
Abstract
Cardiac atrophy as a consequence of mechanical unloading develops following exposure to microgravity or prolonged bed rest. It also plays a central role in the reverse remodelling induced by left ventricular unloading in patients with heart failure. Surprisingly, the intracellular Ca2+ transients which are pivotal to electromechanical coupling and to cardiac plasticity were repeatedly found to remain unaffected in early cardiac atrophy. To elucidate the mechanisms underlying the preservation of the Ca2+ transients, we investigated Ca2+ cycling in cardiomyocytes from mechanically unloaded (heterotopic abdominal heart transplantation) and control (orthotopic) hearts in syngeneic Lewis rats. Following 2 weeks of unloading, sarcoplasmic reticulum (SR) Ca2+ content was reduced by ~55 %. Atrophic cardiac myocytes also showed a much lower frequency of spontaneous diastolic Ca2+ sparks and a diminished systolic Ca2+ release, even though the expression of ryanodine receptors was increased by ~30 %. In contrast, current clamp recordings revealed prolonged action potentials in endocardial as well as epicardial myocytes which were associated with a two to fourfold higher sarcolemmal Ca2+ influx under action potential clamp. In addition, Cav1.2 subunits which form the pore of L-type Ca2+ channels (LTCC) were upregulated in atrophic myocardium. These data suggest that in early cardiac atrophy induced by mechanical unloading, an augmented sarcolemmal Ca2+ influx through LTCC fully compensates for a reduced systolic SR Ca2+ release to preserve the Ca2+ transient. This interplay involves an electrophysiological remodelling as well as changes in the expression of cardiac ion channels.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cardiac atrophy can be observed during prolonged bed rest, space flight or cachexia [19]. It also plays a central role in the reverse remodelling induced by left ventricular unloading in patients with heart failure [19]. In contrast to hypertrophic remodelling, cardiac atrophy is generally not well understood. Intracellular Ca2+ handling plays an essential role in regulating cardiac function and is pivotal to adaptations in hypertrophic cardiac remodelling [18, 19]. An early cellular response to a hypertrophic stimulus is the prolongation of ventricular action potentials (AP) which greatly facilitates Ca2+ influx via L-type Ca2+ channels (LTCC) [10, 48, 53]. In addition, phosphorylation of phospholamban (PLB) is increased, thus relieving the sarcoplasmic reticulum (SR) Ca2+ ATPase (SERCA) from its inhibition [7, 28]. As a consequence, Ca2+ content of the SR and systolic Ca2+ release from the SR are enhanced [3, 5, 16, 31, 53]. Collectively, these alterations cause larger systolic Ca2+ transients which are thought to allow adaptation to the increased cardiac workload in early hypertrophy [9, 11, 17, 43, 47]. We have previously reported a reduced phosphorylation of several phosphoproteins, including PLB, in cardiac atrophy [41]. Unphosphorylated PLB exerts a stronger inhibitory effect on SERCA which should lead to a reduced SR Ca2+ load. Hence, one may expect that Ca2+ release during systole is diminished and amplitudes of systolic Ca2+ transients are dampened in atrophic hearts. The shape of the systolic Ca2+ transient, however, was found to be unaltered in early atrophic remodelling [22, 46].
The mechanisms underlying the maintenance of the Ca2+ transient in early cardiac atrophy are unresolved. Short-term cardiac unloading causes a marked prolongation of ventricular APs and a higher density of the L-type Ca2+ current [40]. Accordingly, a reduced systolic Ca2+ release from the SR may be compensated by a concurrent upregulation of the Ca2+ inflow from the extracellular space in atrophic cardiac myocytes. To test this hypothesis, we determined the effect of cardiac atrophy induced by mechanical unloading on key components of myocardial Ca2+ cycling.
Methods
Animal model
Cardiac atrophy was induced in syngeneic male Lewis rats (270 ± 5 g, n = 34, Charles River, Sulzfeld, Germany) by heterotopic abdominal heart transplantation as previously described [12, 14, 21, 22, 29, 40, 41, 45, 46]. The donor heart was harvested under deep anaesthesia (thiopental-sodium, 100 mg/kg body weight) and was transplanted into the abdominal cavity of the recipient rat under isoflurane anaesthesia (2–2.5 %). Perioperative pain management was performed using buprenorphine (0.1 mg/kg body weight) and metamizole-sodium (300 mg/kg body weight). The aortic and pulmonary vessels of the donor heart were anastomized infrarenally to the abdominal aorta and the inferior vena cava of the recipient animal, respectively. In this configuration, coronary perfusion is conserved and left ventricular filling is substantially reduced. Spontaneous contraction returned within minutes after reperfusion and was checked regularly. The transplanted (atrophic) and the orthotopic (control) hearts of the recipient animal were removed in deep anaesthesia (thiopental-sodium, 100 mg/kg body weight) 2 weeks after transplantation. An unloading period of 2 weeks was chosen to induce a stable cardiac atrophy in accordance with previous studies [12, 14, 40, 41] while avoiding the detrimental effects of prolonged unloading on cardiac excitation–contraction coupling and contractility [21, 22, 29, 45]. For all experiments, the orthotopic hearts served as corresponding controls. Animal experiments were conducted in accordance with institutional guidelines and were approved by local authorities (Ministry of Science and Health, Hamburg, Germany, permit number 02/04). Furthermore, they complied with the European Convention for the Protection of Vertebrate Animals Used for Experimental and Other Scientific Purposes (Council of Europe No. 123).
Isolation of cardiomyocytes
For single-cell experiments, cardiac myocytes were enzymatically isolated from the control or the atrophic heart of one animal. Since the time span between sacrificing the animal and the beginning of the perfusion using the Langendorff apparatus must be kept at a minimum to ensure isolation of cardiac myocytes of high quality, we randomly assigned either the orthotopic or the transplanted heart to the cell isolation procedure. The other heart was discarded. Cardiac myocytes were isolated from the endocardial and epicardial layer of the center part of the left ventricular free wall [15, 40, 51, 52]. For experiments depicted in Fig. 3b, myocytes were isolated from control male Lewis rats (270 g, n = 3). Following isolation, cells were stored in a Ca2+-free modified Tyrode's solution. Only single rod-shaped cells with clear cross-striation and no spontaneous contractions were used for the experiments within 6 h following the isolation. All experiments were performed at a temperature of 21–24 °C.
