
Abstract
Somatic mutations in the isocitrate dehydrogenase genes IDH1 and IDH2 occur at high frequency in several tumour types. Even though these mutations are confined to distinct hotspots, we show that gliomas are the only tumour type with an exceptionally high percentage of IDH1R132H mutations. Patients harbouring IDH1R132H mutated tumours have lower levels of genome-wide DNA-methylation, and an associated increased gene expression, compared to tumours with other IDH1/2 mutations (“non-R132H IDH1/2 mutations”). This reduced methylation is seen in multiple tumour types and thus appears independent of the site of origin. For 1p/19q non-codeleted glioma (astrocytoma) patients, we show that this difference is clinically relevant: in samples of the randomised phase III CATNON trial, patients harbouring tumours with IDH mutations other than IDH1R132H have a better outcome (hazard ratio 0.41, 95% CI [0.24, 0.71], p = 0.0013). Such non-R132H IDH1/2-mutated tumours also had a significantly lower proportion of tumours assigned to prognostically poor DNA-methylation classes (p < 0.001). IDH mutation-type was independent in a multivariable model containing known clinical and molecular prognostic factors. To confirm these observations, we validated the prognostic effect of IDH mutation type on a large independent dataset. The observation that non-R132H IDH1/2-mutated astrocytomas have a more favourable prognosis than their IDH1R132H mutated counterpart indicates that not all IDH-mutations are identical. This difference is clinically relevant and should be taken into account for patient prognostication.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Somatic mutations in the isocitrate dehydrogenase genes IDH1 and IDH2 occur at high frequency in various tumour types including gliomas (primary malignant central nervous system tumours), intrahepatic cholangiocarcinomas (bile duct tumours), enchondromas and chondrosarcomas (bone tumours), sinonasal undifferentiated carcinomas and leukemias [12, 33]. More sporadic but similar mutations have been found in a wide variety of other tumour types including melanoma, and prostate and pancreatic cancer [54]. IDH1/2 mutations are causal for the disease and tumours often remain dependent on the mutation for growth [22, 42]. The importance of the mutation is confirmed by the activity of IDH-inhibitors: inhibiting the mutant activity of either IDH1 or IDH2 shows anti-tumour activity in relapsed/refractory IDH1/2 mutated acute myeloid leukemia [14, 45] and cholangiocarcinoma patients [1]. The objective response rates in these trials are in the order of 40%, though patients eventually relapse. In gliomas, however, mutant IDH1/2 inhibitors have thus far not shown a survival benefit, but further studies on early-stage tumours are ongoing [32].
The IDH1/2 mutations are confined to defined gene hotspots and affect either arginine 132 (R132) in IDH1 or arginines R172 or R140 in IDH2. Although IDH1/2 mutations are confined to these three hotspots, several reports have shown that the IDH-mutation spectrum differs per tumour type [12, 15, 20, 37]. The hotspot mutations all change the activity of the wild-type (wt) protein from an enzyme that produces alpha-ketoglutarate (aKG) to an enzyme that produces D-2 hydroxyglutarate (D-2HG) [12, 27] which ultimately keeps cells in an undifferentiated state [19, 30], but individual IDH1/2 mutations differ in their ability to produce D-2HG [5, 40]. IDH1R132H, the IDH1/2 mutation with relatively low D-2HG production capacity, is the most common mutation in gliomas; other mutations such as IDH1R132C have tenfold lower KM and have higher enzymatic efficiency [5, 40]. This difference may have biological implications as not all aKG-dependent enzymes are equally well inhibited by D-2HG [11, 53]. For example, tet methylcytosine dioxygenase 2 (TET2) enzymes that mediate the first step in DNA-demethylation, requires relatively high D-2HG levels for inhibition [31, 53].
Here, we have used data from six large and independent DNA methylation datasets (the randomised phase III CATNON clinical trial on anaplastic 1p/19q non-codeleted gliomas [49], the TCGA-LGG cohort [8], samples included in the TAVAREC randomised phase 2 clinical trial on astrocytomas [51], a large cohort of acute myeloid leukemias (AML) [48] and a cohort of chondrosarcomas [52]) derived from four different tumour types, to examine the molecular effects of different types of IDH1/2 mutations. We report that tumours harbouring IDH1R132H mutations, regardless of tumour type, have lower genome-wide DNA methylation levels compared to those harbouring other IDH1/2 hotspot mutations (‘non-IDH1-R132H IDH1/2-mutated tumours’). For astrocytoma patients, we show this difference has clinical relevance as patients harbouring such non-IDH1R132H IDH1/2-mutated tumours have improved survival compared to those harbouring IDH1R132H mutations. Our data support the notion that increased genome-wide DNA methylation levels are associated with improved outcome in this tumour type and indicate that the type of IDH1/2 mutation should be taken into account for prognostication of astrocytoma patients.
