
Abstract
To guide school practitioners in the identification and intervention of youth with anxious school refusal, this systematic review used an ecological lens to examine the factors that differentiated children and adolescents with school refusal from those without. Based on the rigorous protocol from the Center for Reviews and Dissemination’s (CRD) internationally recognized guidelines, 15 studies examining 67 different factors were identified. Results reveal 44 individual, social and contextual factors that differentiate youth with school refusal from peers without school refusal. Findings highlight the centrality of anxiety, or anxiety-related symptoms, and diverse learning needs as main points of contrast between youth with school refusal and those without. Implications of an ecological understanding of the factors associated with school refusal for selective and indicative prevention by school and mental health practitioners are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
School refusal (SR) is a school attendance problem (SAP) generally driven by emotional distress [1,2,3]. SR affects between 1 and 15% of youthFootnote 1 according to available North American and European prevalence data [4,5,6]. In addition to the large age range accounted for in available prevalence studies and the types of samples (community vs. clinically referred), the large discrepancy between prevalence rates may be due to the changing ways SR has been operationalized between studies. SR’s first distinction from other SAPs such as truancy stems from the writings of Broadwin [7] and Partridge [8]. These authors described SAPs characterized by fear and distress rather than delinquency. Shortly after, Johnson et al. [9] coined the term “school phobia” to describe this new behavior. School phobia was then described as a form of emotional disturbance in children characterized by a large degree of anxiety and leading to excessive school absences [9]. Almost two decades later, Hersov [10, 11] coined the term “school refusal”.
School phobia was originally used interchangeably with SR in the literature [3], but was replaced because it was an inaccurate label. While school phobia refers to a fear of being in school, the use of “school refusal” is now encouraged because its wider terminology encompasses the different facets of emotional distress (e.g., anxiety, depression, sleep problems, etc.) which underlie the behavior [12]. Generally, youth with SR are identified through operational criteria initially developed by Berg [1] and further specified by others [13, 14]. Notably, Berg’s [2] definition is widely used to this day in scale development (e.g., [15]) and inclusion criteria for sampling (e.g., [16,17,18]). The operational criteria present in Berg’s [2] definition are: (1) school attendance is less than 80% in the classroom during the 2 weeks prior; (2) the presence of an anxiety disorder; (3) parents are aware of their child’s whereabouts during absences; (4) the absence of conduct disorder problems; and (5) parental motivational efforts to encourage their child’s school attendance. For school attendance, Berg’s [2] definition implies more than occasional absences, but rather consistent and repetitive desires to not attend school, leave class early, or avoid certain classes. Moreover, anxiety or emotional distress can manifest itself in different ways. These include physical or psychosomatic forms (e.g., nausea or stomach aches), behavioral forms (e.g., refusing to leave home in the mornings before school), or cognitive forms (e.g., having a panic attack at school before certain classes).
Despite parental and educational efforts, youth with SR face many short- and long-term consequences. Given their low attendance rate, youth with SR may be reluctant to interact with peers. Some short-term consequences derived from this include social isolation, poor academic performance, and, in extreme cases, suicidal ideation [19, 20]. In addition, long-term consequences include an increased susceptibility to adjustment problems in social (e.g., issues with socialization), family (e.g., relational dependence) and professional contexts (e.g., attendance; [21, 22]. Moreover, young adults with a history of school refusal show greater school drop-out rates and are at greater risk of developing psychosocial problems and a form of psychopathology (e.g., major depression) than those with no history of school refusal [23, 24]. These consequences, paired with data that shows that academic achievement is negatively impacted by each day of absence [25], emphasize the importance of early intervention.
Intervention for School Refusal
One of the ways we can aid youth with SR is by mobilizing educators and school practitioners to engage in both selective and indicated prevention (Institute of Medicine (IOM) Classification System). However, these stakeholders are unsure as to the best ways to support students who are at risk and displaying SR-related behaviors [26]. When faced with SR, while educators and school practitioners are conscious that the student is undergoing emotional and behavioral difficulties, they may have difficulty assessing the factors specifically associated to them [12, 27, 28]. Moreover, while addressing students’ mental health concerns is generally a high priority for school practitioners, emotional exhaustion due to high caseloads and/or available resources can be barriers to the quality of care provided [29]. Family-school partnerships have been shown to alleviate this barrier by enhancing not only the quality of care, but also the amount and scope of services available to students [30]. Notably, successful SR interventions in schools suggest mobilizing different stakeholders and emphasize the creation of home-school or parent-practitioner partnerships to promote positive outcomes such as increased attendance (e.g., [31,32,33]). Stakeholders may include parents, school and community practitioners, teachers, and even administrative regional staff such as school-attendance officers [34]. In addition to schools, SR interventions can take place in the home and encourage parental involvement. For instance, in Dialectical Behavior Therapy (DBT) or Cognitive Behavior Therapy (CBT), the involvement of parents is important for youth with SR to generalize what they learn in therapy to their natural home setting [35]. Finally, it is recommended that interventions for SR be adapted and/or specific to the factors underlying non-attendance [35]. For instance, if a student with SR has anxiety related to school performance, then CBT can focus on reappraising negative thoughts about academics. To effectively overcome such difficulties associated to SR and better understand its determining factors, a holistic assessment of the situation is needed.
The Relevance of a Bioecological Theory
Over the last century, several etiological theories have been put forth to explain the development of SR, each extending to prevention and intervention practices. When SR was first introduced in the early twentieth century, psychoanalytic theories were favored. Later, in the 1960s, psychodynamic and behavioral theories were put forth to explain SR. Using a behavioral lens, Kearney and Albano’s [36] functional model of school refusal behavior remains widely used by both researchers to conceptualize SR as a school attendance problem, and by stakeholders to intervene with students who manifest the behavior. However, as research on SR grows, the relevance of an ecological model that accounts for social and contextual factors has increased [3, 37, 38]. While most previous etiological theories focused primarily on the individual and proximal factors associated to youth with SR (e.g., parenting, or separation anxiety), the bioecological theory [39] emphasizes the importance of considering both proximal and distal influencing factors on development. Specifically, the different systems that it encloses (i.e., micro, meso, exo and macro) provide a holistic view of the student and the interrelations between the factors influencing their SR behavior. Moreover, the principles of the ecological model: interdependence, circulation of resources, adaptation, and succession [39] are also helpful to guide interventions for SR. By understanding the relationship between a student with SR and their environment (interdependence), the availability and distribution of resources in their school or home (circulation of resources), how well they can evolve within the school system (adaptation), and the developmental impact of their past, present and future experiences in the school or at home (succession), intervention practices can be tailored to the specific needs of the student.
