiency could erroneously suggest to this group of users that they have a healthy sleeping pattern. This could refrain individuals actually suffering from insomnia to seek medical treatment in a timely manner.
With regard to the group of optimizers, the use of STA may reinforce concerns about getting the right amount of high-quality sleep to compensate for the experienced lack of productivity, concentration, or resilience. Case reports suggest that the use of STA may induce in individuals a ‘perfectionistic quest for the ideal sleep in order to optimize daytime function’ (Baron et al., 2017). The authors of these case reports describe this condition as ‘orthosomnia’ as their patients became ‘preoccupied or concerned with improving or perfecting their wearable sleep data’ (Baron et al., 2017). As these case reports suggest, extensive use of STA may also pose challenges for clinicians as patients may have greater trust in their self-tracked data than in their own experience or clinical results of PSG. Baron et al. (2017) report, for example, that they were unable to convince one of their patients that she slept deeply according to in-laboratory PSG because she insisted that her STA kept telling her otherwise. Such rigid beliefs about the validity of sleep tracking data can complicate, for example, the treatment of insomnia (Baron, 2022).
The STA may have the lowest risks in the group of explorers, although the detection of ‘suboptimal’ sleep parameters may induce in these groups also concerns about sleep efficiency and quality.
Vulnerability
Due to the specific ‘sensitive’ nature of sleeping and the tremendous effects of poor sleep and sleep disorders on one’s health and life, vulnerability is a further important aspect regarding the use of STA. The state of being vulnerable can refer to various conditions and contexts. As Erinn Gilson (2014) emphasized, there is no narrow definition of the term, but ‘[a]cross the diverse instances of vulnerability, a common sense of vulnerability is underscored: vulnerability is defined by openness and, more specifically, to be vulnerable is to be open to being affected and affecting in ways that one cannot control.’ In the context of STA, talking of vulnerability indicates a general concern about the susceptibility of the sleeping users to harm, because sleeping persons lack the ability to protect themselves. They are particularly vulnerable during sleep, simply because they are not awake, and hence, cannot actively control themselves or surveil their environment. Besides this general concern, the three groups of STA users can be considered as vulnerable to varying degrees according to their different group characteristics.
The first group of STA users, the potential patients, can be understood as vulnerable in several dimensions. Individuals who are affected by symptoms associated with sleep disorders or sleep-deprived individuals can be physically vulnerable. The physical performance is - among others - dependent on sufficient sleep. Not enough or poor sleep can influence the immune system, making the body vulnerable to pathogenic actions and thus influence the resistance to illness (Irwin, 2015; Wilder-Smith et al., 2014). Individuals who do not get enough restful sleep are, for example, more likely to catch a common cold (Prather et al., 2016). Sleep deprivation can have a variety of physical consequences, for example, overexertion or lower stamina, increased risk of heart attack or higher risk of being overweight (Liu et al., 2013; Hanson et al., 2021). However, sleep-deprived individuals are also vulnerable in a psychological dimension. Insufficient sleep can manifest, for example, in a lower ability to concentrate, reduced reaction time, decreased vigilance, perceptual and cognitive distortions and an increased stress level (Hanson et al., 2021). Moreover, poor sleep can be a sign or an early phase of mental disorders such as bipolar disorder or depression (Gold & Sylvia, 2016; Nutt et al., 2008). Finally, individuals with sleep disorders may also be socially vulnerable, as sleep loss can have profound adverse effects on social and work life, for example, by not being able to ‘perform well enough’ (Gerald, 1989). Due to sleepiness, occupational actions may be performed in incorrect ways and accidents may occur (Graves & Miller, 2015). Moreover, third parties can misinterpret manifestations of sleep disorders for laziness, lack of interest or reduced intelligence (Stores, 2006; Stores et al., 2006). Undiagnosed sleep disorders can cause anxiety, shame and feelings of helplessness for the individuals affected (Stores, 2006; Stores et al., 2006). The lack of understanding and prejudice from the social environment can lead to social withdrawal and contribute to a reduced quality of life for those affected by sleep disorders (Stores, 2006; Stores et al., 2006).
Given this elevated physical, psychological and social vulnerability of the ‘potential patient’ user group, the use of STA may have far-reaching consequences for the health and well-being of these users, as an unregulated and unembedded use can intensify the problems of an undiagnosed or untreated sleep disorder (Baron, 2022; Baron et al., 2017). Vice versa, a possible exacerbation of the users’ symptoms may increase their vulnerability. By contrast, through early warning signs, raising awareness and preventive measures, STA can help to reduce insufficient sleep, recognize and prevent sleep disorders early and insofar mitigate the vulnerability of potential patients.
