
Abstract
Introduction
Direct apical vertebral rotation represents an important goal of posterior surgery for thoracic adolescent idiopathic scoliosis (AIS), so as to obtain a better cosmetic effect and to avoid posterior thoracoplasty. However, the real effectiveness in correction of vertebral rotation, using posterior only procedures, is still open to debate. The aim of the present study is to compare the correction of axial apical rotation obtained with direct rotation procedure versus simple concave rod rotation, in patients treated by posterior fusion for thoracic AIS using pedicle screw-only construct.
Materials and methods
A retrospective review was performed on a total of 62 consecutive patients (one single institution, three different surgeons) affected by AIS, who had undergone a posterior spinal fusion with pedicle screw-only instrumentation between January 2005 and April 2008 at the reference center. All cases presented a main thoracic curve (Lenke type 1 and 2). The angle of rotation (RAsag) of the apical vertebra was measured from the preoperative and last follow-up axial CT. According to the derotation procedure, two groups were identified: a direct vertebral rotation group (DR group; n = 32 patients) and a simple concave rod rotation group (No-DR group; n = 30 patients). There were no statistical differences between the two groups, in terms of age, Risser’s sign, curve patterns, Cobb main thoracic (MT) curve magnitude and flexibility, extension of fusion, offset measurements on the coronal plane and sagittal preoperative contour.
Results
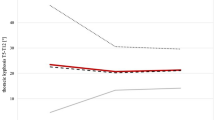
All 62 patients were reviewed at an average follow-up of 3.7 years (range 2.5–4.2 years). The DR group compared to the No-DR group showed a significantly better final correction of apical vertebral rotation (DR 63.4 % vs. No-DR 14.8 %; p < 0.05) and a greater final correction (61.3 vs. 52.4 %; p < 0.05) with better maintenance of the initial correction (−1.7° vs. −1.9°; ns) of the main thoracic curve. Concerning the coronal balance, there was the same aforementioned trend of better results in the DR group, with less final apical MT vertebra translation (DR 2.2 cm vs. No-DR 4.1 cm), greater overall change (preop-final) of lower instrumented vertebra (LIV) coronal tilt (−14.9° vs. −11.1°; p < 0.05); the final global coronal balance (C7–S1) resulted quite better in DR group, but without a significant difference. The T5–T12 kyphosis angle was quite similar in both group before surgery (DR 16.8° vs. No-DR 17.5°) and was little lower at final follow-up evaluation in direct vertebral rotation group (14.5° vs. 16.5°). The T10–L2 sagittal alignment angle was similar in each group before surgery (12.5° in DR vs. 11.8° in No-DR), and at the latest follow-up averaged 5.3° versus 8.2°, respectively. Lumbar lordosis was similar in each group before surgery (DR −42° vs. No-DR −44.1°) and at the final follow-up evaluation (−45.9° vs. −43.2°). At the latest follow-up, SRS-30 and SF-36 findings were similar between the two groups. The complication rate was higher in the simple concave rod rotation group (13.3 vs. 9.3 %), related in two cases to thoracoplasty, which was never utilized in direct rotation patients.
Conclusions
The direct vertebral rotation obtained significantly better final results, when compared to simple concave rod rotation, both concerning correction of apical vertebral rotation and magnitude of MT curve. On the other hand, the DR group presented a little reduction in T5–T12 kyphosis at follow-up, in comparison with concave rod rotation procedure. Both procedures were found to be satisfying from patients’ perspective. Nevertheless overall complication rate was higher in the simple concave rod rotation group, related mainly to thoracoplasty (2 cases), which was never necessary in direct rotation patients.


Similar content being viewed by others


References
Aaro S, Dahlborn M (1981) Estimation of vertebral rotation and the spinal and ribcage deformity in scoliosis by computer tomography. Spine 6:460–467
Apolone G, Mosconi P, Ware JE (1997) Questionario sullo stato di salute SF-36. Guerini e Associati Milano
Asghar J, Samdani AF, Pahys JM et al (2009) Computed tomography evaluation of rotation correction in adolescent idiopathic scoliosis. A comparison of an all pedicle screw construct versus a hook-rod system. Spine 34:804–807
Asher MA, Min Lai S, Burton DC (2000) Further development and validation of the Scoliosis Research Society (SRS) outcomes instrument. Spine 25:2381–2386
Asher M, Min Lai S, Burton D et al (2003) The reliability and concurrent validity of the Scoliosis Research Society-22 patient questionnaire for idiopathic scoliosis. Spine 28:63–69
Bridwell KH (1994) Surgical treatment of adolescent idiopathic scoliosis: the basics and the controversies. Spine 19:1095–1100
Chang MS, Lenke GL (2009) Vertebral derotation in adolescent idiopathic scoliosis. Oper Tech Orthop 19:19–23
Cheng I, Hay D, Iezza A et al (2010) Biomechanical analysis of derotation of the thoracic spine using pedicle screws. Spine 35:1039–1043
Cobb JR (1948) Outline for the study of scoliosis. AAOS Instr Course Lect 5:261–275
Cotrel Y, Dubousset J, Guillamat M (1988) New universal instrumentation in spinal surgery. Clin Orthop 227:10–23
Dalal A, Upasani VV, Bastrom TP et al (2011) Apical vertebral rotation in adolescent idiopathic scoliosis: comparison of uniplanar and polyaxial pedicle screws. J Spinal Disord Tech 24(4):251–257