Materials and methods
Datasets
The COSMIC database (Assessed 27 December 2019) was screened for hotspot IDH1 (R132) and IDH2 (R172 and R140) mutations. Mutations were stratified by tumour type; tumours with a low prevalence of mutations were concatenated (site of origin of ‘other tumours’: prostate n = 11, pancreas n = 6, skin n = 32, large intestine n = 1, soft tissue n = 22, endometrium n = 1, breast n = 9, urinary tract n = 2, liver n = 7, stomach n = 1, upper aerodigestive tract n = 35, salivary gland n = 1, thyroid n = 1). CATNON clinical data [49] and IDH1/2 mutation and DNA methylation data (Tesileanu, submitted) were reported previously. TCGA glioma data (DNA methylation and RNA-seq) [8], MSK-IMPACT data [9] and AML data [48] were downloaded from the TCGA data portal. Clinical data and mutation status for the chondrosarcoma data were reported previously [52]. Clinical data from the TAVAREC trial were derived from ref [51], and supplemented with DNA methylation data of 89 tumours. Most (80%) TAVAREC samples were derived from the initial tumour. Processing of CATNON and TAVAREC DNA methylation data was performed as described (Tesileanu, submitted). For the CATNON, TCGA-astrocytoma and TAVAREC datasets, we included only IDH1/2 mutated samples from non 1p/19q-codeleted tumours. Although all CATNON and TAVAREC samples were initially diagnosed as astrocytomas, DNA methylation analysis found 1p/19q codeletion in 8 samples included in the CATNON trial and 3 samples in the TAVAREC trial (Tesileanu, submitted). To ensure a molecularly homogenous sample cohort, all 1p/19q codeleted samples were removed prior to any analysis presented. For IDH1/2 mutated MSK-IMPACT samples, the distinction between astrocytic and oligodendrocytic tumours was made by absence or presence of telomerase reverse transcriptase (TERT) promoter mutations [26, 46]. In the Chinese Glioma Genome Atlas [CGGA] [23], the exact IDH1/2-mutation was not noted and therefore limited for the scope of this analysis. We used only the 1p/19q codeleted tumours in this dataset with IDH2 mutations being designated as “non-IDH1R132H IDH1/2-mutations” and all IDH1 mutations as “R132H”. In oligodendrogliomas, IDH1 mutations virtually always result in R132H [20]. RNA-seq data (raw read counts) were normalized and processed using DEseq2.
Statistical analysis
Survival curves were created using the Kaplan–Meier method. The log-rank test was used to determine survival differences. A Wilcoxon rank test on beta values (i.e. the intensity of the methylated probe/sum of methylated and unmethylated probe intensity) was used to identify differentially methylated probes in CATNON and TCGA-astrocytoma datasets. To increase power in the smaller sized datasets, we performed an F test on M values (i.e. the log2 ratio of the methylated/unmethylated probe intensities) to identify differentially methylated CpGs using the dmpFinder function in the Minfi Bioconductor package [4]. To further increase statistical power in the chondrosarcoma dataset (required as this dataset had few samples), we first made a selection of the most variable probes (i.e. those with a standard deviation > 2; ~ 5% of the total number of probes) followed by an F test on the M values. In all differential methylation analysis, p-values were corrected for false discovery rate (adjusted p-value).
Differences in mutation frequencies were determined using a chi-squared test. Pathway analysis was performed using Ingenuity pathway analysis (Qiagen, Venlo, The Netherlands). An association model was made with the Cox proportional hazards method and included, next to IDH1/2 mutation type, factors that are known to be related to outcome from literature such as sex, treatment with temozolomide, age at randomization, WHO performance score, O6-methylguanine DNA methyltransferase (MGMT) promoter methylation status, use of corticosteroids at randomization, and DNA methylation profiling. All p values below 0.05 were considered significant. Statistical analysis was performed using R version 3.6.3 and packages minfi, stats, rms, survival.
Results
The IDH1 R132H mutation predominates in gliomas
We screened the catalogue of somatic mutations in the cancer (COSMIC) database [16], extracted IDH1/2 hotspot mutation data (IDH1R132, IDH2R172 and IDH2R140) and stratified them by tumour organ site. As expected, tumours with a high frequency of IDH1/2 mutations include the central nervous system (CNS), biliary tract, bone, haematopoietic and lymphoid tumours (leukemias). Interestingly, even if there are only three mutational hotspots, there are marked differences in the distribution of mutations between tumour sites (Fig. 1). For example, the IDH1R132H mutation is by far the most predominant IDH1/2 mutation in CNS tumours (n = 7265/8026, 90.5%) whereas this mutation is present at much lower frequencies in bone (n = 49/361, 13.6%), leukemic (n = 519/2995, 17.3%) and other tumours (n = 14/129, 10.9%), and thus far has never been identified in biliary tract tumours (n = 212) (p < 0.001, chi-square test). In contrast, the mutation that results in IDH1R132C is quite rare in gliomas (223/8026, 2.8%) but much more prevalent in all other tumour types: bone (n = 212/361, 67.1%), leukemic (n = 493/2995, 16.5%), biliary tract (n = 114/212, 53.8%) and other tumours (n = 14/129, 10.9%). There is also a major difference in the distribution of IDH2 mutations which are very common in haematopoietic and lymphoid tumours but rare in all other tumour types. Mutations of the R140 in IDH2 are virtually exclusive to haematopoietic and lymphoid tumours.

IDH1 and IDH2 hotspot mutation distribution separated by site of origin. IDH1R132H mutations are the most predominant mutation in gliomas, IDH2 mutations are most common to haematopoietic tumours
DNA methylation is lower in IDH1 R132H mutant glioma
We used genome-wide DNA methylation data from CATNON trial samples and compared profiles of IDH1R132H mutated tumours (n = 369) to those harbouring other “non-R132H” IDH1 and IDH2 hotspot mutations (n = 69). Our data shows that the overall level of DNA methylation was significantly lower in tumours harbouring IDH1R132H mutations compared to tumours harbouring non-IDH1R132H IDH1/2-mutations. For example, there are 2461 probes showing a reduction in beta values > 0.2 in IDH1R132H mutated tumours (at p < 0.01) but there are no probes showing an increase > 0.2. This is exemplified in the volcano plot where a strong skew towards increased DNA methylation in non-IDH1R132H IDH1/2- mutated samples is observed (Fig. 2a). Probes showing the largest increase in DNA methylation were those that were partially methylated in IDH1R132H mutated tumours (i.e. probes with beta values between 0.25 and 0.75); there were few probes that became (partially) methylated from an unmethylated state (Fig. 2b).