In comparison with individuals affected by sleep disorders, it may be assumed that individuals in the second group, the optimizers, are physically, psychologically, and socially less vulnerable than the potential patients. For example, their physical and cognitive performance is not impaired by a sleep disorder and they have no symptoms that could be misunderstood in social circumstances or even worsened by using STA. Nevertheless, these users have the wish to enhance their performance by STA use, which might ground on some kind of dissatisfaction with themselves or their productivity. There is the risk that this dissatisfaction will be reinforced by using STA and lead, for example, to mental health risks for the user. Constant data sharing and comparison with others can result in adverse feelings of pressure, shame or guilt, impede productivity, lead to depression or orthosomnia and also involve the potential to become addicted to the app (Jacobs, 2020; Kreitmair et al., 2017; Lupton, 2018). Contrary to their promises, STA would decline in these cases the empowerment and autonomy of the users and instead create new vulnerabilities, especially in the context of a society in which high work performance is socially desired. App users are not abstract, atomized agents but embedded into social structures (Herzog et al., 2021). Hence, the app use can influence the users’ behaviour also due to social desirability bias (Herzog et al., 2021; Jacobs, 2020; Lupton, 2018). Regarding the vulnerability of STA users, it is thus important to consider not only the individual user, but also the social circumstances of the app use. Herzog et al. (2021) suggest, therefore, in the context of mHealth technologies, an approach that links the concept of vulnerability also to structural societal factors.
The third group, the explorers as persons using STA just out of curiosity, have the lowest degree of vulnerability in the triad of users. They show interest but not some dissatisfaction or signs of disorder to the app. Nevertheless, it might occur that a new dissatisfaction with the own ‘normal’ sleep is created by tracking one’s sleep and closely studying the information and pattern recognition the STA provides. In this case, the use of STA could evoke doubts about one’s sleep, lead to behaviour changes - although the user does not experience any physical or psychological strain - make the user dependent upon their STA, and thus create vulnerability that did not exist before. In addition, signs of diseases could be discovered by the STA that the user was not aware of and/or does not want to know.
Relationality
A third aspect that is of particular importance in the use of STA is relationality. Although a ‘relational turn in bioethics’ has already been spotted by Bruce Jennings (2016) some years back, the main focus of bioethical research is still on the single individual as the user of a health application. However, the use of STA may interfere by its very nature with non-users. These can be partners sharing the same bed, babies and children sleeping in the same room, or even strangers that share a dormitory with a STA-user, e.g., in a hostel. Hence, the ethical analysis of STA must also extend to these third parties.
Questions of data protection, data sovereignty and informational autonomy arise, for example, when snoring or talking in one’s sleep is recorded by someone else’s STA. However, relationality goes beyond such risks of second party`s privacy. It is especially in intimate relationships that questions of relational autonomy and trust, negative liberty and power are tackled. Negative liberty is being free from others’ interference, e.g., someone’s intrusion into the other’s private sphere by recording their talking in sleep. Negative liberty - and autonomy - can be understood in an individual or even atomistic fashion as the freedom from obstacles and constraints one faces from the outside. The concept of relational autonomy adds to this by emphasising the individuals’ interdependence and -connectedness, their social embeddedness and relatedness to others (Nedelsky, 2011). Aspects concerning relational autonomy and negative liberty are particularly pertinent for the phase of sleep in which we are not aware of our own and other’s actions. With the use of STA that so far cannot distinguish between one’s own snoring and that of others, it becomes possible to also retrace the sleep of others. Consequently, the STA-user obtains information about their ‘bedfellow’, which the bedfellow may be unaware of or may not wish to disclose. Whether this infringement of the other’s intimacy and (informational) self-determination can be justified does not only depend on the other’s consent, and the data collected, but also on the user’s interests, i.e., the reason behind tracking their sleep. The interests of the three user groups can be assessed differently, for example, with the help of an ethical risk-benefit-analysis or weighing of goods in case of competing interests and preferences that also takes into account the relation between the STA-user and indirectly tracked bedfellow (Broome, 1991). One aspect to pursue is if (and how) the principle of doing no harm - understood in a broad sense that includes all people as addressees of this principle - might justify the use of STA for medical interests, i.e., to avoid harm for the STA-user’s life and wellbeing. For the other two user groups where possible harms for the STA-user are more obscure, looking particularly at the relationality of STA and the structure of the relation that underlies the relationship between STA-user and their bedfellow might help to set up a corridor between morally impermissible and morally unobjectionable uses of STA.
