
Abstract
Introduction
Various fields have used gaze behaviour to evaluate task proficiency. This may also apply to surgery for the assessment of technical skill, but has not previously been explored in live surgery. The aim was to assess differences in gaze behaviour between expert and junior surgeons during open inguinal hernia repair.
Methods
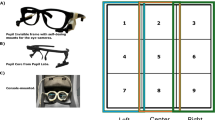
Gaze behaviour of expert and junior surgeons (defined by operative experience) performing the operation was recorded using eye-tracking glasses (SMI Eye Tracking Glasses 2.0, SensoMotoric Instruments, Germany). Primary endpoints were fixation frequency (steady eye gaze rate) and dwell time (fixation and saccades duration) and were analysed for designated areas of interest in the subject’s visual field. Secondary endpoints were maximum pupil size, pupil rate of change (change frequency in pupil size) and pupil entropy (predictability of pupil change). NASA TLX scale measured perceived workload. Recorded metrics were compared between groups for the entire procedure and for comparable procedural segments.
Results
Twenty-five cases were recorded, with 13 operations analysed, from 9 surgeons giving 630 min of data, recorded at 30 Hz. Experts demonstrated higher fixation frequency (median[IQR] 1.86 [0.3] vs 0.96 [0.3]; P = 0.006) and dwell time on the operative site during application of mesh (792 [159] vs 469 [109] s; P = 0.028), closure of the external oblique (1.79 [0.2] vs 1.20 [0.6]; P = 0.003) (625 [154] vs 448 [147] s; P = 0.032) and dwelled more on the sterile field during cutting of mesh (716 [173] vs 268 [297] s; P = 0.019). NASA TLX scores indicated experts found the procedure less mentally demanding than juniors (3 [2] vs 12 [5.2]; P = 0.038). No subjects reported problems with wearing of the device, or obstruction of view.
Conclusion
Use of portable eye-tracking technology in open surgery is feasible, without impinging surgical performance. Differences in gaze behaviour during open inguinal hernia repair can be seen between expert and junior surgeons and may have uses for assessment of surgical skill.



Similar content being viewed by others


References
Cuschieri A, Francis N, Crosby J, Hanna GB (2001) What do master surgeons think of surgical competence and revalidation? Am J Surg 182:110–116
Aggarwal R, Grantcharov TP, Darzi A (2007) Framework for systematic training and assessment of technical skills. J Am Coll Surg 204:697–705
Kohn LT, Corrigan JM, Donaldson MS (1999) To err is human. Building a safer health system Washington. National Academy Press, Washington, DC
van Hove PD, Tuijthof GJ, Verdaasdonk EG, Stassen LP, Dankelman J (2010) Objective assessment of technical surgical skills. Br J Surg 97:972–987
Moorthy K, Munz Y, Sarker SK, Darzi A (2003) Objective assessment of technical skills in surgery. BMJ 327:1032
Niitsu H, Hirabayashi N, Yoshimitsu M, Mimura T, Taomoto J, Sugiyama Y, Murakami S, Saeki S, Mukaida H, Takiyama W (2013) Using the Objective Structured Assessment of Technical Skills (OSATS) global rating scale to evaluate the skills of surgical trainees in the operating room. Surg Today 43:271–275
Richstone L, Schwartz MJ, Seideman C, Cadeddu J, Marshall S, Kavoussi LR (2010) Eye metrics as an objective assessment of surgical skill. Ann Surg 252:177–182
Ericsson KA (2007) An expert-performance perspective of research on medical expertise: the study of clinical performance. Med Educ 41:1124–1130
Koh RY, Park T, Wickens CD, Ong LT, Chia SN (2011) Differences in attentional strategies by novice and experienced operating theatre scrub nurses. J Exp Psychol Appl 17:233–246
Sodergren MH, Orihuela-Espina F, Froghi F, Clark J, Teare J, Yang GZ, Darzi A (2011) Value of orientation training in laparoscopic cholecystectomy. Br J Surg 98:1437–1445
Wilson MR, Vine SJ, Bright E, Masters RS, Defriend D, McGrath JS (2011) Gaze training enhances laparoscopic technical skill acquisition and multi-tasking performance: a randomized, controlled study. Surg Endosc 25:3731–3739
Sodergren MH, Orihuela-Espina F, Mountney P, Clark J, Teare J, Darzi A, Yang GZ (2011) Orientation strategies in natural orifice translumenal endoscopic surgery. Ann Surg 254:257–266
Vine SJ, Masters RS, McGrath JS, Bright E, Wilson MR (2012) Cheating experience: guiding novices to adopt the gaze strategies of experts expedites the learning of technical laparoscopic skills. Surgery 152:32–40
Gegenfurtner A, Lehtinen E, Säljö R (2011) Expertise differences in the comprehension of visualizations: a meta-analysis of eye-tracking research in professional domains. Educ Psychol Rev 23:523–552
Zheng B, Tien G, Atkins SM, Swindells C, Tanin H, Meneghetti A, Qayumi KA, Neely O, Panton M (2011) Surgeon’s vigilance in the operating room. Am J Surg 201:673–677
Atkins MS, Nicolaou M, Yang G-Z (2008) Eye monitoring applications in medicine. Passive eye monitoring. Springer, Berlin, pp 323–343
Sodergren MH, Orihuela-Espina F, Clark J, Teare J, Yang GZ, Darzi A (2010) Evaluation of orientation strategies in laparoscopic cholecystectomy. Ann Surg 252:1027–1036
Zheng B, Cassera MA, Martinec DV, Spaun GO, Swanstrom LL (2010) Measuring mental workload during the performance of advanced laparoscopic tasks. Surg Endosc 24:45–50
General Surgery syllabus, The Intercollegiate Surgical Curriculum
Disclosures
Tien, Pucher, Sodergren, Sriskandarajah, Yang and Darzi have no conflict of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tien, T., Pucher, P.H., Sodergren, M.H. et al. Differences in gaze behaviour of expert and junior surgeons performing open inguinal hernia repair. Surg Endosc 29, 405–413 (2015). https://doi.org/10.1007/s00464-014-3683-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-014-3683-7