Additionally, in the context of SR, previous reviews have identified associated factors in multiple systems such as schools, families and communities (e.g., [12, 38]). Empirical studies also support the influence of more distal factors such as conflicts with peers and school transitions on SR (e.g., [38, 40]). These findings coupled with previous research that supports the use of “multimodal, multisystem, and wraparound intensive team approaches” ([28], p. 122) in SR intervention, support the relevance of an ecological lens to examine SR in children and adolescents.
To date, no truly systematic review of the factors associated to school refusal, that adheres to a systematic and transparent protocol (e.g., [41,42,43]), currently exists. Moreover, existing reviews did not seek to identify factors that differentiate youth with SR from youth without SR. As a result, a systematic review with the use of an ecological lens is needed to provide a more holistic view of the factors associated to school refusal and highlight the complexity of this phenomenon. The use of this lens will provide educators and school practitioners with selective and indicated prevention guidelines to both identify students at risk of developing SR-related behaviors, but also assess which resources they may need to mobilize when supporting students displaying SR.
Accordingly, the current study uses a systematic review to critically analyze empirical literature on the factors associated to school refusal and organize it according to Bronfenbrenner’s Ecological Theory [39]. The use of this ecological model will organize findings by considering individual, school, family and more distal factors (e.g., SES, culture, etc.) that can guide practitioners when developing an intervention plan. The specific aim of the review is to provide a framework which will identify factors associated to children and/or adolescents with school refusal that distinguish them from those without school refusal.
Methods
The systematic review protocol was based on the Center for Reviews and Dissemination’s (CRD; [41]) internationally recognized guidelines. This protocol involves a series of steps to describe and complete to ensure the internal and external validity of the review [44]: (1) identification of studies, (2) selection of studies, (3) data extraction, (4) quality assessment, and (5) synthesis of findings. The methods employed for the identification of studies, the selection of studies, data extraction, and quality assessment are detailed in this section. The synthesis of findings is detailed in the results section.
Identification
References examining factors associated to school refusal were searched in education (ERIC, Education Source, CBCA Complete), health science (PubMed, MEDLINE, CINAHL), social science (Persée, PsycArticles, PsycINFO, Psychology and Behavioral Sciences Collection, SocINDEX, Social Work Abstracts), and multidisciplinary databases (FRANCIS, Érudit, CAIRN, Repère, SCOPUS, Academic Search Complete, Proquest). After multiple preliminary tests and refinements, the following keywords were used: (school refus* OR school phobia) AND (child* OR youth* OR adolescen* OR teen*). These were translated to French as needed for the databases. All possible literature up until the last search date of February 10th 2022 was considered. A database for bibliographical references (Zotero) was used to import and manage references.
Selection
Relevant peer-reviewed references were first selected through a review of titles and abstracts (phase 1), and then a review of full documents that could not be rejected after phase 1 (phase 2). References for which an abstract was not available and could not be excluded based on their title were automatically included after phase 1. References were selected at each phase based on the following five criteria: written in English or French (criterion 1), was an empirical research study (criterion 2), compared a group of children and/or adolescents with school refusal to a group without (criterion 3), identified school non-attendance (criterion 4), and identified the presence of emotional distress in participants with school refusal (criterion 5). For criterion 5, there were three possibilities considered for inclusion: (1) authors used Berg’s [2] operational model to identify school refusers which accounts for the range of psychopathology that distinguishes youth with SR from those with other attendance problems, (2) authors mentioned the presence of anxiety to identify school refusers, or (3) authors report the use of a standardized measure of anxiety to identify school refusers. Berg’s [2] original criteria were chosen rather than criteria updated in the last decade [13, 14] given that the search did not limit dates of publication. If school refusers were hospitalized, the reference was considered to have automatically fulfilled criterions 4 and 5. In each selection phase, Cohen’s Kappa was used to determine inter-rater reliability [45]. A minimum of 25% of studies (until an acceptable agreement of k = 0.8 was reached) were judged by two independent raters. Disagreements between raters were discussed and resolved by consensus. After phase 2, bibliographies of included studies were examined and notable researchers in the field were contacted to identify possible relevant additional studies.
Data Extraction
Information extracted from studies included descriptive statistics related to the sample (i.e., N, age, sex, socio-demographic distribution, and country of origin of sample), the types of groups in the sample (i.e., with SR, control, etc.), study design (cross-sectional or longitudinal), study objective, methodology employed (i.e., instruments to measure SR and associated factors), statistical analyses performed, and the results pertaining to the factors associated to school refusal. Data extraction was first performed by the first author according to a detailed extraction form. Extracted data were then synthesized in tables and organized according to the systems of the ecological model for a second rater to review for accuracy.
Quality Assessment
While multiple tools exist to assess the quality of research studies, no consensus yet exists among researchers [46]. As per Siddaway et al.’s [46] recommendations, four objective indicators of potential bias related to study design (sampling, measures and statistical analyses) and representativeness of the sample were used to produce a descriptive synthesis of the methodological quality of included studies. Results from the quality assessment were also used to provide a nuanced analysis of the findings. Given its use in empirical research (e.g., [13, 16, 17]), these included the use of Berg’s [2] definition to identify school refusers (first indicator), and the method used to measure emotional distress in school refusers (validated instrument, clinical judgment, judgment of researchers, or self-report; second indicator). Moreover, statistical rigor was measured according to analyses used (univariate or multivariate; third indicator) and the ability of each study to detect small, medium and large effect sizes respectively (fourth indicator). These calculations were done using G*Power according to sample sizes, p values and analyses performed.
Results
Study Sample
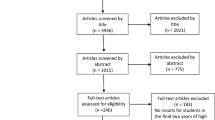
Overall, 4772 studies were identified and imported into a reference manager for further analysis. After elimination of duplicates, 2965 studies were included for phase 1 of 2 of the selection process. Figure 1 documents decisions (inclusions and exclusions) for each stage of the review. In total, 15 studies were included in the final sample.