Finally, the aspect of relationality points to another characteristic of STA that distinguishes these applications from, for example, step tracking. Other’s sleep may not be only tracked by accident, as a side effect, but also on purpose. This can both undermine this other’s autonomy or enhance it (Nedelsky, 2011). One may categorize the use as positive regarding autonomy if the STA is deployed to observe the partner’s breathing interruptions to be warned of obstructive sleep-apnoea that can lead to heart attacks, stroke and even death while sleeping (Al Lawati et al., 2009). Given a transparent, mutually agreed on use of the STA for monitoring purposes, this can enhance the autonomy of both partners as outsourcing the guard position to the STA gives both back more control over their sleep. This relational dimension of tracking can be understood as an intimate and responsible way of caring for each other in the context of relationships or family life (Will et al., 2020). However, if such a use is not justified and not agreed on, at least two thoughts must be taken into account: First, by gathering knowledge on their partner’s sleep the STA-user gains power over them. Second, and given such a (knowledge) power imbalance, this may come with some form of control and, hence, domination which reduces the partner’s capacity for (relational) autonomy (Nedelsky, 2011).
Points for consideration
The current analysis focuses on freely available, consumer-led STA laying the conceptual foundations for their responsible use and implementation. General recommendations for consumer-led STA use are difficult to establish, as they depend on each group’s respective risks, opportunities and varying degrees of vulnerability. Nevertheless, some considerations can be derived that aim at the responsibility of developers and distributors of STAs and need further research and more elaborate reflection in the future. To adequately meet the identified ethical challenges, it would be important to start with the development process of STA and, for example, to provide guidelines for responsible STA development. The awareness of developers and distributors for ethical aspects of STA use and the specific vulnerabilities of the different user groups should be raised, so that they integrate normative considerations into the conceptualization and development of STA. To better address the needs and vulnerabilities of the different user groups (potential or actual patients, optimizers, explorers), these could directly be involved in the development process. Further, the sales, distribution and marketing around STA should also be examined critically. The presentation of STA, for example, in the app store, should be in line with the service the respective STA can actually deliver. Information, warnings, or a kind of 'instruction leaflet' could clearly and briefly explain which user group the app is intended for and what the app can and cannot offer the respective group. More information about the various functions, especially about the potential risks of using the app, should be included, such as references to mental health risks, vulnerabilities, and links to professional help for sleep disturbances. Moreover, the information should indicate that embedding STA in a medical or therapeutic relationship could help avoid wrong coping mechanism and minimize stress and mental health risks for lay users.
Since the focus of this paper is on conceptual and normative aspects of freely available consumer-led STA, these points for consideration are rather 'soft' and primarily appeal to the responsibility of the developers and distributors of STAs. Stricter legal requirements, on the other hand, could result from categorizing lifestyle data as medical data (in contrast to their categorization as ordinary personal data), as currently debated in the European Union. The classification of lifestyle data as medical data comes with further implications regarding a possible regulation of such apps (per Regulation (EU) 2017/745 of the European Parliament and of the Council of 5 April 2017 on Medical Devices). Moreover, data concerned with the app user’s health is subject to the general data protection regulation (GDPR). So far, no consensus among legal scholars and practitioners has been achieved on which data concerns health and/or medical information and how ‘health app’ and ‘medical app’ can be distinguished from each other legally (Maaß et al., 2022). Nevertheless, the tendency is to broaden the definition of health data (Schäfke-Zell, 2022) and, for example, also consider how the users themselves, the STA provider, and possible clinicians involved intend to use the data (Carmi et al., 2022). The latter could be of particular relevance to the user group of potential patients, especially if their data is also used for research purposes. As the ongoing legal debates concerning the classification of lifestyle data as medical/health data show, there is an increasing sense of urgency, especially for developers and distributors of STA, to consider the ethical challenges and different user groups.