Ca2+ epifluorescence measurements
Ca2+ epifluorescence was recorded as previously described [34]. Cells were incubated in an extracellular solution (containing [mmol/l]: NaCl 135, KCl 4.7, KH2PO4 0.6, Na2HPO4 0.6, MgSO4 1.2, Hepes 10, glucose 20, CaCl2 1.25) with Fura-2-AM (4 μmol/l). Cells were transferred into a chamber (Cell MicroControls, Norfolk, VA, USA) mounted on an inverted microscope (Nikon Eclipse TS100). Ca2+ transients of intact myocytes were recorded during field stimulation (0.5 Hz, 4 ms duration; MyoPacer, IonOptix Corporation, Milton, MA, USA). Cells were alternatively excited at 340 and 380 nm (hyper-switch dual excitation, IonOptix Corporation). The F 340/F 380 ratio was used as an index of cytosolic Ca2+ concentration. In some experiments, thapsigargin was washed in and after an incubation time of 5 min, Ca2+ transients were assessed using Fluo-3-AM (10 μmol/l, F/F 0 from excitation at 480 ± 15 nm and emission at 535 ± 20 nm). Ca2+ transients were analysed using Ionwizard (v. 5.0, IonOptix Corporation).
Cellular electrophysiology
The ruptured-patch whole-cell configuration was used with an EPC-9 amplifier controlled by the Pulse software (Heka Elektronik, Lambrecht, Germany) [40, 51]. Membrane capacitance and series resistance were calculated using automated procedures of the EPC-9. Whole-cell currents and membrane potentials were low pass-filtered at 1 kHz, sampled at 5 kHz and analysed using the Pulse-fit software (v. 8.80, Heka Elektronik) and custom-made procedures in IgorPro (v. 6.2, Wavemetrics, Lake Oswego, OR, USA). Patch pipettes were pulled from borosilicate glass (GC150-15, Harvard Apparatus, Holliston, MA, USA). Pipette resistance averaged 2.2 ± 0.1 MΩ (n = 49) in the SR release experiments, 2.7 ± 0.1 MΩ (n = 75) in the I NCX experiments and 3.4 ± 0.1 MΩ (n = 50) in the AP clamp experiments. The series resistance was between 3.0 and 8.9 MΩ and was compensated by 85 %. Sarcoplasmic reticulum (SR) release experiments were performed using a CsCl-based pipette solution (mmol/l): CsCl 128, MgCl2 5 TEA-Cl 20, EGTA 0.1, Hepes 10, Mg2-ATP 2, titrated to pH = 7.20 with CsOH. Extracellular solution (modified Tyrode's solution) contained (mmol/l): NaCl 138, KCl 4, MgCl2 1, NaH2PO4 0.33, CaCl2 2, glucose 10, Hepes 10, titrated to pH = 7.30 with NaOH. For inhibition of K+ currents, 4 mmol/l 4-aminopyridine and 0.1 mmol/l BaCl2 were added to the bath solution [49, 54]. At the beginning of the experiment, cells were repeatedly stepped from a holding potential of −90 to 0 mV (500 ms) at a frequency of 0.5 Hz over 60 s to obtain steady-state filling of the SR. For measurement of I NCX, the pipette solution contained (mmol/l): CsCl 85, glucose 5.5, EGTA 14, MgCl2 3, CaCl2 3.92, Hepes 10, NaCl 15, ATP 2, titrated to pH = 7.20 using CsOH (total Cs, 130 mmol/l). Cells were patched in a K+-free Tyrode solution. To activate I NCX, extracellular solution was switched to a Li+-based solution containing (mmol/l): LiCl 140, MgCl2 1, NaH2PO4 0.33, CaCl2 2, glucose 10, Hepes 10, titrated to pH = 7.30 using LiOH. I NCX was quantified as the difference between the holding current and the maximal outward current when the current amplitude reached a steady state. For AP clamp experiments, a K-glutamate pipette solution containing (mmol/l) K-glutamate 120, KCl 10, MgCl2 2, EGTA 10, Hepes 10, Na2-ATP 2, and titrated to pH = 7.20 with KOH was used in combination with a modified Tyrode's solution. Ca2+ influx was estimated using 30 μmol/l Cd2+. At this rather low concentration, Cd2+ inhibits I Ca,L but only marginally affects other currents such as I to and I NCX [1, 20]. Moreover, more specific inhibitors of I Ca,L, such as dihydropyridines or D600, are potent inhibitors of I to and would thus interfere with the estimation of Q Ca. Overall, the AP-induced Cd2+-sensitive current yields a reasonable estimate for the AP-induced Ca2+ influx [35, 51, 53]. All currents and Ca2+ charges were normalised to cell capacitance.
Ca2+ sparks
Ca2+ sparks were assessed by standard confocal microscopy using a Zeiss Axiovert 200 M microscope and the Zeiss LSM5 image system (Carl Zeiss AG, Oberkochen, Germany) [55]. The bath solution consisted of a modified Tyrode's solution containing 2 mmol/l CaCl2. Cells were loaded with 10 μg/ml Fluo-4-AM (Invitrogen, Darmstadt, Germany). Following an initial phase of field-stimulated pacing (60 s, 0.5 Hz, 4 ms duration), spontaneous Ca2+ release was recorded over 30 s using a line scan, with the scanning line placed parallel to the longitudinal axis of the cell at a central focal plane. Spark frequency was quantified using the sparkmaster plugin in ImageJ (Rasband W, NIH, Bethesda, MD, USA) [33].
Western blot analysis
For determination of protein expression, the transplanted as well as the orthotopic hearts were excised in deep anaesthesia (see earlier discussion). Left ventricular tissue was immediately shock-frozen and stored at −80 °C for later analysis. Western blotting was performed as described previously [41] with primary antibodies against ryanodine receptor (RyR, 1:10,000, Sigma-Aldrich), S2843-phosphorylated RyR (1:5,000, Badrilla), Cav1.2 (1:200, Santa Cruz), calsequestrin (CSQ, 1:2,500, Dianova) and GAPDH (1:20,000, Biotrend).