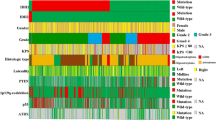
Non-R132H IDH1/2-mutations are associated with higher DNA methylation levels and improved survival of 1p19q non-codeleted astrocytoma patients included in the CATNON trial. Volcano plot (a) and XY plot (b) showing differences in methylation in non-R132H IDH1/2 vs. IDH1R132H mutated tumours. c Patients harbouring non-R132H IDH1/2-mutated tumours have improved outcome, which is independent of methylation class (d). e Heatmap of the most differentially methylated probes (red dots in a and b), shows a gradient in methylation levels. Non-R132H IDH1/2-mutated tumours cluster at the far left (high methylation), where poor prognostic methylation subtypes (epigenetics subtypes) cluster at the opposite end
Gliomas with higher levels of genome-wide DNA methylation generally are associated with longer survival in adults [8, 13, 28, 35]. Since non-R132H IDH1/2-mutated gliomas have increased DNA methylation levels, we compared the overall survival of patients with different IDH mutations. In patients included in the CATNON randomised phase III clinical trial, those harbouring tumours with non-R132H IDH1/2-mutations indeed had longer overall survival compared to patients harbouring IDH1R132H mutated tumours (Fig. 2c). The hazard ratio for non-R132H IDH1/2-mutations compared to IDH1R132H mutations was 0.41, 95% CI [0.24, 0.71], p = 0.0013.
DNA methylation profiling can also assign tumours to specific (prognostic) methylation subclasses. In line with the poorer survival, IDH1R132H mutated tumours also had a significantly higher proportion assigned to the prognostically poorer subclass A_IDH_HG (“IDH-mutant, high-grade astrocytoma”, n = 100/366 vs. 9/71, p = 0.036, Chi-squared test) using the subclasses as defined by Capper et al. (“CNS-classifier”) [7]. They also have a higher proportion of G-CIMP low tumours (18/369 vs. 0/62) and G-CIMP-high tumours with risk to progression to G-CIMP low (111/335 vs. 2/62) in the classifier as defined by the TCGA and de Souza et al. (“glioma classifier”, p < 0.001, chi-squared test, Table 1) [8, 13].
A heatmap of the most differentially methylated CpGs of CATNON data (n = 677, selected on a beta value change > 0.25 and false discovery corrected p values < 10e−5) shows a gradient from high to low methylation levels. As expected, the non-R132H IDH1/2-mutated tumours cluster together at the high-methylation end of this spectrum. Interestingly, most of the tumours with less favourable molecular subtypes (A_IDH_HG, G-CIMP low, G-CIMP high with risk to progression) clustered together at the other, demethylated end (Fig. 2e). Although the clinical follow-up of CATNON patients is limited, the number of mortality events also tended to cluster at the demethylated end of the heatmap which suggests that there is a strong correlation between the level of methylation of these 677 probes and survival.
To determine whether the type of mutation is a prognostic factor independent of the DNA methylation subtypes, we stratified these subtypes by IDH1/2 mutation (IDH1R132H vs. non-R132H IDH1/2 mutated). Our data show that, even within the prognostic DNA methylation subtypes, patients harbouring non-R132H IDH1/2-mutated tumours had a significantly longer survival compared to those harbouring IDH1R132H-mutated tumours, regardless of the classifier used (Fig. 2d, supplementary Fig. 1, Online resource). The type of IDH1/2 mutation was also an independent prognostic factor in a multivariable analysis that included all known factors associated with survival in this trial (treatment, age, corticosteroid use and sex, supplementary Table 1, online resource). It remained significant when DNA methylation subclass was included in this analysis (Table 1, Supplementary Table 2, online resource). These data demonstrate that the type of IDH1/2 mutation is an independent factor associated with patient survival.
To confirm these observations, we performed a similar analysis on the IDH1/2 mutated, 1p/19q non-codeleted glioma patients included in the TCGA dataset [8]. Similar to observed in the CATNON dataset, a striking increase in DNA methylation levels was seen in non-R132H IDH1/2-mutated tumours compared to those harbouring a IDH1R132H mutation (Fig. 3a, b). Also similar was the observation that patients harbouring non-R132H IDH1/2-mutated tumours survived significantly longer; the hazard ratio (HR) of patients harbouring non-R132H IDH1/2- mutated tumours (n = 37) versus IDH1R132H-mutated tumours (n = 177) was 0.20 (95% CI [0.047, 0.837], p = 0.028 Fig. 3c). Finally, IDH1R132H mutated tumours also had a higher proportion of tumours assigned to the prognostically poorer G-CIMP low DNA methylation class (4/116 vs. 0/27) and a higher number at risk of progression to G-CIMP low (29/111 vs. 0/24, p = 0.016). The type of IDH mutation remained a factor significantly associated with survival in a multivariable model that contained tumour grade and patient age (supplementary Table 3, online resource).

Non-R132H IDH1/2-mutations are associated with higher DNA methylation levels, lower gene expression and improved survival of 1p19q non-codeleted astrocytoma patients of the TCGA. Volcano plot (a) and XY plot (b) showing differences in methylation in non-R132H IDH1/2 vs. IDH1R132H mutated tumours. c Patients harbouring non-R132H IDH1/2-mutated tumours have improved outcome. d Volcanoplot showing differential expression of genes between non-R132H IDH1/2 and IDH1R132H mutated tumours. Most differentially expressed genes (red dots) have lower expression in non-R132H IDH1/2-mutated tumours (see also Supplementary Table 2, online resource)
DNA methylation generally shows a negative correlation with gene expression, especially when the methylated CpGs are located near the transcriptional start site [44, 50]. We, therefore, examined whether the reduction in DNA methylation in IDH1R132H mutated tumours is associated with an increase in gene expression in the 1p/19q non-codeleted gliomas present in the TCGA dataset. Indeed, of the genes differentially expressed between IDH mutation types (with > twofold change in expression level at p < 0.01 significance level) in astrocytomas, most (157/183, 86%) were upregulated in IDH1R132H mutated tumours (Fig. 3d, Supplementary Table 4, online resource). Pathway analysis using these 183 genes indicates that genes upregulated in IDH1R132H mutated tumours were involved in cellular movement, cell death and survival, cell-to-cell signalling and interaction and carbohydrate metabolism (Supplementary Fig. 2, online resource).
