
Abstract
Purpose
This study compared outcomes between end-to-end anastomosis and other anastomotic configurations after intestinal resection for patients with Crohn’s disease by using meta-analytical techniques.
Methods
Comparative studies published between 1992 and 2005 of end-to-end anastomosis vs. other anastomotic configurations were included. Using a random effects model, end points evaluated were short-term complications and perianastomotic recurrence of Crohn’s disease. Heterogeneity was assessed and sensitivity analysis was performed to account for bias in patient selection.
Results
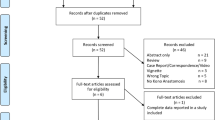
Eight studies (2 prospective, randomized, controlled trials; 1 nonrandomized, prospective; 5 nonrandomized, retrospective studies) reported on 661 patients who underwent 712 anastomoses, of which 383 (53.8 percent) were sutured end-to-end anastomosis and 329 (46.2 percent) were other anastomotic configurations (259 stapled side-to-side, 59 end-to-side or side-to-end, 11 stapled circular end-to-end). Anastomotic leak rate was significantly reduced in the other anastomotic configurations group (odds ratio (OR), 4.37; P = 0.02) and remained significantly lower in studies comparing only side-to-side anastomosis vs. end-to-end anastomosis (OR, 4.37; P = 0.02) and studies including only ileocolonic anastomosis (OR, 3.8; P = 0.05). Overall postoperative complications (OR, 2.64; P < 0.001), complications other than anastomotic leak (OR, 1.89; P = 0.04), and postoperative hospital stay (weighted mean difference, 2.81; P = 0.007) were significantly reduced in the side-to-side anastomosis group when considering studies comparing only side-to-side anastomosis vs. end-to-end anastomosis. There was no significant difference between the groups in perianastomotic recurrence and reoperation needed because of perianastomotic recurrence.
Conclusions
End-to-end anastomosis after resection for Crohn’s disease may be associated with increased anastomotic leak rates. Side-to-side anastomosis may lead to fewer anastomotic leaks and overall postoperative complications, a shorter hospital stay, and a perianastomotic recurrence rate comparable to end-to-end anastomosis. Further randomized, controlled trials should be performed for confirmation.




Similar content being viewed by others


References
Loftus EV Jr, Silverstein MD, Sandborn WJ, Tremaine WJ, Harmsen WS, Zinsmeister AR. Crohn’s disease in Olmsted County, Minnesota, 1940–1993: incidence, prevalence, and survival. Gastroenterology 1998;114:1161–8
Ekbom A, Helmick C, Zack M, Adami HO. The epidemiology of inflammatory bowel disease: a large, population-based study in Sweden. Gastroenterology 1991;100:350–8.
Bernstein CN, Nabalamba A. Hospitalization, surgery, and readmission rates of IBD in Canada: a population-based study. Am J Gastroenterol 2006;101:110–8.
Cohen RD, Larson LR, Roth JM, Becker RV, Mummert LL. The cost of hospitalization in Crohn’s disease. Am J Gastroenterol 2000;95:524–30.
Munkholm P, Langholz E, Davidsen M, Binder V. Intestinal cancer risk and mortality in patients with Crohn’s disease. Gastroenterology 1993;105:1716–23.
Bernell O, Lapidus A, Hellers G. Risk factors for surgery and postoperative recurrence in Crohn’s disease. Ann Surg 2000;231:38–45.
Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology 1990;99:956–63
Olaison G, Smedh K, Sjodahl R. Natural course of Crohn’s disease after ileocolic resection: endoscopically visualised ileal ulcers preceding symptoms. Gut 1992;33:331–5.
Michelassi F, Balestracci T, Chappell R, Block GE. Primary and recurrent Crohn’s disease. Experience with 1379 patients. Ann Surg 1991;214:230–40.
Goldberg PA, Wright JP, Gerber M, Claassen R. Incidence of surgical resection for Crohn’s disease. Dis Colon Rectum 1993;36:736–9.
Cameron JL, Hamilton SR, Coleman J, Sitzmann JV, Bayless TM. Patterns of ileal recurrence in Crohn’s disease. A prospective randomized study. Ann Surg 1992;215:546–52.
Rutgeerts P, Geboes K, Vantrappen G, Kerremans R, Coenegrachts JL, Coremans G. Natural history of recurrent Crohn’s disease at the ileocolonic anastomosis after curative surgery. Gut 1984;25:665–72.
Tytgat GN, Mulder CJ, Brummelkamp WH. Endoscopic lesions in Crohn’s disease early after ileocecal resection. Endoscopy 1988;20:260–2.
Yamamoto T. Factors affecting recurrence after surgery for Crohn’s disease. World J Gastroenterol 2005;11:3971–9
Raab Y, Bergstrom R, Ejerblad S, Graf W, Pahlman L. Factors influencing recurrence in Crohn’s disease. An analysis of a consecutive series of 353 patients treated with primary surgery. Dis Colon Rectum 1996;39:918–25
Sachar DB, Wolfson DM, Greenstein AJ, Goldberg J, Styczynski R, Janowitz HD. Risk factors for postoperative recurrence of Crohn’s disease. Gastroenterology 1983;85:917–21.