Statistical analysis
All data are given as mean ± SEM. When only two groups were compared, statistical significance was calculated by Student's t-test or a Mann–Whitney test as appropriate. Multiple comparisons were performed using a one-way ANOVA followed by Newman–Keuls post hoc test or a repeated-measures two-way ANOVA using PRISM (v. 5.0, GraphPad Software Inc., San Diego, CA, USA). Statistical significance was defined as P < 0.05.
Results
Systolic Ca2+ transients
Systolic Ca2+ transients were investigated in Fura-2-AM-loaded isolated cardiac myocytes under field stimulation. In myocytes isolated from control hearts, no layer-specific differences between endocardial and epicardial cardiac myocytes regarding shape and duration of intracellular Ca2+ transients were observed (data not shown). Therefore, Ca2+ transients were analysed in cell suspensions pooled from endocardial and epicardial myocytes to increase statistical power. Ca2+ transients did not differ between atrophic and control myocytes (Fig. 1a). In particular, the amplitude of the Ca2+ transients (Fig. 1b), the diastolic Ca2+ concentration (Fig. 1c), as well as the time course of the Ca2+ transients (Fig. 1d, e) were not significantly different. These findings confirm that the intracellular Ca2+ transients remain unchanged in early cardiac atrophy [22, 46].

Preserved systolic Ca2+ transients in myocytes of atrophic hearts. a Representative Ca2+ transients from left ventricular myocytes isolated from control (black spectrum, left panel, n = 5) and atrophic (blue spectrum, right panel, n = 5) hearts. b–e Summary data for the main parameters of the Ca2+ transients. Numbers in columns represent the number of individual myocytes. TTP90 time to 90 % peak, TTB90 time to 90 % baseline
SR Ca2+ content
We have previously reported a reduced phosphorylation of PLB in atrophic cardiac myocytes [41] which predicts a lower SERCA activity and consequently a reduced SR Ca2+ load in atrophic hearts. To test this prediction, we quantified the amount of the steady-state SR Ca2+ content in isolated cardiac myocytes using the patch clamp technique. To assess the degree of cellular atrophy and to allow for normalisation to the reduced cell size, cell capacitance was determined at the beginning of each experiment. Consistent with previous reports, cell capacitance was significantly lower in atrophic than in control cardiac myocytes (123 ± 3 pF, n = 96 vs. 161 ± 5 pF, n = 98, p < 0.0001) [40]. At a holding potential of V Pip = −90 mV, Ca2+ release from the SR was induced by rapid superperfusion of the investigated cardiac myocyte with 10 mmol/l caffeine [30, 38, 49, 50, 54]. In the presence of caffeine, Ca2+ is released from the SR, cannot be stored in the SR again and is therefore completely removed from the cytoplasm by the Na+–Ca2+ exchanger [8, 27]. This results in the activation of a transient inward current (I ti) following caffeine application (Fig. 2a). In myocytes isolated from atrophic hearts, the amplitude of this current (peak I ti) was significantly lower than in control myocytes (~ − 10 % in endocardial and ~ −50 % in epicardial myocytes; Fig. 2b). More importantly, the integral of I ti (Qcaff), which reflects the total amount of Ca2+ released from the SR [49], was significantly smaller (~ − 55 %) in the atrophic cardiac myocytes (Fig. 2c). These observations indicate that the amount of Ca2+ stored in the SR is markedly reduced in early atrophy.

Decreased SR Ca2+ content and unaltered I NCX in myocytes of atrophic hearts. a Representative whole-cell current traces recorded from myocytes of control (black spectrum, left panel, n = 6) and atrophic (blue spectrum, right panel, n = 6) hearts. At a pipette potential of −90 mV, caffeine (10 mmol/l) was washed in to induce SR Ca2+ release, resulting in a transient inward current (I ti). b Average values of the peak current density of I ti. c total amount of Ca2+ transported by I ti upon caffeine application (Q caff). Q caff was calculated as the area under the curve of I ti. d Representative whole-cell current traces recorded from left ventricular myocytes of control (black spectrum, left panel, n = 4) and atrophic (blue spectrum, right panel, n = 4) hearts. At a pipette potential of −40 mV, the extracellular solution was replaced by a Li+-based solution resulting in an outward current (I NCX). e Mean current density of I NCX. Numbers in columns represent the number of individual cells. *P < 0.05; **P < 0.01; ***P < 0.001 (two-way ANOVA followed by Newman–Keuls post hoc test). Endo endocardial myocytes, Epi epicardial myocytes
The density of the Na+–Ca2+ exchanger current (I NCX) was quantified in further patch clamp experiments as previously described [26]. Using a K+-free Tyrode solution, myocytes were held at V Pip = −40 mV. Switching the extracellular solution to a Li+-based bath solution activated I NCX in its reverse mode, resulting in an outward current (Fig. 2d). I NCX was quantified as the difference between the holding current and the maximal outward current. Using this approach, no significant difference was detected in the functional expression of I NCX (Fig. 2e), implicating that the Na+–Ca2+ exchanger is not altered in early cardiac atrophy.
Diastolic Ca2+ release
An increased occurrence of spontaneous SR Ca2+ release could also contribute to the marked decrease in the amount of Ca2+ stored in the SR. We therefore quantified the frequency of Ca2+ sparks in isolated ventricular cardiac myocytes. Atrophic cardiac myocytes showed a significantly lower frequency of spontaneous diastolic Ca2+ sparks (~ − 45 %; Fig. 3a). Also, the fraction of cells showing a very low Ca2+ spark activity (<0.5 sparks/100 μm/s) was twofold higher in the atrophic group (46 vs. 23 %; Fig. 3a). These results argue against a major contribution of an increased SR Ca2+ leak to the reduced SR Ca2+ content in the atrophic myocardium at this stage.