We performed a second validation using 1p/19q non-codeleted samples included in the randomised phase II TAVAREC clinical trial. Again, the vast majority of probes had lower DNA methylation levels in IDH1R132H mutated tumours (n = 83) compared to non-R132H IDH1/2- mutated tumours (n = 11, Fig. 4a) and the most differentially methylated probes were those partially methylated in IDH1R132H mutated tumours (Fig. 4b). Moreover, there was a large degree of overlap in differential DNA methylation between CATNON and TAVAREC samples (Fig. 4c). In TAVAREC, there was no significant difference in survival between patients harbouring IDH1R132H and non-R132H IDH1/2-mutated tumours (HR 1.21, 95% CI [0.60, 2.45], p = 0.60). This, however, may be related to the specific inclusion criteria of this trial: patients were included only when the tumour showed signs of malignant progression at the time of progression (i.e. contrast enhancement on the MRI scan). In this respect, it is interesting to note that the percentage of non-R132H IDH1/2-mutated tumours was almost two-fold lower in TAVAREC trial samples (13%) compared to CATNON (19%) and TCGA (20%). Although this difference in frequency was not significant, these numbers are in line with the notion that non-R132H IDH1/2-mutated tumours have lower frequencies of malignant progression. The small number of patients harbouring non-R132H IDH1/2-mutated tumours (n = 11) may also mask potential survival differences. A heatmap of most differentially methylated probes shows that non-R132H IDH1/2-mutated tumours and tumours assigned to the prognostically poorer subclass A_IDH_HG clustered at opposite ends of this heatmap (Fig. 4d).

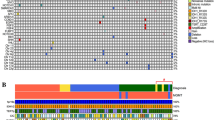
Non-R132H IDH1/2-mutations are associated with higher DNA methylation levels in 1p19q non-codeleted astrocytoma samples of patients included in the Tavarec trial. Volcano plot (a) and XY plot (b) showing differences in methylation in non-R132H IDH1/2 vs. IDH1R132H mutated tumours. c Differential methylation between non-R132H IDH1/2 vs. IDH1R132H mutated tumours showed a large degree of overlap in CATNON (x axis) and Tavarec (y axis) samples. d Heatmap of the most differentially methylated probes (red dots in a and b), shows a gradient in methylation levels. Non-R132H IDH1/2-mutated tumours cluster at the far left (high methylation), where poor prognostic methylation subtypes (epigenetics subtypes) cluster at the opposite end. e Forrest plot showing the summary HR estimate of 1p19q non-codeleted astrocytoma patients harbouring non-R132H IDH1/2 vs. IDH1R132H mutated tumours
A forest plot of the combined CATNON, TCGA and TAVAREC survival data shows a summary estimate HR for non-R132H IDH1/2-mutated tumours of 0.56 with 95% CI [0.37, 0.85], association p = 0.006 (Fig. 4e).
To test whether mutation-dependent DNA methylation differences were restricted to 1p/19q non-codeleted gliomas (astrocytomas), we analysed the genome-wide methylation profiles of (i) IDH1/2 mutated, 1p/19q codeleted gliomas (oligodendrogliomas, TCGA), (ii) acute myeloid leukemias (TCGA) and (iii) chondrosarcomas. Although the sample sizes of these datasets were relatively small in all tumour types (1p/19q codeleted gliomas n = 135 vs. 14; acute myeloid leukemias n = 4 vs. n = 24; chondrosarcomas n = 3 vs. n = 17 for IDH1R132H and non-R132H IDH1/2-mutated tumours respectively), there was less DNA methylation in IDH1R132H vs. non-R132H IDH1/2-mutation tumours (Fig. 5a–c). These data demonstrate that the level of DNA methylation is lower in tumours harbouring IDH1/2 mutations with presumed low D-2HG production.

non-R132H IDH1/2-mutations are associated with higher DNA methylation levels independent of tumour type. Volcano plot of 1p19q codeleted oligodendrogliomas (a), AML (b) and chondrosarcomas (c) showing differences in methylation in non-R132H IDH1/2 vs. IDH1R132H mutated tumours. Red dots depict CpGs that had a > 0.2 change in beta value and were significant (p < 0.01). Although the difference in chondrosarcomas is less than in other tumour types, the majority of significant CpGs was in non-R132H IDH1/2-mutated tumours (e.g. 225 CpG showed a > 0.3 increase in beta value at p < 0.01 where only 47 showed a similar decrease). d Gene expression differences between non-R132H IDH1/2 vs. IDH1R132H mutated tumours in 1p19q non-codeleted astrocytomas (x-axis) and 1p19q codeleted oligodendrogliomas (y-axis) shows a large degree of overlap. Blue, green and red dots depict genes significantly differentially expressed in astrocytomas, oligodendrogliomas or both respectively (see also Supplementary Tables 2 and 3, online resource). e Survival of 1p19q codeleted oligodendroglioma patients present in the TCGA database harbouring non-R132H IDH1/2 vs. IDH1R132H mutated tumours. There were too few events evaluate survival differences per mutation type. f Mutation type-specific survival differences in AML
Gene expression analysis of 1p/19q codeleted gliomas present in the TCGA dataset identified 148 differentially expressed genes (expression fold change > 1 or < − 1 and p < 0.01). Similar to observed in astrocytic tumours, the majority of identified genes (123/148, 83%) were upregulated in IDH1R132H mutated tumours (Supplementary Table 5, online resource). Moreover, there was a relatively large degree of concordance in differential expression between the two analyses (Fig. 5d) and sixteen genes were identified in both analyses.