Selection process flowchart
Study Sample Characteristics
Sample characteristics for each of the selected references are presented in Table 1. Included studies were published between 1983 and 2015. There are 13 journal articles, one thesis and one conference paper. All studies used cross-sectional designs. Samples were recruited in North (n = 5) and South America (n = 1), Europe (n = 5), Asia (n = 2) and Australia (n = 2). Samples were all convenience-based with the exception of Egger et al. [4] who examined a population-based sample. Sample sizes varied between 11 and 3629 participants. Most studies examined youth aged 6–17 years old, without distinguishing between children and adolescents. One study examined the parents of school refusers. In terms of sex, samples were mixed and relatively equivalent in number (37–68% male school refusers). Finally, most studies who reported ethnicity reflected the demographic distribution of the country in which they were recruited.
Quality Assessment
The methodological qualities of each included study are presented in Table 2. Most included studies can be qualified as being of moderate quality, specifically due to their statistical characteristics. Very few could detect small and medium effect sizes. However, Carless et al.’s [16] and Maric et al.’s [17] studies seem to be of higher quality. In addition to having been published in the last decade, these studies use Berg’s definition to identify school refusers and a validated standardized measure to evaluate the presence of emotional distress in their clinical group. Moreover, their use of multivariate analyses considers the influence of overlapping contributions between variables. Despite the presence of lower quality studies, all 15 were included in the final sample for data extraction and, when applicable, they are interpreted in light of their quality.
Factors Associated with SR
All factors examined in relation to children and/or adolescents with school refusal are presented in Table 3. This review identified 15 studies examining 67 different factors. Examined factors were mainly related to Bronfenbrenner’s ontosystem (14/15 studies), followed by the microsystem (9/15 studies), the exosystem (2/15 studies) and chronosystem (2/15 studies). No studies examined factors pertaining to Bronfenbrenner’s meso- and macro-systems. Specifically, no studies examined factors pertaining to partnerships or collaborations between youth’s microsystems (e.g., schools and families), or factors of the macrosystem pertaining to culture, customs, or the youth’s educational system for instance.
Overall, 44 individual, social and contextual factors were found to differentiate youth with SR from peers without SR. These are presented in the following sections. For each system of Bronfenbrenner’s ecological model, significant factors associated to children are presented first, followed by adolescents and factors that were not compared across age groups. When contradictions between studies exist, associated factors are also evaluated as a function of their quality.
Ontosystem (13 Studies/15)
A total of 30 ontosystemic factors were examined with 23 yielding significant differences between youth with SR and those without in at least one study.
With regards to data pertaining to children exclusively (n = 1 study), Granell de Aldaz, et al. [47] found that having a difficult personality, a diagnosis of depression, a dependency towards parents, and fears related to school were all significantly related to children with SR when compared to children without SR.
In adolescents (n = 4 studies), it was found that a diagnosis of depression or anxiety were significantly associated to students with SR (3 studies/4). Other significant associated factors include academic, social, and interpersonal concernsFootnote 2 (3 studies/4), pessimism (2 studies/4), high stress levels (1 study/4), anhedonia (1 study/4), somatic complaints (1 study/4), behavior problems (1 study/4), performance anxiety (1 study/4), difficulties with social problem solving (1 study/4), and high mathematical ability (1 study/4).
In both children and adolescents (n = 9 studies), identified associated factors include interpersonal, family, social, and academic worries (4 studies/9), somatic complaints (2 studies/9), performance anxiety (1 study/9), a diagnosis of anxiety (1 study/9), diagnosis of depression (1 study/9), fatigue (1 study/9), sleep problems (1 study/9), difficulties in processing emotional information (1 study/9), difficulties with emotional regulation (1 study/9), verbal comprehension problems (1 study/9), language problems (1 study/9), learning problems (1 study/9), and poor school performance in mathematics, reading and writing (1 study/9).
Contradictions did emerge in relation to some factors. Specifically, organic diseases were significantly associated to adolescents with SR when univariate analyses were used and the sample of youth with SR was clinically referred, and thus, potentially more severe in symptomatology [48]. However, in Egger et al. [4], no such associations were found with a community sample and when multivariate analyses were used. Age also yielded mixed results in the studies that examined developmental differences. For instance, when examining a sample of 9–16-year-olds, Egger et al. [4] found that younger children were more susceptible to develop symptoms of SR. Conversely, Maric et al. [17] found that, in a sample of 11–17-year-olds, it was older children that were more susceptible. Moreover, age was not significantly associated to SR in any way in Honjo, et al.’s [49] study. While all three studies used multivariate statistical analyses and non-clinically-referred samples of youth with SR, Maric, et al. [17] is the only one to have used a standardized measure to evaluate the presence of emotional distress in their SR sample. Finally, while a diagnosis of generalized anxiety was a significant factor in adolescents between 11 and 17 years with SR [16, 17], it seemed to not be the case for specific types of anxiety (e.g., social anxiety in students aged 9–16 years, [4]; separation anxiety, [48]).
Microsystem (9 Studies/15)
A total of 33 microsystemic factors were examined with 20 yielding significant differences between youth with SR and those without in at least 1 study. Within this section, factors are further broken down into family, school, and peer systems.
Family (6 Studies/9)
No significant factors emerged in relation to children (n = 1 study). However, in the studies that exclusively examined adolescents (n = 3 studies), family conflict (2 studies/3), dysfunctional family environments (2 studies/3), poor familial cohesion (1 study/3), and poor communication (1 study/3) distinguished adolescents with SR from those without. In addition, authoritarian parenting styles (1 study/3), relationship conflicts (1 study/3), being a young parent (1 study/3), parent psychopathology (anxiety or depression) (1 study/3), poor self-efficacy (1 study/3), and low perceived levels of caring (1/3) were significantly associated to parents of adolescents with SR when compared to those without.
Finally, for children and adolescents (n = 2 studies), the presence of parental psychopathology (2 studies/2) and the presence of an organic disease in parents (1 study/2) were significantly related to youth with SR.
Some contradictory results emerged from Adams [50] and Carless’, et al. [16] studies with regards to parents’ levels of education. While Adams [50] found that parents of adolescents with SR were significantly more educated than parents of adolescents without SR, Carless, et al. [16] did not find any significant relationship between parents’ levels of education and SR. Both studies are of similar methodological quality and recruited non-clinically referred youth with SR. However, Carless, et al. [16] used a validated instrument to measure emotional distress in their SR participants, while Adams [50] relied on parent report. Also, Carless, et al. [16] had a slightly larger medium effect size than Adams [50].
School (3 Studies/9)
No studies exclusively examined school factors in children, and no significant factors were exclusively associated to adolescents (n = 1 study) (1/3). For both children and adolescents (n = 2 studies), children with SR attended more schools with students from neighborhoods with high crime rates (1/2), and had more negative perceptions of classroom management (1/2) than those without SR.