Decreased Ca2+ spark frequency in myocytes of atrophic hearts and increased ryanodine receptor expression. a Average Ca2+ spark frequency (left panel) in left ventricular myocytes obtained from control (black bar, n = 7) and atrophic (blue bar, n = 7) hearts. The right panel illustrates the corresponding histogram. Ca2+ spark frequency was quantified over 1,856 ± 75 μm s per cell (n = 67) following steady-state pacing. b Average Ca2+ spark frequency in left ventricular myocytes obtained from control hearts (n = 3). Sparks were quantified in control myocytes (black bar) and in myocytes pre-treated with 100 nmol/l thapsigargin (TG, white bar). At this concentration, TG induced a depletion of the SR which closely matched the SR load of atrophic cardiac myocytes. The left panel illustrates the mean Ca2+ spark frequency and the right panel the corresponding histogram. c Representative immunoblots of RyR, S2814-RyR and GAPDH in tissue samples of control (C) and atrophic (A) left ventricular myocardium. d, e Densitometric analysis of gene expression. RyR expression was normalised to GAPDH, and the phosphorylation of RyR at S2814 was normalised to total RyR amount in control (black bar) and atrophic (blue bar) tissue samples, respectively. All data are given relative to the mean of the expression in control hearts. Numbers in columns represent the number of cardiac myocytes (a, b) or tissue samples (d, e). *P < 0.05; ***P < 0.001 (Student's t-test)
The occurrence of spontaneous Ca2+ release depends on the SR Ca2+ load [42]. Thus, the reduced spark frequency in atrophic hearts may be a consequence of the reduced SR Ca2+ load. To address this issue, we assessed the effect of a partial depletion of the SR on the Ca2+ spark frequency in control myocytes using thapsigargin as previously described [44]. To match the lower SR Ca2+ load of atrophic cardiac myocytes, control cardiac myocytes were treated with 100 nmol/l of the SERCA blocker thapsigargin. This resulted in a reduction of the caffeine-induced Ca2+ release from the SR by 54 ± 12 % (n = 10), which closely resembles the depletion in atrophic cardiac myocytes. Quantification of spontaneous Ca2+ release in control and thapsigargin-treated cardiac myocytes revealed that the partial depletion of the SR caused a ~65 % lower mean Ca2+ spark frequency and a 2.5-fold higher fraction of cells with a very low spark activity (Fig. 3b). Thus, a quantitatively nearly identical reduction of the SR Ca2+ load was associated with a moderately smaller reduction of the spark frequency in atrophic (~ −45 %) than in control (~ − 65 %) cardiac myocytes. Since this difference may be the consequence of an increased functional expression of RyRs, we determined their abundance and the phosphorylation (Fig. 3c–e). Indeed RyR expression was significantly increased (~130 % of control; Fig. 3d) in the atrophic myocardium, whereas its phosphorylation at S2814 was unaltered (Fig. 3e).
Systolic SR Ca2+ release
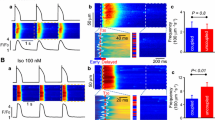
Unaffected Ca2+ transients in spite of a decreased SR Ca2+ content could be a consequence of an unaltered absolute amount of Ca2+ released from the SR during systole. To test this, the contribution of SR Ca2+ release to the total cytosolic Ca2+ transient was quantified. Ca2+ transients were assessed during continuous field stimulation in the absence and subsequently in the presence of thapsigargin (1 μmol/l; Fig. 4a). In the presence of 1 μmol/l thapsigargin, reuptake of cytosolic Ca2+ into the SR is fully inhibited, and the increase in cytosolic Ca2+ concentration during the following APs mainly derives from AP-induced Ca2+ influx [23]. If the total amount of Ca2+ released from the SR was similar in both groups, the Ca2+ transient should be depressed by a comparable degree in both groups. In control myocytes, thapsigargin significantly reduced the amplitude of Ca2+ transients by ~55 %. In atrophic myocytes, however, the amplitude was reduced by only ~35 % (Fig. 4b). Application of thapsigargin increased diastolic Ca2+ levels (Fig. 4c) and the time course of the Ca2+ transients (Fig. 4d, e) similarly in myocytes of both groups. While the experimental condition of completely absent Ca2+ release from the SR is likely to interfere with Ca2+-dependent LTCC inactivation and therefore possibly alters their contribution to the Ca2+ transient, these results suggest a reduced amount of Ca2+ released from the SR in the atrophic cardiac myocytes during systole. Thus, the Ca2+ transient in atrophic cardiac myocytes must be maintained by a compensatory mechanism other than an increased fractional release from the SR.

Decreased systolic Ca2+ release from the SR in myocytes of atrophic hearts. a Representative recordings of Ca2+ transients from myocytes isolated from control (black spectrum, left panel, n = 4) and atrophic (blue spectrum, right panel, n = 5) hearts. Following steady-state recordings (Ctrl), thapsigargin (1 μmol/l) was washed in (TG). b–e Summary data for the main parameters of Ca2+ transients under control conditions (Ctrl) and in the presence of thapsigargin (TG). Numbers in columns represent the number of individual myocytes. TTP90 time to 90 % peak, TTB90 time to 90 % baseline. **P < 0.01; ***P < 0.001 (repeated-measures two-way ANOVA followed by Newman–Keuls post hoc test)
Systolic Ca2+ influx
A possible explanation for unchanged Ca2+ transients in the presence of a reduced SR Ca2+ load is an increased Ca2+ influx during the AP. Supporting this hypothesis, we have previously reported an increased AP duration in atrophic cardiac myocytes [40]. Ca2+ influx into the cell via the LTCC is regulated by several factors, including the AP waveform, the availability of LTCC and the negative feedback loop induced by the Ca2+-dependent LTCC inactivation. This complex regulation makes prediction of the absolute amount of systolic Ca2+ influx during the AP difficult. We therefore assessed the AP-induced Ca2+ influx using the AP clamp technique. This allows the quantification of the Ca2+ influx in individual cardiac myocytes using their own AP waveform [51, 53]. The steady-state AP waveform of the cardiac myocyte under investigation was recorded in the current clamp mode at the beginning of each patch clamp experiment (Fig. 5a, upper panels). Consistent with our previous findings [40], cardiac atrophy was associated with significantly prolonged APs in endocardial myocytes (~150 % of control) and epicardial myocytes (~250 % of control; Fig. 5b). After switching to the voltage clamp mode, the membrane potential of each individual myocyte was clamped to its own previously recorded AP. The AP-induced current was recorded in the absence and presence of the Ca2+ channel blocker Cd2+ (30 μmol/l). Subtraction analysis of the resulting currents yielded the Cd2+-sensitive current, which gives an estimate for the AP-induced Ca2+ current through LTCC (I Ca; Fig. 5a, lower panels). To calculate total Ca2+ influx during the AP, I Ca was integrated (Q Ca). Q Ca was approximately two- to fourfold higher in atrophic endocardial and epicardial myocytes than in control myocytes from the corresponding layer (Fig. 5c). In addition, Western blot analysis revealed an upregulation of Cav1.2 subunits in the atrophic myocardium (Fig. 5d, e). These results indicate that in atrophic cardiac myocytes Ca2+ influx through LTCC is augmented both by an increased electrical driving force caused by prolonged APs and by an increased membrane abundance of Ca2+ channel protein.