The number of samples and events of the various datasets in patients with 1p/19q codeleted gliomas was insufficient to determine mutation type-dependent survival differences. For example, there were only 14 non-R132H IDH1/2-mutated 1p/19q codeleted tumours in the TCGA dataset, with only 1 event noted (in the IDH1R132H mutated tumours there were 14 events in 135 patients). The HR for TCGA samples was 0.59 (95% CI [0.077, 4.595], p = 0.62, Fig. 5e). Also in the MSK-Impact [9] and the Chinese Glioma Genome Atlas (CGGA) [23] there were too few samples and events to determine survival benefit in patients harbouring non-R132H IDH1/2–mutated tumours. In these datasets, the events/number in non-R132H IDH1/2 vs. IDH1R132H mutated samples was 0/6 vs. 3/34 and 0/5 vs. 3/31 in MSK impact, and CGGA datasets respectively. We were not able to determine survival differences in AML (n = 12 with 5 events vs. n = 89, 54 events, HR 1.49, 95% CI [0.59, 3.75], p = 0.39, Fig. 5f).
Discussion
Our data shows that IDH1/2mt gliomas are distinct when compared to other IDH1/2mt tumours in that they have a disproportionally high percentage of IDH1R132H mutations and raise the attractive clinical association between different rarer (codon 132) mutations and outcome. Patients harbouring IDH1R132H mutated tumours have lower levels of genome-wide DNA methylation, regardless of tumour type (1p/19q non-codeleted gliomas, 1p/19q codeleted gliomas, AML and chondrosarcomas). For 1p/19q non-codeleted IDH1/2mt gliomas, this difference is clinically relevant as patients harbouring non-R132H IDH1/2-mutated tumours have improved outcome. Since IDH1R132H mutations are presumed to be relatively poor in D-2HG production, our data are in line with the observation that glioma patients with higher D-2HG levels have improved outcome [34]. Our data are also in line with data from a meeting abstract showing similar mutation-specific survival differences [17].
The observation that patients harbouring non-R132H IDH1/2-mutated gliomas have longer survival is of importance for clinical practice as the specific IDH1/2 mutation could alter patient prognostication. In this respect diagnostic assays should be able to discriminate between the type of IDH-mutation present; non-R132H IDH1/2-mutations comprise ~ 10% of all IDH-mutations in astrocytomas. Moreover, the efficacy of treatment with alkylating agents, IDH1/2 inhibitors, or other novel treatments might vary per mutation type, and therefore may be taken into account as a stratification factor in future clinical trials.
It has been reported that individual IDH1/2 mutations differ in their ability to produce D-2HG. In fact, the most common mutation in gliomas, IDH1R132H, is reported to be relatively inefficient in producing this oncometabolite [5, 40]. The differential capacity of IDH mutations in D-2HG production is supported by observations from cell lines and clinical samples where tumours harbouring the IDH1R132H mutation generally have lower D-2HG levels compared to those with other IDH mutations [21, 24, 25, 29, 40] (but not in all [10]) though confounding factors such as tumour purity may influence these observations. Previous reports have shown that D-2HG is a weak inhibitor of TET2 enzymes as relatively high levels of D-2HG are required to inhibit the enzyme [31, 53]. In fact, the IC50 value for TET2 inhibition (~ 5 mM) is in the same range as the intratumoral D-2HG levels [10, 21, 29, 31]. As TET2 mediates the first step in DNA demethylation, lower D-2HG levels may result in reduced inhibition of DNA-demethylation. Therefore, although we did not directly measure D-2HG levels, the partial inhibition of TET2 may explain the lower overall methylation in IDH1R132H-mutated tumours.
The improved outcome of non-R132H IDH1/2-mutated astrocytomas may be explained by a reduced expression of genes that support tumour growth and/or induce treatment sensitivity caused by the increase in CpG methylation. Evidence supporting this hypothesis is the observation that many of the differentially expressed genes are involved in pathways associated with cancer. However, the improved outcome of non-R132H IDH1/2-mutated astrocytomas may also be related to the observation that D-2HG is toxic to cells, though only at high concentrations. For example, we have previously shown that exposure to D-2HG or expression of mutated IDH constructs reduced proliferation of cells, both in-vitro and in-vivo [6]. Later independent studies largely confirmed these observations and also conversely, reduction of D-2HG levels by mutant IDH inhibitors increased cell proliferation [18, 38, 40, 47, 55]. It should be noted, however, that in some preclinical model systems a growth inhibitory effect of IDH-inhibitors was observed [39, 41]. Functional experiments should confirm this hypothesis. Alternatively, differences in genetic stress and related mutational signatures may also explain the differential distribution of mutations in IDH [2, 3].
Apart from the type of IDH mutation present in the tumour, other prognostically relevant factors have also been described [43]. This includes histological tumour grade where patients with grade 2 astrocytomas have longer survival than those with grade 3 or grade 4 [36]. It should be noted, however, that we find that tumour grade is not a prognostic factor for the TCGA samples included in this study while the type of IDH-mutation is. In addition, the CATNON trial was performed on anaplastic (grade 3) tumours only.
Limitations of this study include the relatively small sample size of several datasets, especially those with a diagnosis other than the non-1p/19q codeleted gliomas. In addition, the absence of D-2HG level data limits the exploration of a direct correlation between IDH1/2 mutation type and genome-wide DNA methylation.
In short, we described the effect of IDH1/2 mutation type on patient outcome and the strong correlation between these specific mutations and genome-wide DNA methylation status. Our observation that non-R132H IDH1/2-mutated 1p/19q non-codeleted gliomas have a more favourable prognosis than their IDH1R132H mutated counterpart is clinically relevant and should be taken into account for patient prognostication.