Chardavoyne R, Flint GW, Pollack S, Wise L. Factors affecting recurrence following resection for Crohn’s disease. Dis Colon Rectum 1986;29:495–502.
Wettergren A, Christiansen J. Risk of recurrence and reoperation after resection for ileocolic Crohn’s disease. Scand J Gastroenterol 1991;26:1319–22.
Sutherland LR, Ramcharan S, Bryant H, Fick G. Effect of cigarette smoking on recurrence of Crohn’s disease. Gastroenterology 1990;98:1123–8.
Cottone M, Rosselli M, Orlando A, et al. Smoking habits and recurrence in Crohn’s disease. Gastroenterology 1994;106:643–8.
Caprilli R, Corrao G, Taddei G, Tonelli F, Torchio P, Viscido A. Prognostic factors for postoperative recurrence of Crohn’s disease. Gruppo Italiano per lo Studio del Colon e del Retto (GISC). Dis Colon Rectum 1996;39:335–41.
Brignola C, Cottone M, Pera A, et al. Mesalamine in the prevention of endoscopic recurrence after intestinal resection for Crohn’s disease. Italian Cooperative Study Group. Gastroenterology 1995;108:345–9.
McLeod RS, Wolff BG, Steinhart AH, et al. Prophylactic mesalamine treatment decreases postoperative recurrence of Crohn’s disease. Gastroenterology 1995;109:404–13
Yamamoto T, Bain IM, Mylonakis E, Allan RN, Keighley MR. Stapled functional end-to-end anastomosis versus sutured end-to-end anastomosis after ileocolonic resection in Crohn disease. Scand J Gastroenterol 1999;34:708–13.
Yamamoto T, Allan RN, Keighley MR. Strategy for surgical management of ileocolonic anastomotic recurrence in Crohn’s disease. World J Surg 1999;23:1055–61
Munoz-Juarez M, Yamamoto T, Wolff BG, Keighley MR. Wide-lumen stapled anastomosis vs. conventional end-to-end anastomosis in the treatment of Crohn’s disease. Dis Colon Rectum 2001;44:20–6.
Hashemi M, Novell JR, Lewis AA. Side-to-side stapled anastomosis may delay recurrence in Crohn’s disease. Dis Colon Rectum 1998;41:1293–6.
Ikeuchi H, Kusunoki M, Yamamura T. Long-term results of stapled and hand-sewn anastomoses in patients with Crohn’s disease. Dig Surg 2000;17:493–6.
Resegotti A, Astegiano M, Farina EC, et al. Side-to-side stapled anastomosis strongly reduces anastomotic leak rates in Crohn’s disease surgery. Dis Colon Rectum 2005;48:464–8.
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomised controlled trials: the QUOROM Statement. Onkologie 2000;23:597–602.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177–88.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629–34.
Yusuf S, Peto R, Lewis J, Collins R, Sleight P. Beta blockade during and after myocardial infarction: an overview of the randomized trials. Prog Cardiovasc Dis 1985;27:335–71.
Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 1959;22:719–48.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses. Presented at 3rd symposium on systematic reviews: beyond the basics. Oxford, 2000
Taggart DP, D’Amico R, Altman DG. Effect of arterial revascularisation on survival: a systematic review of studies comparing bilateral and single internal mammary arteries. Lancet 2001;358:870–5.
Athanasiou T, Al-Ruzzeh S, Kumar P, et al. Off-pump myocardial revascularization is associated with less incidence of stroke in elderly patients. Ann Thorac Surg 2004;77:745–53.
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials 1996;17:1–12
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg 2003;73:712–6.
Smedh K, Andersson M, Johansson H, Hagberg T. Preoperative management is more important than choice of sutured or stapled anastomosis in Crohn’s disease. Eur J Surg 2002;168:154–7.
Egger M, Smith GD. Misleading meta-analysis. BMJ 1995;311:753–4.
Moskovitz D, McLeod RS, Greenberg GR, Cohen Z. Operative and environmental risk factors for recurrence of Crohn’s disease. Int J Colorectal Dis 1999;14:224–6
Scott NA, Sue-Ling HM, Hughes LE. Anastomotic configuration does not affect recurrence of Crohn’s disease after ileocolonic resection. Int J Colorectal Dis 1995;10:67–9.
Kusunoki M, Ikeuchi H, Yanagi H, Shoji Y, Yamamura T. A comparison of stapled and hand-sewn anastomoses in Crohn’s disease. Dig Surg 1998;15:679–82
Frieri G, Pimpo MT, Palumbo G, et al. Anastomotic configuration and mucosal 5-aminosalicyclic acid (5-ASA) concentrations in patients with Crohn’s disease: a GISC study. Gruppo Italiano per lo Studio del Colon e del Retto. Am J Gastroenterol 2000;95:1486–90.