Increased Ca2+ influx during the AP in myocytes from atrophic hearts. a Representative APs and corresponding Cd2+ sensitive currents (I Ca) recorded in endocardial and epicardial myocytes isolated from control (black spectrum, n = 3) and atrophic (blue spectrum, n = 4) hearts. The AP waveform (upper panels) of each individual cell was used to record the AP-driven Ca2+ influx via L-type Ca2+ channels (I Ca, lower panels) of each myocyte in the voltage clamp configuration (AP clamp). I Ca was calculated as the difference between the whole-cell current evoked by the AP waveform in the absence and in the presence of 30 μmol/l Cd2+. b, c Mean values of AP duration (APD90, b) and of Ca2+ influx (Q Ca, c). Q Ca was calculated as the area under the curve of I Ca normalised to the cell capacitance. d Representative immunoblots of Cav1.2 and calsequestrin (CSQ) of tissue samples from control and atrophic left ventricular myocardium. e Mean values of Cav1.2 expression normalised to CSQ in control (black bar) and atrophic (blue bar) tissue samples, respectively. All data are given relative to the mean of the expression in control hearts. Numbers in columns represent the number of individual myocytes (b, c) or tissue samples (e). Endo endocardial myocytes, Epi epicardial myocytes. *P < 0.05; **P < 0.01; ***P < 0.001 (ANOVA followed by Newman–Keuls post hoc test or Student's t-test)
Discussion
Two major interdependent mechanisms contribute to the systolic elevation of cytosolic Ca2+ in ventricular cardiac myocytes (Fig. 6a). Systolic Ca2+ cycling is initiated by the sarcolemmal Ca2+ influx through LTCC during the AP. Besides directly raising the intracellular Ca2+ concentration, this triggers further Ca2+ release from the SR (Ca2+-induced Ca2+ release). The amount of Ca2+ released from the SR depends on the size of the trigger signal, on the SR Ca2+ load and on the Ca2+ release threshold [6, 13, 24, 50]. In cardiac myocytes, the majority of the total Ca2+ increase is normally met by Ca2+ release from the SR [4, 13]. Here we show that cardiac atrophy induces a pronounced alteration of the balance of Ca2+ cycling between the two major Ca2+ sources. While SR Ca2+ content and the amount of Ca2+ released during the Ca2+-induced Ca2+ release are greatly reduced in atrophic hearts, this reduced contribution of the SR is fully compensated by an increased Ca2+ influx through LTCC. As a result, systolic Ca2+ transients remain normal in atrophic myocardium.

Ca2+ cycling in normal and atrophic cardiac myocytes. Schemes illustrating Ca2+ cycling under steady-state conditions in normal (a) and in atrophic cardiac myocytes (b). a In normal ventricular cardiac myocytes, Ca2+ influx during the AP through LTCC triggers Ca2+ release from the SR. Increasing cytosolic Ca2+ concentrations (by Ca2+ influx and SR Ca2+ release) inhibit LTCC, thus limiting further Ca2+ influx. The cytosolic Ca2+ concentration is reduced by the reuptake of Ca2+ into the SR via SERCA and by extrusion via Na+–Ca2+ exchanger. b In atrophic hearts, SERCA activity is reduced secondary to a diminished phosphorylation of PLB, resulting in reduced Ca2+ uptake into the SR, SR Ca2+ content and SR Ca2+ release during systole. Accordingly, the inhibition of LTCC by Ca2+ released from the SR is reduced. This, in combination with prolonged APs and an increased density of LTCC on the cell surface allows for a larger net Ca2+ influx during the AP. Relative changes compared to the control myocytes are indicated by colours (dark blue increase, light blue decrease). LTCC L-type Ca2+ channel, NCX Na+–Ca2+ exchanger, SR sarcoplasmic reticulum, PLB phospholamban, SERCA SR Ca2+ ATPase
In myocytes of atrophic hearts, the amount of Ca2+ stored in the SR was ~55 % lower than in myocytes isolated from control hearts. This may result from an increased SR Ca2+ leak and/or a decreased Ca2+ uptake. Diastolic spark frequency was decreased by ~45 % in atrophic cardiac myocytes, which argues against a relevant contribution of an increased diastolic Ca2+ leak to the SR depletion. SR Ca2+ content itself, however, influences the spark frequency, complicating the interpretation. A quantitatively similar reduction of SR Ca2+ load induced by a pharmacological SERCA inhibition in control cardiac myocytes induced a modestly larger SR Ca2+ spark reduction (~ − 65 %). This finding suggests that the reduced frequency of spontaneous Ca2+ release in atrophic cardiac myocytes may be mainly a consequence of the reduced SR Ca2+ load which is partly offset by an increased ryanodine receptor density. Ca2+ uptake into the SR is governed by SERCA activity, which depends on the cytosolic Ca2+ concentration and modulation by several regulator proteins, including PLB and sarcolipin [25]. Under steady-state conditions, even a mild reduction in SERCA activity can lead over time to a markedly reduced SR Ca2+ load. Consistently, we have previously reported a decrease in phosphorylation of PLB in atrophic myocardium which is expected to contribute to a reduction in SERCA activity [41]. Given that the decay of the intracellular Ca2+ transient is unaltered in atrophic myocardium (Fig. 1) [22, 46], it seems likely that SERCA activity is reduced to a degree that the resulting slowing of the Ca2+ uptake into the SR is fully compensated for by Ca2+ transport via the Na+–Ca2+ exchanger. Taken together, the data currently available indicate that the reduction in SR Ca2+ load is predominantly a consequence of a moderately decreased SERCA activity, possibly mediated by reduced PLB phosphorylation and potentially in combination with a reduced set point of SR Ca2+ content [24] or an increased nonspark diastolic Ca2+ release [39]. It cannot be excluded that during an earlier phase of atrophic remodelling, an increased SR leak contributes to the development of the reduced SR Ca2+ load.