Conclusion
The fast-growing market of STA creates (new) facts for the users and affected non-users, e.g., partners. Together with legal considerations and a discussion of the broader societal implications of consumer-driven STA use, the normative dimensions should also be addressed in debates about STA implementation. Along the normative concepts of medicalization, vulnerability and relationality, and the three user groups of potential patients, optimizers and explorers, the current analysis provides an ethical classification that focuses on the specific characteristics of STA in contrast to, for example, step tracking. The analysis aims to improve the understanding of the conceptual nature and ethical implications of technologies such as STA, thereby laying the conceptual foundations for their responsible and sustainable implementation. The current analysis focuses on the specific context of STA and provides input on the theoretical level. Future (empirical) research could address concrete social and ethical implications, for example, how STA influence the different user groups, their informational sovereignty and privacy and potential effects on third parties.
Notes
The PSG is considered the ‘gold standard’ for diagnosing sleep disorders. The main reasons to undergo PSG are obstructive sleep apnea syndrome and neurological indications, such as epilepsy or narcolepsy. A first step in the clinical diagnosis of sleep disorders is an assessment of sleepiness, which is based on well-established questionnaires (e.g., STOP-BANG questionnaire) and the guidelines of the American Academy of Sleep Medicine (AASM 2022). Further diagnostic steps include polygraphy, mostly followed by full-clinical PSG.
Abbreviations
- PSG:
-
Polysomnography
- STA:
-
Sleep tracking application
References
American Academy of Sleep Medicine (AASM). Guidelines at a Glance. Retrieved March 14, 2022, from https://learn.aasm.org/Listing/a1341000002pxTNAAY.
Al Lawati, N. M., Patel, S. R., & Ayas, N. T. (2009). Epidemiology, risk factors, and consequences of obstructive sleep apnea and short sleep duration. Progress in Cardiovascular Diseases, 51(4), 285–293. https://doi.org/10.1016/j.pcad.2008.08.001
Aledavood, T., Torous, J., Triana Hoyos, A. M., Naslund, J. A., Onnela, J., & Keshavan, M. (2019). Smartphone-based tracking of sleep in depression, anxiety, and psychotic disorders. Current Psychiatry Reports, 21, 49. https://doi.org/10.1007/s11920-019-1043-y
Asgari Mehrabadi, M., Azimi, I., Sarhaddi, F., Axelin, A., Niela-Vilén, H., Myllyntausta, S., Stenholm, S., Dutt, N., Liljeberg, P., & Rahmani, A. M. (2020). Sleep tracking of a commercially available smart ring and smartwatch against medical-grade actigraphy in everyday settings: instrument validation study. JMIR mHealth and uHealth, 8(10), e20465. https://doi.org/10.2196/20465
Assefa, S. Z., Diaz-Abad, M., Wickwire, E. M., & Scharf, S. M. (2015). The functions of sleep. AIMS. Neuroscience, 2(3), 155–171. https://doi.org/10.3934/Neuroscience.2015.3.155
Baron, K. G. (2022). CBT-I for patients with orthosomnia. In S. Nowakowski, S. N. Garland, M. A. Grandner, & L. J. Cuddihy (Eds.), Adapting cognitive behavioral therapy for insomnia (pp. 135–145). Academic Press.
Baron, K. G., Abbott, S., Jao, N., Manalo, N., & Mullen, R. (2017). Orthosomnia: Are some patients taking the quantified self too far? Journal of Clinical Sleep Medicine, 13(2), 351–354. https://doi.org/10.5664/jcsm.6472
Baron, K. G., Duffecy, J., Berendsen, M. A., Cheung Mason, I., Lattie, E. G., & Manalo, N. C. (2018). Feeling validated yet? A scoping review of the use of consumer-targeted wearable and mobile technology to measure and improve sleep. Sleep Medicine Reviews, 40, 151–159. https://doi.org/10.1016/j.smrv.2017.12.002
Behar, J., Roebuck, A., Domingos, J. S., Gederi, E., & Clifford, G. D. (2013). A review of current sleep screening applications for smartphones. Physiological Measurement, 34(7), R29-46. https://doi.org/10.1088/0967-3334/34/7/R29
Berryhill, S., Morton, C. J., Dean, A., Berryhill, A., Provencio-Dean, N., Patel, S. I., Estep, L., Combs, D., Mashaqi, S., Gerald, L. B., Krishnan, J. A., & Parthasarathy, S. (2020). Effect of wearables on sleep in healthy individuals: A randomized crossover trial and validation study. Journal of Clinical Sleep Medicine, 16(5), 775–783. https://doi.org/10.5664/jcsm.8356
Bhat, S., Ferraris, A., Gupta, D., Mozafarian, M., DeBari, V. A., Gushway-Henry, N., Gowda, S. P., Polos, P. G., Rubinstein, M., Seidu, H., & Chokroverty, S. (2015). Is there a clinical role for smartphone sleep apps? Comparison of sleep cycle detection by a smartphone application to polysomnography. Journal of Clinical Sleep Medicine, 11(7), 709–715. https://doi.org/10.5664/jcsm.4840
Broome, J. (1991). Weighing Goods: Equality, Uncertainty and Time. Wiley-Blackwell.
