
Abstract
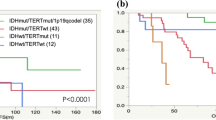
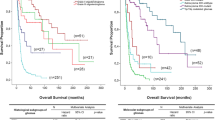
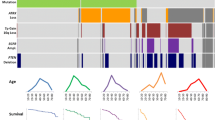
The “integrated diagnosis” for infiltrating gliomas in the 2016 revised World Health Organization (WHO) classification of tumors of the central nervous system requires assessment of the tumor for IDH mutations and 1p/19q codeletion. Since TERT promoter mutations and ATRX alterations have been shown to be associated with prognosis, we analyzed whether these tumor markers provide additional prognostic information within each of the five WHO 2016 categories. We used data for 1206 patients from the UCSF Adult Glioma Study, the Mayo Clinic and The Cancer Genome Atlas (TCGA) with infiltrative glioma, grades II-IV for whom tumor status for IDH, 1p/19q codeletion, ATRX, and TERT had been determined. All cases were assigned to one of 5 groups following the WHO 2016 diagnostic criteria based on their morphologic features, and IDH and 1p/19q codeletion status. These groups are: (1) Oligodendroglioma, IDH-mutant and 1p/19q-codeleted; (2) Astrocytoma, IDH-mutant; (3) Glioblastoma, IDH-mutant; (4) Glioblastoma, IDH-wildtype; and (5) Astrocytoma, IDH-wildtype. Within each group, we used univariate and multivariate Cox proportional hazards models to assess associations of overall survival with patient age at diagnosis, grade, and ATRX alteration status and/or TERT promoter mutation status. Among Group 1 IDH-mutant 1p/19q-codeleted oligodendrogliomas, the TERT-WT group had significantly worse overall survival than the TERT-MUT group (HR: 2.72, 95% CI 1.05–7.04, p = 0.04). In both Group 2, IDH-mutant astrocytomas and Group 3, IDH-mutant glioblastomas, neither TERT mutations nor ATRX alterations were significantly associated with survival. Among Group 4, IDH-wildtype glioblastomas, ATRX alterations were associated with favorable outcomes (HR: 0.36, 95% CI 0.17–0.81, p = 0.01). Among Group 5, IDH-wildtype astrocytomas, the TERT-WT group had significantly better overall survival than the TERT-MUT group (HR: 0.48, 95% CI 0.27–0.87), p = 0.02). Thus, we present evidence that in certain WHO 2016 diagnostic groups, testing for TERT promoter mutations or ATRX alterations may provide additional useful prognostic information.


Similar content being viewed by others
References
Arita H, Narita Y, Fukushima S, Tateishi K, Matsushita Y, Yoshida A, Miyakita Y, Ohno M, Collins VP, Kawahara N et al (2013) Upregulating mutations in the TERT promoter commonly occur in adult malignant gliomas and are strongly associated with total 1p19q loss. Acta Neuropathol 126:267–276. doi:10.1007/s00401-013-1141-6
Arita H, Yamasaki K, Matsushita Y, Nakamura T, Shimokawa A, Takami H, Tanaka S, Mukasa A, Shirahata M, Shimizu S et al (2016) A combination of TERT promoter mutation and MGMT methylation status predicts clinically relevant subgroups of newly diagnosed glioblastomas. Acta Neuropathol Commun 4:79. doi:10.1186/s40478-016-0351-2
Ceccarelli M, Barthel FP, Malta TM, Sabedot TS, Salama SR, Murray BA, Morozova O, Newton Y, Radenbaugh A, Pagnotta SM et al (2016) Molecular profiling reveals biologically discrete subsets and pathways of progression in diffuse glioma. Cell 164:550–563. doi:10.1016/j.cell.2015.12.028
Chamberlain MC, Born D (2015) Prognostic significance of relative 1p/19q codeletion in oligodendroglial tumors. J Neurooncol 125:249–251. doi:10.1007/s11060-015-1906-y
Clark KH, Villano JL, Nikiforova MN, Hamilton RL, Horbinski C (2013) 1p/19q testing has no significance in the workup of glioblastomas. Neuropathol Appl Neurobiol 39:706–717. doi:10.1111/nan.12031
Eckel-Passow JE, Lachance DH, Molinaro AM, Walsh KM, Decker PA, Sicotte H, Pekmezci M, Rice T, Kosel ML, Smirnov IV et al (2015) Glioma Groups Based on 1p/19q, IDH, and TERT Promoter Mutations in Tumors. N Engl J Med 372:2499–2508. doi:10.1056/NEJMoa1407279
Giannini C, Scheithauer BW, Weaver AL, Burger PC, Kros JM, Mork S, Graeber MB, Bauserman S, Buckner JC, Burton J et al (2001) Oligodendrogliomas: reproducibility and prognostic value of histologic diagnosis and grading. J Neuropathol Exp Neurol 60:248–262
