
Summary
Sarcopenia is a constant in aging. Observed over long periods, it can reach 1% per year. But it is such a tenuous phenomenon that it cannot be observed over short periods at steady state. The aging phenomenon mainly hits fibers, Type II but on aged muscle thin, normal, and hypertrophic fibers cohabit with sclerosis and fat increases.
Sarcopenia is difficult to study, due to the lack of simple clinical, biochemical, or imaging measures. Anthropometric data are largely dependent on water content. DEXA gives better information on appendicular muscle loss. Measures of strength analyze functional outcomes of sarcopenia.
Sarcopenia appears largely multifactorial. Hormonal changes, e.g., drop in growth hormone, menopause, and andropause, explain impaired protein synthesis. Disuse (sedentary, bed rest) may explain chronical protein lysis. But the main factor for muscle lysis imply life events and occurring diseases.
Cytokines (IL6, TNF alpha) and stress hormones (cortisol) induce quick protein lysis in muscle. Rapid and intensive successive aggressions during life cannot be compensated by slowed synthesis.
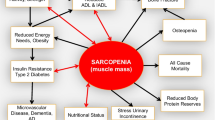
Harmful consequences of sarcopenia explain many disabilities of old age: loss of strength, inducing itself loss of mobility, falls, equilibrium disorders, poor ADL; loss of nutritional reserves (protein and glycogen) impairing capacities of immune response. Muscle loss spoils vital functions as respiration.
Treatment remains rather limited to resistance exercise. Although, these results are thin, they are the only ones to be validated in all the elderly even the frail or the old. However it is not efficient during the evolution of an inflammatory process. The powerful action of cytokine and cortisol on muscular hypermetabolism must be incited for early treatment of any infectious or inflammatory event. Nutritional supplementation has no efficiency in the absence of malnutrition and without exercise.
Although mobility impairments mainly due to sarcopenia are the first cause of disablement in the elderly, we lack information on etiology, evolution, and measurement of sarcopenia. We also lack controlled therapeutical studies.
Zusammenfassung
Sarkopenie – d. h. der alternsgängige Verlust von Muskelmasse und Muskelkraft – ist eine Konstante des Alterns. Über längere Zeitspannen beobachtet, kann sie etwa 1% pro Jahr ausmachen. Sie verläuft aber so schleichend, daß man sie bei kurzen Beobachtungszeiten nicht erkennen kann.
Dieser Prozeß betrifft vorwiegend Typ-II-Muskelfasern. Dennoch findet man in alter Muskulatur neben dünnen atrophischen auch normale und hypertrophische Fasern mit Sklerose und vermehrtem Fettgehalt.
Sarkopenie ist schwierig zu objektivieren, denn es fehlt an entsprechenden einfachen klinischen, biochemischen und bildgebenden Verfahren. Anthropometrische Daten hängen im weiten Bereich vom Wassergehalt des Gewebes ab. DEXA vermittelt hier bessere Informationen. Messungen der Muskelkraft untersuchen primär die funktionellen Folgen der Sarkopenie.
Sarkopenie imponiert als ein multifaktorielles Geschehen. Hormonale Änderungen – nämlich Abnahme des Wachstumshormons. Meno- und Andropause – erklären eine verschlechterte Proteinsynthese. Inaktivität verschiedener Ursachen kann eine chronische Proteolyse erklären. Aber die Hauptfaktoren des Muskelschwundes liegen in Lebensereignissen und in abgelaufenen Krankheiten.
Zytokine (IL 6 TNF-alpha) und Streßhormone (Cortisol) bewirken eine schnelle Proteolyse im Muskel. Rasche und wiederholte intensive Störungen können infolge einer verminderten Proteinsynthese nicht kompensiert werden.
Die negativen Auswirkungen der Sarkopenie erklären viele Nachteile des Alterns: Verlust von Kraft – die zu einem Mobilitätsverlust führt –, Stürze, Gleichgewichtsstörungen, Verminderung der ADL, Verlust von Protein und Glycogen mit negativen Rückwirkungen auf die Immunkompetenz. Muskelabbau kann außerdem vitale Funktionen wie z. B. die Atmung negativ beeinflussen.
Behandlung durch konsequentes Training bleibt wenig wirksam. Dennoch sind diese Ereignisse die einzigen bisher als sicher wirksam geltenden Maßnahmen bei allen Älteren, sogar bei Gebrechlichen und Hochbetagten. Sie helfen aber nicht bei Infektionen oder Entzündungen. Und die intensive Wirkung von Zytokinen und Cholesterol auf den muskulären Hyperkatabolismus muß zu einer möglichst frühen Behandlung von jeglichen Infekten oder Entzündungen anspornen.
Eine ausgewogenere Ernährung bleibt bei Fehlen von Mangelernährung und ohne konsequentes Training ohne Effekt.
Obgleich Mobilitätsstörungen als Folge von Sarkopenie die erste Ursache der Behinderungen im Alter sind, fehlen uns Kenntnisse über deren Ätiologie, Entwicklung oder Meßbarkeit. Und es mangelt auch noch an kontrollierten therapeutischen Studien.
Similar content being viewed by others

Author information
Authors and Affiliations
Additional information
Received: 10 July 1999, Accepted: 11 August 1999
Rights and permissions
About this article
Cite this article
Moulias, R., Meaume, S. & Raynaud-Simon, A. Sarcopenia, hypermetabolism, and aging. Z Gerontol Geriat 32, 425–432 (1999). https://doi.org/10.1007/s003910050140
Issue Date:
DOI: https://doi.org/10.1007/s003910050140