Consistent with previous reports, no significant differences were detected regarding diastolic Ca2+, systolic Ca2+ amplitude or the onset and decay of the Ca2+ transients [22, 46]. In principle, the Ca2+ transient in atrophic hearts could be conserved by an unaltered amount of Ca2+ released from the SR in spite of its depletion (i.e. higher fractional Ca2+ release). Using the SERCA blocker thapsigargin we could demonstrate that in atrophic myocytes the quantity of Ca2+ released from the SR was significantly lower than in control cardiac myocytes. Therefore, to maintain a normal Ca2+ transient, an increased Ca2+ influx through LTCC has to compensate for the depressed SR Ca2+ release. Ca2+ influx is mainly governed by the shape of the AP and the availability of Ca2+ channels. We have previously reported that a diminished density of the transient outward K+ current (I to) in combination with an increased density of the L-type Ca2+ current results in a net prolongation of APs in atrophic hearts [40]. We now demonstrate that this electrophysiological remodelling is associated with a two- to fourfold increase in Ca2+ influx during the AP, providing a mechanism for the maintenance of the systolic Ca2+ transient.
Sarcolemmal Ca2+ influx increases the intracellular Ca2+ concentration, hence activating ryanodine receptors and initiating the Ca2+-induced Ca2+ release (Fig. 6a). At the same time, however, the increasing Ca2+ concentration in the subsarcolemmal space will limit further Ca2+ influx by inactivating LTCC [4]. This negative feedback mechanism regulates the relation between Ca2+ influx and Ca2+ release from the SR and assures a finely tuned Ca2+ transient [13]. In cardiac atrophy, two remodelling processes (increased Ca2+ influx and decreased SR Ca2+ release) seem to exactly balance each other, resulting in unchanged Ca2+ transients (Fig. 6b). A primary decrease of SR Ca2+ load and SR Ca2+ release would lead to a slower increase of subsarcolemmal Ca2+ concentrations during systole, thus causing less inhibition of LTCC. This would facilitate escalating Ca2+ influxes until the initial Ca2+ transient is balanced again. If the initial response to cardiac atrophy was an augmentation of Ca2+ influx through LTCC, the resulting increase in cytosolic Ca2+ concentrations may induce a reduction of the SR Ca2+ load and SR Ca2+ release, e.g. via a diminished phosphorylation of PLB, eventually resulting in a new steady state. This functional coupling between Ca2+ influx and Ca2+ release from the SR seems to be supported by changes in the expression of ion channels which are relevant for regulating Ca2+ influx with an upregulation of LTCC (Fig. 5) and a downregulation of K+ channel subunits underlying I to [40]. The expression of all of these channels is modulated via the CaMKII-DREAM and/or calcineurin pathways by the Ca2+ concentration [32, 37]. Collectively, these observations suggest that during atrophic remodelling, localized changes of the intracellular Ca2+ concentration preserve the systolic Ca2+ transient both via a functional feedback as well as via a modulation of ion channel expression.
Cardiac hypertrophy induced by an increased afterload and cardiac atrophy have been proposed to induce a common pattern of cellular remodelling [2, 12, 36]. Consistent with this concept, we have previously shown that cardiac atrophy is associated with similar prolongations in cardiac action potentials as cardiac hypertrophy [3, 15, 31, 40, 52]. This may potentially create an arrhythmogenic substrate, e.g. by inducing early after depolarizations. Here, we demonstrate that the same changes in Ca2+ and K+ channel expression underlying the AP prolongation are functionally also associated with an increased AP-induced Ca2+ influx in atrophic hearts. Accordingly, the concept of a common response pattern seems also to hold true for these aspects of cell physiology. In contrast, however, cardiac atrophy is associated with reduced PLB phosphorylation, a reduced SR Ca2+ content and a reduced SR Ca2+ release. Each of these aspects could be expected to be increased in cardiac hypertrophy [5, 9, 31, 47]. The remodelling of these SR-associated properties in cardiac atrophy therefore appears to be opposite to that in cardiac hypertrophy. The remodelling of the resulting systolic Ca2+ transients cannot be assigned to either concept. While cardiac hypertrophy is typically associated with an increased amplitude of systolic Ca2+ transients [9, 47], atrophic hearts have identical Ca2+ transients as control hearts. Thus, the load-dependent remodelling of systolic Ca2+ transients may follow a “rectification”: while they are increased in response to an increased cardiac workload, they are conserved during states of decreased cardiac workload.