Heaphy CM, de Wilde RF, Jiao Y, Klein AP, Edil BH, Shi C, Bettegowda C, Rodriguez FJ, Eberhart CG, Hebbar S et al (2011) Altered telomeres in tumors with ATRX and DAXX mutations. Science 333:425. doi:10.1126/science.1207313
Jiao Y, Killela PJ, Reitman ZJ, Rasheed AB, Heaphy CM, de Wilde RF, Rodriguez FJ, Rosemberg S, Oba-Shinjo SM, Nagahashi Marie SK et al (2012) Frequent ATRX, CIC, FUBP1 and IDH1 mutations refine the classification of malignant gliomas. Oncotarget 3:709–722. doi:10.18632/oncotarget.588
Kannan K, Inagaki A, Silber J, Gorovets D, Zhang J, Kastenhuber ER, Heguy A, Petrini JH, Chan TA, Huse JT (2012) Whole-exome sequencing identifies ATRX mutation as a key molecular determinant in lower-grade glioma. Oncotarget 3:1194–1203. doi:10.18632/oncotarget.689
Killela PJ, Reitman ZJ, Jiao Y, Bettegowda C, Agrawal N, Diaz LA Jr, Friedman AH, Friedman H, Gallia GL, Giovanella BC et al (2013) TERT promoter mutations occur frequently in gliomas and a subset of tumors derived from cells with low rates of self-renewal. Proc Natl Acad Sci USA 110:6021–6026. doi:10.1073/pnas.1303607110
Leeper HE, Caron AA, Decker PA, Jenkins RB, Lachance DH, Giannini C (2015) IDH mutation, 1p19q codeletion and ATRX loss in WHO grade II gliomas. Oncotarget 6:30295–30305. doi:10.18632/oncotarget.4497
Liu XY, Gerges N, Korshunov A, Sabha N, Khuong-Quang DA, Fontebasso AM, Fleming A, Hadjadj D, Schwartzentruber J, Majewski J et al (2012) Frequent ATRX mutations and loss of expression in adult diffuse astrocytic tumors carrying IDH1/IDH2 and TP53 mutations. Acta Neuropathol 124:615–625. doi:10.1007/s00401-012-1031-3
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK (2016) WHO Classification of Tumours of the Central Nervous System. International Agency for Research on Cancer, City
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW (2016) The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol 131:803–820. doi:10.1007/s00401-016-1545-1
Mur P, Mollejo M, Hernandez-Iglesias T, de Lope AR, Castresana JS, Garcia JF, Fiano C, Ribalta T, Rey JA, Melendez B (2015) Molecular classification defines 4 prognostically distinct glioma groups irrespective of diagnosis and grade. J Neuropathol Exp Neurol 74:241–249. doi:10.1097/nen.0000000000000167
Nguyen HN, Lie A, Li T, Chowdhury R, Liu F, Ozer B, Wei B, Green RM, Ellingson BM, Wang HJ et al (2016) Human TERT promoter mutation enables survival advantage from MGMT promoter methylation in IDH1 wild-type primary glioblastoma treated by standard chemoradiotherapy. Neuro Oncol. doi:10.1093/neuonc/now189
Ohgaki H, Kleihues P (2005) Population-based studies on incidence, survival rates, and genetic alterations in astrocytic and oligodendroglial gliomas. J Neuropathol Exp Neurol 64:479–489
Olar A, Sulman EP (2015) Molecular markers in low-grade glioma-toward tumor reclassification. Semin Radiat Oncol 25:155–163. doi:10.1016/j.semradonc.2015.02.006
R Core Team (2016) R: A language and environment for statistical computing. R Foundation for Statistical Computing, City
Reuss DE, Mamatjan Y, Schrimpf D, Capper D, Hovestadt V, Kratz A, Sahm F, Koelsche C, Korshunov A, Olar A et al (2015) IDH mutant diffuse and anaplastic astrocytomas have similar age at presentation and little difference in survival: a grading problem for WHO. Acta Neuropathol 129:867–873. doi:10.1007/s00401-015-1438-8
Scheie D, Meling TR, Cvancarova M, Skullerud K, Mork S, Lote K, Eide TJ, Helseth E, Beiske K (2011) Prognostic variables in oligodendroglial tumors: a single-institution study of 95 cases. Neuro Oncol 13:1225–1233. doi:10.1093/neuonc/nor114
Schwartzentruber J, Korshunov A, Liu XY, Jones DT, Pfaff E, Jacob K, Sturm D, Fontebasso AM, Quang DA, Tonjes M et al (2012) Driver mutations in histone H3.3 and chromatin remodelling genes in paediatric glioblastoma. Nature 482:226–231. doi:10.1038/nature10833
Suzuki H, Aoki K, Chiba K, Sato Y, Shiozawa Y, Shiraishi Y, Shimamura T, Niida A, Motomura K, Ohka F et al (2015) Mutational landscape and clonal architecture in grade II and III gliomas. Nat Genet 47:458–468. doi:10.1038/ng.3273
Walsh KM, Wiencke JK, Lachance DH, Wiemels JL, Molinaro AM, Eckel-Passow JE, Jenkins RB, Wrensch MR (2015) Telomere maintenance and the etiology of adult glioma. Neuro Oncol 17:1445–1452. doi:10.1093/neuonc/nov082
