
Abstract
Background
Normocalcemic (NCpHPT) and normohormonal (NHpHPT) variants have been recognized primary hyperparathyroidism entities that pose serious challenges. We sought to define the differences among them in a series of surgically treated patients.
Patients and methods
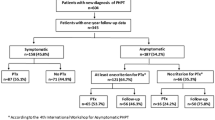
Between 2011 and 2015, 149 patients were enrolled into three groups: CpHPT (Ca > 10.2 mg/dL, PTH > 65 pg/mL), NCpHPT (normal Ca, PTH > 65 pg/mL) and NHpHPT (Ca > 10.2 mg/dL, normal PTH). Descriptive statistics and inter-group differences were computed, whereas multiple logistic/linear regression tests were used for further analysis.
Results
Of these patients 125 were female and 24 male, mean age 56.3 years (range 8–83). A total of 115 (77.2%) patients presented with CpHPT, 23 (15.4%) with NCpHPT and 11 (7.4%) with NHpHPT. MGD was found in 25 (16.8%) patients and SGD in 124 (83.2%); multivariate analysis failed to reveal statistically significant association of MGD with any pHPT variant (CpHPT 16.5% vs NCpHPT 21.7% vs NHpHPT 9.1%, p = 0.726). Conversely, NCpHPT patients exhibited statistically significant smaller adenoma weight (p = 0.023). Moreover, U/S in these patients had smaller positive predictive value (p = 0.278), whereas concordance between U/S and MIBI was also lower (p = 0.669). The utility of MIBI and U/S differed significantly (p < 0.001); more frequent use of U/S was observed for all groups. However, their predictive values did not differ significantly (p = 0.832).
Conclusions
NCpHPT is more similar than different to CpHPT. NCpHPT constitutes the most challenging entity: it is associated with smaller adenoma weight, whereas U/S exhibited lower positive predictive value and lower concordance rate with MIBI. A trend for higher MGD presence in this group of patients was observed, though without statistical significance.
Similar content being viewed by others


References
Bilezikian JP (2017) Primary hyperparathytoidism. In: De Groot LJ, Chrousos G, Dungan K, et al., (eds) Endotext. MDText.com, Inc, South Dartmouth (internet)
Gasser RW (2013) Clinical aspects of primary hyperparathyroidism: clinical manifestations, diagnosis, and therapy. Wien Med Wochenschr 163(17–18):397–402
Yeh MW, Ituarte PH, Zhour HC et al (2013) Incidence and prevalence of primary hyperparathyroidism in a racially mixed population 2013. J Clin Endocrinol Metab 98:1122–1129
Bilezikian JP, Khan A, Potts JT et al (2009) Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the third international workshop. J Clin Endocrinol Metab 94:335–339
Silverberg SJ, Clarke BL, Peacock M et al (2014) Current issues in the presentation of asymptomatic primary hyperparathyroidism: proceedings of the fourth international workshop. J Clin Endocrinol Metab 99(10):3580–3594. https://doi.org/10.1210/jc.2014-1415
Forster J, Monchik JM, Martin HF (1988) A comparative study of serum ultrafiltrable, ionized, and total calcium in the diagnosis of primary hyperparathyroidism in patients with intermittent or no elevation in total calcium. Surgery 104:1137–1142
Wills MR, Pak CY, Hammond WG, Bartter FC (1967) Normocalcemic primary hyperparathyroidism. Am J Med 47:384–391
Wallace LB, Parikh RT, Ross LV et al (2011) The phenotype of primary hyperparathyroidism with normal parathyroid hormone levels: how low can parathyroid hormone go? Surgery 150(6):1102–1112. https://doi.org/10.1016/j.surg.2011.09.011
Applewhite MK, White MG, Tseng J et al (2017) Normohormonal primary hyperparathyroidism is a distinct form of primary hyperparathyroidism. Surgery 161(1):62–69. https://doi.org/10.1016/j.surg.2016.03.038
Lavryk OA, Siperstein AE (2017) Use of calcium and parathyroid hormone nomogram to distinguish between atypical primary hyperparathyroidism and normal patients. World J Surg 41(1):122–128. https://doi.org/10.1007/s00268-016-3716-6
Lim JY, Herman MC, Bubis L et al (2017) Differences in single gland and multigland disease are seen in low biochemical profile primary hyperparathyroidism. Surgery 161(1):70–77. https://doi.org/10.1016/j.surg.2016.08.054
Amin AL, Wang TS, Wade TJ et al (2011) Normal PTH levels in primary hyperparathyroidism: still the same disease? Ann Surg Oncol 18(12):3437–3442. https://doi.org/10.1245/s10434-011-1744-x
Bergenfelz A, Lindblom P, Lindergard B, Valdemarsson S, Westerdahl J (2003) Preoperative normal level of parathyroid hormone signifies an early and mild form of primary hyperparathyroidism. World J Surg 27(4):481–485
Hollenberg AN, Arnold A (1991) Hypercalcemia with low-normal serum intact PTH: a novel presentation of primary hyperparathyroidism. Am J Med 91(5):547–548
Bilezikian JP, Brandi ML, Eastell R et al (2014) Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the fourth international workshop. Clin Endocrinol Metab 99(10):3561–3569. https://doi.org/10.1210/jc.2014-1413
Tordjman KM, Greenman Y, Osher E et al (2004) Characterization of normocalcemic primary hyperparathyroidism. Am J Med 117:861–863
Lowe H, McMahon DJ, Rubin MR et al (2007) Normocalcemic primary hyperparathyroidism: further characterization of a new clinical phenotype. J Clin Endocrinol Metab 92:3001–3005
García-Martín A, Reyes-García R, Muñoz-Torres M (2012) Normocalcemic primary hyperparathyroidism: one-year follow-up in one hundred postmenopausal women. Endocrine 42(3):764–766
Kontogeorgos G, Trimpou P, Laine CM et al (2015) Normocalcemic, vitamin D sufficient hyperparathyroidism—high prevalence and low morbidity in the general population: a long-term follow-up study, the WHO MONICA project, Gothenburg, Sweden. Clin Endocrinol (Oxf) 83(2):277–284
Lo CY, Chan WF, Kung AW et al (2004) Surgical treatment for primary hyperparathyroidism in Hong Kong: changes in clinical pattern over 3 decades. Arch Surg 139:77–82
McCoy KL, Chen NH, Armstrong MJ et al (2014) The small abnormal parathyroid gland is increasingly common and heralds operative complexity. World J Surg 38(6):1274–1281. https://doi.org/10.1007/s00268-014-2450-1
Mazeh H, Chen H, Leverson G et al (2012) Creation of a “Wisconsin Index” nomogram to predict the likelihood of additional hyperfunctioning parathyroid glands during parathyroidectomy. Ann Surg 257:138–141
Wade TJ, Yen TW, Amin AL et al (2012) Surgical management of normocalcemic primary hyperparathyroidism. World J Surg 36(4):761–766. https://doi.org/10.1007/s00268-012-1438-y
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Kiriakopoulos, A., Petralias, A. & Linos, D. Classic Primary Hyperparathyroidism Versus Normocalcemic and Normohormonal Variants: Do They Really Differ?. World J Surg 42, 992–997 (2018). https://doi.org/10.1007/s00268-018-4512-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-018-4512-2