References
Agus ZS, Dukes ID, Morad M (1991) Divalent cations modulate the transient outward current in rat ventricular myocytes. Am J Physiol 261:C310–C318
Baskin KK, Taegtmeyer H (2011) Taking pressure off the heart: the ins and outs of atrophic remodelling. Cardiovasc Res 90:243–250
Benitah JP, Alvarez JL, Gomez AM (2010) L-type Ca2+ current in ventricular cardiomyocytes. J Mol Cell Cardiol 48:26–36
Bers DM (2008) Calcium cycling and signaling in cardiac myocytes. Annu Rev Physiol 70:23–49
Bito V, Heinzel FR, Biesmans L, Antoons G, Sipido KR (2008) Crosstalk between L-type Ca2+ channels and the sarcoplasmic reticulum: alterations during cardiac remodelling. Cardiovasc Res 77:315–324
Bode EF, Briston SJ, Overend CL, O'Neill SC, Trafford AW et al (2011) Changes of SERCA activity have only modest effects on sarcoplasmic reticulum Ca2+ content in rat ventricular myocytes. J Physiol 589:4723–4729
Boknik P, Heinroth-Hoffmann I, Kirchhefer U, Knapp J, Linck B et al (2001) Enhanced protein phosphorylation in hypertensive hypertrophy. Cardiovasc Res 51:717–728
Callewaert G, Cleemann L, Morad M (1989) Caffeine-induced Ca2+ release activates Ca2+ extrusion via Na+–Ca2+ exchanger in cardiac myocytes. Am J Physiol 257:C147–C152
Carvalho BM, Bassani RA, Franchini KG, Bassani JW (2006) Enhanced calcium mobilization in rat ventricular myocytes during the onset of pressure overload-induced hypertrophy. Am J Physiol Heart Circ Physiol 291:H1803–H1813
Cerbai E, Barbieri M, Li Q, Mugelli A (1994) Ionic basis of action potential prolongation of hypertrophied cardiac myocytes isolated from hypertensive rats of different ages. Cardiovasc Res 28:1180–1187
Chorvatova A, Hart G, Hussain M (2004) Na+/Ca2+ exchange current (I Na/Ca) and sarcoplasmic reticulum Ca2+ release in catecholamine-induced cardiac hypertrophy. Cardiovasc Res 61:278–287
Depre C, Shipley GL, Chen W, Han Q, Doenst T et al (1998) Unloaded heart in vivo replicates fetal gene expression of cardiac hypertrophy. Nat Med 4:1269–1275
Dibb KM, Graham HK, Venetucci LA, Eisner DA, Trafford AW (2007) Analysis of cellular calcium fluxes in cardiac muscle to understand calcium homeostasis in the heart. Cell Calcium 42:503–512
El-Armouche A, Schwoerer AP, Neuber C, Emmons J, Biermann D et al (2010) Common microRNA signatures in cardiac hypertrophic and atrophic remodeling induced by changes in hemodynamic load. PLoS One 5:e14263
Foltz WU, Wagner M, Rudakova E, Volk T (2012) N-Acetylcysteine prevents electrical remodeling and attenuates cellular hypertrophy in epicardial myocytes of rats with ascending aortic stenosis. Basic Res Cardiol 107:290
Goonasekera SA, Hammer K, Auger-Messier M, Bodi I, Chen X et al (2012) Decreased cardiac L-type Ca2+ channel activity induces hypertrophy and heart failure in mice. J Clin Invest 122:280–290
Harzheim D, Movassagh M, Foo RS, Ritter O, Tashfeen A et al (2009) Increased InsP3Rs in the junctional sarcoplasmic reticulum augment Ca2+ transients and arrhythmias associated with cardiac hypertrophy. Proc Natl Acad Sci U S A 106:11406–11411
Heineke J, Molkentin JD (2006) Regulation of cardiac hypertrophy by intracellular signalling pathways. Nat Rev Mol Cell Biol 7:589–600
Hill JA, Olson EN (2008) Cardiac plasticity. N Engl J Med 358:1370–1380
Hobai IA, Bates JA, Howarth FC, Levi AJ (1997) Inhibition by external Cd2+ of Na/Ca exchange and L-type Ca channel in rabbit ventricular myocytes. Am J Physiol 272:H2164–H2172
Ibrahim M, Al MA, Navaratnarajah M, Siedlecka U, Soppa GK et al (2010) Prolonged mechanical unloading affects cardiomyocyte excitation–contraction coupling, transverse-tubule structure, and the cell surface. FASEB J 24:3321–3329
Ito K, Nakayama M, Hasan F, Yan X, Schneider MD et al (2003) Contractile reserve and calcium regulation are depressed in myocytes from chronically unloaded hearts. Circulation 107:1176–1182
Janczewski AM, Lakatta EG (1993) Thapsigargin inhibits Ca2+ uptake, and Ca2+ depletes sarcoplasmic reticulum in intact cardiac myocytes. Am J Physiol 265:H517–H522
Kashimura T, Briston SJ, Trafford AW, Napolitano C, Priori SG et al (2010) In the RyR2R4496C mouse model of CPVT, β-adrenergic stimulation induces Ca waves by increasing SR Ca content and not by decreasing the threshold for Ca waves. Circ Res 107:1483–1489
Kranias EG, Hajjar RJ (2012) Modulation of cardiac contractility by the phospholamban/SERCA2a regulatome. Circ Res 110:1646–1660
Litwin SE, Bridge JH (1997) Enhanced Na(+)–Ca2+ exchange in the infarcted heart. Implications for excitation–contraction coupling. Circ Res 81:1083–1093
Mechmann S, Pott L (1986) Identification of Na–Ca exchange current in single cardiac myocytes. Nature 319:597–599
Mills GD, Kubo H, Harris DM, Berretta RM, Piacentino V III et al (2006) Phosphorylation of phospholamban at threonine-17 reduces cardiac adrenergic contractile responsiveness in chronic pressure overload-induced hypertrophy. Am J Physiol Heart Circ Physiol 291:H61–H70
Minatoya Y, Ito K, Kagaya Y, Asaumi Y, Takeda M et al (2007) Depressed contractile reserve and impaired calcium handling of cardiac myocytes from chronically unloaded hearts are ameliorated with the administration of physiological treatment dose of T3 in rats. Acta Physiol (Oxf) 189:221–231
Negretti N, Varró A, Eisner DA (1995) Estimate of net calcium fluxes and sarcoplasmic reticulum calcium content during systole in rat ventricular myocytes. J Physiol 486:581–591