Carmi, L., Zohar, M., & Riva, G. M. (2022). The European general data protection regulation (GDPR) in mhealth: Theoretical and practical aspects for practitioners’ use. Medicine, Science and the Law. https://doi.org/10.1177/00258024221118411
Centers for Disease Control and Prevention (2021). Sleep and Sleep Disorders. Retrieved March 14, 2022, from https://www.cdc.gov/sleep/index.html.
Choi, Y. K., Demiris, G., Lin, S. Y., Iribarren, S. J., Landis, C. A., Thompson, H. J., McCurry, S. M., Heitkemper, M. M., & Ward, T. M. (2018). Smartphone applications to support sleep self-management: Review and evaluation. Journal of Clinical Sleep Medicine, 14(10), 1783–1790. https://doi.org/10.5664/jcsm.7396
Conrad, P. (2005). The shifting engines of medicalization. Journal of Health and Social Behavior, 46(1), 3–14. https://doi.org/10.1177/002214650504600102
Conrad, P. (2007). Medicalization of society. On the transformation of human conditions into treatable disorders. John Hopkins University Press.
Conrad, P., & Schneider, J. W. (1980). Looking at levels of medicalization: A comment on strong’s critique of the theses of medical imperialism. Social Science and Medicine, 14A(1), 75–79.
de Zambotti, M., Baker, F. C., & Colrain, I. M. (2015a). Validation of sleep-tracking technology compared with polysomnography in adolescents. Sleep, 38(9), 1461–1468. https://doi.org/10.5665/sleep.4990
de Zambotti, M., Baker, F. C., Willoughby, A. R., Godino, J. G., Wing, D., Patrick, K., & Colrain, I. M. (2016). Measures of sleep and cardiac functioning during sleep using a multi-sensory commercially-available wristband in adolescents. Physiology & Behavior, 158, 143–149. https://doi.org/10.1016/j.physbeh.2016.03.006
de Zambotti, M., Claudatos, S., Inkelis, S., Colrain, I. M., & Baker, F. C. (2015b). Evaluation of a consumer fitness-tracking device to assess sleep in adults. Chronobiology International, 32(7), 1024–1028. https://doi.org/10.3109/07420528.2015.1054395
Diekelmann, S., & Born, J. (2010). The memory function of sleep. Nature Reviews Neuroscience, 11, 114–126. https://doi.org/10.1038/nrn2762
Doug, H., Knutson, K. L., & Orzech, K. M. (2013). Sleep, culture and health: Reflections on the other third of life. Social Science and Medicine, 79, 1–6. https://doi.org/10.1016/j.socscimed.2012.11.023
Espie, C. A., & Morin, C. M. (2012). Introduction: Historical landmarks and current status of sleep research and practice: An introduction to the timeliness, aims, and scope of this handbook. In C. M. Morin & C. A. Espie (Eds.), The oxford handbook of sleep and sleep disorders (pp. 1–8). Oxford University Press.
Fino, E., & Mazzetti, M. (2019). Monitoring healthy and disturbed sleep through smartphone applications: A review of experimental evidence. Sleep Breath, 23, 13–24. https://doi.org/10.1007/s11325-018-1661-3
Fino, E., Plazzi, G., Filardi, M., Marzocchi, M., Pizza, F., Vandi, S., & Mazzetti, M. (2020). (Not so) Smart sleep tracking through the phone: Findings from a polysomnography study testing the reliability of four sleep applications. Journal of Sleep Research. https://doi.org/10.1111/jsr.12935
Gerald, P. K. (1989). Sustained work, fatigue, sleep loss and performance: A review of the issues. Work & Stress, 3(2), 129–141. https://doi.org/10.1080/02678378908256939
Gilson, E. C. (2014). The Ethics of Vulnerability. Routledge.