Peers (5 Studies/9)
In children (n = 2 studies), victimization (1 study/2) and social isolation (1 study/2) were significantly associated with SR. In adolescents (n = 4 studies), social isolation (2 studies/4) and victimization (1 study/4) were also significantly associated with SR. Adolescents with SR also had significantly more difficulty using the social support (1 study/4) available to them than those without SR. Finally, in both children and adolescents (n = 1), youth with SR were significantly more timid, in conflict with others and exposed to aggressive peers than those without.
There are contradictory findings in relation to social isolation. Social isolation was significant in Granell de Aldaz, et al.’s [47] study, but it was not in Havik, et al.’s [5] study. Both studies used non-clinically referred samples, but the differences may be due to the types of analyses and measure specificity. Specifically, Granell de Aldaz, et al. [47] solely used univariate analyses with data from the Child Behavior Checklist. Conversely, Havik, et al. [5] considered interactive influences of other dependent variables on the presence of SR using multivariate analyses, and with data from the Social Isolation at School Scale which is more specific to assess the construct of social isolation.
Exosystem (2 Studies/15)
Two exosystemic factors in two separate studies (n = 2) were examined: socio-economic status and neighborhood crime. Neither factor was significantly associated with SR when compared with youth without SR.
Chronosystem (2 Studies/15)
Of the two chronosystem factors examined, one was significant (n = 2 studies). Children with SR were more likely to change schools frequently than those without.
Discussion
This systematic review identified 15 empirical studies that compared the factors associated to youth with SR to those associated to youth without SR. Factors of a psychological, social, and contextual nature were identified, thus highlighting the importance of an ecological lens with which to view SR. The majority of identified references examined proximal factors of an ontosystemic and microsystemic nature. There is also evidence that more distal factors such as non-normative transitions, notably, frequent school transitions, influence the appearance of SR. Finally, the relationship between youth with SR and their associated factors align with the principles of interdependence, resource circulation, adaptation and succession that are at the heart of the ecological model.
Psychopathology and SR
At both an individual (ontosystem) and family level (microsystem), compared with peers without SR, youth with SR and their parents were more anxious, and some were depressed. Anxiety is present in most of the youth referred for treatment for SR [18], and is known to be highly comorbid with depression in children [51] and adults [52] alike. In the reviewed references, while not all youth with SR had diagnoses of anxiety or depression, they did have characteristics that underlie both disorders [53]. Specifically, youth with SR were inflicted with worries and concerns about their academic, familial, and interpersonal life which supports interactions between these individual level factors and youth’s environmental stressors. They also had problems with emotional regulation, sleep, and presented with anhedonia.
Moreover, while specific anxiety disorders such as separation anxiety [48] and social anxiety [4] were not found to differentiate youth with and without SR, generalized anxiety disorders [16, 17] and performance anxiety were [4, 54]. This may be due to age. Bahali et al. [48] did not specify the age range of their child participants. However, they indicated in their inclusion criteria that the children had to be over 5 years-old, while separation anxiety is known to commonly afflict younger children during preschool years [55]. Conversely, Egger et al.’s [4] sample ranged from 9 to 16 years old, with a mean age of 12 for their SR sample. There is evidence to support an earlier onset of social anxiety in childhood (i.e., around age 8; [56]), but, for most, social anxiety tends to develop around 13 years of age with a mean age of onset of 15 years old [57]. This could explain why Egger et al. [4] did not detect a significant presence of social anxiety in their sample. However, given that performance anxiety is a type of social anxiety when it pertains to social or interpersonal performance [53], significant findings in Egger et al.’s [4] and Ficula et al.’s [54] studies with adolescents could hint at a possible association between SR and subtypes of social anxiety. Nonetheless, symptoms of these disorders, such as concerns associated to academic, social and family life, can be delt with when observed by school practitioners through current common interventions for anxiety that account for interactions between symptoms of these disorders and the student’s family and school environments.
Most successful interventions for children and adolescents with anxiety include CBT-based approaches [58]. The same is true for selective and indicative school-based interventions for anxiety which generally involve CBT strategies and target school-based stress and anxiety [59, 60]. In the context of SR, it is important that the strategies used are adapted to the specific factors underlying students’ non-attendance [35]. For instance, activities on negative thought reappraisal should be adapted according to whether the root of students’ anxieties concern academic, family or interpersonal issues. In addition, if family concerns are at the root of their anxieties, school practitioners can consider involving parents as partners. Notably, it is often preferred to include parents as partners, not only because it shares the responsibilities of care. It is also consistent with the principle of resource circulation in the ecological model, whereby collaboration can increase the generalizability of interventions [31]. Parental accommodation can also be integrated wherein parents can engage in certain behaviors and avoid others in efforts to reduce their child’s distress [61].
Regarding the family microsystem, compared to peers without SR, youth with SR are more likely to have parents with a history of psychopathology. Anxiety is well known to be subject to intergenerational transmission [48] and could be the way in which youth with SR develop their own symptoms of anxiety or depression. However, in line with the ecological principle of interdependence, parents of youth with SR may have low self-efficacy which can interact with youth with SR in different ways. For instance, youth with SR have perhaps learned low self-efficacy themselves through parental modelling (Social Learning Theory; [62]). Another possibility is that their parents themselves may have poor coping mechanisms to deal with their children’s SR, and their problem persists [16]. Through this lens, the development of SR can be seen as interdependent with parenting models and follow the principle of succession. Children’s previous experiences may have led to the development of poor coping mechanisms which, in turn, may act as a barrier when dealing with current experiences of school-related adversities such as transitions to new communities, or being exposed to criminal activities. In this regard, compared to peers without SR, youth with SR attend schools that serve students from neighborhoods with higher rates of poverty and community violence and are known to change schools often. Their ability to adapt to these non-normative transitions might impact the development of SR as it is suggested to be the case with other stressful life events (e.g., divorce, peer conflict, etc. [48]).
If permitted by the availability of resources, partnership-based interventions may be especially beneficial when youth with SR present with underlying family factors. These can be structural by involving parents in direct activities that engage them in students’ learning, or relational by involving parents in their children’s learning through regular communication [30]. Direct parental involvement in intervention through a structural partnership can be a facilitator to attendance for youth with SR who have difficulties leaving home in the morning, because parents can facilitate their children’s transition to school through strategies they learn from a school partner. Moreover, parents can engage in family-based CBT and gain tools for modelling adaptive coping mechanisms for their children with SR [58]. While not all parents may have the time and resources to engage in active structural partnerships, both structural and relational partnerships have been shown to increase consistency in interventions [30].