References
Abou-Alfa GK, Macarulla T, Javle MM, Kelley RK, Lubner SJ, Adeva J et al (2020) Ivosidenib in IDH1-mutant, chemotherapy-refractory cholangiocarcinoma (ClarIDHy): a multicentre, randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol 21:796–807
Alexandrov LB, Kim J, Haradhvala NJ, Huang MN, Tian Ng AW, Wu Y et al (2020) The repertoire of mutational signatures in human cancer. Nature 578:94–101
Alexandrov LB, Nik-Zainal S, Wedge DC, Aparicio SA, Behjati S, Biankin AV et al (2013) Signatures of mutational processes in human cancer. Nature 500:415–421
Aryee MJ, Jaffe AE, Corrada-Bravo H, Ladd-Acosta C, Feinberg AP, Hansen KD et al (2014) Minfi: a flexible and comprehensive bioconductor package for the analysis of infinium DNA methylation microarrays. Bioinformatics 30:1363–1369
Avellaneda Matteo D, Grunseth AJ, Gonzalez ER, Anselmo SL, Kennedy MA, Moman P et al (2017) Molecular mechanisms of isocitrate dehydrogenase 1 (IDH1) mutations identified in tumors: the role of size and hydrophobicity at residue 132 on catalytic efficiency. J Biol Chem 292:7971–7983
Bralten LB, Kloosterhof NK, Balvers R, Sacchetti A, Lapre L, Lamfers M et al (2011) IDH1 R132H decreases proliferation of glioma cell lines in vitro and in vivo. Ann Neurol 69:455–463
Capper D, Jones DTW, Sill M, Hovestadt V, Schrimpf D, Sturm D et al (2018) DNA methylation-based classification of central nervous system tumours. Nature 555:469–474
Ceccarelli M, Barthel FP, Malta TM, Sabedot TS, Salama SR, Murray BA et al (2016) Molecular profiling reveals biologically discrete subsets and pathways of progression in diffuse glioma. Cell 164:550–563
Cheng DT, Mitchell TN, Zehir A, Shah RH, Benayed R, Syed A et al (2015) Memorial Sloan Kettering-integrated mutation profiling of actionable cancer targets (MSK-IMPACT): a hybridization capture-based next-generation sequencing clinical assay for solid tumor molecular oncology. J Mol Diagn JMD 17:251–264
Choi C, Ganji SK, DeBerardinis RJ, Hatanpaa KJ, Rakheja D, Kovacs Z et al (2012) 2-hydroxyglutarate detection by magnetic resonance spectroscopy in IDH-mutated patients with gliomas. Nat Med 18:624–629
Chowdhury R, Yeoh KK, Tian YM, Hillringhaus L, Bagg EA, Rose NR et al (2011) The oncometabolite 2-hydroxyglutarate inhibits histone lysine demethylases. EMBO Rep 12:463–469
Clark O, Yen K, Mellinghoff IK (2016) Molecular pathways: isocitrate dehydrogenase mutations in cancer. Clin Cancer Res 22:1837–1842
de Souza CF, Sabedot TS, Malta TM, Stetson L, Morozova O, Sokolov A et al (2018) A distinct DNA methylation shift in a subset of glioma CpG island methylator phenotypes during tumor recurrence. Cell Rep 23:637–651
DiNardo CD, Stein EM, de Botton S, Roboz GJ, Altman JK, Mims AS et al (2018) Durable remissions with ivosidenib in IDH1-mutated relapsed or refractory AML. N Engl J Med 378:2386–2398
Farshidfar F, Zheng S, Gingras MC, Newton Y, Shih J, Robertson AG et al (2017) Integrative genomic analysis of cholangiocarcinoma identifies distinct IDH-mutant molecular profiles. Cell Rep 18:2780–2794
Forbes SA, Beare D, Boutselakis H, Bamford S, Bindal N, Tate J et al (2017) COSMIC: somatic cancer genetics at high-resolution. Nucleic Acids Res 45:D777–D783
Franceschi E, De Biase D, Pession A, Tosolini A, Paccapelo A, Visani L et al (2019) Survival outcomes in glioma patients with noncanonical IDH mutations: beyond diagnostic improvements. J Clin Oncol 37:2028
Fu X, Chin RM, Vergnes L, Hwang H, Deng G, Xing Y et al (2015) 2-Hydroxyglutarate inhibits ATP synthase and mTOR signaling. Cell Metab 22:508–515
Gagne LM, Boulay K, Topisirovic I, Huot ME, Mallette FA (2017) Oncogenic activities of IDH1/2 mutations: from epigenetics to cellular signaling. Trends Cell Biol 27:738–752
Gravendeel LA, Kloosterhof NK, Bralten LB, van Marion R, Dubbink HJ, Dinjens W et al (2010) Segregation of non-p.R132H mutations in IDH1 in distinct molecular subtypes of glioma. Hum Mutat 31:E1186-1199
Gross S, Cairns RA, Minden MD, Driggers EM, Bittinger MA, Jang HG et al (2010) Cancer-associated metabolite 2-hydroxyglutarate accumulates in acute myelogenous leukemia with isocitrate dehydrogenase 1 and 2 mutations. J Exp Med 207:339–344
Hirata M, Sasaki M, Cairns RA, Inoue S, Puviindran V, Li WY et al (2015) Mutant IDH is sufficient to initiate enchondromatosis in mice. Proc Natl Acad Sci U S A 112:2829–2834
Hu H, Mu Q, Bao Z, Chen Y, Liu Y, Chen J et al (2018) Mutational landscape of secondary glioblastoma guides MET-targeted trial in brain tumor. Cell 175(1665–1678):e1618
Jin G, Reitman ZJ, Spasojevic I, Batinic-Haberle I, Yang J, Schmidt-Kittler O et al (2011) 2-hydroxyglutarate production, but not dominant negative function, is conferred by glioma-derived NADP-dependent isocitrate dehydrogenase mutations. PLoS ONE 6:e16812
Kanamori M, Maekawa M, Shibahara I, Saito R, Chonan M, Shimada M et al (2018) Rapid detection of mutation in isocitrate dehydrogenase 1 and 2 genes using mass spectrometry. Brain Tumor Pathol 35:90–96