Gold, A., & Sylvia, L. (2016). The role of sleep in bipolar disorder. Nature and Science of Sleep, 8, 207–214. https://doi.org/10.2147/NSS.S85754
Graves, J. M., & Miller, M. E. (2015). Reduced sleep duration and history of work-related injuries among Washington State adolescents with a history of working. American Journal of Industrial Medicine, 58(4), 464–471. https://doi.org/10.1002/ajim.22416
Hagendorff, T. (2020). The ethics of AI ethics: An evaluation of guidelines. Minds and Machines, 30(1), 99–120.
Hanson, J. A., & Huecker, M. R. (2021). Sleep deprivation. StatPearls Publishing.
Herzog, L., Kellmeyer, P., & Wild, V. (2021). Digital behavioral technology, vulnerability and justice: Towards an integrated approach. Review of Social Economy. https://doi.org/10.1080/00346764.2021.1943755
Ienca, M., Ferretti, A., Hurst, S., Puhan, M., Lovis, C., & Vayena, E. (2018). Considerations for ethics review of big data health research: A scoping review. PLoS ONE, 13(10), e0204937. https://doi.org/10.1371/journal.pone.0204937
Irish, L. A., Kline, C. E., Gunn, H. E., Buysse, D. J., & Hall, M. H. (2015). The role of sleep hygiene in promoting public health: A review of empirical evidence. Sleep Medicine Review. https://doi.org/10.1016/j.smrv.2014.10.001
Irwin, M. R. (2015). Why sleep is important for health: A psychoneuroimmunology perspective. Annual Review of Psychology, 66, 143–172. https://doi.org/10.1146/annurev-psych-010213-115205
Jacobs, N. (2020). Two ethical concerns about the use of persuasive technology for vulnerable people. Bioethics, 34(5), 519–526. https://doi.org/10.1111/bioe.12683
Jennings, B. (2016). Reconceptualizing autonomy: A relational turn in bioethics. Hastings Center Report, 46, 11–16. https://doi.org/10.1002/hast.544
Jobin, A., Ienca, M., & Vayena, E. (2019). The global landscape of AI ethics guidelines. Nature Machine Intelligence, 1(9), 389–399. https://doi.org/10.1038/s42256-019-0088-2
Kim, E., & Dimsdale, J. E. (2007). The effect of psychosocial stress on sleep: A review of polysomnographic evidence. Behavioral Sleep Medicine, 5(4), 256–278. https://doi.org/10.1080/15402000701557383
Ko, P. R., Kientz, J. A., Choe, E. K., Kay, M., Landis, C. A., & Watson, N. F. (2015). Consumer sleep technologies: A review of the landscape. Journal of Clinical Sleep Medicine, 11(12), 1455–1461. https://doi.org/10.5664/jcsm.5288
Kreitmair, K., Cho, M., & Magnus, D. (2017). Consent and engagement, security, and authentic living using wearable and mobile health technology. Nature Biotechnology, 35, 617–620. https://doi.org/10.1038/nbt.3887
Kryger, M. (2019). Sleep in Art: How Artists Portrayed Sleep Over the Last 7000 Years. Independently published.
Lanzing, M. (2019). “Strongly recommended”. Revisiting decisional privacy to judge hypernudging in self-tracking technologies. Philosophy & Technology, 32, 549–568. https://doi.org/10.1007/s13347-018-0316-4
Lee-Tobin, P. A., Ogeil, R. P., Savic, M., & Lubman, D. I. (2017). Rate my sleep: Examining the information, function, and basis in empirical evidence within sleep applications for mobile devices. Journal of Clinical Sleep Medicine, 13(11), 1349–1354. https://doi.org/10.5664/jcsm.6814
Liu, Y., Croft, J. B., Wheaton, A. G., Perry, G. S., Chapman, D. P., Strine, T. W., McKnight-Eily, L. R., & Presley-Cantrell, L. (2013). Association between perceived insufficient sleep, frequent mental distress, obesity and chronic diseases among US adults, 2009 behavioral risk factor surveillance system. BMC Public Health, 13, 84. https://doi.org/10.1186/1471-2458-13-84
Liu, Y., Wheaton, A. G., Chapman, D. P., Cunningham, T. J., Lu, H., & Croft, J. B. (2016). Prevalence of healthy sleep duration among adults—United States, 2014. MMWR. Morbidity and Mortality Weekly Report, 65, 137–141.
Lupton, D. (2016). The quantified self. A sociology of self-tracking. Polity Press.