Learning and SR
Compared with peers without SR, youth with SR are more likely to have diverse learning needs. Some had problems with verbal comprehension, language, and poor academic achievement in mathematics, reading and writing. It is possible that these factors are influenced by the ecological principle of adaptation which is defined as an individual’s ability to evolve within their different systems [39]. Specifically, SR may develop because they have difficulties adapting to the challenges of their academic work. These students may have underlying worries that lead to maladaptive coping mechanisms. It is also possible that they have missed too many classes and have fallen behind on work. As a result, special attention should be given to youth with learning difficulties and high rates of absences. Web-based therapy for SR [31] can be a good place to begin intervention with these students.
Through web-based therapy, students with SR can receive coaching such as DBT from the comfort of their homes. This is beneficial because it allows children to gradually be exposed to school stressors while remaining in a non-anxious environment. Additionally, in Chu et al.’s [31] multimodal approach, parents were included in daily therapy sessions that occurred in the mornings, when the likelihood youth would refuse to leave home for school was highest. As a result, the dose, timeliness, and context of the students’ natural environment were facilitators to increase the likelihood of attendance [31]. Remote tutoring can also be done with these students to increase their sense of readiness for school. Finally, tutoring and academic support can be offered as a form of selective prevention to students who present with learning difficulties but are still attending class.
Microsystems within the school itself also seem to influence the development of SR. Compared with peers without SR, youth with SR have poor perceptions of classroom management from teachers. This can be problematic if they do not perceive that they have support from their teachers [5], especially in cases of victimization and social conflict which are also more associated to youth with SR more than those without. If youth do not feel like they have support to deal with these issues within the school this may interact with their poor coping mechanisms to deal with social conflict [63], and youth’s feelings of a lack of support may become a barrier to school attendance.
When youth with SR present with school-related barriers, interventions that allow for generalization to the school context might be most beneficial. This can include selective prevention in the form of school-based group CBT [60]. Specifically, this form of intervention can include exposure by being delivered gradually in the school-setting, and strategies and opportunities to practice conflict resolution for instance. In this sense, the student with SR is not only learning adaptive social strategies to deal with stressors at school but is also gradually generalizing the use of those tools to their school-setting.
Future Directions for SR Research and Limitations
Overall, this review shed light on how more proximal systems of the ecological model can be applied as a lens with which to understand the complex symptomatology of youth with SR. Specifically, the ecological model highlighted the presence of individual, social and contextual factors and provided insight into how factors from different environments might interact to influence the development of SR-related symptoms. However, a deeper understanding of distal factors is needed to address the nature of interrelations between factors as well as additional interactions with proximal level factors. It remains unclear how bidirectional influences exist between different microsystems (e.g., mesosystem), and also how macro- or exo-system factors interact with proximal factors in the appearance of SR symptoms. For instance, with regards to the mesosystem, future studies could consider examining the quality of the interactions between schools and families. Given that youth with SR tend to have families with a history of psychopathology, which can act as a barrier to support, research on home-school partnerships can shed light on facilitators to collaboration and communication between parents and schools in the context of SR.
While exosystemic factors were examined, socio-economic status (SES) and neighborhoods did not significantly differentiate youth with SR from youth without. However, given that factors such as SES, but also including race, age and sex, are known to moderate the efficacy of school-based CBT interventions [59], more research using standardized methodology and assessments of SR is needed to further understand the contribution of exosystemic factors. Moreover, other distal factors such as educational curriculums and educational policy have been shown to impact school climate, mental health and adaptation to transitions between primary and secondary school [64]. It is possible that they influence school engagement, academic achievement, perceptions of classroom management and other school factors that differentiate youth with SR from youth without.
With regards to the macrosystem, while the studies included in this review originated from countries in Europe, North America, South America and Asia, global differences were not examined. Future research should examine cultural differences in how SR is conceptualized to develop diverse and inclusive SR interventions globally. Moreover, the cultural value of education has been shown to impact performance expectations of achievement [65,66,67]. If performance is highly valued, youth might feel more pressure and more anxiety towards academic achievement, and thus develop SR-related factors such as performance anxiety. As a result, specific geographic differences could be examined in future research to account for cultural differences in school systems that might underlie SR.
Moreover, it is important to note that only cross-sectional studies that compared groups with and without SR were identified in this systematic review. As a result, it is not possible to know the specific types of associated factors identified (e.g., risk, precipitating, maintenance, consequence, etc.), their causal relationship with SR, or the dynamic relationships at the forefront of Bronfenbrenner’s ecological model. Future longitudinal research is needed to identify specific risk factors associated with the development of SR. Longitudinal research could also highlight developmental patterns associated with the appearance of SR, potential continuous dimensions of SR, and how they differ from other SAPs. The heterogeneity of studies identified in terms of factors and methodological characteristics limits the generalizability of the findings. Specifically, the studies examined 67 different factors, and used different methods to measure the presence of emotional distress underlying SR. As presented in Table 2, these methods were not always standardized or reliable. While determinant profiles exist to distinguish school attendance problems [3, 68], one solution to the heterogeneity of factors associated to youth with SR would also be the development of SR profiles through latent class analysis. This way, we may be able to better identity youth with different presentations of SR and better able to identify their underlying intervention needs. In addition, the identified studies date between 1983 and 2015 and might not reflect the reality of youth with SR in today’s reality and the impact of additional contextual factors such as digital media and digital literacy in the classroom. For instance, during the COVID-19 pandemic, remote learning has led some students to feel socially isolated and present more mental health issues [69, 70]. For students with SR, remote learning may have been a facilitator to school attendance for those with underlying psychopathology such as a performance anxiety subtype of social anxiety, but may have been an added barrier for students with learning difficulties. Future research is needed to further clarify the impact of remote learning on both the factors associated to SR and schools’ ability to monitor attendance and identify students with SR. In addition, most of these studies were conducted with WEIRD samples [71], which further limits the generalizability of these findings. Finally, considering the limited number of studies that compare youth with SR to youth without SR, future research is needed to highlight the developmental mechanisms underlying SR to help school practitioners identify youth with this type of attendance problem early and to differentiate potential presentations at different ages.