Wiestler B, Capper D, Holland-Letz T, Korshunov A, von Deimling A, Pfister SM, Platten M, Weller M, Wick W (2013) ATRX loss refines the classification of anaplastic gliomas and identifies a subgroup of IDH mutant astrocytic tumors with better prognosis. Acta Neuropathol 126:443–451. doi:10.1007/s00401-013-1156-z
Wrensch M, Jenkins RB, Chang JS, Yeh RF, Xiao Y, Decker PA, Ballman KV, Berger M, Buckner JC, Chang S et al (2009) Variants in the CDKN2B and RTEL1 regions are associated with high-grade glioma susceptibility. Nat Genet 41:905–908. doi:10.1038/ng.408
Yang P, Cai J, Yan W, Zhang W, Wang Y, Chen B, Li G, Li S, Wu C, Yao K et al (2016) Classification based on mutations of TERT promoter and IDH characterizes subtypes in grade II/III gliomas. Neuro Oncol 18:1099–1108. doi:10.1093/neuonc/now021
Acknowledgements
Work at University of California, San Francisco, was supported by the National Institutes of Health (Grant Numbers R01CA52689, P50CA097257, R01CA126831, R01CA139020 and R25CA112355), as well as the loglio Collective, the National Brain Tumor Foundation, The Sontag Foundation, the Stanley D. Lewis and Virginia S. Lewis Endowed Chair in Brain Tumor Research, the Robert Magnin Newman Endowed Chair in Neuro-oncology, and by donations from families and friends of John Berardi, Helen Glaser, Elvera Olsen, Raymond E. Cooper, and William Martinusen.
Work at the Mayo Clinic was supported by the National Institutes of Health (Grant Numbers P50CA108961 and P30CA15083), National Institute of Neurological Disorders and Stroke (Grant Number RC1NS068222Z), the Bernie and Edith Waterman Foundation, and the Ting Tsung and Wei Fong Chao Family Foundation.
This publication was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through UCSF-CTSI Grant Number UL1RR024131. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
The collection of cancer incidence data used in this study was supported by the California Department of Public Health as part of the statewide cancer reporting program mandated by California Health and Safety Code Sect. 103885; the National Cancer Institute’s Surveillance, Epidemiology and End Results Program under contract HHSN261201000140C awarded to the Cancer Prevention Institute of California, contract HHSN261201000035C awarded to the University of Southern California, and contract HHSN261201000034C awarded to the Public Health Institute; and the Centers for Disease Control and Prevention’s National Program of Cancer Registries, under agreement # U58DP003862-01 awarded to the California Department of Public Health. The ideas and opinions expressed herein are those of the author(s) and endorsement by the State of California Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors is not intended nor should be inferred.
The results published here are in whole or part based upon data generated by The Cancer Genome Atlas managed by the NCI and NHGRI. Information about TCGA can be found at http://cancergenome.nih.gov.
The authors wish to acknowledge study participants, the clinicians and research staff at the participating medical centers, the UCSF Helen Diller Family Comprehensive Cancer Center Genome Analysis Core which is supported by a National Cancer Institute Cancer Center Support Grant (5P30CA082103), the UCSF Cancer Registry, the UCSF Neurosurgery Tissue Bank, Katherine Cornelius, the late Dr. Bernd Scheithauer, the Mayo Clinic Center for Individualized Medicine, and the Mayo Clinic Comprehensive Cancer Center Biospecimens and Processing and Genotyping Shared Resources.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in this study.
Additional information
R. B. Jenkins and M. R. Wrensch contributed equally to this publication.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Pekmezci, M., Rice, T., Molinaro, A.M. et al. Adult infiltrating gliomas with WHO 2016 integrated diagnosis: additional prognostic roles of ATRX and TERT . Acta Neuropathol 133, 1001–1016 (2017). https://doi.org/10.1007/s00401-017-1690-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00401-017-1690-1