Lupton, D. (2018). ‘I just want it to be done, done, done!’ Food tracking apps, affects, and agential capacities. Multimodal Technologies and Interaction, 2(2), 29. https://doi.org/10.3390/mti2020029
Maaß, L., Freye, M., Pan, C.-C., Dassow, H.-H., Niess, J., & Jahnel, T. (2022). The definitions of health apps and medical apps from the perspective of public health and law: Qualitative analysis of an interdisciplinary literature overview. JMIR mHealth and uHealth, 10(10), e37980. https://doi.org/10.2196/37980
Meltzer, L. J., Hiruma, L. S., Avis, K., Montgomery-Downs, H., & Valentin, J. (2015). Comparison of a commercial accelerometer with polysomnography and actigraphy in children and adolescents. Sleep, 38(8), 1323–1330. https://doi.org/10.5665/sleep.4918
Mendelsohn, A. R., & Larrick, J. W. (2013). Sleep facilitates clearance of metabolites from the Brain: Glymphatic function in aging and neurodegenerative diseases. Rejuvenation Research, 16(6), 518–523. https://doi.org/10.1089/rej.2013.1530
Murnane E, Abdullah S, Matthews M, Choudhury, T., & Gay, G. (2015) Social (media) jet lag: how usage of social technology can modulate and reflect circadian rhythms Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing - UbiComp 15, ACM Press
Nedelsky, J. (2011). Law’s Relations A Relational Theory of Self, Autonomy, and Law. Oxford University Press.
Nutt, D., Wilson, S., & Paterson, L. (2008). Sleep disorders as core symptoms of depression. Dialogues in Clinical Neuroscience, 10(3), 329–336. https://doi.org/10.31887/DCNS.2008.10.3/dnutt
Ong, A. A., & Gillespie, M. B. (2016). Overview of smartphone applications for sleep analysis. World Journal Otorhinolaryngology Head Neck Surgery, 2(1), 45–49. https://doi.org/10.1016/j.wjorl.2016.02.001
Owens, J., & Cribb, A. (2019). ‘My fitbit thinks I can do better!’ Do health promoting wearable technologies support personal autonomy? Philos. Technology, 32, 23–38. https://doi.org/10.1007/s13347-017-0266-2
Prather, A. A., & Leung, C. W. (2016). Association of insufficient sleep with respiratory infection among adults in the United States. JAMA Internal Medicine, 176, 850–853. https://doi.org/10.1001/jamainternmed.2016.0787
Reed, D. L., & Sacco, W. P. (2016). Measuring sleep efficiency: What should the denominator be? Journal of Clinical Sleep Medicine, 12(2), 263–266. https://doi.org/10.5664/jcsm.5498
Rial, R. V., Nicolau, M. C., Gamundí, A., Akaârir, M., Aparicio, S., Garau, C., Tejada, S., Roca, C., Gené, L., Moranta, D., & Esteban, S. (2007). The trivial function of sleep. Sleep Medicine Revision, 11(4), 311–325. https://doi.org/10.1016/j.smrv.2007.03.001
Rivera, G. L., & Orff, H. J. (2020). Insomnia. In K. Sedky, R. Nazir, & D. Bennett (Eds.), Sleep medicine and mental health A guide for psychiatrists and other healthcare professionals. Springer.
Rosekind, M. R., Gregory, K. B., Mallis, M. M., Brandt, S. L., Seal, B., & Lerner, D. (2010). The cost of poor sleep: Workplace productivity loss and associated costs. Journal of Occupational and Environmental Medicine, 52(1), 91–98. https://doi.org/10.1097/JOM.0b013e3181c78c30
Sadek, I., Demarasse, A., & Mokhtari, M. (2020). Internet of things for sleep tracking: Wearables vs. nonwearables. Health Technology, 10, 333–340. https://doi.org/10.1007/s12553-019-00318-3
Schäfke-Zell, W. (2022). Revisiting the definition of health data in the age of digitalized health care. International Data Privacy Law, 12(1), 33–43. https://doi.org/10.1093/idpl/ipab025
Sharon, T. (2017). Self-tracking for health and the quantified self: Re-articulating autonomy, solidarity, and authenticity in an age of personalized healthcare. Philosophy & Technology, 30, 93–121. https://doi.org/10.1007/s13347-016-0215-5
Shelgikar, A. V., Anderson, P. F., & Stephens, M. R. (2016). Sleep tracking, wearable technology, and opportunities for research and clinical care. Chest, 150(3), 732–743. https://doi.org/10.1016/j.chest.2016.04.016
SimilarWeb (2022). Mobile App Ranking. Retrieved January 04, 2023, from https://www.similarweb.com/de/apps/top/google/store-rank/gb/health-fitness/top-free/
Spreitzer, G., & Barne, C. M. (2015). Why sleep is a strategic resource. MIT Sloan Management Review.