Conclusions
This study was the first to systematically review existing literature on the factors that differentiate youth with SR from youth without SR. It is an important step forward in understanding how to implement an ecological approach to assessment and intervention for youth with SR. Overall, the use of an ecological model allowed for a holistic view of the factors underlying SR in youth. This facilitates the development of intervention plans that can rely on multisystem and intensive team approaches to tackle SR [28], as well as orient psychosocial interventions from which youth with SR are known to benefit from Maynard et al. [18]. Accordingly, our review points towards the relevance to focus on modifiable factors from different ecological systems and, when applicable, to gather the expertise of practitioners from these different systems (i.e., parents in addition to educators) to provide a well-rounded intervention plan. In terms of selective prevention, special attention should be made towards students presenting with diverse learning needs and characteristics that underlie anxiety and depression before attendance begins to drop. For indicative prevention, school practitioners can focus on increasing attendance [18] by providing support in areas of academic achievement, social interactions, emotional distress and teacher-student relations. Further research is needed that examines the differences between factors present in youth with and without SR, particularly longitudinal research that highlight profiles of youth that are susceptible to developing SR. Such research can provide additional insight for school practitioners to develop equitable, diverse and inclusive interventions for students with SR.
Summary
School refusal is a school attendance problem characterized by emotional distress [3]. While the emotional and behavioral difficulties of youth with anxious school refusal are usually evident, the specific factors associated to them are not [28]. To provide a more holistic view of school refusal, the current study relied on both the principles and systems of Bronfenbrenner’s [39] ecological model. Through this ecological lens, this systematic review examined the factors that differentiated children and adolescents with school refusal from those without. Based on the Center for Reviews and Dissemination’s (CRD; [41]) internationally recognized guidelines, the review identified 15 studies comparing youth with and without school refusal and examining 67 different factors. Fourty-four individual, social and contextual factors that differentiate youth with school refusal from peers without school refusal were identified. The centrality of anxiety, or anxiety-related symptoms, and diverse learning needs were highlighted as main points of contrast between youth with school refusal and those without. In accordance with the findings and principles of the ecological model, recommendations were made for the inclusion of multiple stakeholders (e.g., parents in addition to teachers or school practitioners) in intervention for school refusal. Future longitudinal research is needed to gain insight into a developmental understanding of the profiles of youth that are more likely to develop anxious forms of school refusal.
Notes
The term «youth» is used to refer to school-aged children between the ages of 5 and 17.
It is important to note that while some factors such as dependency towards parents, and interpersonal concerns, are of an interpersonal nature due to their association with relationships with others, they were considered to be of an ontosystemic nature because they qualify an individual rather than contextual characteristic by how it is measured (e.g., the Child Behavior Checklist).
References
References marked with an asterisk indicate documents identified in the review
Berg I (1997) School refusal and truancy. Arch Dis Child 76:90–91. https://doi.org/10.1136/adc.76.2.90
Berg I (2002) School avoidance, school phobia, and truancy. In: Lewis M (ed) Child and adolescent psychiatry: a comprehensive textbook. Lippincott Williams et Wilkins, Sydney, pp 1260–1266
Heyne D, Landell MG, Melvin GA, Gentle-Genitty CS (2019) Differentiation between school attendance problems: why and how? Cogn Behav Pract 26:8–34. https://doi.org/10.1016/j.cbpra.2018.03.006
*Egger HL, Costello EJ, Angold A (2003) School refusal and psychiatric disorders: a community study. J Am Acad Child Adolesc Psychiatry 42:797–807. https://doi.org/10.1097/01.chi.0000046865.56865.79
*Havik T, Bru E, Ertesvag SK (2015) School factors associated with school refusal-and truancy-related reasons for school non-attendance. Sch Psychol Educ 18:221–240. https://doi.org/10.1007/s11218-015-9293-y
Heyne D, King NJ (2004) Treatment of school refusal. In: Barrett PM, Ollendick TH (eds) Handbook of interventions that work with children and adolescents: prevention and treatment. Wiley, West Sussex, pp 243–273. https://doi.org/10.1002/9780470753385.ch11
Broadwin IT (1932) A contribution to the study of truancy. J Orthopsychiatry 2:253–259. https://doi.org/10.1111/j.1939-0025.1932.tb05183.x
Partridge JM (1939) Truancy. Br J Psychiatry 85:45–81. https://doi.org/10.1192/bjp.85.354.45
Johnson AM, Falstein EI, Szurek SA, Svendson M (1941) School phobia. Am J Orthopsychiatry 11:702–711. https://doi.org/10.1111/j.1939-0025.1941.tb05860.x
Hersov L (1960) School phobia. BMJ 2:1017. https://doi.org/10.1136/bmj.2.5204.1017
Hersov L (1960) Refusal to go to school. J Child Psychol Psychiatry 1:137–145. https://doi.org/10.1111/j.1469-7610.1960.tb01988.x
Thambirajah MS, Grandison KJ, De-Hayes L (2008) Understanding school refusal: a handbook for professionnals in education, health and social care. Jessica Kingsley Publishers, London
Heyne D, Sauter FM, Van Widenfelt BM, Vermeiren R, Westenberg PM (2011) School refusal and anxiety in adolescence: non-randomized trial of a developmentally sensitive cognitive behavioral therapy. J Anxiety Disord 25:870–878. https://doi.org/10.1016/j.janxdis.2011.04.006
Maric M, Heyne D, MacKinnon DP, Van Widenfelt BM, Westenberg PM (2013) Cognitive mediation of cognitive-behavioral therapy outcomes for anxiety-based school refusal. Behav Cogn Psychother 41:549–564. https://doi.org/10.1017/S1352465812000756