Scarpa M, Angriman I, Barollo M, et al. Role of stapled and hand-sewn anastomoses in recurrence of Crohn’s disease. Hepatogastroenterology 2004;51:1053–7.
Tersigni R, Alessandroni L, Barreca M, Piovanello P, Prantera C. Does stapled functional end-to-end anastomosis affect recurrence of Crohn’s disease after ileocolonic resection? Hepatogastroenterology 2003;50:1422–5.
Makin AJ, Garnham AW, Keighley MR. Disruption of a stapled anastomosis following therapeutic ultrasonics–is there a risk? Report of a case. Dis Colon Rectum 1995;38:993–5.
Didolkar MS, Reed WP, Elias EG, Schnaper LA, Brown SD, Chaudhary SM. A prospective randomized study of sutured versus stapled bowel anastomoses in patients with cancer. Cancer 1986;57:456–60.
Beart RW Jr, Kelly KA. Randomized prospective evaluation of the EEA stapler for colorectal anastomoses. Am J Surg 1981;141:143–7
Anonymous. Suturing or stapling in gastrointestinal surgery: a prospective randomized study. West of Scotland and Highland Anastomosis Study Group. Br J Surg 1991;78:337–41
Elhadad A. Colorectal anastomosis: manual or mechanical? A controlled multicenter study. Chirurgie 1990;116:425–8.
Kracht M, Hay JM, Fagniez PL, Fingerhut A. Ileocolonic anastomosis after right hemicolectomy for carcinoma: stapled or hand-sewn? A prospective, multicenter, randomized trial. Int J Colorectal Dis 1993;8:29–33.
Friend PJ, Scott R, Everett WG, Scott IH. Stapling or suturing for anastomoses of the left side of the large intestine. Surg Gynecol Obstet 1990;171:373–6.
Galandiuk S. Stapled and hand-sewn anastomoses in Crohn’s disease. Dig Surg 1998;15:679–82
Graffner H, Andersson L, Lowenhielm P, Walther B. The healing process of anastomoses of the colon. A comparative study using single, double-layer or stapled anastomosis. Dis Colon Rectum 1984;27:767–71.
Hallbook O, Johansson K, Sjodahl R. Laser Doppler blood flow measurement in rectal resection for carcinoma–comparison between the straight and colonic J pouch reconstruction. Br J Surg 1996;83:389–92
Meagher AP, Wolff BG. Right hemicolectomy with a linear cutting stapler. Dis Colon Rectum 1994;37:1043–5.
D’Haens GR, Geboes K, Peeters M, Baert F, Penninckx F, Rutgeerts P. Early lesions of recurrent Crohn’s disease caused by infusion of intestinal contents in excluded ileum. Gastroenterology 1998;114:262–7
Rutgeerts P, Goboes K, Peeters M, et al. Effect of faecal stream diversion on recurrence of Crohn’s disease in the neoterminal ileum. Lancet 1991;338:771–4.
Osborne MJ, Hudson M, Piasecki C, et al. Crohn’s disease and anastomotic recurrence: microvascular ischaemia and anastomotic healing in an animal model. Br J Surg 1993;80:226–9.
Angerson WJ, Allison MC, Baxter JN, Russell RI. Neoterminal ileal blood flow after ileocolonic resection for Crohn’s disease. Gut 1993;34:1531–4.
Wakefield AJ, Sankey EA, Dhillon AP, et al. Granulomatous vasculitis in Crohn’s disease. Gastroenterology 1991;100:1279–87.
Shapiro S. Is there is or is there ain’t no baby? Dr. Shapiro replies to Drs. Petitti and Greenland. Am J Epidemiol 1994;140:788–91.
Shapiro S. Meta-analysis/Shmeta-analysis. Am J Epidemiol 1994;140:771–8
Petitti DB. Of babies and bathwater. Am J Epidemiol 1994;140:779–82.
Greenland S. Can meta-analysis be salvaged? Am J Epidemiol 1994;140:783–7
Longnecker MP. Re: “Point/counterpoint: meta-analysis of observational studies.” Am J Epidemiol 1995;142:779–82
Deeks JJ, Dinnes J, D’Amico R, et al. Evaluating non-randomised intervention studies. Health Technol Assess 2003;7(27):iii–x,1–173
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented to the European Society of Coloproctology, Lisbon, Portugal, September 13 to 16, 2006.
About this article
Cite this article
Simillis, C., Purkayastha, S., Yamamoto, T. et al. A Meta-Analysis Comparing Conventional End-to-End Anastomosis vs. Other Anastomotic Configurations After Resection in Crohn’s Disease. Dis Colon Rectum 50, 1674–1687 (2007). https://doi.org/10.1007/s10350-007-9011-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10350-007-9011-8