Killela PJ, Reitman ZJ, Jiao Y, Bettegowda C, Agrawal N, Diaz Jr LA et al (2013) TERT promoter mutations occur frequently in gliomas and a subset of tumors derived from cells with low rates of self-renewal. Proc Natl Acad Sci U S A 110:6021–6026
Kloosterhof NK, Bralten LB, Dubbink HJ, French PJ, van den Bent MJ (2011) Isocitrate dehydrogenase-1 mutations: a fundamentally new understanding of diffuse glioma? Lancet Oncol 12:83–91
Kloosterhof NK, de Rooi JJ, Kros M, Eilers PH, Sillevis Smitt PA, van den Bent MJ et al (2013) Molecular subtypes of glioma identified by genome-wide methylation profiling. Genes Chromosomes Cancer 52:665–674
Longuespee R, Wefers AK, De Vita E, Miller AK, Reuss DE, Wick W et al (2018) Rapid detection of 2-hydroxyglutarate in frozen sections of IDH mutant tumors by MALDI-TOF mass spectrometry. Acta Neuropathol Commun 6:21
Losman JA, Kaelin WG Jr (2013) What a difference a hydroxyl makes: mutant IDH, (R)-2-hydroxyglutarate, and cancer. Genes Dev 27:836–852
Losman JA, Koivunen P, Kaelin WG Jr (2020) 2-Oxoglutarate-dependent dioxygenases in cancer. Nat Rev Cancer 20:710–726
Mellinghoff IK, Ellingson BM, Touat M, Maher E, De La Fuente MI, Holdhoff M et al. (2020) Ivosidenib in Isocitrate Dehydrogenase 1-Mutated Advanced Glioma. J Clin Oncol JCO1903327
Mito JK, Bishop JA, Sadow PM, Stelow EB, Faquin WC, Mills SE et al (2018) Immunohistochemical detection and molecular characterization of IDH-mutant sinonasal undifferentiated carcinomas. Am J Surg Pathol 42:1067–1075
Natsumeda M, Igarashi H, Nomura T, Ogura R, Tsukamoto Y, Kobayashi T et al (2014) Accumulation of 2-hydroxyglutarate in gliomas correlates with survival: a study by 3.0-tesla magnetic resonance spectroscopy. Acta Neuropathol Commun 2:158
Noushmehr H, Weisenberger DJ, Diefes K, Phillips HS, Pujara K, Berman BP et al (2010) Identification of a CpG island methylator phenotype that defines a distinct subgroup of glioma. Cancer Cell 17:510–522
Ostrom QT, Cioffi G, Gittleman H, Patil N, Waite K, Kruchko C et al (2019) CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2012–2016. Neuro Oncol 21:v1–v100
Pansuriya TC, van Eijk R, d’Adamo P, van Ruler MA, Kuijjer ML, Oosting J et al (2011) Somatic mosaic IDH1 and IDH2 mutations are associated with enchondroma and spindle cell hemangioma in Ollier disease and Maffucci syndrome. Nat Genet 43:1256–1261
Pickard AJ, Sohn AS, Bartenstein TF, He S, Zhang Y, Gallo JM (2016) Intracerebral Distribution of the oncometabolite d-2-hydroxyglutarate in mice bearing mutant isocitrate dehydrogenase brain tumors: implications for tumorigenesis. Front Oncol 6:211
Pusch S, Krausert S, Fischer V, Balss J, Ott M, Schrimpf D et al (2017) Pan-mutant IDH1 inhibitor BAY 1436032 for effective treatment of IDH1 mutant astrocytoma in vivo. Acta Neuropathol 133:629–644
Pusch S, Schweizer L, Beck AC, Lehmler JM, Weissert S, Balss J et al (2014) D-2-Hydroxyglutarate producing neo-enzymatic activity inversely correlates with frequency of the type of isocitrate dehydrogenase 1 mutations found in glioma. Acta Neuropathol Commun 2:19
Rohle D, Popovici-Muller J, Palaskas N, Turcan S, Grommes C, Campos C et al (2013) An inhibitor of mutant IDH1 delays growth and promotes differentiation of glioma cells. Science 340:626–630
Sasaki M, Knobbe CB, Munger JC, Lind EF, Brenner D, Brustle A et al (2012) IDH1(R132H) mutation increases murine haematopoietic progenitors and alters epigenetics. Nature 488:656–659
Shirahata M, Ono T, Stichel D, Schrimpf D, Reuss DE, Sahm F et al (2018) Novel, improved grading system(s) for IDH-mutant astrocytic gliomas. Acta Neuropathol 136:153–166
Spainhour JC, Lim HS, Yi SV, Qiu P (2019) Correlation patterns between DNA methylation and gene expression in the cancer genome atlas. Cancer Inform 18:1176935119828776
Stein EM, DiNardo CD, Pollyea DA, Fathi AT, Roboz GJ, Altman JK et al (2017) Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood 130:722–731
Suzuki H, Aoki K, Chiba K, Sato Y, Shiozawa Y, Shiraishi Y et al (2015) Mutational landscape and clonal architecture in grade II and III gliomas. Nat Genet 47:458–468
Tateishi K, Wakimoto H, Iafrate AJ, Tanaka S, Loebel F, Lelic N et al (2015) Extreme vulnerability of IDH1 mutant cancers to NAD+ depletion. Cancer Cell 28:773–784
Tyner JW, Tognon CE, Bottomly D, Wilmot B, Kurtz SE, Savage SL et al (2018) Functional genomic landscape of acute myeloid leukaemia. Nature 562:526–531
van den Bent MJ, Baumert B, Erridge SC, Vogelbaum MA, Nowak AK, Sanson M et al (2017) Interim results from the CATNON trial (EORTC study 26053–22054) of treatment with concurrent and adjuvant temozolomide for 1p/19q non-co-deleted anaplastic glioma: a phase 3, randomised, open-label intergroup study. Lancet 390:1645–1653
van den Bent MJ, Gravendeel LA, Gorlia T, Kros JM, Lapre L, Wesseling P et al (2011) A hypermethylated phenotype is a better predictor of survival than MGMT methylation in anaplastic oligodendroglial brain tumors: a report from EORTC study 26951. Clin Cancer Res 17:7148–7155