Gallé-Tessonneau M, Gana K (2019) Development and validation of the school refusal evaluation scale for adolescents. J Pediatr Psychol 44:153–163. https://doi.org/10.1093/jpepsy/jsy061
*Carless B, Melvin GA, Tonge BJ, Newman LK (2015) The role of parental self-efficacy in adolescent school-refusal. J Fam Psychol 29:162–170. https://doi.org/10.1037/fam0000050
*Maric M, Heyne D, de Heus P, Van Widenfelt BM, Westenberg PM (2012) The role of cognition in school refusal: an investigation of automatic thoughts and cognitive errors. Behav Cogn Psychother 40:255–269. https://doi.org/10.1017/s1352465811000427
Maynard BR, Heyne D, Brendel KE, Bulanda JJ, Thompson AM, Pigott TD (2018) Treatment for school refusal among children and adolescents: a systematic review and meta-analysis. Res Soc Work Pract 28:56–67. https://doi.org/10.1177/1049731515598619
Christle CA, Jolivette K, Nelson CM (2007) School characteristics related to high school dropout rates. Remedial Speci Educ 28:325–339. https://doi.org/10.1177/07419325070280060201
Heyne D, Rollings S (2002) School refusal. Blackwell Publishing, Oxford
Carroll HCM (2010) The effect of pupil absenteeism on literacy and numeracy in primary school. Sch Psychol Int 31:115–130. https://doi.org/10.1177/0143034310361674
Kearney CA (2008) School absenteeism and school refusal behavior in youth: a contemporary review. Clin Psychol Rev 28:451–471. https://doi.org/10.1016/j.cpr.2007.07.012
Flakierska-Paquin N, Lindstrom M, Gillberg C (1997) School phobia with separation anxiety disorder: a comparative 20- to 29-year follow-up on 35 school refusers. Br J Psychiatry 38:17–22. https://doi.org/10.1016/s0010-440x(97)90048-1
McCune N, Hynes J (2005) Ten year follow-up of children with school refusal. Ir J Psychol Med 22:56–58. https://doi.org/10.1017/s0790966700008946
Hancock KJ, Shepherd CCJ, Lawrence D, Zubrick SR (2013) Student attendance and educational outcomes: every day counts. Report for the Department of Education, Employment and Workplace Relations, Canberra
Heyne D (2019) Developments in classification, identification, and intervention for school refusal and other attendance problems: introduction to the special series. Cogn Behav Pract 26:1–7. https://doi.org/10.1016/j.cbpra.2018.12.003
Martin R, Benoit JP, Moro MR, Benoit L (2020) School refusal or truancy? A qualitative study of misconceptions among school personnel about absenteeism of children from immigrant families. Front Psychiatry 11:1–16. https://doi.org/10.3389/fpsyt.2020.00202
Tonge BJ, Silverman WK (2019) Reflections on the field of school attendance problems: for the times they are a-changing? Cogn Behav Pract 26:119–126. https://doi.org/10.1016/j.cbpra.2018.12.004
Conroy K, Hong N, Poznanski B, Hart KC, Ginsburg GS, Fabiano GA, Comer JS (2021) Harnessing home-school partnerships and school consultation to support youth with anxiety. Cogn Behav Pract. https://doi.org/10.1016/j.cbpra.2021.02.007
Smith TE, Sheridan SM, Kim EM, Park S, Beretvas SN (2020) The effects of family-school partnership interventions on academic and social-emotional functioning: a meta-analysis exploring what works for whom. Educ Psychol Rev 32:511–544. https://doi.org/10.1007/s10648-019-09509-w
Chu BC, Rizvi SL, Zendegui EA, Bonavita-cola L (2015) Dialectical behavior therapy for school refusal: treatment development and incorporation of web-based coaching. Cogn Behav Pract 22:317–330. https://doi.org/10.1016/j.cbpra.2014.08.002
McKay-Brown L, McGrath R, Dalton L, Graham L, Smith A, Ring J, Eyre K (2019) Reengagement with education: a multidisciplinary home-school-clinic approach developed in Australia for school-refusing youth. Cogn Behav Pract 26:92–106. https://doi.org/10.1016/j.cbpra.2018.08.003
Reissner V, Knollman M, Spie S, Jost D, Neumann A, Hebebrand J (2019) Modular treatment for children and adolescents with problematic school absenteeism: development and description of a program in Germany. Cogn Behav Pract 26:63–74. https://doi.org/10.1016/j.cbpra.2018.07.001
Brouwer-Borghuis ML, Heyne D, Sauter FM, Scholte RH (2019) The link: an alternative educational program in the Netherlands to reengage school-refusing adolescents with schooling. Cogn Behav Pract 26:75–91. https://doi.org/10.1016/j.cbpra.2018.08.001
Elliot JG, Place M (2019) Practitioner review: school refusal: developments in conceptualisation and treatment since 2000. J Child Psychol Psychiatry 60:4–15. https://doi.org/10.1111/jcpp.12848
Kearney CA, Albano AM (2007) When children refuse school: a cognitive-behavioral therapy approach, 2nd edn. Oxford University Press, New York
Chu BC, Guarino D, Mele C, O’Connell J, Coto P (2019) Developing an online early detection system for school attendance problems: results from a research-community partnership. Cogn Behav Pract 26:35–45
Ingul JM, Havik T, Heyne D (2019) Emerging school refusal: a school-based framework for identifying early signs and risk factors. Cogn Behav Pract 26:46–62. https://doi.org/10.1016/j.cbpra.2018.03.005
Bronfenbrenner U (1979) The ecology of human development. Harvard University Press, Cambridge
Havik T, Bru E, Ertesvag SK (2014) Parental perspectives of the role of school factors in school refusal. Emot Behav Diffic 19:131–153. https://doi.org/10.1080/13632752.2013.816199
Center for Reviews and Dissemination (2009) Systematic reviews. CRD’s guidance for undertaking reviews in health care. University of York. http://www.york.ac.uk/inst/crd/index_guidance.htm
Gough D, Oliver S, Thomas J (eds) (2017) An introduction to systematic reviews. Sage, Thousand Oaks
Uman LS (2011) Systematic reviews and meta-analyses. J Can Acad Child Adolesc Psychiatry 20:57–59
Pelham BW, Blanton H (2018) Conducting research in psychology: measuring the weight of smoke. SAGE Publications, Thousand Oaks
Cohen J (1988) Statistical power for the behavioral sciences, 2e éd. Lawrence Erlbaum Associates, Hillsdale
Siddaway A, Wood AM, Hedges LV (2019) How to do a systematic review: a best practice guide for conducting and reporting narrative reviews, meta-analyses, and meta-syntheses. Annu Rev Psychol 70:747–770. https://doi.org/10.1146/annurev-psych-010418-102803
*Granell de Aldaz E, Feldman L, Vivas E, Gelfand DM (1987) Characteristics of Venezuelan school refusers: toward the development of a high-risk profile. J Nerv Ment Dis 175:402–407. https://doi.org/10.1097/00005053-198707000-00003