Osadchii OE (2007) Cardiac hypertrophy induced by sustained β-adrenoreceptor activation: pathophysiological aspects. Heart Fail Rev 12:66–86
Perrier E, Perrier R, Richard S, Benitah JP (2004) Ca2+ controls functional expression of the cardiac K+ transient outward current via the calcineurin pathway. J Biol Chem 279:40634–40639
Picht E, Zima AV, Blatter LA, Bers DM (2007) SparkMaster: automated calcium spark analysis with ImageJ. Am J Physiol Cell Physiol 293:C1073–C1081
Pohlmann L, Kroger I, Vignier N, Schlossarek S, Kramer E et al (2007) Cardiac myosin-binding protein C is required for complete relaxation in intact myocytes. Circ Res 101:928–938
Puglisi JL, Yuan W, Bassani JW, Bers DM (1999) Ca2+ influx through Ca2+ channels in rabbit ventricular myocytes during action potential clamp: influence of temperature. Circ Res 85:e7–e16
Rajabi M, Kassiotis C, Razeghi P, Taegtmeyer H (2007) Return to the fetal gene program protects the stressed heart: a strong hypothesis. Heart Fail Rev 12:331–343
Ronkainen JJ, Hanninen SL, Korhonen T, Koivumaki JT, Skoumal R et al (2011) Ca2+-calmodulin-dependent protein kinase II represses cardiac transcription of the L-type calcium channel α1C-subunit gene (Cacna1c) by DREAM translocation. J Physiol 589:2669–2686
Rousseau E, Meissner G (1989) Single cardiac sarcoplasmic reticulum Ca2+-release channel: activation by caffeine. Am J Physiol 256:H328–H333
Santiago DJ, Curran JW, Bers DM, Lederer WJ, Stern MD et al (2010) Ca sparks do not explain all ryanodine receptor-mediated SR Ca leak in mouse ventricular myocytes. Biophys J 98:2111–2120
Schwoerer AP, Melnychenko I, Goltz D, Hedinger N, Broichhausen I et al (2008) Unloaded rat hearts in vivo express a hypertrophic phenotype of cardiac repolarization. J Mol Cell Cardiol 45:633–641
Schwoerer AP, Neuber C, Schmechel A, Melnychenko I, Mearini G et al (2008) Mechanical unloading of the rat heart involves marked changes in the protein kinase–phosphatase balance. J Mol Cell Cardiol 45:846–852
Shannon TR, Ginsburg KS, Bers DM (2002) Quantitative assessment of the SR Ca2+ leak–load relationship. Circ Res 91:594–600
Shorofsky SR, Aggarwal R, Corretti M, Baffa JM, Strum JM et al (1999) Cellular mechanisms of altered contractility in the hypertrophied heart: big hearts, big sparks. Circ Res 84:424–434
Song LS, Stern MD, Lakatta EG, Cheng H (1997) Partial depletion of sarcoplasmic reticulum calcium does not prevent calcium sparks in rat ventricular myocytes. J Physiol 505(Pt 3):665–675
Soppa GK, Lee J, Stagg MA, Siedlecka U, Youssef S et al (2008) Prolonged mechanical unloading reduces myofilament sensitivity to calcium and sarcoplasmic reticulum calcium uptake leading to contractile dysfunction. J Heart Lung Transplant 27:882–889
Takaseya T, Ishimatsu M, Tayama E, Nishi A, Akasu T et al (2004) Mechanical unloading improves intracellular Ca2+ regulation in rats with doxorubicin-induced cardiomyopathy. J Am Coll Cardiol 44:2239–2246
Toischer K, Rokita AG, Unsold B, Zhu W, Kararigas G et al (2010) Differential cardiac remodeling in preload versus afterload. Circulation 122:993–1003
Tomaselli GF, Marban E (1999) Electrophysiological remodeling in hypertrophy and heart failure. Cardiovasc Res 42:270–283
Varró A, Negretti N, Hester SB, Eisner DA (1993) An estimate of the calcium content of the sarcoplasmic reticulum in rat ventricular myocytes. Pflügers Arch 423:158–160
Venetucci LA, Trafford AW, Eisner DA (2007) Increasing ryanodine receptor open probability alone does not produce arrhythmogenic calcium waves: threshold sarcoplasmic reticulum calcium content is required. Circ Res 100:105–111
Volk T, Nguyen THD, Schultz JH, Ehmke H (1999) Relationship between transient outward K+ current and Ca2+ influx in rat cardiac myocytes of endo- and epicardial origin. J Physiol 519:841–850
Volk T, Nguyen THD, Schultz JH, Faulhaber J, Ehmke H (2001) Regional alterations of repolarizing K+ currents among the left ventricular wall of rats with ascending aortic stenosis. J Physiol 530:443–455
Volk T, Noble PJ, Wagner M, Noble D, Ehmke H (2004) Ascending aortic stenosis selectively increases action potential-induced Ca2+ influx in epicardial myocytes of the rat left ventricle. Exp Physiol 90:111–121
Volk T, Schwoerer AP, Thiessen S, Schultz JH, Ehmke H (2003) A polycystin-2-like large conductance cation channel in rat left ventricular myocytes. Cardiovasc Res 58:76–88
Wittköpper K, Fabritz L, Neef S, Ort KR, Grefe C, Unsöld B, Kirchhof P, Maier LS, Hasenfuss G, Dobrev D, Eschenhagen T, El-Armouche A (2010) Constitutively active phosphatase inhibitor-1 improves cardiac contractility in young mice but is deleterious after catecholaminergic stress and with aging. J Clin Invest 120(2):617–626
Acknowledgments
This work was supported by the Deutsche Herzstiftung (APS and AEA), by the Deutsche Forschungsgemeinschaft (DFG, EL 270/5-1), by the DFG FOR-604 (HE) and DFG SFB-1002 (AEA, WHZ, LSM) and by the Deutsches Zentrum für Herz-Kreislauf-Forschung (DZHK; German Centre for Cardiovascular Research: APS, HE, LC, WHZ, TE, AEA, LSM).
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article
Cite this article
Schwoerer, A.P., Neef, S., Broichhausen, I. et al. Enhanced Ca2+ influx through cardiac L-type Ca2+ channels maintains the systolic Ca2+ transient in early cardiac atrophy induced by mechanical unloading. Pflugers Arch - Eur J Physiol 465, 1763–1773 (2013). https://doi.org/10.1007/s00424-013-1316-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00424-013-1316-y