Di Silvestre M, Parisini P, Lolli F, Bakaloudis G (2007) Complications of thoracic pedicle screws in scoliosis treatment. Spine 32:1655–1661
Dobbs MB, Lenke LG, Kim YL et al (2006) Selective posterior thoracic fusions for adolescent idiopathic scoliosis: comparison of hooks versus pedicle screws. Spine 31:2400–2404
Fu G, Kawakami N, Goto M et al (2009) Comparison of vertebral rotation corrected by different techniques and anchors in surgical treatment of adolescent thoracic idiopathic scoliosis. J Spinal Disord Tech 22:182–189
Greggi T, Bakaloudis G, Fusaro I et al (2010) Pulmonary function after thoracoplasty in the surgical treatment of adolescent idiopathic scoliosis. J Spinal Disord Tech 23:e63–e69
Harvey CJ Jr, Betz RR, Clements DH et al (1993) Are there indications for partial rib resection in patients with adolescent idiopathic scoliosis treated with Cotrel-Dubousset instrumentation? Spine 18:1593–1598
Hwang SW, Samdani AF, Gressot LV, Hubler K, Marks MC, Bastrom TP, Betz RR, Cahill PJ (2012) Effect of direct vertebral body derotation on the sagittal profile in adolescent idiopathic scoliosis. Eur Spine J 21(1):31–39
Jhaveri SN, Zeller R, Miller S, Lewis SJ (2009) The effect of intra-operative skeletal (skull femoral) traction on apical vertebral rotation. Eur Spine J 18(3):352–356
Kadoury S, Cheriet F, Beausejour M et al (2009) A three-dimensional retrospective analysis of the evolution of spinal instrumentation for the correction of adolescent idiopathic scoliosis. Eur Spine J 18:23–37
Krismer M, Bauer R, Sterzinger W (1992) Scoliosis correction by Cotrel-Dubousset instrumentation. The effect of derotation and three-dimensional correction. Spine 17:S263–S269
Kuklo TR, Potter BK, Polly DW Jr et al (2005) Monaxial versus multiaxial thoracic pedicle screws in the correction of adolescent idiopathic scoliosis. Spine 30:2113–2120
Lee SM, Suk SI, Chung ER (2004) Direct vertebral rotation: a new technique of three-dimensional deformity correction with segmental pedicle screw fixation in adolescent idiopathic scoliosis. Spine 29:343–349
Lehman RA, Lenke LG, Keeler KA et al (2008) Operative treatment of adolescent scoliosis with posterior pedicle screw-only constructs: minimum three-year follow-up of one hundred fourteen cases. Spine 33:1598–1604
Lenke LG, Bridwell KH, Baldus C et al (1992) Analysis of pulmonary function and axis rotation in adolescent and young adult idiopathic scoliosis patients treated with Cotrel-Dubousset instrumentation. J Spinal Disord 5:16–25
Lenke LG, Bridwell KH, Baldus C et al (1992) Cotrel Dubousset instrumentation for adolescent idiopathic scoliosis. J Bone Jt Surg Am 74:1056–1067
Lenke L, Betz R, Harms J et al (2001) Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Jt Surg Am 83:1169–1181
Lowenstein JE, Matsumoto H, Vitale MG et al (2007) Coronal and sagittal plane correction in adolescent idiopathic scoliosis: a comparison between all pedicle screw versus hybrid thoracic hook lumbar screw construct. Spine 32:448–452
Luhmann SJ, Lenke LG, Kim YJ, Bridwell KH, Schootman M (2005) Thoracic adolescent idiopathic scoliosis curves between 70° and 100°. Is anterior release necessary? Spine 30:2061–2067
Mladenov KV, Vaeterlein C, Stuecker R (2011) Selective posterior thoracic fusion by means of direct vertebral derotation in adolescent idiopathic scoliosis: effects on the sagittal alignment. Eur Spine J 20(7):1114–1117
O’Brein M, Kuklo T, Blanke K et al (2004) Spinal Deformity Study Group. Radiographic measurement manual Ed. Medtronic Sofamor Danek, USA, pp 59–61
Pratt RK, Webb JK, Burwell RG, Cole AA (2001) Changes in surface and radiographic deformity after Universal Spine System for right thoracic adolescent idiopathic scoliosis: is rib-hump reassertion a mechanical problem of the thoracic cage rather than an effect of relative anterior spinal overgrowth? Spine 26(16):1778–1787
Quan GM, Gibson MJ (2010) Correction of main thoracic adolescent idiopathic scoliosis using pedicle screw instrumentation. Does higher implant density improve correction? Spine 35(5):562–567
Richards BS (1992) Measurement error in assessment of vertebral rotation using the Perdriolle torsion meter. Spine 17:513–517
Schwartz DM, Auerbach JD, Dormans JP et al (2007) Neurophysiological detection of impending spinal cord injury during scoliosis surgery. J Bone Joint Surg Am 89:2440–2449
Stokes IAF (1994) Three-dimensional terminology of spinal deformity. A report presented to the Scoliosis Research Society by the Scoliosis Research Society Working Group on 3-D terminology of spinal deformity. Spine 19:236–248
Vallespir GP, Flores JB, Trigueros IS et al (2008) Vertebral coplanar alignment. A standardized technique for three dimensional correction in scoliosis surgery: technical description and preliminary results in Lenke type 1 curves. Spine 33:1588–1597
Vora V, Crawford A, Babekhir N et al (2007) A pedicle screw construct gives an enhanced posterior correction of adolescent idiopathic scoliosis when compared with other constructs: myth or reality. Spine 32:1869–1874
Yazici M, Acaroglu ER, Alanay A et al (2001) Measurement of vertebral rotation in standing versus supine position in adolescent idiopathic scoliosis. J Pediatr Orthop 21:252–256
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Di Silvestre, M., Lolli, F., Bakaloudis, G. et al. Apical vertebral derotation in the posterior treatment of adolescent idiopathic scoliosis: myth or reality?. Eur Spine J 22, 313–323 (2013). https://doi.org/10.1007/s00586-012-2372-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-012-2372-2