van den Bent MJ, Klein M, Smits M, Reijneveld JC, French PJ, Clement P et al (2018) Bevacizumab and temozolomide in patients with first recurrence of WHO grade II and III glioma, without 1p/19q co-deletion (TAVAREC): a randomised controlled phase 2 EORTC trial. Lancet Oncol 19:1170–1179
Venneker S, Kruisselbrink AB, Baranski Z, Palubeckaite I, Briaire-de Bruijn IH, Oosting J et al (2020) Beyond the influence of IDH mutations: exploring epigenetic vulnerabilities in chondrosarcoma. Cancers (Basel) 12:3589
Xu W, Yang H, Liu Y, Yang Y, Wang P, Kim SH et al (2011) Oncometabolite 2-hydroxyglutarate is a competitive inhibitor of alpha-ketoglutarate-dependent dioxygenases. Cancer Cell 19:17–30
Zehir A, Benayed R, Shah RH, Syed A, Middha S, Kim HR et al (2017) Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nat Med 23:703–713
Zhang Y, Pusch S, Innes J, Sidlauskas K, Ellis M, Lau J et al (2019) Mutant IDH sensitizes gliomas to endoplasmic reticulum stress and triggers apoptosis via miR-183-mediated inhibition of semaphorin 3E. Cancer Res 79:4994–5007
Acknowledgements
The CATNON study was funded by Merck, Sharp and Dohme, and the Brain Tumor Group. The genome-wide DNA methylation profiles study was funded by Grant GN-000577 from The Brain Tumour Charity, grant 10685 from the Dutch Cancer Society, financial support from the Vereniging Heino ’Strijd van Salland’, and Grant CA170278 from the United States Department of Defence. The authors thank the European Organization for Research and Treatment of Cancer for permission to use the data from EORTC studies 26053/22054 (CATNON) and 26091 (TAVAREC) for this research.
Author information
Authors and Affiliations
Contributions
Conceptualization: PJF. Methodology: CMT, YH, PJF. Validation: CMT. Investigation CMT, WRV, IdH, MdW, LB, PJF. Resources: MS, WT, PMC, WW, AAB, JFV, OLC, HW, SG, MG, LR, RR, MW, CMcB, JR, RHE, FC, TL, SC, AG, EL, FdV, PJM, MJBT, SV, JO, JVMGB, SE, MAV, AKN, WPM, JMK, PW, KA, RBJ, HJD, BB, VG, MvdB. Data curation CMT, TG, PJF. Writing-original draft: CMT, WRV, MvdB, PJF. Writing-review and editing: all authors. Visualization: CMT, PJF. Supervision: MvdB, PJF.
Corresponding author
Ethics declarations
Conflict of interest
MS reports research grants from Astra-Zeneca, travel grant from Abbvie, personal fees from Genenta, outside the submitted work, PM reports support to attend conferences from BMS and an award towards an investigator-initiated study from BMS. BB reports a MERCK grant for the EORTC22033 lGG study. MAV has indirect equity interest and royalty rights from Infuseon Therapeutics, Inc. He has received honoraria from Tocagen, Cellinta, and Celgene. None of these interests overlaps with the research presented in this manuscript. Wolfgang Wick receives trial funding from Apogenix, Boehringer Ingelheim, Pfizer and Roche to the institution. He serves on advisory boards for Agios, Bayer, MSD, Novartis, Roche with compensation paid to the institution. MJvdB reports grants from Dutch Cancer Foundation, grants from Brain Tumor Charity, grants from Strijd van Salland, grants from MSD formerly Schering Plough, during the conduct of the study; personal fees from Carthera, personal fees from Nerviano, personal fees from Bayer, personal fees from Celgene, personal fees from Agios, personal fees from Abbvie, personal fees from Karyopharm, personal fees from Boston Pharmaceuticals, personal fees from Genenta, outside the submitted work. AN received research funding from Astra Zeneca, and Douglas Pharmaceuticals, consultancies for Bayer, Roche, Boehringer Ingelheim, MSD, Douglas Pharmaceuticals, Pharmabcine, Atara biotherapeutics, Trizell and Seagen. MW has received research grants from Abbvie, Adastra, Merck, Sharp & Dohme (MSD), Merck (EMD), Novocure and Quercis, and honoraria for lectures or advisory board participation or consulting from Abbvie, Adastra, Basilea, Bristol Meyer Squibb (BMS), Celgene, Medac, Merck, Sharp & Dohme (MSD), Merck (EMD), Nerviano Medical Sciences, Novartis, Orbus, Philogen, Roche and Tocagen. FdV reports support from AbbVie, Bioclin Therapeutics, BMS, GSK, Novartis, Octimed Oncology and Vaximm, outside the submitted work. PC reports support from BMS, AbbVie, Merck Serono, MSD, Vifor Pharma, Daiichi Sankyo, Leo Pharma and Astra Zeneca, outside the submitted work. PJF reports grants from Dutch Cancer Foundation, the Brain Tumor Charity, the Strijd van Salland, de Westlandse ride and Hersentumorfonds, outside submitted work. Other authors report no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tesileanu, C.M.S., Vallentgoed, W.R., Sanson, M. et al. Non-IDH1-R132H IDH1/2 mutations are associated with increased DNA methylation and improved survival in astrocytomas, compared to IDH1-R132H mutations. Acta Neuropathol 141, 945–957 (2021). https://doi.org/10.1007/s00401-021-02291-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00401-021-02291-6