*Bahali K, Tahiroglu AY, Avci A, Seydaoglu G (2011) Parental psychological symptoms and familial risk factors of children and adolescents who exhibit school refusal. East Asian Arch Psychiatry 21:164–169
*Honjo S, Nishide T, Niwa S, Sasaki Y, Kaneko H, Inoko K, Nishide Y (2001) School refusal and depression with school inattendance in children and adolescents: comparative assessment between the Children’s Depressive Inventory and somaric complaints. Psychiatry Clin Neurosci 55:629–634. https://doi.org/10.1046/j.1440-1819.2001.00916.x
*Adams (1997) School refusal and parental bonding: a study of characteristics and typologies. Ann Arbor University, Faculty of Political and Social Science of the New School for Social Research, Doctoral thesis
Vasileva M, Graf RK, Reinelt T, Petermann U, Petermann F (2021) Research review: a meta-analysis of the international prevalence and comorbidity of mental disorders in children between 1 and 7 years. J Child Psychol Psychiatry 62:372–381. https://doi.org/10.1111/jcpp.13261
Jacobson NC, Newman MG (2017) Anxiety and depression as bidirectional risk factors for one another: a meta-analysis of longitudinal studies. Psychol Bull 143:1155–1200. https://doi.org/10.1037/bul0000111
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Association, Washington, D.C. https://doi.org/10.1176/appi.books.9780890425596
*Ficula TV, Gelfand DM, Richards G, Ulloa A (1983) Factors associated with school refusal in adolescents. Research report published at the American Psychological Association Meeting, 1–19
Battaglia M, Touchette É, Garon-Carrier G, Dionne G, Côté SM, Vitaro F, Tremblay RE, Boivin M (2016) Distinct trajectories of separation anxiety in the preschool years: persistence at school entry and early-life associated factors. J Child Psychol Psychiatry 57:39–46. https://doi.org/10.1111/jcpp.12424
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 62:593–602. https://doi.org/10.1001/archpsyc.62.6.593
Khalid-Khan S, Santibanez MP, McMicken C, Rynn MA (2007) Social anxiety disorder in children and adolescents. Pediatr Drugs 9:227–237. https://doi.org/10.2165/00148581-200709040-00004
Higa-McMillan CK, Francis SE, Rith-Najarian L, Chorpita BF (2016) Evidence base update: 50 years of research on treatment for child and adolescent anxiety. J Clin Child Adolesc Psychol 45:91–113. https://doi.org/10.1080/15374416.2015.1046177
Feiss R, Dolinger SB, Merritt M, Reiche E, Martin K, Yanes JA et al (2019) A systematic review and meta-analysis of school-based stress, anxiety, and depression prevention programs for adolescents. J Youth Adolesc 48:1668–1685. https://doi.org/10.1007/s10964-019-01085-0
Gee B, Reynolds S, Carroll B, Orchard F, Clarke T, Martin D et al (2020) Practitioner review: effectiveness of indicated school-based interventions for adolescent depression and anxiety—a meta-analytic review. J Child Psychol Psychiatry 61:739–756. https://doi.org/10.1111/jcpp.13209
Norman KR, Silverman WK, Lebowitz ER (2015) Family accommodation of child and adolescent anxiety: mechanisms, assessment, and treatment. J Child Adolesc Psychiatr Nurs 28:131–140. https://doi.org/10.1111/jcap.12116
Bandura A, McLelland C (1977) Social learning theory. Prentice Hall, Englewood Cliffs
*Place M, Hulsmeier J, Davis S, Taylor E (2002) The coping mechanisms of children with school refusal. J Res Spec Educ Needs. https://doi.org/10.1111/j.1471-3802.2002.00167.x
Lester L, Cross D (2015) The relationship between school climate and mental and emotional wellbeing over the transition from primary to secondary school. Psychol Well-Being 5:1–15. https://doi.org/10.1186/s13612-015-0037-8
Danisman S (2017) The effect of parent involvement on student achievement. In: Karadag E (ed) The factors affecting student achievement. Spring, Cham
Li W, Xie Y (2020) The influence of family background on educational expectations: a comparative study. Chin Sociol Rev 52:269–294. https://doi.org/10.1080/21620555.2020.1738917
Pearce RR (2006) Effects of cultural and social structural factors on the achievement of white and Chinese American students at school transition points. Am Educ Res J 43:75–101. https://doi.org/10.3102/00028312043001075
Gonzalvez C, Kearney CA, Jiménez-Ayala CE, Sanmartin R, Vicent M, Inglés CJ, Garcìa-Fernandez JM (2018) Functional profiles of school refusal behavior and their relationship with depression, anxiety and stress. Psychiatry Res 269:140–144. https://doi.org/10.1016/j.psychres.2018.08.069
Creswell C, Shum A, Pearcey S, Skripkauskaite S, Patalay P, Waite P (2021) Young people’s mental health during the COVID-19 pandemic. Lancet Child Adolesc Health 5:535–537. https://doi.org/10.1016/S2352-4642(21)00177-2
Ma L, Mazidi M, Li K, Li Y, Chen S, Kirwan R et al (2021) Prevalence of mental health problems among children and adolescents during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord 293:78–89. https://doi.org/10.1016/j.jad.2021.06.021
Henrich J, Heine SJ, Norenzayan A (2010) The weirdest people in the world? Behav Brain Sci 33:61–83
*Cooper M (1984) Self-identity in adolescent school refusers and truants. Educ Rev 36:229–237. https://doi.org/10.1080/0013191840360302
*Foreman DM, Dover SJ, Hill AB (1997) Emotional and semantic priming as a measure of information processing in young people with school refusal: a research note. J Child Psychol Psychiatry 38:855–860. https://doi.org/10.1111/j.14697610.1997.tb01603.x
*Hughes EK, Gullone E, Dudley A, Tonge B (2009) A case–control study of emotion regulation and school refusal in children and adolescents. J Early Adolesc 30:691–706. https://doi.org/10.1177/0272431609341049
*Naylor MW, Stastowski M, Kenney MC, King CA (1994) Language disorders and learning disabilities in school-refusing adolescents. J Am Acad Child Adolesc Psychiatry 33:1331–1337. https://doi.org/10.1097/00004583-199411000-00016
*Tomoda A, Miike T, Yonamine K, Adachi K, Shiraishi S (1997) Disturbed circadian core body temperature rhythm and sleep disturbance in school refusal children and adolescents. Biol Psychiat 41:810–813. https://doi.org/10.1016/s0006-3223(96)00179-5
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Leduc, K., Tougas, AM., Robert, V. et al. School Refusal in Youth: A Systematic Review of Ecological Factors. Child Psychiatry Hum Dev (2022). https://doi.org/10.1007/s10578-022-01469-7
Accepted:
Published:
DOI: https://doi.org/10.1007/s10578-022-01469-7