Stippig, A., Hübers, U., & Emerich, M. (2015). Apps in sleep medicine. Sleep Breath, 19, 411–417. https://doi.org/10.1007/s11325-014-1009-6
Stores, G. (2006). The protean manifestations of childhood narcolepsy and their misinterpretation. Developmental Medicine and Child Neurology, 48(4), 307–310. https://doi.org/10.1017/S0012162206000661
Stores, G., Montgomery, P., & Wiggs, L. (2006). The psychosocial problems of children with narcolepsy and those with excessive daytime sleepiness of uncertain origin. Pediatrics, 118(4), e1116–e1123. https://doi.org/10.1542/peds.2006-0647
Stuck, B. A., Maurer, J. T., Schlarb, A., Schredl, M., & Weeß, H.-G. (2020). Practice of Sleep Medicine Sleep Disorders in Children and Adults. Springer.
Toon, E., Davey, M. J., Hollis, S. L., Nixon, G. M., Horne, R. S., & Biggs, S. N. (2016). Comparison of commercial wrist-based and smartphone accelerometers, actigraphy, and PSG in a clinical cohort of children and adolescents. Journal of Clinical Sleep Medicine, 12(3), 343–350. https://doi.org/10.5664/jcsm.5580
Van de Water, A. T., Holmes, A., & Hurley, D. A. (2011). Objective measurements of sleep for non-laboratory settings as alternatives to polysomnography–a systematic review. Journal of Sleep Research, 20(1 Pt 2), 183–200. https://doi.org/10.1111/j.1365-2869.2009.00814.x
Van den Bulck, J. (2015). Sleep apps and the quantified self: Blessing or curse? Journal of Sleep Research, 24(2), 121–123. https://doi.org/10.1111/jsr.12270
Van Haasteren, A., Gille, F., Fadda, M., & Vayena, E. (2019). Development of the mHealth app trustworthiness checklist. Digit Health, 5, 2055207619886463. https://doi.org/10.1177/2055207619886463
Vayena, E., Haeusermann, T., Adjekum, A., & Blasimme, A. (2018). Digital health: Meeting the ethical and policy challenges. Swiss Medical Weekly. https://doi.org/10.4414/smw.2018.14571
Wilder-Smith, A., Mustafa, F. B., Earnest, A., Gen, L., & Macary, P. A. (2014). Impact of partial sleep deprivation on immune markers. Sleep Medicine. https://doi.org/10.1016/j.sleep.2013.07.001
Will, C. M., Henwood, F., Weiner, K., & Williams, R. (2020). Negotiating the practical ethics of ‘self-tracking’ in intimate relationships: Looking for care in healthy living. Social Science & Medicine. https://doi.org/10.1016/j.socscimed.2020.113301
Xafis, V., Schaefer, G. O., Labude, M. K., Brassington, I., Ballantyne, A., Lim, H. J., Lipworth, W., Lysaght, T., Stewart, C., Sun, S., Graeme, T. L., & Tai, E. S. (2019). An ethics framework for big data in health and research. Asian Bioethics Review, 11(3), 227–254. https://doi.org/10.1007/s41649-019-00099-x
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors declare that no funds, grants, or other support were received during the preparation of this manuscript
Author information
Authors and Affiliations
Contributions
RM, EK, RR, JH and NP conceived the analysis. All authors were significantly involved in the development of the manuscript. All authors edited the manuscript and approved the final version of the manuscript
Corresponding author
Ethics declarations
Competing interests
The authors have no relevant financial or non-financial interests to disclose
Ethical approval
Not applicable
Consent to participate
Not applicable
Consent to publish
Not applicable
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Müller, R., Kuhn, E., Ranisch, R. et al. Ethics of sleep tracking: techno-ethical particularities of consumer-led sleep-tracking with a focus on medicalization, vulnerability, and relationality. Ethics Inf Technol 25, 4 (2023). https://doi.org/10.1007/s10676-023-09677-y
Accepted:
Published:
DOI: https://doi.org/10.1007/s10676-023-09677-y